
Abstract
Objective:
Hospitals in India use the National Accreditation Board for Hospitals and Healthcare Providers guidelines as criteria to ensure safe prescribing practices. This audit was conducted to provide insight into in-patient prescription of drugs to (1) evaluate the quality of prescriptions (2) reduce prescription and medication errors (3) improve the quality of care in terms of prescriptions that the hospital provides to the patient.
Methods:
The cross-sectional study was conducted in an in-patient department of a tertiary care teaching hospital in Chennai where 153 paper-based prescriptions were continuously collected from the internal medicine department over 1 month. The prescriptions were evaluated on 13 parameters that is, patient details (including name, age, sex and Hospital unique ID), height and weight, allergies, capital letters, legibility, date and time of prescription, medicine prescribed by generic name, brand name or both, dosage, route of administration, frequency, relation with food, stop order and signature of the doctor. The data obtained was summarised and analysed using Google Sheets.
Results:
A total of 153 prescriptions from the in-patient department of a tertiary care teaching hospital were audited. Out of the 153 prescriptions and 13 parameters assessed, patient details (including name, age, sex and Hospital unique ID), legibility, route of administration and frequency were found in all of the prescriptions. On further analysis, we found that only 12.26% of the prescriptions were compliant with the components of the stop order. The majority of the prescriptions (69.28%) contained both generic and trade names.
Conclusion:
Prescriptions are the most common areas of errors. This study shows the form of errors that can arise while prescribing medications. Doctors must be adequately trained to write prescriptions and follow the standards set by the National Accreditation Board for Hospitals and Healthcare Providers. Audits need to be conducted regularly to ensure and improve the quality of prescriptions.
Keywords
Introduction
As prescriptions are delivered by medical residents and interns in most teaching hospitals in India, it is important to identify errors and implement improvements to provide quality care to patients. 1 To our knowledge, significant data regarding the errors made by medical residents and interns has not been published. Therefore, a comprehensive prescription audit was conducted, as a part of a quality improvement project, across the internal medicine department of a tertiary care teaching hospital in Chennai.
“A Clinical audit is a quality improvement process that seeks to improve patient care and outcomes through systematic review of care against explicit criteria and the implementation of change. Aspects of the structure, processes and outcomes of care are selected and systematically evaluated against explicit criteria. Where indicated, changes are implemented at an individual, team, or service level and further monitoring is used to confirm improvement in healthcare delivery.” 2
Prescription auditing is a form of audit to analyse the components, clarity and detail of the generated prescriptions from the physician to the nurses and patients, against a set standard.
In this audit, in-patient prescriptions are collected from a tertiary care teaching hospital as part of a quality improvement project and will be evaluated for 13 parameters that is, patient details (including name, age, sex and Hospital unique ID), height and weight, allergies, capital letters, legibility, date and time of prescription, medicine prescribed by generic name, brand name or both, dosage, route of administration, frequency, relation with food, stop order and signature of the doctor, which are derived from the standards set by the National Accreditation Board for Hospitals and Healthcare Providers (NABH). 3 The study is analysed by the Hospital Quality Assurance Division.
Methods
The cross-sectional study was conducted in an in-patient department of a tertiary care teaching hospital in Chennai, Tamil Nadu, India, with authorisation from the Hospital Quality and Assurance Division. Complete confidentiality was maintained throughout the study. A total of 153 paper-based prescriptions were continuously collected from the department of internal medicine over a period of 1 month from October to November 2023.
The prescriptions were analysed for the following parameters:
General details: Patient details (including name, age, sex and Hospital unique ID), height and weight, capital letters and legibility.
Pharmacological components: Allergies, date and time of prescription, medicine prescribed by generic name/brand name or both, dosage, route of administration, frequency, relation with food, stop order, signature of doctor.
Each prescription is documented by hand on a drug chart that remains valid for up to 3 days from the addition of the first drug, hence needs to be renewed regularly. This process is almost always facilitated by medical residents and interns as it is their role in the hospital.
The data obtained was collected on a daily basis, from those who fit under the inclusion and exclusion criteria and from the in-patient department and organised in a tabular column against the 13 parameters. The percentage of compliance was calculated for each parameter and was analysed using Google Sheets. A pictorial representation of the data was created using Google Sheets.
Inclusion criteria
(1) Participants who are admitted under the internal medicine in-patient department.
(2) Participants admitted during the study period.
Exclusion criteria
(1) Participants who are not admitted under internal medicine in-patient departments.
(2) Participants who are discharged during the study period.
Source of data
The data obtained was sourced from prescriptions retrieved from the internal medicine in-patient department of a tertiary care teaching hospital. Patients’ case files were collected only after seeking prior permission from the hospital authority and prescriptions were evaluated.
Written informed consent was obtained from patients at the time of admission for usage of any clinical data required for education and research while maintaining complete confidentiality. As per the institutional review board, ethical committee approval was not required as this was an analysis of data collected as a part of a quality improvement programme and there was no active involvement of participants during this study. Ethical principles were followed regardless.
Results
A total of 153 prescriptions were evaluated for the audit out of which patient details (including name, age, sex and Hospital unique ID), legibility, route of administration and frequency were accurate in all whereas relation with food was mentioned in none of the prescriptions. According to set guidelines, a stop order must include the stop order, date and signature but on evaluation, it was found that 12.26% met the standards (Table 1). The drug names in capital letters were written in only 84.97% of the prescriptions, meanwhile, date and time were mentioned in 82.35% of prescriptions. The drug allergies of patients were mentioned roughly in 91.67% of the prescriptions. The dosage of the drugs was given in about 98.03%. Only 94.78% of the prescriptions were signed by the doctor. The height and weight details of the patients were given in only 24.18%. The majority of the prescriptions (69.28%) contained both generic and trade names (Table 2).
The table displays the compliance percentage for stop order, including date, time and sign in the written prescriptions.

Among 153 prescriptions, only 106 had the stop order/sign/date/time and 47 had none.
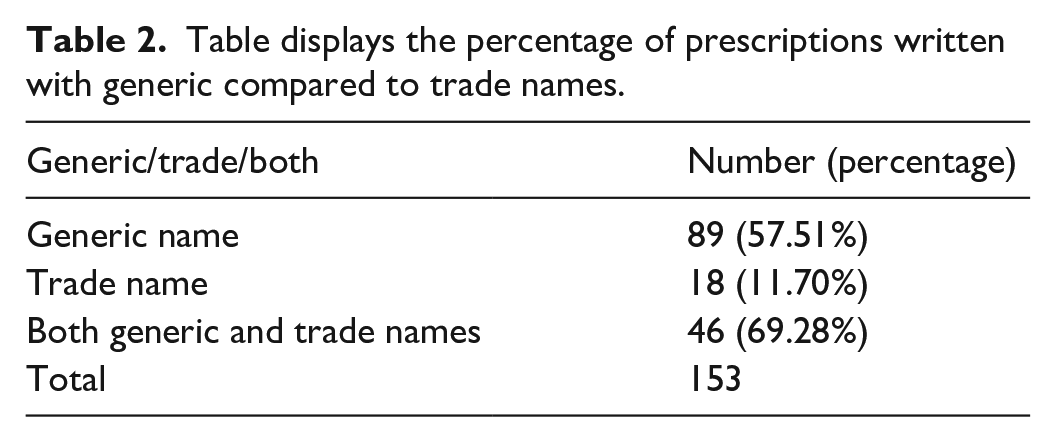
Table displays the percentage of prescriptions written with generic compared to trade names.
Discussion
In our study, we found that the date of admission patient details (including name, age, sex and Hospital unique ID), route of administration and frequency of drug intake were present in every prescription as the details were printed on a barcode at the time of registration hence making it convenient to comply. Comparable results were also observed in a study conducted by Meenakshi et al. 4 The patient details must be accurate for medicolegal purposes and to ensure that the patient receives the appropriate treatment for their diagnosis. The route of administration and frequency of drug intake are vital information that is necessary for the appropriate administration of drugs by other health care professionals. A graphical representation of the analysed data was made to better visualise the errors (Figure 1).

Bar graph illustrating the percentage of compliance for each parameter of in-patient prescriptions.
On further analysis, the prescriptions were incomplete in the following areas:
Relation with food
Capital letters
Dosage
Height and weight
Allergy
Stop order
Date and time of prescription of the drug
Signature by doctor
According to the data collected, the relation with food (before or after food) was not mentioned in any of the prescriptions. Certain drugs are required to be taken before food either due to their mechanism of action or adverse effects. Since not every drug prescribed has been studied for its relation with food, there is a limitation in providing definitive evidence. However, exploring and documenting this relationship could prove beneficial in preventing potential adverse effects. 5 Therefore, a relationship with food would be a favourable component to be mentioned in a prescription to reduce errors by other healthcare workers.
Capitalisation in prescription aids in clarity and legibility and, therefore, decreases errors such as the administration of similar-sounding drugs. 6 We have found that almost 85% of the prescriptions were written in capital letters. Ideally, capital letters should be at 100% to avoid such errors. According to the study conducted by Rebecca Fallaize et al., 7 legibility is found to be improved by the use of capital letters. Therefore, incorporating capitalisation as a component in a prescription reduces the likelihood of errors in prescription. On the other hand, all prescriptions were found to be legible regardless of capitalisation but this finding does not diminish the importance of capitalisation as it ensures a safe prescription.
Our study found that 98% of prescriptions had the dosage of drugs mentioned. Dosages of drugs are crucial components because they determine the required amount of drug for his or her treatment plan. It also avoids the confusion of availability between the various drug strengths and dosage forms, which can complicate the dispensing process. 8 As inaccurate dosing can lead to drug toxicity and treatment inefficacy, it is crucial to mention the dosages to prevent unintended consequences.
Height and weight are essential in calculating the dosage of drugs 9 ; however, it was found that the patient’s height and weight were only mentioned in the prescription during the time of admission and hence had only 24% compliance. Patient’s height and weight are indicators of their well-being. They are important factors in calculating appropriate drug dosages, nutritional counselling and calculating BMI. Each prescription drug chart is valid for 3 days; therefore, entering height and weight routinely can aid in promptly detecting any acute changes in these parameters. This could be an effective use for height and weight being entered.
Around 91% of the prescriptions had the allergy status of the patients. The allergy documentation includes medication, food and any other substances the patient is aware of. Any allergic reaction is immediately reported and details of the reaction are documented. This is imperative as it prevents such reactions from happening in the future. 10
Awareness of date and time during prescription is a crucial component for keeping track of the treatment plan. It was found that 82.35% were compliant with date and time.
As per NABH guidelines, to stop a particular drug, details such as stop order, date, time and signature must be present and only 12% of the prescriptions met the guidelines (Table 1). Approximately 94% of prescriptions had the signature of the healthcare provider.
A total of 69.3% of the prescriptions written contained both trade and generic names, while only 57.51% used generic names to prescribe drugs. Meanwhile, around 12% used the trade name while prescribing medications (Table 2). Using generic names has advantages such as having common terminology which would result in a reduction of errors while dispensing drugs whereas using trade names may be easier to prescribe due to familiarity, the availability of that specific brand may vary. 11
Prescriptions are a cornerstone of medical practice, comprehensive interventions to reduce errors such as the usage of electronic prescribing12,13 enhance safety by ensuring all the parameters are filled (e.g. drug dosage, strength, capitalisation and legibility), 14 standardised prescription forms to aid in improving prescription writing and participating in continuous quality improvement initiatives such as regular medication safety rounds and quality improvement projects to help identify further errors. By conducting regular audits, prescriptions can be assessed, enabling institutions to implement necessary improvements. 15
We recognise several limitations of this study. Firstly, prescriptions were collected over a period of time without a predetermined sample size. This approach may impact the study’s statistical power and increase the risk of bias. Secondly, this audit focuses primarily on the process of prescribing rather than the outcomes or effectiveness of the medications prescribed. Thirdly, it is difficult to confirm if all prescriptions were written by the resident or intern as faculty may modify drug charts in the absence of resident or intern. This limitation can affect the findings of this audit as it becomes challenging to attribute responsibility accurately. Effective quality improvement requires understanding which practitioners are involved in specific issues so interventions can be designed and implemented as required.
Conclusion
This study shows the form of errors that can arise while prescribing medications and it is important that doctors need to be trained adequately to write prescriptions and follow the set National Accreditation Board for Hospitals and Healthcare.
There was 100% compliance in key parameters such as patient details, legibility, route of administration, dosage and frequency while parameters such as height and weight, relationship with food, stop order of drugs were of very poor compliance. This highlights the need for adequately training medical residents and interns with frequent feedback and the need for implementing clinical protocols more effectively.
Teaching hospitals serve as an environment for learning and continuous improvement hence through conduction of regular audits, prescriptions may be evaluated, allowing institutions to bring adequate improvement.
Footnotes
Acknowledgements
The authors appreciate the Chairman and Head of the Hospital Quality and Assurance Division for their guidance and help in the completion of the audit. The authors are also thankful to all those who participated in this audit.
Author contribution
Afrah and Lahal Mohammed Abdulla conceived the study, analysed the data and drafted the manuscript; Nishfa Saleem, Aishwarya Baktharatchagan and Usha Vishwanath analysed the data and drafted the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethics approval
As per institutional review board, ethical committee approval was not required as this was an analysis of data collected as a part of a quality improvement programme and there was no active involvement of participants during this study. Ethical principles were followed regardless.
Informed consent
Written informed consent was obtained from patients at the time of admission for usage of any clinical data required for education and research while maintaining complete confidentiality.
Trial registration
Not applicable.