
Abstract
The concept of quality has moved to the top of the international healthcare agenda in the past 30 years. This has been driven by a growing awareness of the scale of variation in patient outcomes, influenced by both the paucity of and consistency in implementation of evidence-based actions or interventions performed during the delivery of patient care. Concurrently there has been growing interest on the part of healthcare professionals to use a wider range of knowledge and available techniques, from outside of medicine, to continuously improve standards of safe and effective patient care. This is the first in a series of three articles introducing Quality Improvement (QI) methodology and supporting concepts to multidisciplinary teams working in Urology departments in the United Kingdom. We start, in this article, by providing an overview of key QI principles and their industrial roots; we position QI in the context of other approaches to improvement, such as audit, and we outline the key organisations and infrastructure supporting QI work on the ground.
What is quality in healthcare?
What constitutes ‘quality’ in the context of healthcare provision is likely very different depending on who you ask. For patients it might relate to how quickly an appointment can be secured, the ease of communication or the outcome of a procedure; for clinicians perhaps it has more to do with access to state of the art equipment, dependable resources and decreasing risk; for the manager or commissioner, improving patient flow and the meeting of performance targets may be a greater consideration.
Within healthcare there is no universally accepted definition of ‘quality’, but those commonly used pick up on this multi-dimensionality. The following popular definition, from the US Institute of Medicine and also used by the World Health Organization, describes quality as ‘the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge’.1,2 It identifies six dimensions of quality, stating that healthcare must be:
Safe: Minimising risk and harm to service users, including avoiding preventable injuries and reducing medical errors;
Effective: Providing services based on scientific knowledge and evidence-based guidelines;
Patient-centred: Providing care that responds to individual preferences, needs and values;
Timely: Reducing (sometimes harmful) delays in providing and receiving health care;
Efficient: Maximising the benefit of available resources and avoiding waste;
Equitable: Care that does not differ in quality according to personal characteristics such as gender, race, ethnicity, geographical location or socioeconomic status.
These dimensions are a product of both the wider health systems environment and the actions of providers and individuals working within the system. In the United Kingdom’s National Health Service (NHS), they underpin a shared vision and commitment to delivering quality care on behalf of multiple stakeholders within the system, each with a different function, including commissioners, staff, providers, regulators, research and innovation partners and patients and communities. 3 (The specific roles of some of these bodies are discussed further later on.)
QI: definition and background
Alongside the recognition of what constitutes high-quality care has been the quest to understand how best to go about improving quality. We now know that to make the best use of available resources, to prevent the occurrence and recurrence of system failures, and to achieve excellence in care delivery requires continuous improvement of healthcare processes in a manner that is systematic and sustainable.4,5
QI approaches were introduced into healthcare following several decades of development and applications in other industries – most notably the manufacturing industry. QI approaches used in healthcare today date back almost 100 years and are often identified with Walter Shewhart, William Edwards Deming and Joseph Juran (and more latterly in healthcare Don Berwick), who all worked to quality assure industrial manufacturing processes through the use of standardised tools and measurements6–15 (Box 1).
Pioneers of Quality Improvement.

QI: Quality Improvement.
These practical approaches to improvement coalesced around the turn of the 21st century into what is now termed ‘Improvement Science’ in healthcare, which has emerged as a burgeoning science in its own right. While the terms QI and Improvement Science are often used interchangeably, there is an important distinction between the two. QI refers to practical efforts to make changes to healthcare configuration and delivery, usually in the form of discrete QI projects utilising QI tools and methodologies, whereas Improvement Science is the broader scientific discipline sitting behind it. Improvement science aims to inform QI practice by finding out how to improve and make changes in the most effective way. It is about systematically examining the methods and factors that best work to facilitate QI. 16 In the rest of this article, and indeed the broader series of papers, we focus on the practice of QI as opposed to the wider field of Improvement Science per se.
QI can be defined as ‘better patient experience and outcomes achieved through changing provider behavior and organization through using systematic change methods and strategies’. 17 This definition captures the core features of QI which are the combination of a ‘change’ (improvement), a ‘method’ (a systematic approach aided by appropriate tools) and a ‘context’ (the environment in which the improvement is made) in order to achieve better ‘outcomes’. 18 Importantly, ‘better outcomes’ might not refer to patient outcomes alone, but to additional factors related to high-quality care, such as system performance and professional development (learning). 4 Alternative definitions of QI propose that it should not only refer to the practice of making changes on the ground, but to a general outlook and ambition to continually strive to make things better for patients. 19 Practically, in most hospitals in high-income countries globally, and certainly in all UK hospitals, this ambition translates into the presence of QI departments and relevant expertise, which can be used in-house to help frontline clinicians improve their services.
Underlying QI principles
A number of key principles underlie QI approaches in healthcare which are listed here and elaborated on in subsequent articles of this series:
An iterative approach: The concept of improvement through iterative cycles is the basis of the structured QI approaches used in healthcare today. Such cycles (most commonly referred to as ‘Plan, Do, Study, Act’, or PDSA cycles) are characterised by a continual process of planning, testing, studying and learning by comparing results to an expected outcome, and then adapting the hypotheses and re-testing these again. What results is a process of ‘fine-tuning’ (adopting, adapting and discarding of improvement efforts) with consecutive iterations of the cycle to bring you closer to a desired goal.7,20
Using data to drive improvement: Reliable, valid and sequential data collection processes should be in place in order to provide baseline measurements of care quality and their changes over time. This helps to drive decision-making by capturing the impact of interventions and understanding variation in processes and outcomes to separate out improvement, or deterioration, from the expected level of performance variation.6,18
Empowerment and involvement of service users, frontline staff and hospital management: Evidence shows that QI works best and is more likely to be sustained if it is done with and not to healthcare providers and users. Thus, staff and patients should be empowered and equipped to contribute towards improvement efforts from a very early stage in its development. Engagement allows these stakeholders to identify the metrics that are relevant to them and to offer their tacit knowledge regarding aspects of the services that require redevelopment or substantial change. It also helps to foster a shared commitment and enthusiasm for changes to services.18,21–24 All of this should be supported by the involvement and alignment of hospital management in QI strategy and delivery, which is an important determinant in the ultimate success of QI interventions. 25
A deep understanding of systems and processes: One cannot improve what one does not understand. Therefore, part of the improvement process should involve a detailed analysis of the care pathways, processes and procedures that are to be improved. This is often done through techniques such as process mapping, which provide a detailed description of an entire care pathway (or more discrete processes) by charting each step. This enables identification of which steps add value, and where there may be waste or delay; it enriches understanding of processes and systems and their interfaces between different areas, teams and organisations; and it helps to involve staff and bring them on board with the improvement journey.26,27
Scale up and spread with adaptation to context: What works in one setting does not readily transfer to other settings, suggesting that many improvements are context-dependent. Key to successful diffusion of improvement is the adaptation of interventions to new environments, patient and staff groups, available resources and even personal preferences of healthcare providers in surrounding areas, again using an iterative testing approach. 28 A number of implementation frameworks are available to guide the process of introducing and adapting interventions in healthcare settings.
An emphasis on reliability: Interventions should not be ‘one-off’ improvements but should aim to ensure that care is consistent over time – hence of high reliability. Ensuring reliability mitigates against waste and defects in the system and reduces error and harm. 29
Why QI is a valuable addition to clinical audit, research and other approaches to improvement
To understand the value of QI it is useful to compare it to similar approaches that seek to introduce or evaluate improvement in healthcare, most commonly clinical audit, research, service evaluation and clinical transformation (Figure 1). In reality, these approaches have many overlaps but also some very important differences.
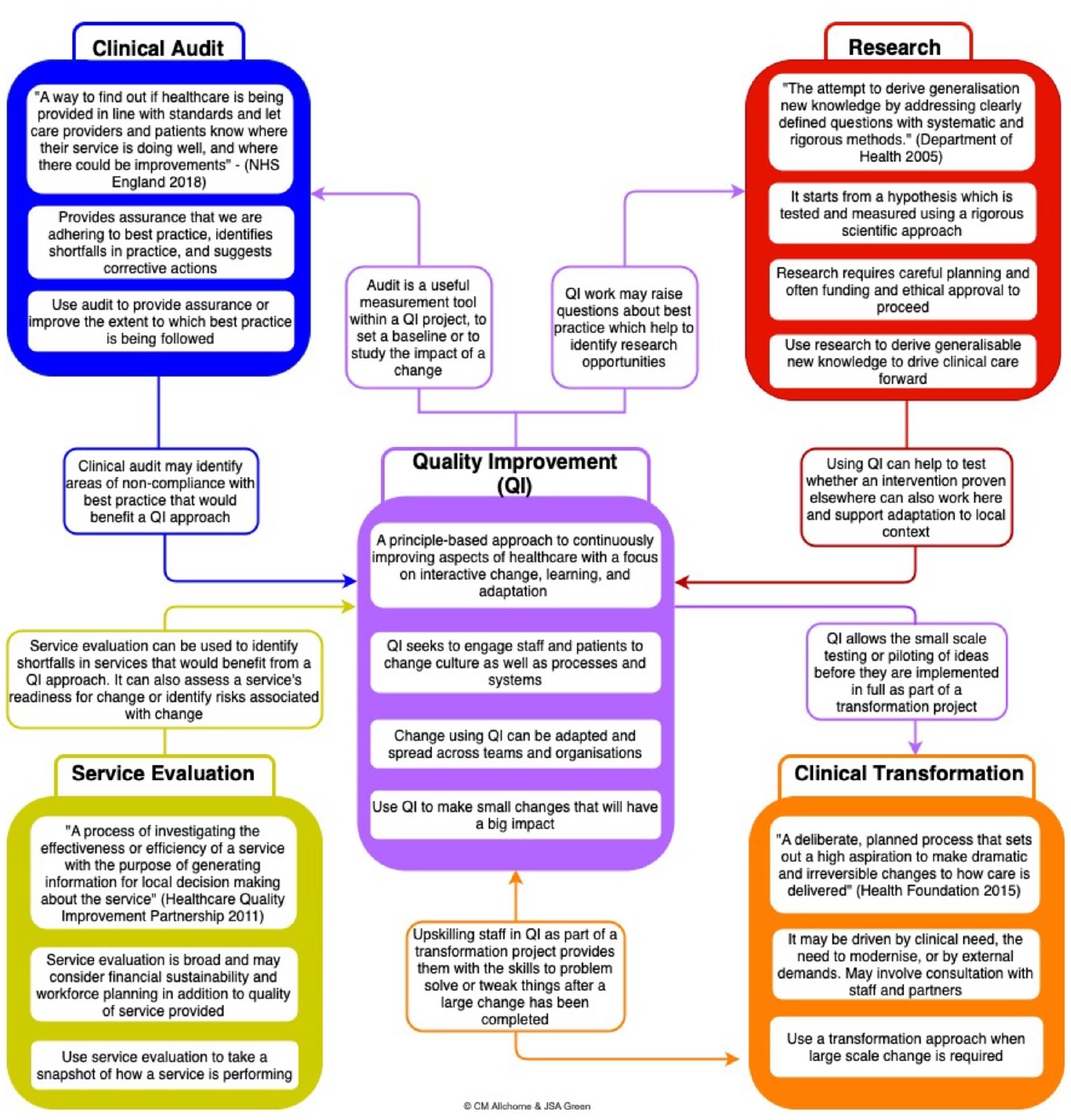
The intersection between Quality Improvement, Audit, Research, Service Evaluation and Clinical Transformation.
QI and clinical audit: Clinical audit can be seen as an approach to establish the accepted or baseline performance of health services, that is., it measures current practice against a defined (desired) standard, to let care providers and patients know where their service is doing well, and where there could be improvements. 30 Audit forms part of quality assurance and clinical governance, which aim to safeguard high-quality clinical care for patients and may take place at a local level or at a national level (e.g. the national clinical audit programme in the NHS). Given that the outcome of an audit can highlight where improvements are needed, it is often the first step in the QI process. Equally, if used iteratively, interspersed with improvement action, a ‘clinical audit cycle’ can be used as part of a QI project as an assurance tool to help track whether improvements have been sustained over time. However, there are some important distinctions to draw between audit and QI. First, many audits end at the data collection stage and fail to lead to improvement interventions. This might be because the audit is only required as an assurance function, but also because it is comparatively easy to collect data, but using that data to drive changes in behaviour is far more resource-intensive and challenging. Audit also frequently fails to engage frontline staff and service users in the same way as QI – clinical staff might be aware that an audit is happening but may not be part of a broader improvement effort. In addition, audit is often used to focus on clinical outcomes or the management of particular conditions, while QI can focus on any part of service delivery taking a more cross-cutting view to identify systemic issues across care pathways. Therefore, while one round of audit can give a cross section of performance, it is best used as part of a QI approach, to help understand in a more dynamic way what did and did not lead to an improvement.20,31
QI and research: Research is about creating new generalisable knowledge by addressing clearly defined questions with systematic and rigorous methods. This also has similarities and differences to QI. While both QI and research are characterised by the use of systematic and consistent methodology, QI does not seek to create generalisable knowledge, rather it generates several lessons as to what actually works and does not work and why in the specific area you want to improve. In QI, the measurement framework is not about pre- and post-intervention (which is commonly the case in research), but rather about continuously measuring the metric of interest that you want to improve and coming up with not just one intervention but multiple interventions based on learning from prior ‘PDSA’ cycles to generate sustained improvement. In addition, in QI the goal is to improve rather than to prove, which means the data can be ‘just good enough’ rather than perfect; statistical significance is not the focus but rather data are aggregated for time-series analysis to understand meaningful trends and patterns in the data. What is more, testing interventions via large-scale research projects such as feasibility studies and randomised controlled trials (RCTs) usually requires external funding and associated timely application processes with no guarantee of success, followed by further time-consuming processes such as ethical approval and peer review publication. QI projects in comparison can get off the ground very quickly at significantly less cost and administrative load (although dissemination is encouraged which may include publication of results).20,32,33
It should be noted that Improvement Science (i.e. the scientific discipline underlying and informing practical QI work) is where research and QI coalesce. Improvement research projects which are typically well-designed and with some form of control groups and comparators can both address improvement priorities and generate generalisable research data at the same time. Such projects tend to be larger, often funded through research budgets and undergoing research governance processes (e.g. ethical approvals), compared to the usually smaller scale, more modest QI projects. Improvement science falls under the ‘research’ panel of Figure 1.
QI and service evaluation
In contrast to QI, which aims to make changes to drive improvements in care, service evaluation aims to assess how well a service is achieving its intended aims. While bearing similarities to QI, research and audit in particular, service evaluation usually operates over a longer time-frame and has the purpose of evaluating an already established change to a service, or the introduction of a new service (an example would be the use of virtual clinics during the covid-19 pandemic). Service evaluation is used to determine whether a service is fit for practice and will usually be used to inform local decision-making about a service where particular issues need solving. As such it may be used to initiate QI activity by identifying areas for improvement or readiness for change. Conversely it may be used to evaluate the impact of changes made as a result of QI.20,34
QI and clinical transformation
Clinical transformation is a term used to describe radical approaches to change which involve dramatically re-engineering or re-designing how health care is delivered, usually irreversibly, based on a clearly articulated vision of the desired end-state. Clinical transformation is therefore usually driven by a top-down approach, involving shifting mindsets, changing relationships and re-distributing power, in contrast to the bottom-up, collaborative approach taken for QI. By definition, the iterative tests of change that characterise QI cannot take a transformational approach, as they involve making continuous adaptations, as opposed to implementing an already agreed solution. Despite these differences, QI methods and measurement can be used to support clinical transformation, for example, by testing ideas before full-scale transformation takes place, or following-up transformation with QI to drive continuous improvement of the new ways of working. 20
Support for QI: local and national infrastructure
With growing awareness and prioritisation of QI in healthcare, the infrastructure for supporting it at a practical level has also evolved rapidly. In the United Kingdom and other high-income countries, this can be seen at the level of individual healthcare providers (e.g. Trusts) and also at a national level.
Many hospital Trusts in the United Kingdom now have hospital QI departments and personnel specialising in improvement techniques. A recent report by the Care Quality Commission (CQC) – the independent regulator for health and social care in England – found that Trusts with an established improvement culture were most often characterised by having a central QI team or hub who facilitated improvement work across the organisation, with an explicit focus of transferring expertise in improvement methodologies to frontline staff, managers and senior leaders. This was often supported by regular open-access QI project meetings and reinforced in organisational processes including performance management, induction and governance. Other features of these trusts included having a clearly articulated strategic intent for QI with commitment and a hands-on approach at senior leadership level, a culture for QI that engages clinical leaders and empowers all staff to become involved in making improvements, easily accessible channels for patient involvement in QI, and the adoption of a systems approach resulting in improvements being made beyond organisational or functional boundaries. 35
At a national level, numerous organisations have a specific focus on QI and support it in various practical respects. These include organisations who set standards for QI and those who provide guidance and assistance in achieving these standards. Examples from the United Kingdom include the following.
Standard-setting organisations
General Medical Council (GMC): The independent regulator of doctors in the United Kingdom. 36 Their ‘General Professional Capabilities Framework’ (GPCF) sets out clearly defined QI-related outcomes that should be achieved as part of medical education and continuing professional development. These range from being able to use data to identify areas for improvement, through to deploying QI methodologies and engaging stakeholders.
CQC: The independent regulator of health and adult social care in England. Their role is both to ensure healthcare providers meet government standards of quality and safety and to support improvement work. 37 Healthcare Improvement Scotland and Health Inspectorate Wales provide similar functions for the devolved healthcare systems.38,39
The National Institute for Health and Care Excellence (NICE): An independent organisation sponsored by the Department of Health and Social care aiming to improve quality and outcomes through producing national evidence-based guidelines and advice for practitioners, and quality standards and performance metrics for health and social care providers. 40
Organisations providing assistance in achieving QI standards
NHS England and NHS Improvement: NHS Improvement was formally a non-departmental body in England but has now merged with NHS England under one operating system. Collectively they are responsible for overseeing NHS-funded providers and supporting them in delivering consistently safe, high quality, compassionate and financially sustainable care. 41
The National Quality Board (NQB): Formed in 2009, the NQB drives system alignment of quality across the NHS on behalf of a number of the aforementioned organisations, including NHS Improvement, the CQC and NICE. It aims to support delivery of the NHS’ long-term plan form quality across the next 10 years. It provides advice, recommendations and endorsement on matters relating to quality and acts as a collective to influence, drive and ensure system alignment of quality programmes and initiatives. Its membership comprises senior clinical and professional leaders alongside patient and public representatives. 42
The Healthcare Quality Improvement Partnership (HQIP): An independent organisation working in partnership with patients and healthcare professionals aiming to enable measurement and improvement of healthcare services, with a focus on increasing the impact that clinical audit has on QI and providing QI resources. 43
Independent charitable organisations: For example, The King’s Fund and The Health Foundation, who conduct research, systems analysis, training and knowledge sharing to understand better how to shape policy, transform services and bring about behavioural change for QI.44,45
A number of additional external influences complement the work of these organisations to drive improvements in quality. These include economic drivers, such as the Commissioning for Quality and Innovation (CQUINs) payment framework, which enables commissioners to reward excellence by linking a proportion of service providers’ income to the achievement of national and local QI goals. 46 The publication of annual ‘Quality Accounts’ – reports about the quality of services and improvements that have or will be made – has also, since 2009, been mandatory for NHS providers, making QI a requirement as opposed to a ‘nice to have’. 47 There are also various national campaigns and programmes aiming to drive a reduction in variation in the quality of care and share best practice sit alongside these initiatives, for example., ‘1000 Lives Plus’ – the Welsh national improvement programme – and Getting it Right First Time (GIRFT) – a national initiative to improve the quality of surgical care in the United Kingdom.48,49
Application to urology
Urology has moved from a focus on audit (quality control) to one of continuous improvement (QI). A good recent example of this in Urology is GIRFT.50,51 Up until now GIRFT has reviewed large national data sets (big data) in order to identify areas of variation in care delivered by different departments. Now this variation has been established there is a pressing need to remedy it and GIRFT (Urology), NHSi, the British Association of Urological Surgeons (BAUS), the British Association of Urological Nurses (BAUN) and The Urology Foundation (TUF) are supporting this initiative going forward. It works on the premise that if the level of care provided by Urology departments in the lower deciles was able to attain the performance of the top decile departments, then significant gains in patient care would be achieved. The recent GIRFT National Specialty Report for Urology outlined 18 recommendations for improving the quality of Urological care at both a departmental and national level. 50 These included priorities such as
Reducing average length of stay across the specialty through enhanced recovery and increased use of day case pathways, while monitoring causes and rates of emergency readmissions.
Improving the secondary care pathway for patients with urinary tract stones;
Ensuring high-quality emergency urological care is available in all areas 7 days a week by focusing available resources at weekends on a smaller number of departments, while allowing some departments to operate on a 5-day basis.
The vision for Urology and other healthcare specialties is that multi-disciplinary teams receive training in the practice of QI throughout their professional careers, beginning at the undergraduate level and being reinforced throughout post-graduate education and continuous professional development. This will enable teams to identify and systematically address the improvement needs of their own departments as well as improving the implementation of best practice 52 and increasing the likelihood of GIRFT successfully delivering on its aim to improve patient care. The outlook is that continuous improvement is embedded as standard practice in Urology departments and QI becomes part of the enduring armoury of Urology teams.
Conclusion
QI is the practice of using systematic change methods and strategies originating from other industries to make measurable improvements to the configuration and delivery of healthcare services. Distinct from other approaches to improvement, such as audit and research, QI relies on the use of iterative cycles to introduce and evaluate change, combining a thorough analysis of care processes with pragmatic yet systematic measurement, and strong engagement of frontline staff, hospital management and service users. The infrastructure for supporting QI work in the United Kingdom and other developed health systems is rapidly evolving, both within organisations and at a national level, driven by an ambition to embed continuous and sustainable improvement work into the everyday practice of healthcare teams. In the next edition of this series of articles we provide an introduction to QI approaches, tools and measurement to guide multidisciplinary Urology teams in planning and delivering robust QI projects of their own.
Footnotes
Conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: N.S. is the director of the London Safety and Training Solutions Ltd, which offers training in patient safety, implementation solutions and human factors to healthcare organisations and the pharmaceutical industry. The other authors have no conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This article series and the EQUIP research programme are funded by The Urology Foundation. The Urology Foundation gratefully acknowledges further funding from the Schroder Foundation.
S.J.R. research is supported by the NIHR through a Knowledge Mobilisation Fellowship. N.S. and S.J.R. research is supported by the National Institute for Health Research (NIHR) Applied Research Collaboration (ARC) South London at King’s College Hospital NHS Foundation Trust. N.S. is a member of King’s Improvement Science, which offers co-funding to the NIHR ARC South London and is funded by King’s Health Partners (Guy’s and St Thomas’ NHS Foundation Trust, King’s College Hospital NHS Foundation Trust, King’s College London and South London and Maudsley NHS Foundation Trust), and Guy’s and St Thomas’ Charity. N.S.’ research is further supported by the ASPIRES research programme (Antibiotic use across Surgical Pathways – Investigating, Redesigning and Evaluating Systems), funded by the Economic and Social Research Council. N.S. is further funded by the National Institute of Health Research (NIHR) Global Health Research Unit on Health System Strengthening in Sub-Saharan Africa, King’s College London (GHRU 16/136/54) using UK aid from the UK Government to support global health research. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR, the charities, the ESRC or the Department of Health and Social Care.
Guarantor
JG.
Contributorship
S.J.R. and J.G. drafted the manuscript which was then reviewed and amended by the remaining authors. All authors are members of the EQUIP steering group which spearheaded the work leading to this special series of articles.