
Abstract
Zinner’s syndrome is a very rare congenital condition characterised by seminal vesicle cyst, obstruction of the ejaculatory duct and ipsilateral renal agenesis. Here, we present a 25-year- old young short-statured male presented with left lower abdominal colicky pain. MRI abdomen showed the absence of the left kidney with a seminal vesicle cyst on the left side. The cyst in question was laparoscopically de-roofed. A second case is a 16-years-old young male who presented with intermittent lower abdominal pain. MRI abdomen showed seminal vesicle cyst with ipsilateral absent kidney which is managed conservatively with medication.
Introduction
Zinner’s syndrome is a very rare congenital condition characterised by an ipsilateral absent kidney, seminal vesicle cyst, ejaculatory duct obstruction from a developmental anomaly of the Wolfian duct. Kidney and seminal vesicle have a common embryological origin, an anomaly of the Wolfian duct can result in genital tract maldevelopment and ureteric bud abnormality can results in non-attachment to metanephric blastema. This is the embryological basis of Zinner’s syndrome. It is considered as Mayer-Raukitansky-Kuster-Hauser (MRKH) counterpart in males. 1
Case series
Case 1
A 26-year-old young male presented with recurrent left lower abdominal pain. He underwent ventricular septal defect (VSD) and aortic regurgitation (AR) repair in infancy due to congenital valvular heart disease. He also had recurrent left testicular pain since puberty. He got married 2 years previously, had no erectile dysfunction but complaints of poor volume ejaculate and has not been able to impregnate. Blood investigations were within the normal limit. Ultrasonography abdomen showed a normal right kidney with the absent left kidney and there was a cystic lesion behind and to the left of the urinary bladder. Contrast-enhanced computed tomography (CECT) and magnetic resonance imaging (MRI) confirmed the ultrasonographic findings as a left seminal vesicle cyst with an absent left kidney (Figures 1 and 2). Semen analysis showed 1-mL ejaculate with severe oligoasthenospermia. The cyst was laparoscopically deroofed which relieved the pain of the patient. He is planned for TESA as a treatment plan for his infertility.
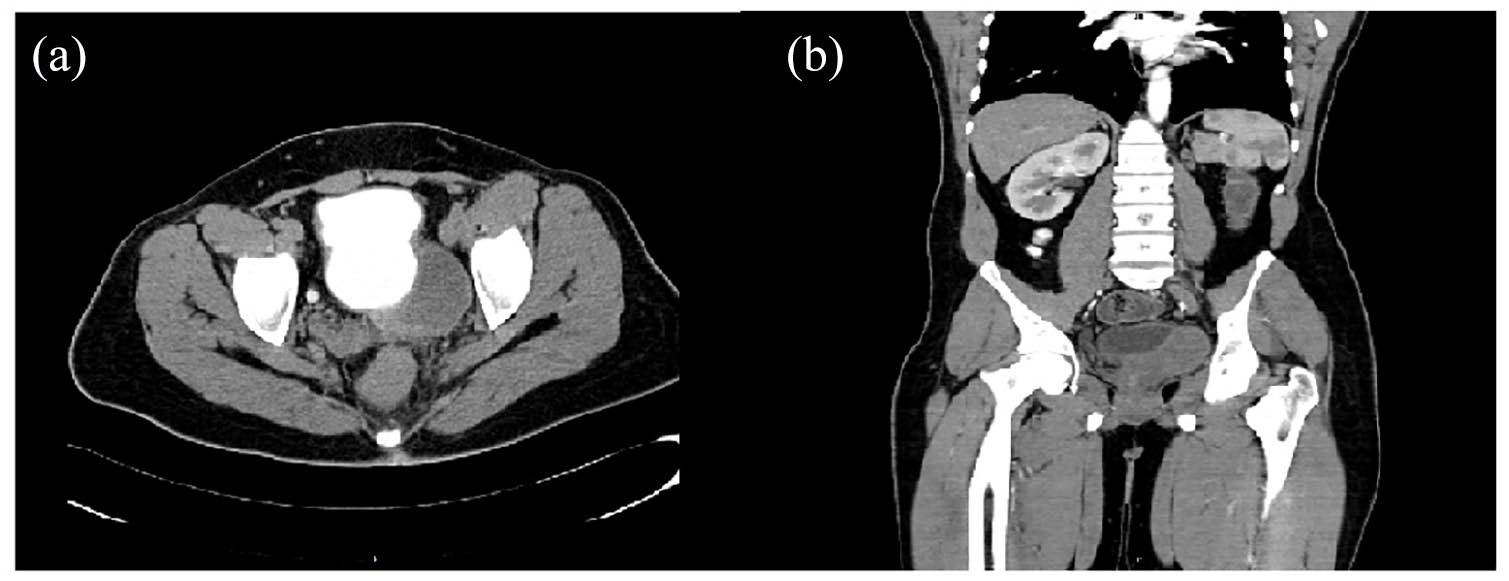
(a) CT Urogram axial view showing bladder filled with contrast and left seminal vesicle cyst without any contrast. (b) CECT abdomen coronal view showing no kidney in left renal fossa with left seminal vesicle cyst.
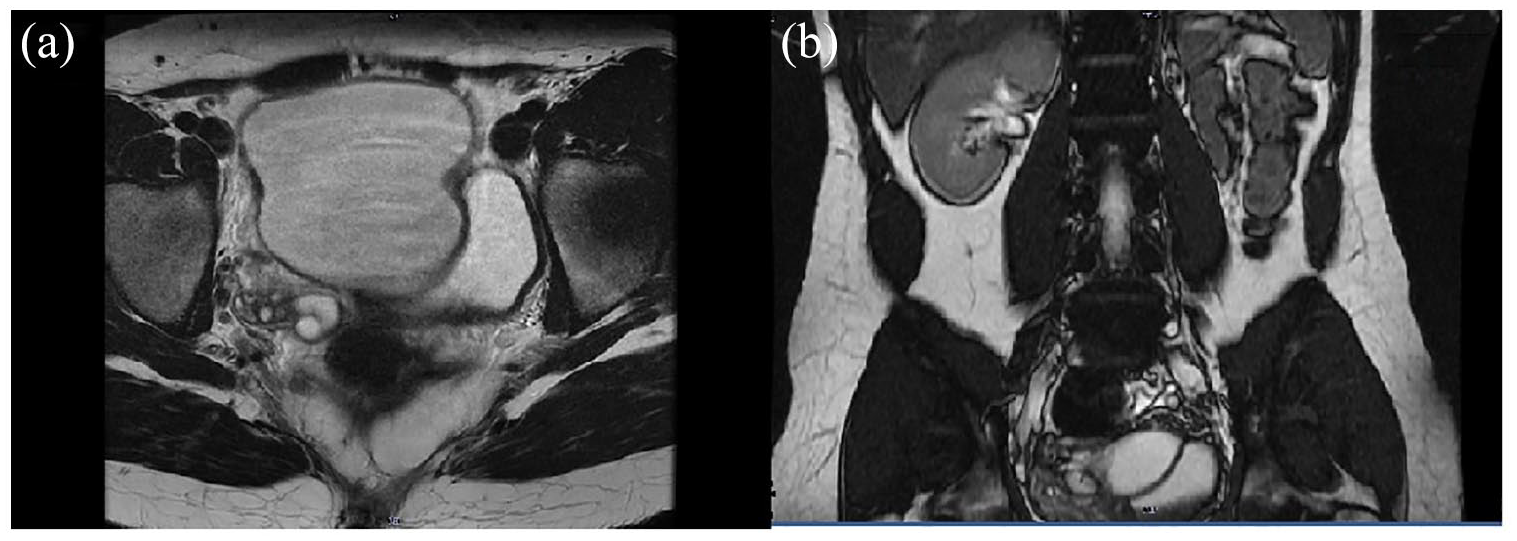
(a) MRI abdomen axial view showing bladder with left seminal vesicle cyst. (b) MRI abdomen coronal view showing no kidney in left renal fossa with left seminal vesicle cyst.
Case 2
A 16-year-old young male presented with intermittent lower abdominal pain. No previous history of any medical disease. He is unmarried and denied any sexual activity. Blood investigations did not reveal any abnormality. Ultrasonography showed cystic lesion behind the bladder and ipsilateral non visualised kidney and MRI were done which confirmed the diagnosis of seminal vesicle cyst with ipsilateral renal agenesis (Figure 3). Semen analysis was deferred as he is not sexually active at this time and his fertility would be assessed at an appropriate time. He was managed conservatively with medication without any intervention at present. He is planned for minimally invasive intervention if the pain became intractable in future.
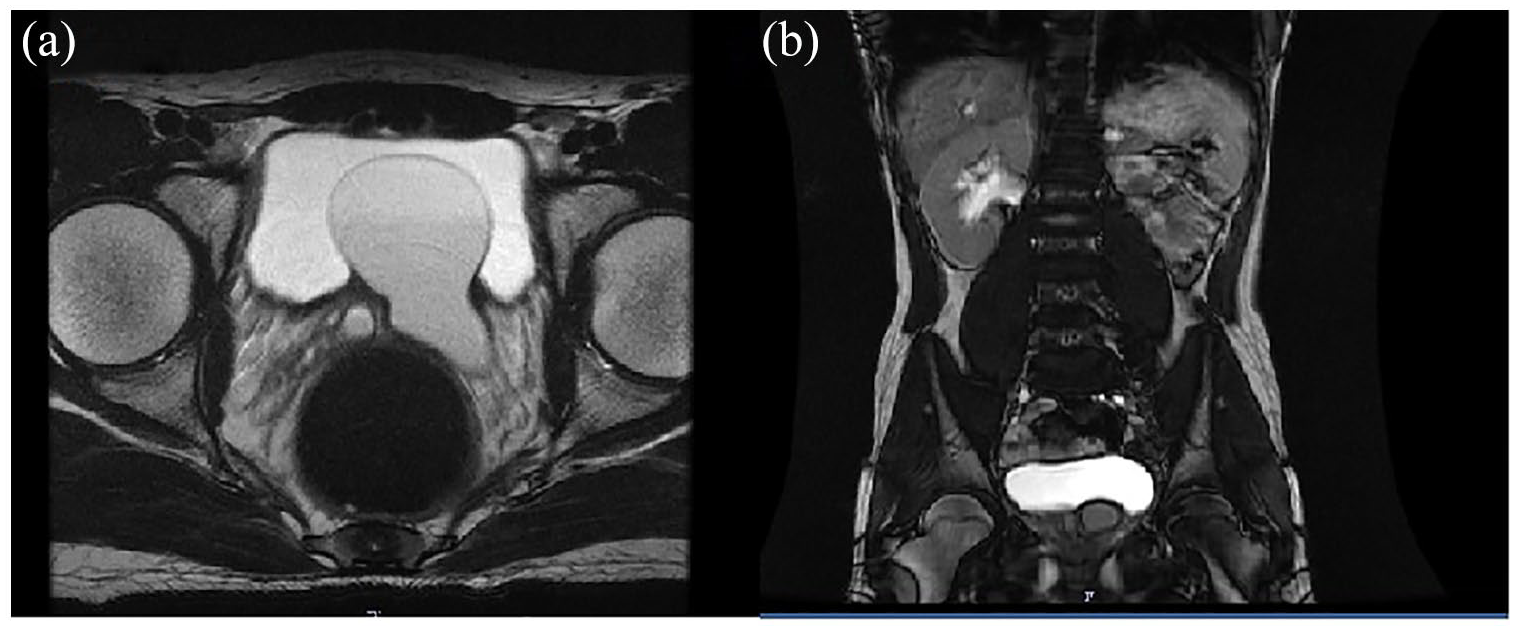
(a) MRI abdomen axial view showing bladder with left seminal vesicle cyst. (b) MRI abdomen coronal view showing no kidney in left renal fossa with left seminal vesicle cyst.
Discussion
Zinner’s syndrome was first described by Zinner in 1994 and 200 cases were reported in world literature to date. 2 Incidence is 1 in 4000 newborns. The frequency of this condition is reported to be < 0.0046%. 3 The syndrome can be explained as a Wolfian duct (which develops the male reproductive system) anomaly and absence or mutation of ureteric bud which failed to fuse with metanephric blastema leading to renal agenesis. 4 Usually, this condition is asymptomatic but for symptomatic patients, treatment may be offered. 5 Symptomatic patients typically present with lower abdominal pain with dysuria, frequency and post-ejaculatory pain. 6 Patients may also present only with infertility without any of the above symptoms. Treatment in the form of medications followed by minimally invasive intervention can be offered for symptomatic patients like in our cases. Many of these patients have oligoasthenospermia which results in infertility and can be planned for TESA to father their child. No genetic, hereditary or environmental co-relation has been established with this condition to date. Screening and early diagnosis of this condition will be difficult as it is very rare and there is no definitive co-relation with any hereditary or familial conditions.
Conclusion
The triad of Zinner’s syndrome, that is, ipsilateral renal agenesis, seminal vesicle cyst, and ejaculatory duct obstruction is a very rare condition. A high index of suspicion is required to unearth this condition more frequently. Symptomatic management can be offered with a minimally invasive procedure. Infertility is a more serious sequela that also needs to be addressed along with symptomatic management.
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Amrita Institute of Medical Science does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Guarantor
Dr. Appu Thomas, Professor and HOD, Department of Urology, Amrita Institute of Medical Science, Kochi, Kerala.
Contributorship
Dr. Hiranya Deka, Dr. Rohit Kumar Singh, Dr. Appu Thomas