
Abstract
Background:
This study analyses patients’ knowledge of common radiological investigations.
Methods:
At a university teaching hospital, 100 patients attending urological clinics, who had had a plain X-ray of the kidney, ureter and bladder, magnetic resonance imaging (MRI), computed tomography (CT) or ultrasound scan (USS), completed a 14-item Likert scale questionnaire assessing patients’ perception of safety (both qualitatively and quantitatively) and the hazards of radiological investigations.
Results:
Using a radiation risk score, patients perceived the following investigations to be in rank order of increasing radiation risk: USS (0.84), MRI (1.4), CT (1.5) and plain X-ray (1.6). On the same scale (0–5), only 17% of patients correctly attributed a risk score of 3 or 4 for a CT scan, and 49% were able to identify a plain X-ray’s risk score correctly as 1 or 2. In addition, more patients identified CT (34%) as having a lower risk of 0 than an X-ray (24%). The mean (1.35 vs. 1.60), median (1 vs. 1) and mode (0 vs. 1) for the CT risk scores are less than those for a plain X-ray, demonstrating that patients perceived CT scans to be safer. Further, the majority of patients understood USS to have no radiation exposure (56%) but thought that MRI posed a radiation risk (62%). Patients were unable to quantify radiation exposure correctly: USS (37% correctly attributed – 0 mSv), MRI (22% – 0 mSv), X-ray (47% – 1 mSv) and CT scan (28% – 10 mSv).
Conclusion:
This demonstration of suboptimal patient awareness of radiation exposure of common radiological investigations highlights the need to educate patients in order to improve patient autonomy and possibly reduce the demand for unnecessary radiological investigations such as CT.
Level of evidence:
Level 2.
Introduction
Modern radiographic techniques have revolutionised the investigation of numerous medical conditions, from urgent non-contrast computed tomography (CT) scans of the kidney, ureter and bladder (KUB) in acute stone disease 1 to the use of CT scans of the abdomen and pelvis to assess the metastatic spread of prostate cancer. 2 The most frequent radiological modalities used in urology are the plain X-ray, ultrasound scan (USS), CT and magnetic resonance imaging (MRI).
In recent years, there has been a widespread increase in the number of radiological investigations performed, particularly CT scans,3,4 which have nearly doubled from 3 million in 2012 to 5.2 million in 2018. 5 In the UK, despite accounting for only 7% of imaging procedures, CT scans accounted for 68% of total effective manufactured radiation dose. 6 Furthermore, given that the number of X-rays is ever increasing in the UK, 5 accounting for 19% of manufactured radiation dose in 2008, it is only envisaged that the effective radiation dose due to X-rays is proportionally increasing as well. 7 Thus, despite their substantial benefits, radiological investigations deliver significant radiation exposure, ranging from 0.7 for plain X-rays of the abdomen to 10 mSv for a standard CT of the abdomen and pelvis.8,9 This radiation exposure is associated with risk, where there is a 1/2000 lifetime additional risk of fatal cancer per CT scan in patients 16–69 years old in the UK. 8
With this risk in mind and the increasing use and demand for radiological investigations, it is important to try to reduce the amount of unnecessary radiological investigations. Patient knowledge and perception of radiation risk is a key determinant in reducing demand. In 2008, Menoch et al. showed a transient decline in CT scans attributable to public awareness and published studies regarding the radiation exposure of radiological investigations. 10 Our study sought to ascertain patients’ perception of the safety of the different radiological investigations and their knowledge on the hazards of these common radiological investigations.
Methods
Participants
The study was conducted at the urology department of an urban tertiary referral centre over a six-month period. Inclusion criteria were patients referred to urology clinics and patients who had had a plain X-ray, MRI scan, CT scan or USS. Exclusion criteria included those whose first language was not English or those with special communication needs. Health Research Authority approval and ethical clearance were obtained. Prior to the start of each urology clinic, eligible patients were identified. This study was then discussed with each patient, and their consent to enrol in the study was sought. If the patient granted informed consent, the questionnaire was handed to the patient to complete on their own.
Survey structure
This 10-point questionnaire presented on a single A4 sheet of paper (Appendix 1) did not contain any patient-sensitive information, and patient confidentiality was ensured.
The initial questions obtained basic demographic information such as age, sex and the radiological investigations that each patient had had. The next four questions were designed to assess patients’ perception of the relative safety of each radiological investigation by asking the patient to mark their perceived safety of the relevant radiological investigation on six-point Likert scale (0–5), with 0 being the safest and 5 being the least safe.
In order to assess patients’ knowledge of radiation exposure of the radiological investigations, it is important to understand patients’ general knowledge on radiation risks, most notably the risks of artificial radiation exposure and background radiation. Thus, several risks were listed, both actual risks and non-risks, and patients were asked to circle all the relevant risks that they thought were an effect from radiation exposure. The hazards of ionising radiation are cancer, 11 infertility 12 and leukaemia. 13
Background radiation is the radiation that an individual is exposed to in an environment without deliberate introduction of radiation sources (2.4 mSv/year). 14 Thus, to assess their knowledge on background radiation accurately, the next three questions asked patients to mark their perceived exposure to three different environments (‘natural habitats’, ‘long-haul flights’ and ‘living near Heathrow airport’) on a six-point scale (0–5).
Finally, the last question asked patients to quantify radiation exposure. For this, instead of using the usual 0–5 scale, we used a 0–1000 mSv log 10 scale. The logarithmic scale was necessary to assess whether patients knew the actual radiation exposure of each radiological investigation.
Data analysis
A Microsoft Excel spreadsheet with simple drop-box options was developed to input the data collected from the questionnaires. If patients did not complete a question, the answer was marked as incomplete for that question and excluded from the analysis of that question.
Results
The questionnaire was completed by 100 participants, of whom 70 were male and 30 were female. The majority of the male patients were between 56 and 65 years old (24%), and the majority of the female patients were between 66 and 75 years old (17%). This resembles the typical demographical distribution in a urological clinic. Most had had only one investigation (60%), with USS being the most common (83%), followed by X-ray (39%), CT scan (28%) and MRI scan (24%).
Patients’ perception of safety of radiological investigations
On the 0–5 scale, only 16% of patients correctly attributed the set risk score of 3 or 4 for a CT scan, where either risk would be suitable. In fact, 34% of patients identified a CT scan as having no radiation exposure. This shows that many patients attributed CT to be safe.
On the same scale, we set the risk score for a single plain KUB X-ray to be 1 or 2, where either risk score would be suitable. Most patients (49%) correctly identified the radiation risk of an X-ray to be 1 or 2. However 24% of patients incorrectly perceived X-ray to have no risk. The fact that more patients identified CT (34%) as having a lower risk than an X-ray (24%) and the fact that the mean (1.35 vs. 1.60) risk score was lower with CT compared to X-ray demonstrate that patients perceive CT scans to be safer than X-rays in terms of radiation exposure (Figure 1).
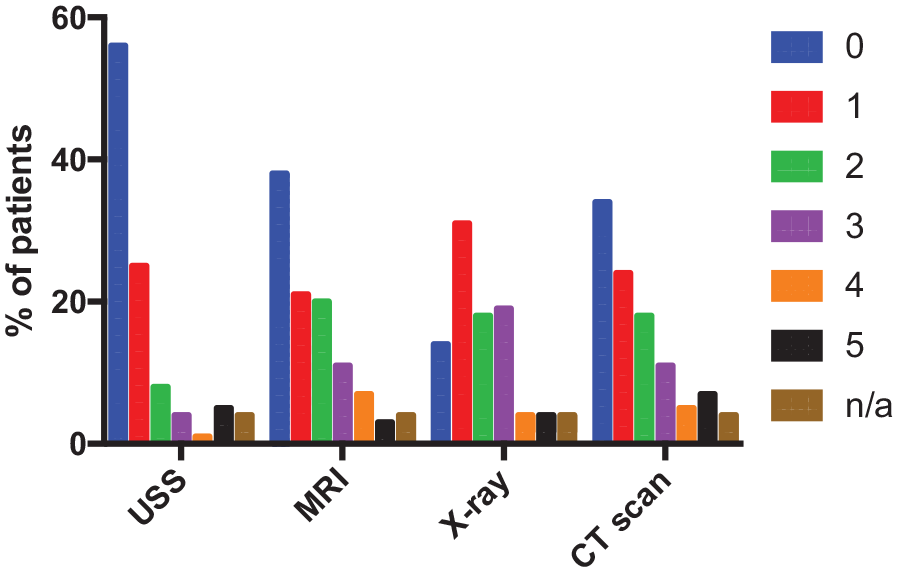
Bar chart depicting patients’ perception of risk of the radiological investigations.
Finally, on the same scale, we set the risk score for USS and MRI to be 0, as both investigations pose no radiation risk. It is important to note that MRI is not without risks, since the presence of a metal implant can be dangerous due to excessive magnetic field interactions. 15 To prevent this, all patients are screened and evaluated for metal implants, for example coils used for brain aneurysms and cochlear implants, prior to entering the MRI scanning area. 16 As this study focused on patient perceptions of ionising radiation safety, MRI was given a risk score of 0 due to the limited radiation risk. The majority of patients (56%) correctly identified USS with a risk score of 0. However, 62% identified MRI as having some radiation exposure (1.4). Hence most patients understand that USS poses no radiation risk but are not aware that this is the case with MRI.
The mean radiation scores were calculated (Table 1) and clearly demonstrate patients’ perception of risk of the radiological investigations, in order of increasing risk score: USS (0.84), MRI (1.4), CT (1.5) and X-ray (1.6).
Patients’ perception of safety of the radiological investigation.
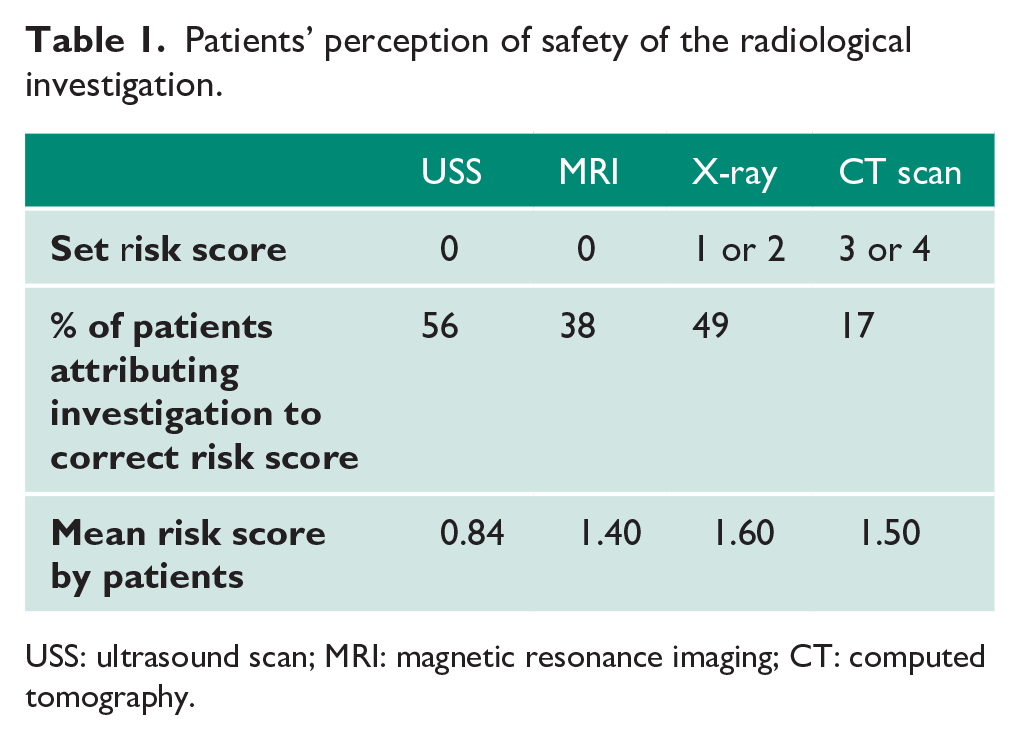
USS: ultrasound scan; MRI: magnetic resonance imaging; CT: computed tomography.
Hazards of radiation
With both risks and non-risks stated, patients were able to identify cancer, infertility and leukaemia (60%, 59% and 49% patients, respectively) correctly as the main hazards of radiation (Figure 2).
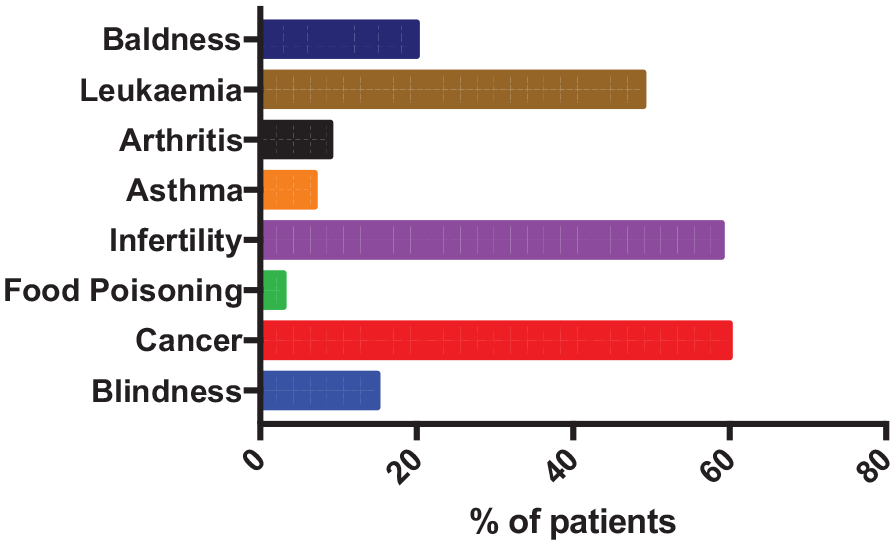
Bar chart depicting patients’ perception of hazards of radiation.
Background radiation
The natural habitat environment was set a risk score of 1, representing natural background radiation. Although 43% patients were able to identify correctly that there was background radiation, albeit in minimal doses, 27% of patients were unaware of the presence of background radiation.
The other two environments were included to obtain a comprehensive picture of patients’ perception of natural background radiation. ‘Long-haul flights’ were set a risk score of 2, as the radiation exposure from a four-hour long-haul flight (0.035 mSv) is the equivalent of five days of background radiation. 17 Only 34% were correctly able to identify that long-haul flights had a risk score of 2, and 9% associated such flights with no radiation exposure at all.
‘Living near Heathrow airport’ was set a risk score of 1, as living near Heathrow airport poses no additional risk compared to background radiation. Only 28% correctly identified Heathrow airport as having the same risk score as background radiation.
These three environments show that a significant proportion of patients were unaware of background radiation and are generally unaware of the radiation that they are exposed to in day-to-day life.
Patients’ quantification of radiation exposure from radiological investigations
To our knowledge, this paper is one of the first to report findings on patients’ quantification of radiation exposure, which was addressed by the last set of questions. Question 14 (Appendix 1) was the most complex question, as there were two elements to the question: (a) understanding the presented information and (b) matching the presumed risk of the investigation to the presented information. There were a high number of incomplete (40/100) responses to this question, which was to be expected due to the complexity of the question. Nevertheless, this question was the best discriminator of patients’ knowledge on not just the presence or absence of radiation exposure, but rather the magnitude of the radiation exposure. This question analyses the actual risk, which is what current medical knowledge defines as the radiation exposure for the different radiological modalities.
The mode of all the investigations was 1 mSv (Figure 3), suggesting that either the patients perceived all the investigations to have the same radiation exposure or they were unsure as to what the actual radiation exposure was and just took a guess. Either way, it identifies that the patients were unable to quantify radiation exposure correctly. However, no patients identified any of the investigations to have 10,000 mSv, suggesting that patients understood 10,000 mSv was an unsafe dose.
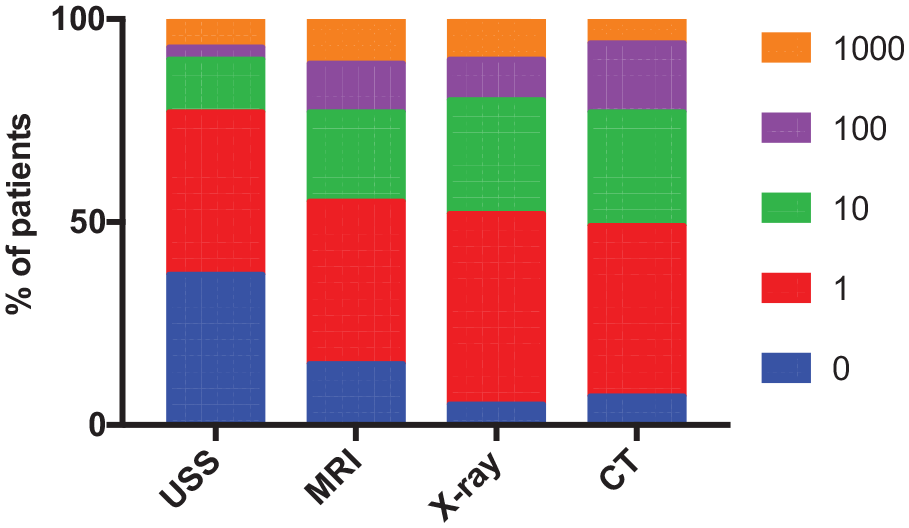
Compound bar chart depicting patients’ quantification of radiation exposure for the radiological investigations.
Only 28% of patients correctly identified CT scans as 10 mSv, and only 47% of patients identified X-rays as 1 mSv. This demonstrates that most patients were unable to quantify the radiation exposure of CT scans and X-rays correctly. It was interesting to note that the same percentage of patients (28%) quantified both CT scans and X-rays as 10 mSv (Figure 3). This clearly demonstrates that patients did not believe that CT scans posed more radiation risk than X-rays.
Both USS and MRI pose no radiation exposure (0 mSv). 18 Only 37% of the patients correctly identified USS to have no radiation exposure. Further, 23% thought USS has a radiation exposure of ⩾10 mSv. Although the qualitative data demonstrate that patients are able to identify USS as having no radiation exposure, the quantitative data show that they are unable to quantify it correctly.
With regards to MRI, only 22% of patients correctly identified MRI as having no radiation exposure. Most patients associated MRI with higher radiation exposures than USS, with 40% and 45% identified MRI to have 1 mSv and >10 mSv of radiation exposure, respectively. This clearly demonstrates that patients are unable to quantify radiation exposure and that they perceive it to be more unsafe than USS.
Discussion
The majority of patients associate CT with a lower radiation exposure and think that it is safer than X-rays when in fact the reverse is true. Patients were correctly able to identify that USS had no radiation exposure, but they misattributed MRI as posing as risk of radiation exposure and felt MRI to be less safe than USS. Although patients were able to identify hazards of radiation correctly, they were unaware of the naturally occurring background radiation to which they are continuously exposed. Finally, most patients were unable to quantify the radiation exposure from the common radiological investigations.
Most previous studies have not reported patients’ perception of radiation exposure of individual radiological investigations. Ricketts et al. 19 grouped investigations with radiation and without radiation, which is misleading for understanding patients’ perception. Ria et al.’s study 20 was one of the first to report individual radiological investigations such as MRI, which does not pose additional radiation exposure. The majority of patients wrongly stated that MRI used sources of X-rays, but attributed MRI to low radiation doses, lending itself as a possible explanation for the higher radiation risk scores in our study. However, their study may not be representative due to a poor response rate of only 24.6% compared to the 60–96% response rate in our study. Further, 10.3% of respondents in Ria et al.’s study had not received any radiological procedure in the last three years, and thus may not be representative of a typical study population, unlike our paper, where all the patients had had at least one of the four radiological investigations within the previous three months. Their study is one of the few studies that attempts to quantify perceived radiation exposure, but it uses a scale of 1–10, which is very subjective and is not as reliable as the millisevert scale.
Finally, Repplinger et al. 3 report similar findings to our study, where only 14.1% identified CT as posing more radiation than X-ray and only 22.8% identifying MRI as having no radiation exposure. However, similar to the other studies, their paper does not quantify perceived radiation exposure and does not include USS. Our study, along with the limited current literature, highlights patients’ limited awareness of the radiation exposure of radiological investigations, both qualitatively and quantitatively.
Patients’ awareness could be improved via education across different platforms in the form of leaflets, websites and personalised consultations that are specifically tailored to the patient. 21 Wider availability and local modification of the National Radiological Protection Board patient information leaflet may go some way in redressing this knowledge deficit. Innovative approaches such as incorporating the radiation dose of the scan that patient is about to undergo on the appointment letter and medical report 22 will allow patients to track their radiation exposure due to radiological investigations personally. Further, explanation of radiation doses in terms of background radiation may go some way to improving patients’ understanding of their radiation exposure with each scan, where each standard CT scan of the abdomen and pelvis exposes patients to a radiation dose equivalent to three years of background radiation. 23
Other than inadequate education of the patient, the current literature demonstrates that the patients’ suboptimal knowledge could possibly be attributed to patients not being well informed. With only 50% of the patients inquiring about radiation exposure, 91% 19 and 68.3% 22 of patients were not informed about radiation exposure, demonstrating that there is a need to improve communication between patients and medical staff.
The current literature mainly delves into clinicians’ and other health-care professionals’ suboptimal knowledge being a potential reason for patients poor knowledge. In an American study, only 22% of interviewed emergency department (ED) physicians and 13% of radiologists were correctly able to quantify the radiation exposure of a CT scan.22,24 Only 2% of physicians were able to answer more than 50% of questions on approximate doses of radiation correctly, 21 with 19% of physicians 24 being unaware that diagnostic tests increase cancer likelihood. Although medical students – the future opinion shapers among patients – were aware of relative amounts of radiation exposure, they have also been identified to have poor knowledge on the quantification of radiation exposure 19 and incorrectly identified MRI as having radiation. 24 This inadequate knowledge, from trainees to consultants, illustrates the need for education via methods such as incorporation into the medical curriculum and educational seminars on medical radiation exposure. In addition, the radiation doses of each radiological investigation could be included on the electronic system, such that the doctor is aware of the radiation dose. Further, it is noteworthy that there have been significant technological developments, where low-dose CT scans used for the diagnosis of acute stone disease have a much lower radiation dose comparable to that of a single plain radiograph. 25 Although some of this information is available through RCR iRefer guidelines, 26 they are not freely available across the whole of the NHS in the UK. Improving clinicians’ knowledge across the board will ultimately allow for more informed choice and better patient care.
Conclusion
To the best of our knowledge, this is the first study to report patients’ qualitative and quantitative perception of safety for all four common radiological investigations, and it is the first study in the UK to report findings on this subject. It highlights the need for a large-scale prospective, multicentre study across the UK. Urgent education to increase patient awareness, improving patient–doctor communication and improving health-care professionals’ awareness is required for more informed choice and reduced radiation exposure from unnecessary radiological investigations.
Supplemental Material
Appendix_1-_Copy_of_Questionnaire – Supplemental material for Patients’ perception of radiation safety of radiological investigations in urology
Supplemental material, Appendix_1-_Copy_of_Questionnaire for Patients’ perception of radiation safety of radiological investigations in urology by Prakrit R Kumar and Stuart Irving in Journal of Clinical Urology
Footnotes
Acknowledgements
We would like to thank all the patients who completed the questionnaire, and all staff in the urology outpatient clinic who have made this study possible.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethics approval
We have North East Scotland Research Ethics Committee approval (Reference Number: 14/ES/0052).
Informed consent
Written informed consent was obtained for each participant in the study.
Guarantor
S.I.
Contributorship
Both authors participated in all aspects of the research and authorship of this paper.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.