
Abstract
Objective
To investigate the experience of remote outpatient menopause service delivery by clinicians and patients during the COVID-19 pandemic.
Methods
Two surveys explored the experiences of patients and clinicians separately. Patients attending menopause clinics in the UK were directed to an online survey which included questions on demographics and on their experience of their most recent appointment. A clinician survey was shared to members of the British Menopause Society (BMS) via email and was made available on the BMS website. It contained questions on clinic characteristics and clinicians’ experience of delivering remote menopause consultations. Surveys were available for completion between 01/12/2020 and 10/02/2021.
Results
Of 180 patients who completed the patient survey, 52% felt remote consultations were the same or better than face-to-face consultations, and 90% of patients felt a choice between remote and face-to-face consultations should be offered. Patients overall were satisfied with many aspects of care, though numerous problems were highlighted with appointment administration. Of 76 clinicians who completed the clinician survey, most found remote patient consultations either no different or a bit worse than face-to face consultations but found that they offered more flexibility. In some cases, significant rescheduling was necessary to accommodate for the clinical needs of the consultation.
Conclusion
A ‘one-size-fits-all’ approach to managing the delivery of menopause care is not supported by patients or clinicians. There must be a robust process in place to avoid problems with appointment scheduling and associated communications. Lessons learned from the pandemic can help to provide holistic menopause care.
Key points and recommendations
Patients
• 52% felt remote consultations the same or better than face to face consultations. • 90% of patients felt a choice between remote and face-to-face consultations should be offered. • Patients overall were satisfied with the convenience, duration and feeling of involvement in decisions about their care. • Satisfaction with the quality of service appeared to be higher in NHS hospital or private clinics than with GP review. • Irrespective of whether consultations took place in primary or secondary care, there were numerous problems with appointment administration (e.g. scheduling. cancellation, waiting times).
Clinicians
• Most clinicians found remote patient consultations, which were mostly by telephone (fewer via video), either no different, or a bit worse than face-to face consultations but to offer more flexibility. • In a small minority, however, significant rescheduling was necessary to accommodate for the clinical needs of the consultation (e.g. clinical examination, patient language and hearing difficulties). • There is a perception that remote consultations are associated with lower DNA rates.
Recommendations/conclusions
• A ‘one-size-fits-all’ approach to managing the delivery of menopause care is not supported by patients or clinicians. • Patient triage would enable a service tailored to medical and social need. Ideally this requires a nationally agreed consensus. • There must be a robust process in place, with sufficient administrative support, to avoid problems with appointment scheduling and associated communications. • Educational support for menopause management in primary care is required.
Introduction
This was an exploratory evaluation to investigate the impact of the COVID-19 pandemic on menopause service delivery for both patients and clinicians. Traditionally, outpatient care in NHS or private settings for most medical specialities has been almost exclusively face-to-face. This provides the opportunity to examine patients, perform tests ‘real time’ and build a patient/clinician relationship. However, the Covid-19 pandemic forced many clinics to re-evaluate how services could be organised and many clinics moved to a virtual setting. This can be a telephone or where possible a video consultation. While some areas of gynaecology do not lend themselves to this mode of communication, much of menopause care can be successfully conducted virtually. Symptom control and other concerns can be managed and any tests or examinations required can be scheduled appropriately. While some clinics had started to move towards this model, the Covid-19 pandemic and advances in technology allowing remote working have accelerated this. Patients are now able to schedule an appointment for their menopause care while at work, removing the time and expense involved in travelling to appointments.
We set out to explore and evaluate the experience of patients and clinicians during the pandemic via online surveys to ascertain the optimum style of menopause service. This should then be tailored to the clinical and social needs of the patients and clinicians leading to a nationally agreed standard of care.
Methods
Two surveys were designed following the format of the NHS GP Survey to assess the experience of remote outpatient menopause service delivery by clinicians and patients during the COVID-19 pandemic. 1 The content of both was agreed by the Medical Advisory Committee of the British Menopause Society (BMS). They were created using Google Forms and hosted online between 1st December 2020 and 10th February 2021. Patients and clinicians were directed to the surveys by convenience sampling.
The first survey, which explored patient experience, included 16 questions about their most recent appointment, 6 questions on patient demographics and a free-text question for further comments (Online Appendix A). Patients attending specialist menopause clinics in the UK were directed to the WHC website homepage where it was hosted.
The second survey was directed at clinicians and included 10 questions on their experience of delivering remote consultations, 3 questions on the characteristics of the clinic to which the clinician worked in and a free-text question for further comments (Online Appendix B). This survey was shared to clinicians who were BMS members via email link. This was sent directly to BMS members and was also available on the BMS website homepage.
Statistical analysis was performed in R (version 4.0.2). 95% confidence intervals (95% CI) are reported for proportions and were calculated using an exact binomial method.
2
As this was an exploratory analysis, there were no predefined hypothesis tests, and we do not report p-values. Data for both the patient and clinician surveys are available online at https://github.com/hugaped/BMS-Menopause-Clinic-Surveys. Themes emerging from the patient free-text responses were identified by two-independent researchers from free-text coding recommendations supplied by Patient and Public Involvement, King’s College Hospital NHS Foundation Trust (
Results
Patient survey
Characteristics of participants who completed the patient survey.
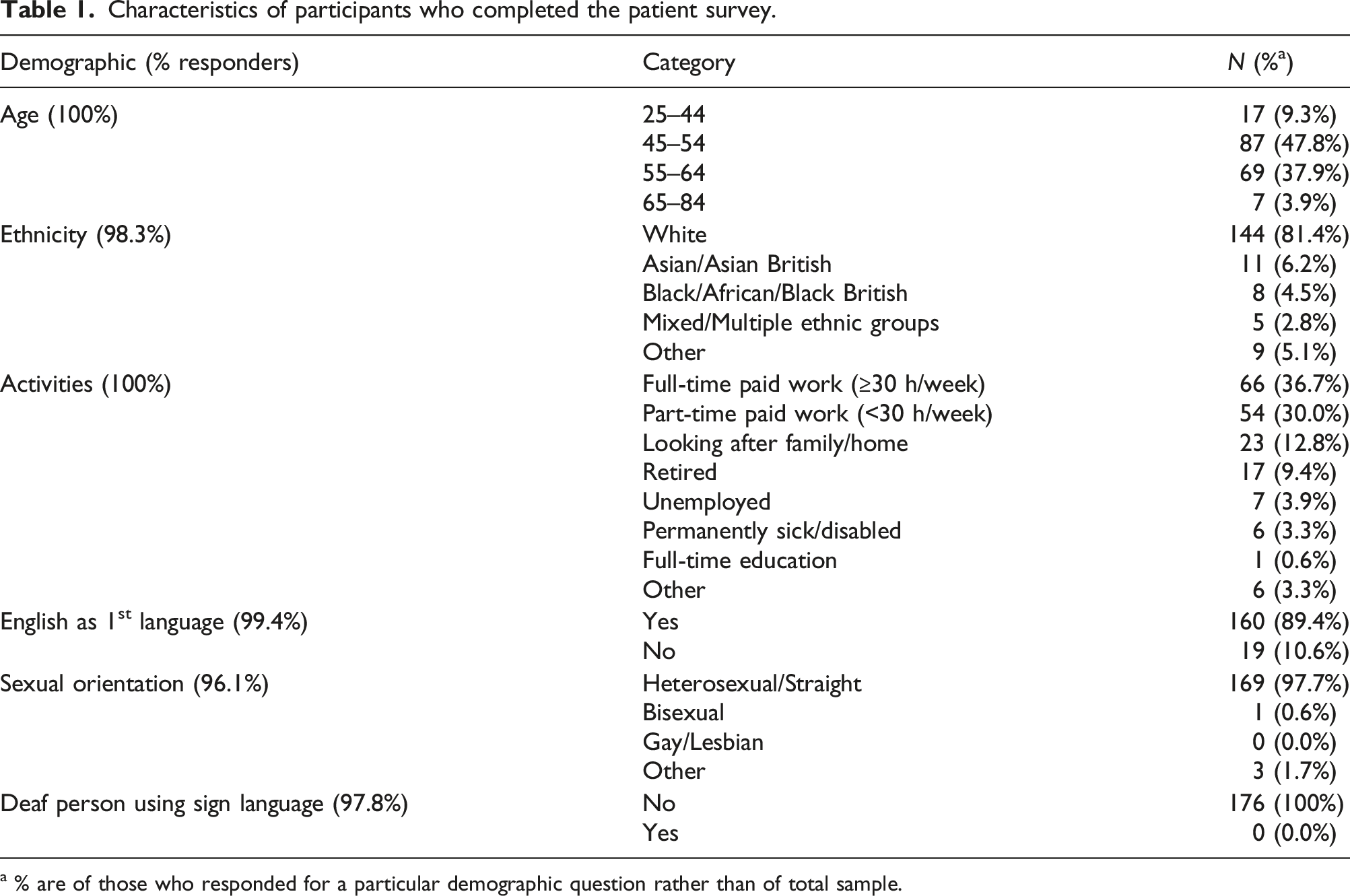
a % are of those who responded for a particular demographic question rather than of total sample.
Details regarding the previous menopause clinic appointment for participants who completed the patient survey.
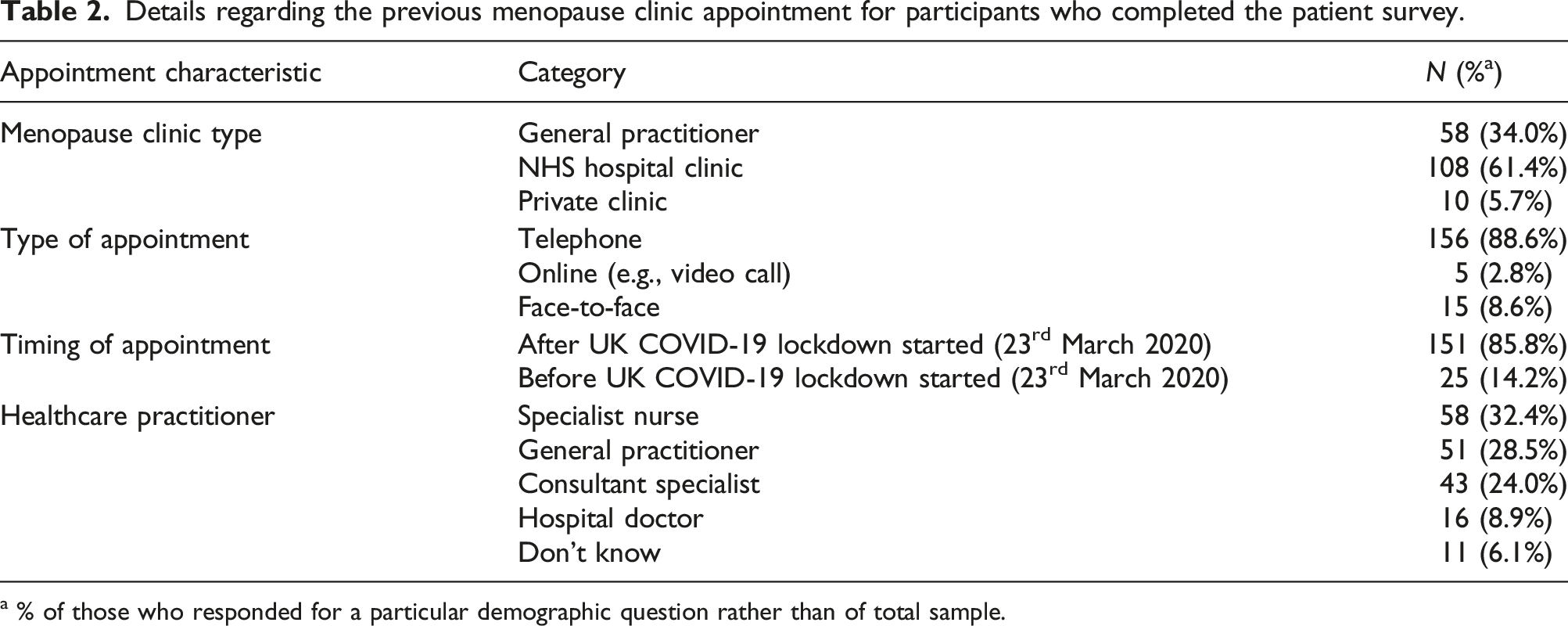
a % of those who responded for a particular demographic question rather than of total sample.
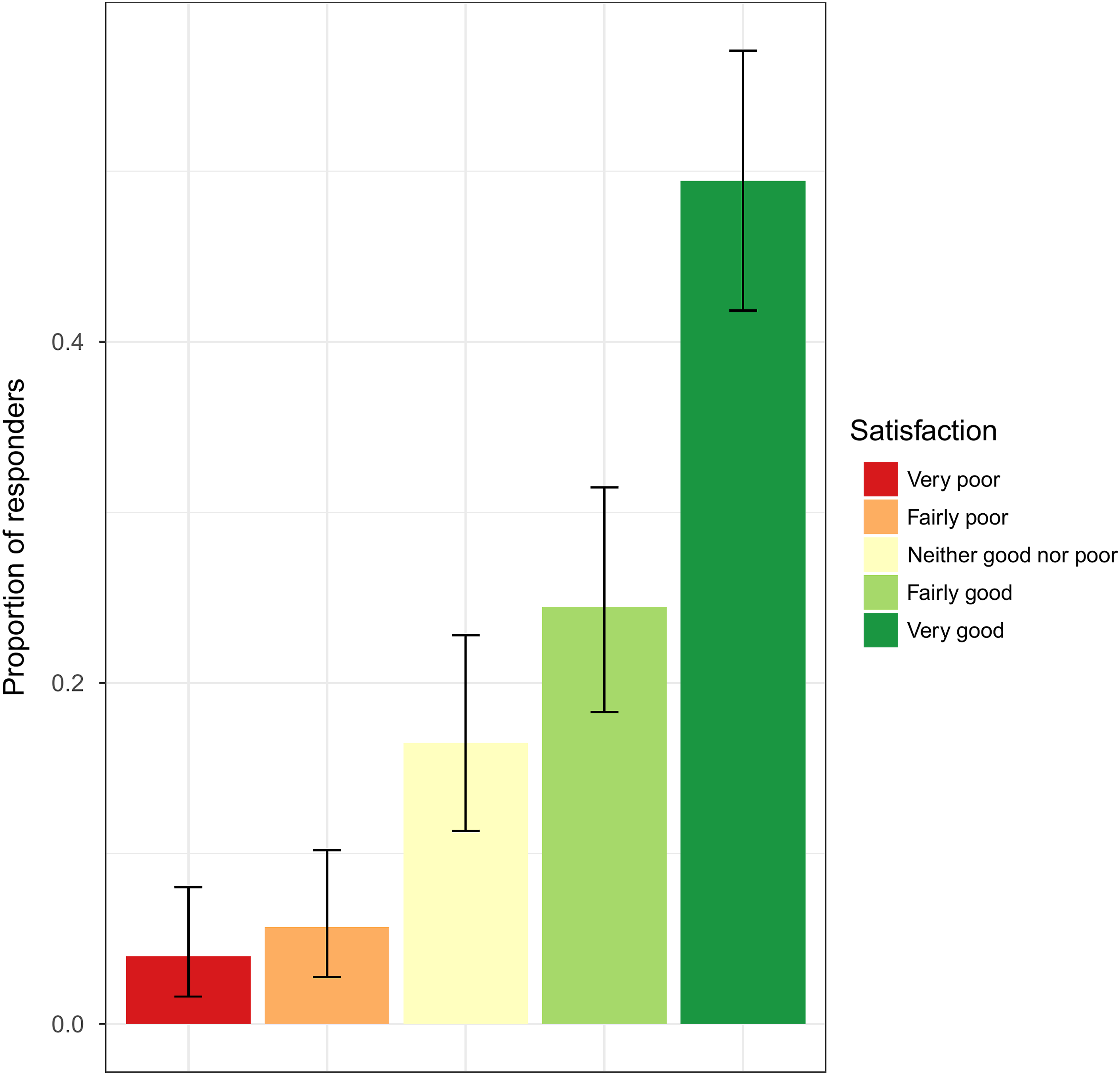
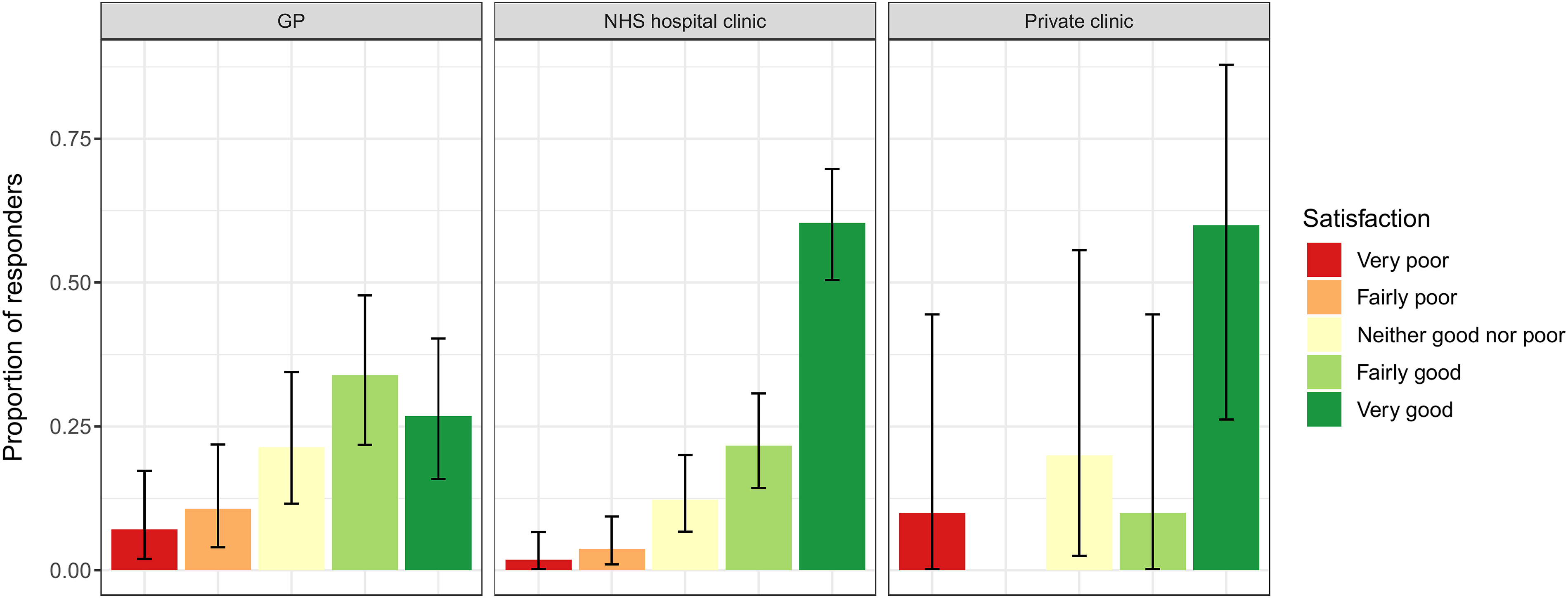
Key quantitative results for patient survey
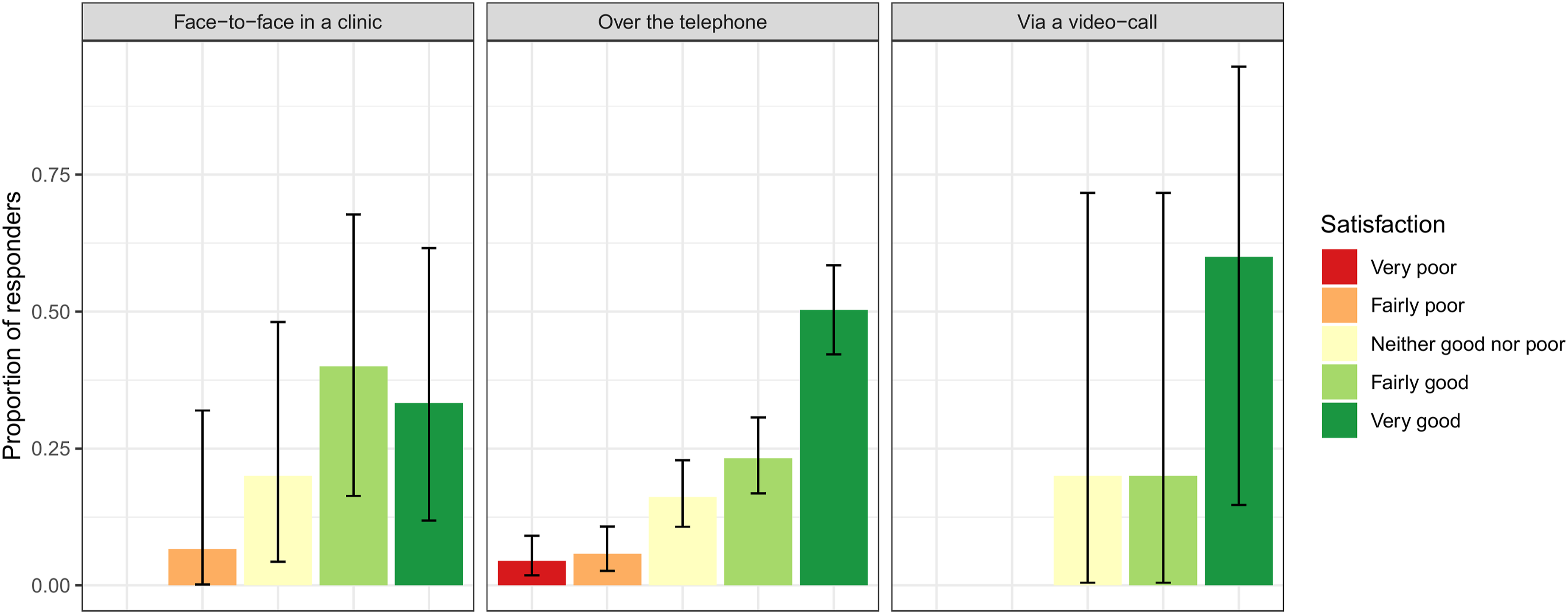
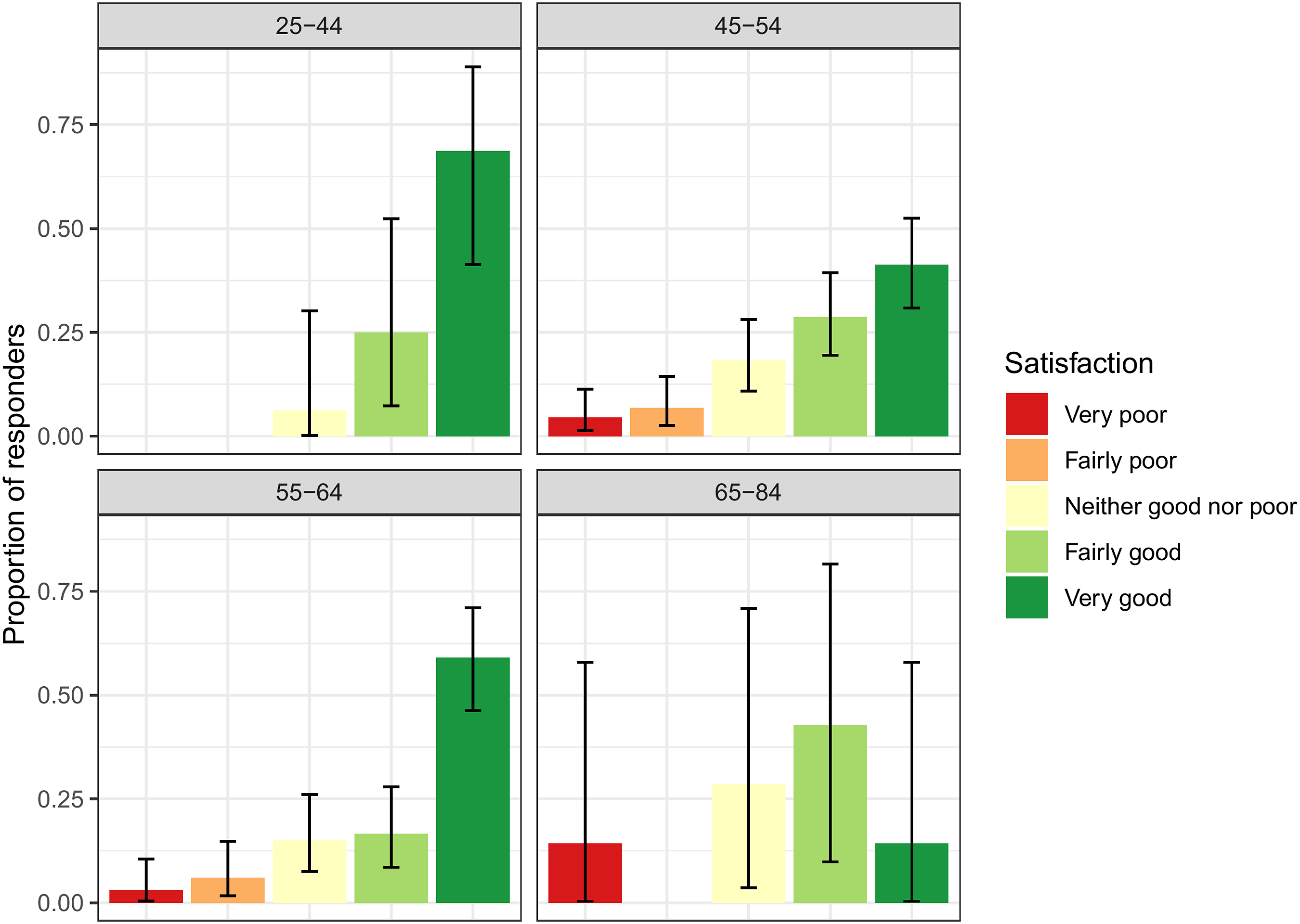
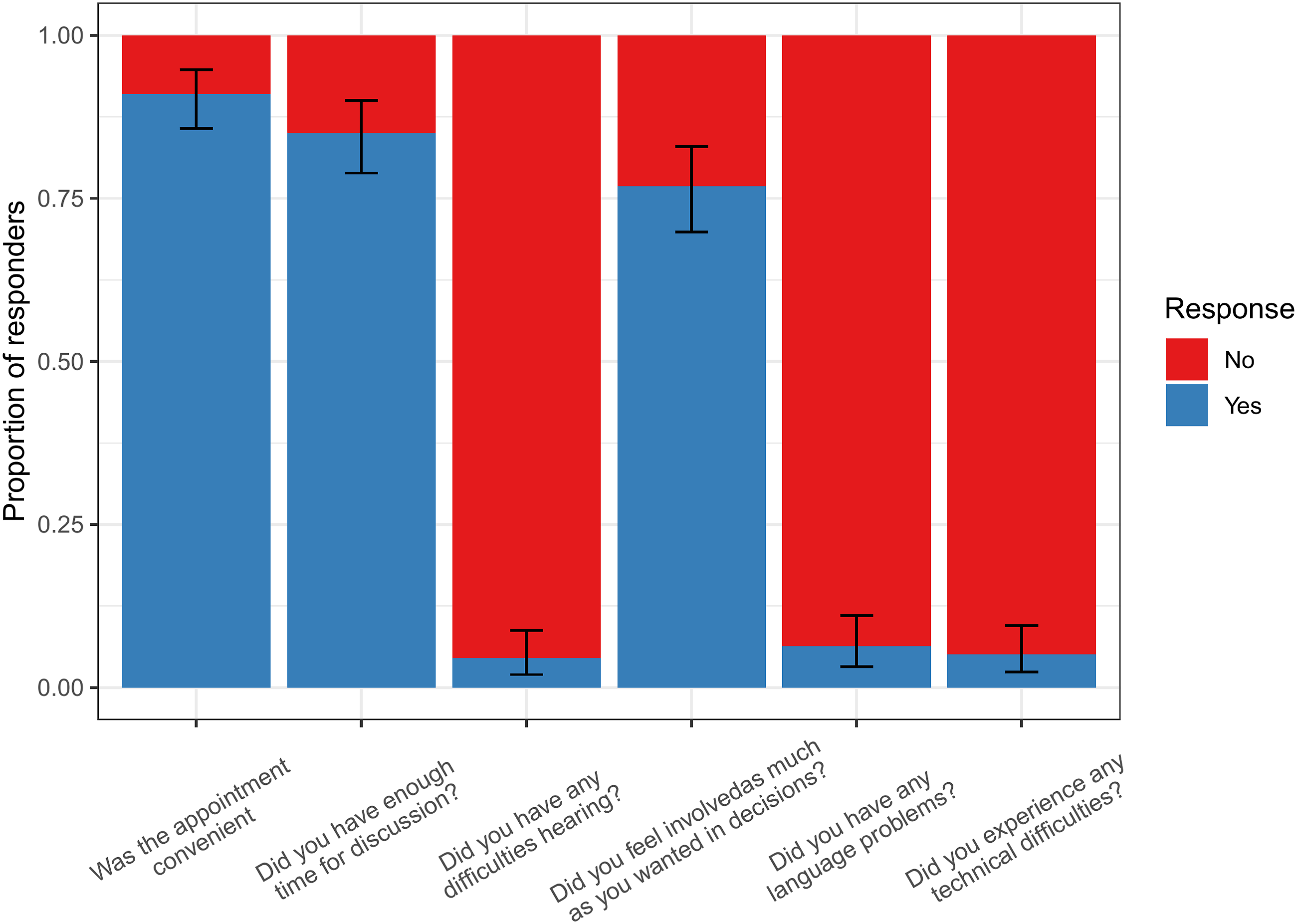
• Of the 114 patients who had attended a menopause clinic previously: • 73.9% (95% CI: 66.7-80.2) found their remote menopause consultation to be "Fairly good" or "Very good" (Figure 1). ∘ 48.2% (95% CI: 38.8–57.8) thought that their remote consultation was ‘Not as good’. ∘ 40.4% (95% CI: 31.2–50.0) thought it was no different ∘ 11.4% (95% CI: 6.2–18.7) thought it was better. • Most patients (89.9%; 95% CI: 84.5–93.9) felt that a choice between having a face-to-face or remote consultation should be offered. 7.9% (95% CI: 0.44–12.8) had no preference and 2.2% (95% CI: 0.6–5.6) did not think patients should be offered a choice. • Satisfaction appeared to be higher in NHS hospital or private clinics than GP review (see Figure 2). • There were too few responses to determine if experience differed between video call compared to telephone call consultations (see Figure 3). • Satisfaction appeared to be lower in older patients, particularly in patients aged 65–84, though it was difficult to determine a clear trend due to limited numbers of responders (see Figure 4). • For patients’ last menopause clinic appointment, 91.4% were remote (telephone/online) and 8.6% were face-to face (Table 2). In these appointments, only very few patients experienced technical, hearing or language difficulties (Figure 5), and 91% (95% CI: 85.7–94.7) found the appointment convenient. Proportion of patients responding to the question ‘How satisfied were you with your appointment experience’? in the patient survey. Proportion of patients responding to the question ‘How satisfied were you with your appointment experience’? in the patient survey, displayed by menopause clinic type. Proportion of patients responding to the question ‘How satisfied were you with your appointment experience’? in the patient survey, displayed by type of appointment. Proportion of patients responding to the question ‘How satisfied were you with your appointment experience’? in the patient survey, displayed by patient age. Proportion of patients responding to the question ‘How satisfied were you with your appointment experience’? in the patient survey, displayed by patient age.
Key qualitative results for patient survey
Patients’ free-text responses demonstrated positive and negative experience due to the type of consultation. A separate issue unrelated to consultation type was the quality of advice provided. Examples are given below.
Consultation issues
• Lack of access to GPs including inability to contact GP surgeries and get appointments. • Cancelling and rescheduling of appointments in primary and secondary care was frustrating and often poorly communicated. • Although some found telephone appointments convenient, others felt that face-to-face communication was preferable due to concerns about privacy and safety as physical examination could not take place for example, blood pressure and weight checks. “It was hard to direct the conversation without being face to face” “Telephone appointments are fine if you are at home……..The law doesn't make the employer give you time off for a telephone call whereas it does for an appointment. Plus, they’re not obliged to let you leave your desk or provide a private room….. I’m already worried about potentially having conversations about more intimate elements in the future.” “I prefer telephone appointments as you can be prepared with the questions you wanted to ask and it is so convenient as you don’t have to take time off work.” “The appointment mentioned didn't take place as I missed the consultant call. I tried to call to rebook the appointment this did not work either as I was told to leave a message and someone will get back to me. Since, I have not received any call yet.” “I was able to have a lengthy consultation over the phone on site which was useful. It would have been even better if I was able to have a video call and therefore able to see who I was speaking to.”
Medical advice
• GPs were considered to lack knowledge and skills in dealing with menopause problems. • Uncertainty about treatment plans and follow-up. “Feel no one interested in the issues I have due to menopause. I feel as if I just ‘have to get on with it’” “I have not had my menopause review, which was due last month, no contact from my GP surgery.” “All regular GPs need to have comprehensive menopause training”
Clinician survey
Characteristics of responders who completed the clinician survey.
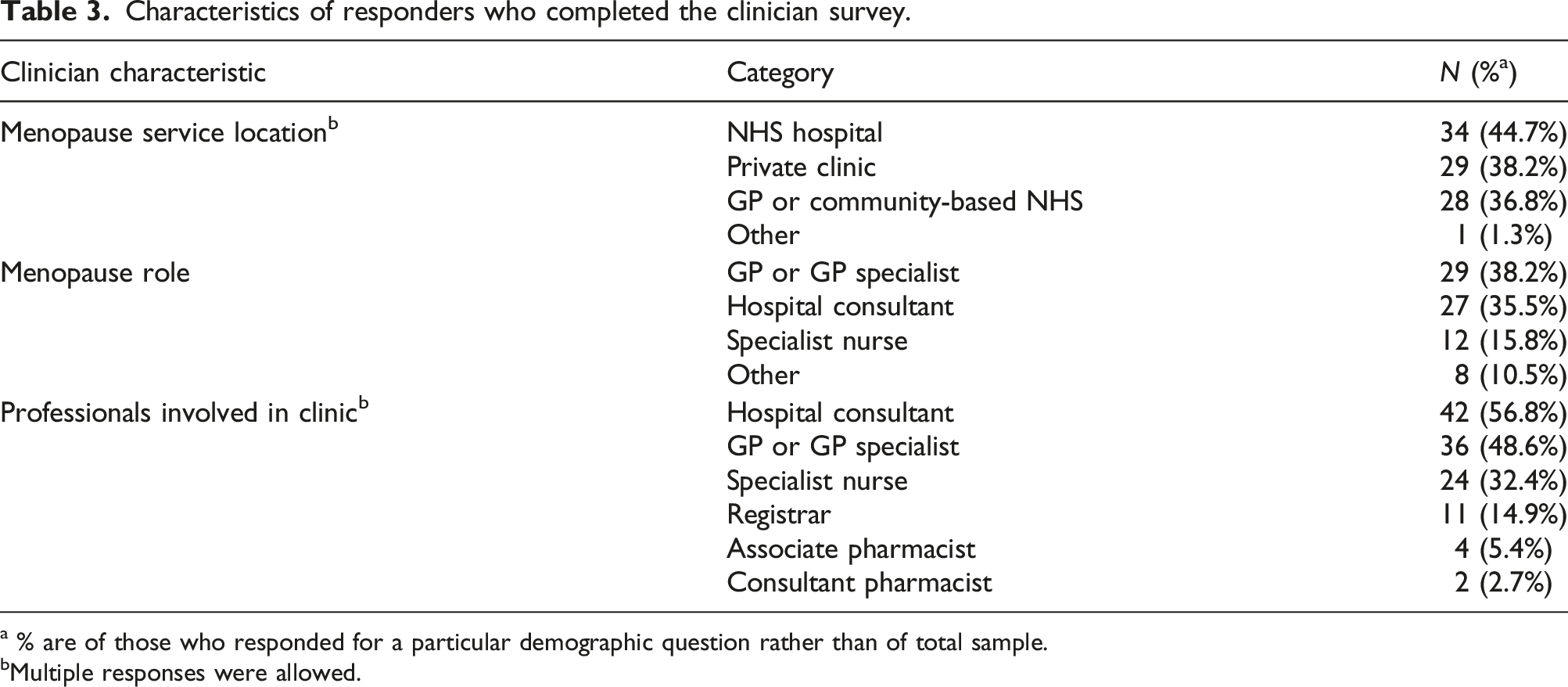
a % are of those who responded for a particular demographic question rather than of total sample.
bMultiple responses were allowed.
Key points for the clinician survey
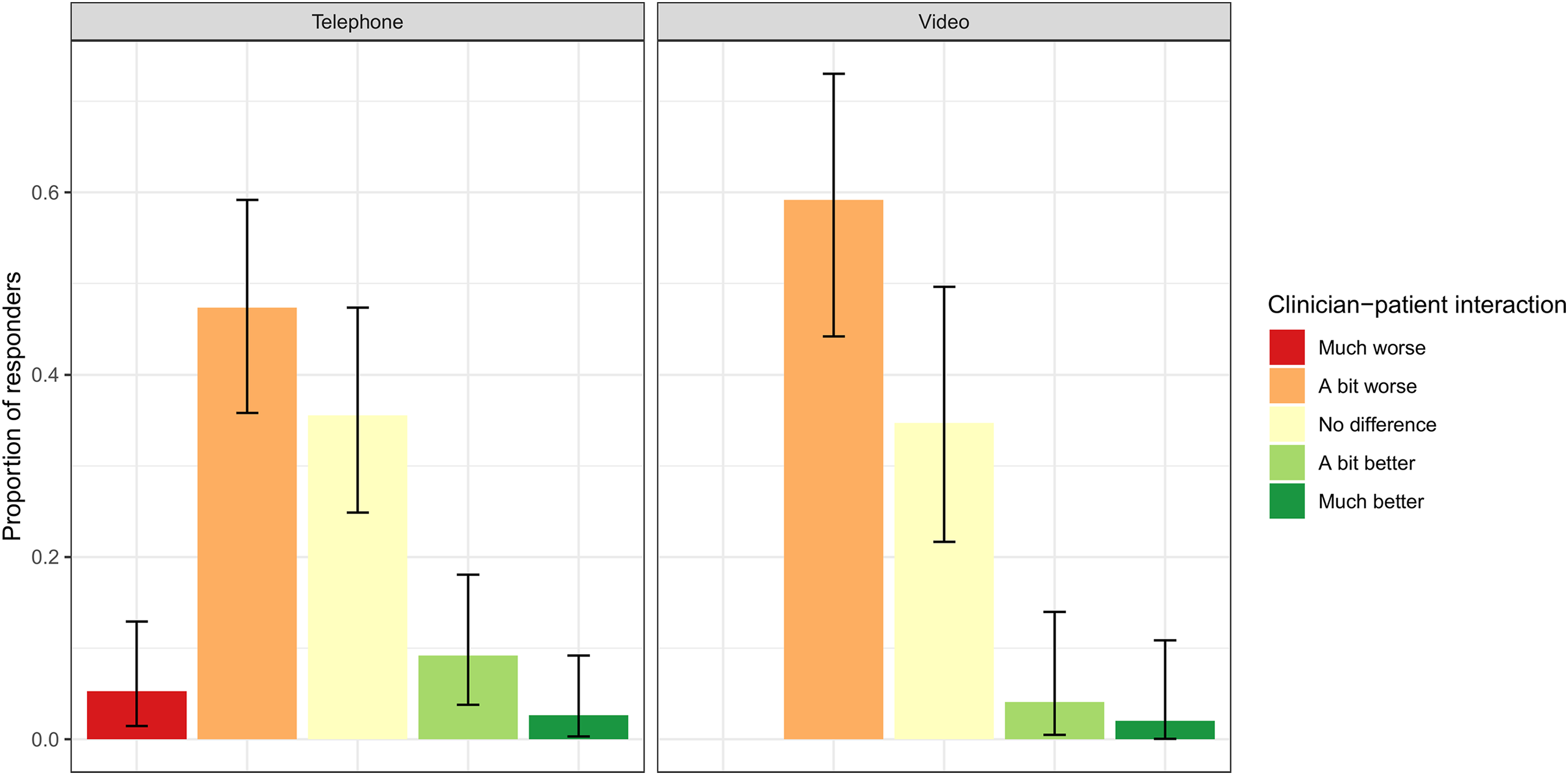
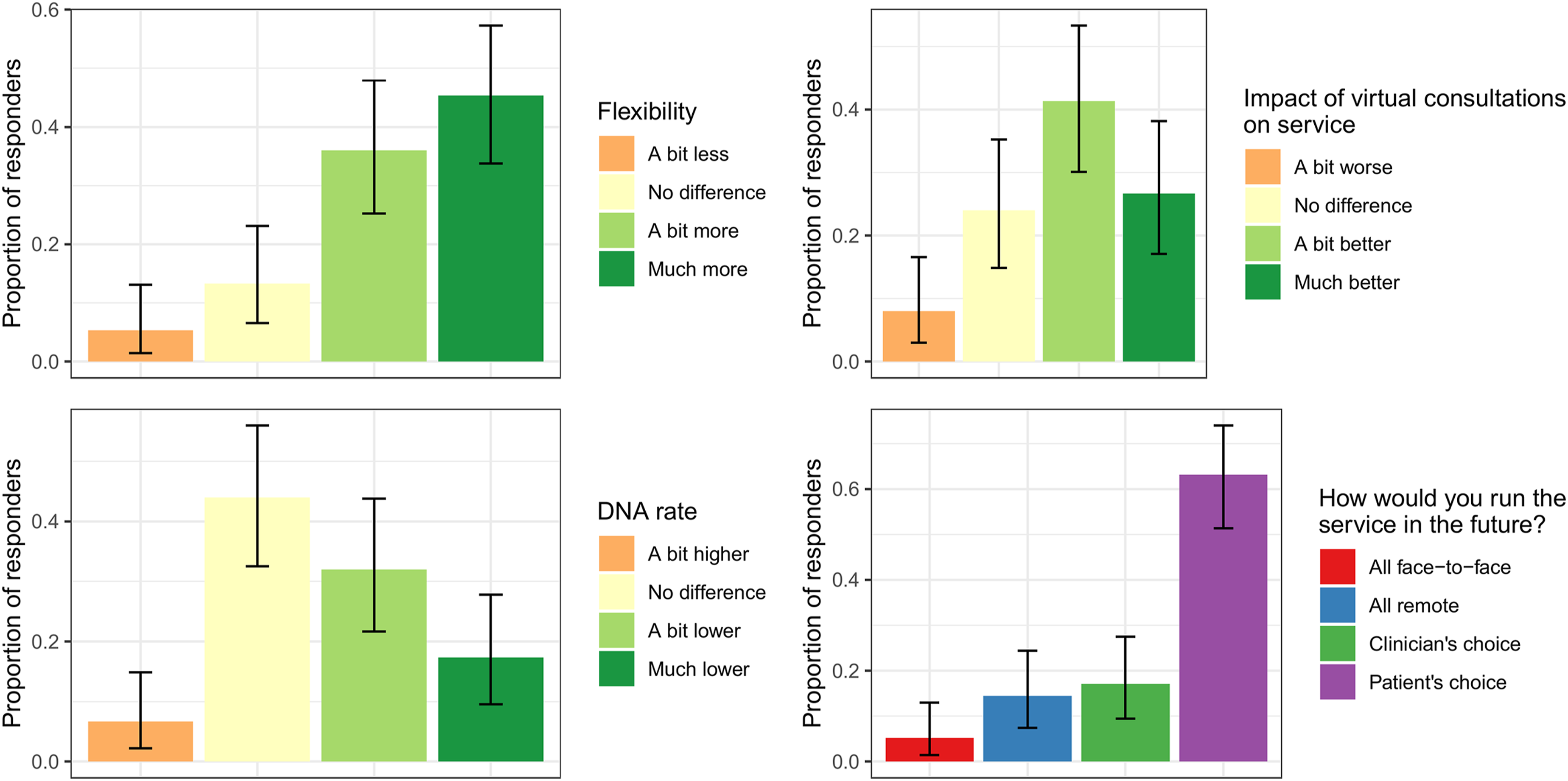
• Most clinicians conducted their remote consultations by telephone 68.4% (95% CI: 56.7–78.6), fewer used video consultations 11.8% (95% CI: 5.6–21.3). The remainder used both. • At the time of the survey (1st December 2020 to 10th February 2021), most had not reverted to face-to-face consultations 77.6% (95% CI: 66.6–86.4). • A small proportion of clinicians rescheduled a significant proportion of appointments as they considered remote consultation inappropriate 10.5% (95% CI: 4.7–19.7) due to a need for physical examination or patient language and hearing difficulties. • Most clinicians found patient interaction in virtual consultations either no different or a bit worse than face-to face consultations (Figure 6). • Virtual consultations were reported by most to provide more flexibility to face-to-face consultations (80.3%; 95% CI: 69.5–88.5, see Figure 6). • 48.7% (95% CI: 37.0–60.4) of clinicians believe that the DNA rate has decreased with virtual consultations (Figure 7 – bottom left panel). • Overall, 67% (95% CI: 55.4–77.5) of clinicians felt that virtual consultations have improved their service, whilst only 7.9% (95% CI: 3.0–16.4) feel they have worsened their service (Figure 7 – top right panel). • The majority of clinicians (63.2%; 95% CI: 51.3–73.9) would prefer to run either face-to-face or virtual consultations depending on patient choice (Figure 7 – bottom right panel). Proportion of clinician-patient interaction reported by clinicians in both telephone and video consultations. Proportion of responses from the clinician survey for four questions: the degree of flexibility and Did Not Attend (DNA) rate for virtual consultations versus face-to-face consultations (left panels), the impact of virtual consultations on the service (top right panel) and a choice of how clinicians would choose to run the service in the future (bottom right panel).
Discussion and conclusions
This is the only survey of menopause consultations before and during the UK Covid pandemic. It explores the patient and clinician perspective on the shift from almost exclusive face-to-face consultations to virtual via either telephone or video.
Whilst there are clear limitations to the design of the study with regards to the convenience sampling of participants and the way in which the surveys were distributed, it clearly identifies that there is at least a group of patients for whom remote consultations are acceptable and may even be preferable in terms of convenience. However, response to the survey is likely to be strongly correlated with patient experience/satisfaction, meaning that we cannot use this sample to reliably infer anything about the experience of non-responders, which may be very different to those surveyed here.
The outcome from the surveys demonstrate that while the majority of clinicians who responded found virtual consultations more flexible and convenient, patients who responded would prefer to be offered a choice between face-to-face and virtual consultations. Clinicians found that the interactions with patients on the whole were less optimal virtually compared to face to face. As the minority of respondents used video consultations, it was not possible to ascertain the satisfaction of these compared to telephone.
There is certainly scope for improvement with virtual consultations and the COVID-19 pandemic forced us into a rapid conversion to telephone or video consults we would not have undertaken in other circumstances. With good planning, virtual consulting could be optimised using video and waiting room technology so that patients can see their clinician and are reassured that their appointment has not been cancelled or forgotten about. As the vast majority of clinicians felt that the mode of consultation should be patient driven, a hybrid system should be adopted for menopause patients. In many cases, the first appointment may be more appropriate to be face to face so that a rapport is developed between the clinician and patient. Subsequent appointments could be offered as virtual depending on requirements for physical examination, language difficulties or special needs. Virtual appointments are more eco-friendly, avoiding lengthy commutes and cheaper for many patients avoiding parking and travel costs. This can also be cost saving for NHS hospital trusts who may need to achieve certain ‘green standards’ and avoid the cost of providing hospital transport for patients requiring additional assistance. The majority (66.7%) of participants were working, and therefore, a remote consultation is advantageous regarding minimising time away from the workplace.
The future design of menopause care services should be holistic and our findings suggest this should be a hybrid of face-to-face and virtual interactions. Post-reproductive health is a growing speciality, and although a national practicing standard exists, 3 further cross-discipline consensus, particularly around virtual consultations, would be invaluable.
Supplemental Material
Supplemental Material - An evaluation of menopause service delivery during the COVID-19 pandemic
Supplemental Material for An evaluation of menopause service delivery during the COVID-19 pandemic by Hugo Pedder, Lynne Robinson, Kathy Abernethy, Haitham Hamoda and Jo Marsden in Post Reproductive Health
Footnotes
Acknowledgements
Thanks to all members of the British Menopause Society’s Medical Advisory Council with their help in designing the survey questions.
Contributorship
Hugo Pedder: Conceptualization, Data curation, Analysis, Methodology, Software, Visualization, Writing (original draft), Writing (reviewing and editing). Lynne Robinson: Conceptualization, Analysis, Methodology, Writing (original draft), Writing (reviewing and editing). Kathy Abernethy: Conceptualization, Methodology, Writing (reviewing and editing). Haitham Hamoda: Conceptualization, Methodology, Writing (reviewing and editing). Jo Marsden: Conceptualization, Data curation, Analysis, Methodology, Writing (original draft), Writing (reviewing and editing).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: HP was supported by funding from the National Institute of Health and Social Care’s Guidelines Technical Support Unit and Bristol Technology Assessment Group.
Ethical Approval
No ethical approval was required. Responses were collected anonymously online and patients were informed that by completing the form they agreed that:
• The details provided can be held and used by The British Menopause Society for analysis.
• The anonymous information provided will be handled securely if it is used for any medical publications.
Guarantor
HP.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.