
Abstract
Background:
Understanding experiences of care for endometriosis is an important source of evidence for supporting the improvement of care quality for this long-term condition. Patient-reported experience measures are a key tool for providing this insight. However, in England, there is no national survey of experiences of endometriosis care, making it difficult to understand where care is working well and how it can be improved.
Objectives:
This scoping review aimed to identify and describe existing surveys globally for measuring patient experience of care for people with endometriosis.
Eligibility criteria:
The population of interest included people with endometriosis. The concept was questionnaires in any format (e.g. article or web-based) exploring the experience of care for endometriosis in the context of any care setting.
Sources of evidence:
PubMed and ProQuest databases were searched between August and September 2024.
Charting methods:
Information extracted included study information (e.g. article title, authors, year of publication, research objectives, country), inclusion/exclusion criteria (e.g. population, concept, context) and patient experience measure characteristics (e.g. name of experience measure, number of questions, domains of person-centred care, survey mode and contact approach, development process).
Results:
Out of the 209 articles screened, only seven surveys were identified for inclusion in the review. These surveys varied in context, number of items, domains of care, survey mode and contact approach. Most of the surveys focussed narrowly on one aspect of care, such as diagnosis or inpatient treatment, and three surveys included only two questions related to patient experience. Only one survey, the ENDOCARE Questionnaire, covered all eight Picker Principles of Person-Centred Care.
Conclusions:
With only a small number of surveys identified and only one capturing all core aspects of person-centred care, there are limited resources available for those wishing to understand and improve care quality for people with endometriosis.
Keywords
Introduction
Endometriosis is a condition where tissue similar to the lining of the womb is found elsewhere in the body. It can affect people of any age and is considered a long-term condition that, for many, can have a significant impact on quality of life. 1 It is thought that around 1.5 million women in the United Kingdom (UK) are living with endometriosis and are having to deal with symptoms such as chronic pain, nausea and heavy periods.2 –4 A recent systematic review looked at the evidence exploring the relationship between endometriosis and quality of life. Mental and physical wellbeing were both found to be significantly impacted by experiences of pain, infertility and stress. 5 Stigma is an issue for many and can significantly impact the mental health of those affected, as shown by a literature review that found people often experience invalidation and normalisation of their pain from an early age, leading to social exclusion and despair. 6 This is not helped by misinformation, which can contribute to a poor understanding of what constitutes good gynaecological health. A 2024 study analysed the evidence-based nature of content on Instagram about endometriosis. Much of the content was found to be inaccurate or only partially evidence-based, highlighting the risks this poses for health decisions and the importance of providing accurate, accessible information online. 7
Currently, there is no cure for endometriosis, with treatments aimed at reducing the severity of such symptoms and improving quality of life. 8 As of 2024, there are 63 specialist endometriosis centres in the UK. 9 These centres have a goal of supporting people with all grades of endometriosis by providing evidence-based care delivered by multi-disciplinary teams. However, studies show that many people encounter problems related to a lack of joined-up care for diagnosing, accessing, treating and managing endometriosis.
The implications of delays in diagnosing endometriosis, such as the potential for worsened symptoms, have been well explored. 10 The issue of diagnostic delays has also seen discussion by members of parliament in the UK with an inquiry by the All-Party Parliamentary Group on endometriosis finding that the average length to diagnosis from onset of symptoms was 8 years in the UK with three in five saying that they had visited their GP more than 10 times with symptoms prior to getting a diagnosis. 11
A need for holistic interdisciplinary care (i.e. care that brings together different services to meet a person’s full range of needs) was raised by participants in a study of treatment use and satisfaction in Australian women. The study saw 36% say they were dissatisfied with their care, with reasons given including barriers such as lack of access, stigma and medical professionals being perceived as uncaring. 12 The importance of holistic care is a message that has been repeated in work by the National Confidential Enquiry into Patient Outcome and Death which recommended that a formalised care pathway is needed in order for people to experience care that considers the whole person. 13
It has been recognised that to achieve a full picture of quality, one must look at safety, effectiveness of care and experience. 14 It is not uncommon for patient-reported outcome measures (PROMs) to be used for collecting information on health outcomes and patients’ perspectives on their condition in endometriosis care. 15 Patient-reported experience measures (PREMs) are also a key tool for providing insight on quality from the patient perspective. 16 Designed with the goal of measuring what matters to people, PREMs are able to deliver actionable insights for quality improvement, service evaluation and assessment, and for supporting patient choice. 17 PREMs are typically structured around core domains of person-centred care, such as the Picker Principles of Person-Centred Care. 18
There is a wide range of PREMs available for use across different care settings and for different conditions. In England (one of the four countries that constitute the UK), a number of these surveys are rolled out as part of a national programme owned by the independent regulator of health and social care in England, the Care Quality Commission. However, in England, the absence of a national survey on experiences of endometriosis care makes it difficult to identify gaps in service provision, understand patient needs and highlight areas where care is effective. This lack of comprehensive data hinders the evaluation of healthcare services and limits the ability of NHS providers—such as those in primary and secondary care—to improve care at local, regional and national levels.
The objective of this scoping review was therefore to identify and describe existing surveys globally for measuring patient experience of care for people with endometriosis.
Methods
A preliminary search of PubMed was conducted in August 2024 to see if any current scoping or systematic reviews on this topic were identified. No reviews were found.
The scoping review was conducted in accordance with the Joanna Briggs Institute methodology for scoping reviews. 19 The protocol for this review was published on the Open Science Framework (https://osf.io/fnyjm). A PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) diagram presents the search strategy in a flowchart (see Figure 1). A PRISMA-ScR checklist has been completed and submitted as Supplemental Material. The reporting of this study conforms to the PRISMA-ScR guidelines. 20

PRISMA flow chart of search.
Eligibility criteria
The population of interest included people with endometriosis. The concept was questionnaires exploring the experience of care for endometriosis in the context of any care setting.
Questionnaires in any format (e.g. paper-based or web-based) were in scope; however, qualitative surveys using only open-ended questions (or free text questions) were excluded. Experience surveys designed for completion by people with endometriosis with or without support were included.
Experience surveys conducted in a healthcare setting that do not measure patient experience, such as healthcare staff experience, were excluded. Surveys purely focussed on health-related outcomes or quality of life (such as PROMs) were excluded. Surveys that only include questions that focus on satisfaction or recommendation (such as the Net Promotor Score or other similar overall likelihood to recommend questions) rather than experience were excluded as they do not produce actionable insights for quality improvement. Finally, studies that included the use of an experience survey, even if the main outcome was not developing or validating the measure, were included to ensure the breadth of the review.
Search strategy
An initial limited search of PubMed and ProQuest was undertaken to identify articles. An analysis of the words contained in the title, abstract and index terms of the retrieved articles followed. A second search using all identified keywords was then undertaken across the two databases. A final search was carried out using the reference lists of the articles selected for full-text review. The searches took place in August and September 2024.
Studies published in peer-reviewed journals were included. We included articles published over the past 20 years (up to 30 September 2024) to ensure relevancy to current practice. Articles needed to be published in the English language.
The search was carried out using the terms “endometriosis” AND (“experience” OR “satisfaction”) AND (“survey” OR “tool” OR “measure” OR “questionnaire” OR “inventory” OR “short form” OR “instrument”). No Medical Subject Headings terms were applied to the search. The search fields included title and abstract.
Following the search, all identified citations were uploaded into Rayyan software (developed by Rayyan Software Inc.) and duplicates were removed. Titles and abstracts were independently screened against the inclusion criteria by two reviewers. Potentially relevant sources were retrieved as full-text articles and again screened by two reviewers. Any disagreements were discussed until a consensus was achieved. Reviewer 1 is a researcher with 17 years’ experience carrying out health care research and quality improvement, including involvement in systematic and scoping reviews. Reviewer 2 has 17 years’ experience in social research methods, both quantitative and qualitative, including the design and implementation of cross-sectional and longitudinal surveys. Neither reviewer reported conflicts of interest related to this review topic.
Data extraction
Data from full-text articles that met the prespecified inclusion criteria were extracted in table form by a member of the study team. A selected sample of this extracted data was then reviewed and verified against the original articles by a second member of the team to ensure accuracy and completeness. Data items extracted included study information (e.g. article title, authors, year of publication, research objectives, research question, country), inclusion/exclusion criteria (e.g. population, concept, context) and patient experience measure characteristics (e.g. name of experience measure, number of questions in survey, domains of person-centred care explored, survey mode and contact approach, development process). Authors of included articles were contacted to request missing or supplementary data where required.
Data synthesis
A narrative synthesis of the results was carried out to answer the objectives. Narrative methods of synthesis are often used where meta-analysis is not appropriate, as was the case for this study. 21 This was aided by the use of tabulation and visual mapping, which allowed for gaps in coverage to be recognised and discussed. Thematic summaries were used to create different groups based on study information and measure characteristics. Content analysis was used to synthesise data into the pre-determined domains of person-centred care.
Results
After duplicates were removed, 290 articles were identified through an electronic data search. Screening of titles and abstracts resulted in the identification of 15 articles that met the criteria for full review. A full review resulted in eight of these articles being excluded, leaving seven as included. Reasons for exclusion included surveys being duplicates of already included measures, a questionnaire being qualitative in nature, a focus on treatment satisfaction rather than experience and a focus on overall satisfaction rather than experience.
Table 1 details the key characteristics of the final seven articles included for review.22 –28
Key study characteristics.
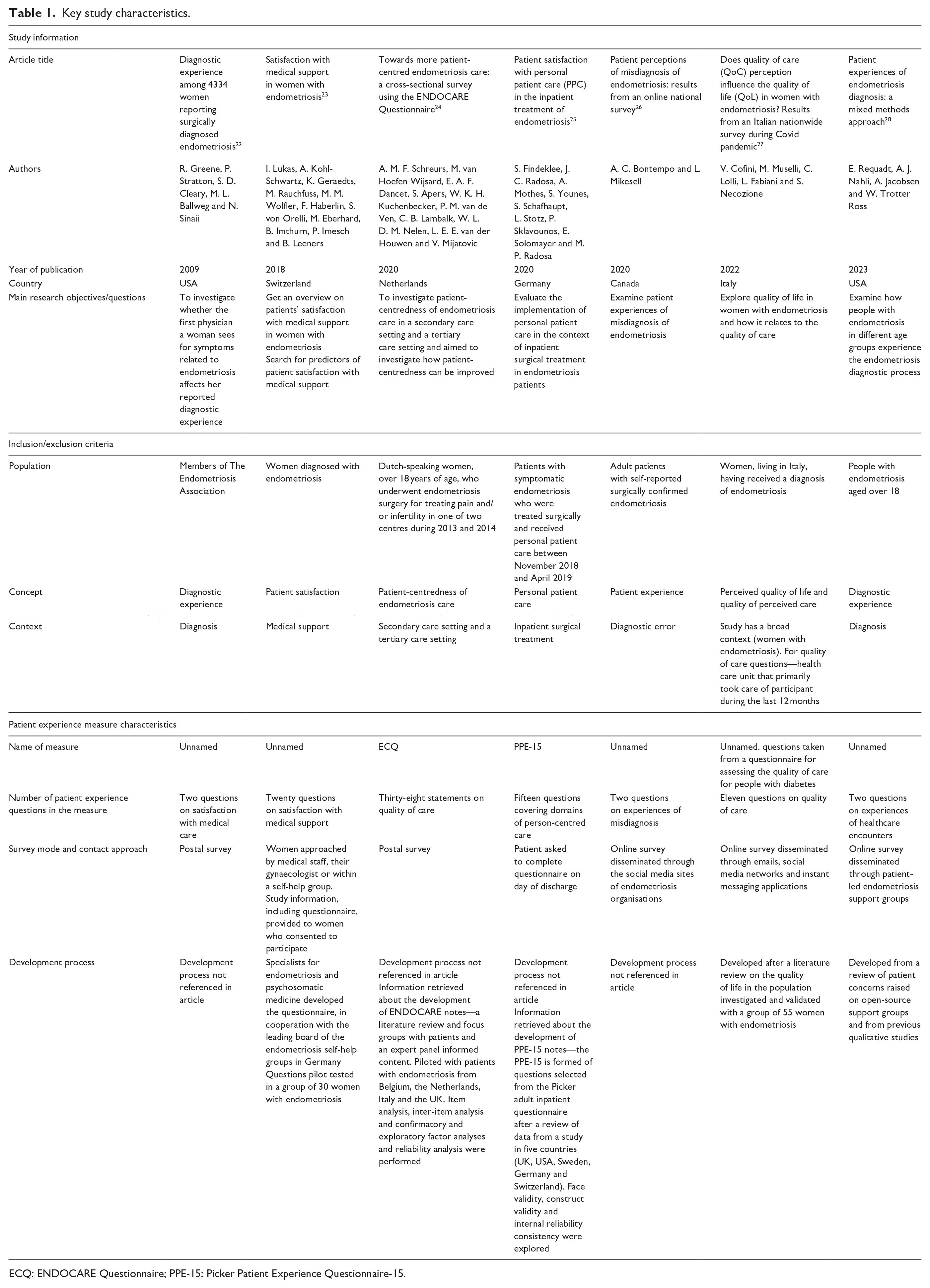
ECQ: ENDOCARE Questionnaire; PPE-15: Picker Patient Experience Questionnaire-15.
International scope of studies
The studies were conducted in six countries. Two of the articles originated from the United States of America and one from Canada.22,26,28 The remaining four articles originated from different countries in Europe (Germany, Italy, Netherlands and Switzerland).23 –25,27
Description of the surveys
All of the articles describing the seven surveys included for review were published between 2009 and 2023, with the majority (n = 6) being published between 2020 and 2024. Of the seven surveys, five were developed specifically for exploring endometriosis.22–24,26,28 Two of these five surveys had multiple questions (n = 20 and n = 38) exploring patient experience, with three only including a small subset of experience questions (n = 2 in each case) in wider surveys about endometriosis. The remaining two surveys were originally developed for populations other than people with endometriosis (one was designed for people receiving diabetes care and one focussed on inpatient care) that were repurposed for the included studies.25,27
Looking at context, three of the seven surveys focussed on diagnostic experience, though in each case, this was limited to a small subset of questions (n = 2) specifically addressing experience.22,26,28 One survey focussed on the general quality of care. 27 The remaining three surveys focussed on the different contexts of medical support, inpatient surgical treatment and secondary and tertiary care.23 –25
Coverage of key domains of person-centred care
The surveys were examined to see how questions mapped to the eight key domains of person-centred care as recognised by the Picker Principles of Person-Centred Care. Table 2 shows this mapping.
Picker principles of person-centred care covered by each survey.

Only one of the surveys, the ENDOCARE Questionnaire (ECQ), covered all eight domains. 24 The Picker Patient Experience Questionnaire was the next best in terms of coverage, with six domains being explored. 25 Three of the seven surveys (those with two experience questions included) only explored the domain of effective treatment by trusted professionals.22,23,26 Effective treatment by trusted professionals was also the most common domain to be covered, appearing in five of the seven surveys. The least common domains, only appearing in two surveys, were fast access to reliable healthcare advice and involvement and support for family and carers.
All identified questions could be mapped to at least one of the Picker Principles of Person-Centred Care.
Mode of administration
Three of the seven surveys were implemented using an online survey approach with dissemination via networks (such as patient-led endometriosis support groups and sites of endometriosis organisations) and social media.26 –28 Two of the surveys were disseminated at patient interaction with health and support group services (e.g. on discharge from inpatient treatment).23,25 A postal survey approach (with questionnaire being mailed to the recipient’s home address) was used with two of the surveys.22,24
Development process
Articles were reviewed for detail on the survey development process. Three of the articles provided information on development with techniques such as literature review, stakeholder consultation, qualitative research with people with endometriosis and pilot testing being used to inform question content.23,27,28 The four remaining articles did not include any detail on development. However, for two of these articles, supplementary information accessed revealed that development included similar activities to those noted above.24,25
Discussion
The purpose of this scoping review was to identify and describe existing surveys for measuring patient experience of care for people with endometriosis. We found a small selection of seven surveys that met this criterion, highlighting that there are limited resources available for those wishing to understand and improve care quality for people with endometriosis. The lack of widely used tools restricts the capacity to make evidence-based improvements and can lead to issues of exclusion and inequity where voices, particularly those from marginalised groups, remain unheard.
The seven surveys identified varied in context, number of items and the domains of care covered, survey mode and contact approach. This heterogeneity presents challenges for establishing a standardised understanding of patient experience in endometriosis care. It also underscores the need for greater alignment in the development of future surveys to support the identification of best practices and service improvement efforts.
With six of the articles reviewed published between 2020 and 2024, we see that over the last 5 years, there has been a greater focus on understanding experiences of care for this population. This trend recognises the value of patient-reported experiences, particularly in the context of global events, such as the COVID-19 pandemic, that can cause widespread disruptions to healthcare. For people with endometriosis, this often meant delayed access to necessary care and treatments, heightening their health challenges. This is evident from survey research conducted during the pandemic, which explored the effects of the pandemic on quality of life. Worsening mental and physical health was found to be linked to impaired medical care. 29 Pandemic-related stress was also found to be associated with poorer outcomes among women with endometriosis. 30 During such times, collecting data on patient experiences becomes especially important for informing efforts to maintain or improve care quality amid evolving challenges.
The included articles stem from only a small number of countries, predominantly from Europe, with developing countries not represented, suggesting that there is work to do to ensure that the value of understanding and measuring experiences of endometriosis care is seen globally and that disparities in care can be identified. However, it should also be noted that even where there is awareness of the value of person-centred care, developing countries can often face broader challenges with the implementation of patient experience measurement, such as limited resources and funding.
With three of the seven surveys making use of support groups, charities and social media to reach people with endometriosis, we see the importance of such networks for engagement in addition to important services such as raising awareness, advocacy, emotional support and sharing of advice. Research exploring online support group use by people with endometriosis found that being able to share experiences and hearing the experiences of others was a commonly cited benefit of support groups. 31 In the absence of any national endometriosis experience surveys carried out by regulators or commissioners of healthcare services, support groups and charities are important resources for listening to people and communities. Although it is important to note that the views of support group members, who may be more active in their care, may not be representative of all people with endometriosis. Furthermore, many support groups and charities operate with limited funding and capacity, making heavy reliance on them as primary sources of feedback unsustainable. This highlights the need for commissioner or regulator funded, systematic efforts to collect and respond to patient experience data.
Recent updates to the endometriosis guidelines by the National Institute for Health and Care Excellence in the UK and the European Society of Human Reproduction and Embryology (ESHRE) have looked to strengthen recommendations on diagnosis and referral.32,33 ESHRE themselves note in their guidance that high-quality data is required in some areas in order to develop further evidence-based recommendations. It is therefore perhaps unsurprising that three of the seven surveys identified focussed on the diagnostic experience, given the widespread recognition that diagnosis is often delayed and can significantly impact quality of life. However, in each of these surveys, the focus on diagnostic experience was limited to a small subset of questions (n = 2), which may not adequately capture the full range of factors involved in someone’s diagnostic journey. Important components—such as experiences of symptom recognition, interactions with healthcare professionals, time to diagnosis and the quality of information provided—may therefore be underrepresented. This type of information is important for supporting efforts to improve the process of diagnosing to help can lead to earlier detection and more timely symptom management and treatment.
Coverage of the person-centred care domain of effective treatment by trusted professionals by five of the seven surveys demonstrates the importance given to having positive therapeutic relationships with healthcare staff. Effective treatment by trusted professionals supports the delivery of care for physical symptoms as well as the emotional impact of endometriosis. These relationships should inspire a sense of confidence and trust, but evidence suggests that it is often the case that people can feel dismissed and ignored. 13 The gap between expected and experienced care underlines the importance of robust tools to measure patient experience in a way that captures both clinical and relational dimensions of person-centred care.
Whilst it is clear that effective treatment by trusted professionals is a priority, it is important that the quality of care across all core domains of person-centred care is adequately captured by patient experience measures, allowing a comprehensive picture to be developed of experiences across the complete patient pathway and for a complete understanding of patients’ needs, preferences and values. Only one of the seven surveys included in this review, the ECQ, meets this ambition with a question set that covers each of the Picker Principles of Person-Centred Care and that was developed specifically for understanding experiences of endometriosis. 24 Details of the development of the ECQ, which included qualitative research and a pilot survey with people with endometriosis, have been published and the measure presents itself as a good starting point for those wishing to carry out patient experience measurement. 34 Whilst it is acknowledged that the scope and objectives of surveys included in this review vary, survey authors should give consideration to incorporating questions that address each of the key domains of person-centred care, as this will support the generation of meaningful data that can inform service development.
Touching upon the limitations of this study, the search strategy only included studies that referenced experience or satisfaction, and so others exploring patient experience, which did not include these terms, may have been missed. Only studies published in English were included. No grey literature was included in this review, and so there may be surveys used by organisations that this review did not pick up.
This scoping review found only a small number of surveys measuring experiences of endometriosis care, with variation and limited coverage of key aspects. Future efforts should prioritise the development or adaptation of patient experience surveys that reflect the full care journey, so that the voices of people with endometriosis are meaningfully heard and acted upon.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251358042 – Supplemental material for Patient experience surveys for endometriosis care: A scoping review
Supplemental material, sj-docx-1-whe-10.1177_17455057251358042 for Patient experience surveys for endometriosis care: A scoping review by Jenny King and Caroline Killpack in Women’s Health
Footnotes
Author contributions
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.