
Abstract
In countries with established programmes for vaccination of infants, toddlers and adolescents with meningococcal conjugate vaccines, serogroup B invasive meningococcal disease remains the major cause of septicaemia and meningitis in the paediatric and adolescent age groups. Novartis has developed a serogroup B meningococcal vaccine, 4CMenB, to meet this need. We reviewed all 4CMenB studies. The studies found 4CMenB to be highly immunogenic when administered in all schedules, with protective antibody levels (serum bactericidal antibody titres ≥4 or ≥5 with human complement, hSBA) against serogroup B strains expressing vaccine antigens in >95% of vaccinated cohorts. When antibody levels waned, all tested groups demonstrated booster responses. Although possibly an underestimation, the Meningococcal Antigen Typing System (MATS) technique predicts that global coverage of 4CMenB against all serogroup B strains is in the range 66% (Canada) to 91% (USA). The vaccine was found to be generally well tolerated, although local and systemic reactions, notably fever in infants, typical of many vaccines, were increased following concomitant administration of 4CMenB with routine vaccines. When tested, prophylactic paracetamol significantly decreased the frequency and severity of reactions in infants, with no clinically significant impact on immunogenicity of 4CMenB or concomitant routine vaccines. The vaccine is approved for use in the following age groups in the European Union (2 months+), Canada (2 months through 17 years), Australia (2 months+) and Chile (2 months+), following clinical evaluation in 4843 infants and toddlers, and 1712 adolescents and adults, in schedules including a three-dose (2, 3, 4 or 2, 4, 6 months) and a two-dose (6–11 months) infant series with a booster in the second year of life, a two-dose series in toddlers (12–23 months) and children (2–10 years) given 2 months apart (with a booster at least in the EU), and a two-dose series in adolescents (11–17 years) given 1–6 months apart. 4CMenB presents a solution to the unmet medical need of offering protection against serogroup B invasive meningococcal disease in all age groups above 2 months.
Keywords
Introduction
Meningococcus is an organism feared for its ability to invade rapidly and to cause high levels of morbidity and mortality. Invasive meningococcal disease (IMD) is unpredictable, with a rapid clinical course, a potentially devastating impact on the individual patient, and a notable impact on the communities in which it occurs. Although relatively rare, IMD is an important cause of bacterial meningitis and septicaemia worldwide [Thompson et al. 2006]. It is a life-threatening illness and can progress within 24 hours from initial, nonspecific symptoms and signs, such as fever and irritability, to death. The clinical presentation can be atypical, as demonstrated by the recent outbreaks of serogroup B disease in the USA [NFID, 2014]. IMD poses an ongoing challenge to clinicians and public health authorities alike.
Most cases of IMD occur in otherwise healthy, and usually young, individuals and often without warning. Even with appropriate medical intervention, IMD is life-threatening and is fatal in 5–10% of cases [Thompson et al. 2006; Cohn et al. 2010]. The fatality may be as high as 40% in septicaemia. In France, purpura fulminans is reported to occur in 17% of serogroup B cases and 39% of serogroup C cases [Gaschignard et al. 2013].
Up to 20% of survivors of IMD have significant, permanent sequelae including brain damage, adrenal impairment, hearing loss, renal failure and disfigurement [Rosenstein et al. 2001; Viner et al. 2012]. Approximately 10% of children who survive IMD caused by serogroup B will experience major amputations, seizures, major hearing loss and cognitive delay [Viner et al. 2012]. More than one third of survivors of serogroup B disease will experience other lifelong deficits such as psychological disorders, decreased IQ, digit amputations, minor or unilateral hearing loss and minor communication deficits [Viner et al. 2012]. The psychosocial burden of IMD is also high for families: parents of children with severe episodes of IMD report psychological distress for months and even years [Ehrlich et al. 2005].
The global epidemiology of meningococcal infection has changed over the last 15 years, first since the introduction of monovalent meningococcal serogroup C conjugate vaccines and, second, since the introduction of MenAfriVac®, the serogroup A conjugate vaccine deployed in sub-Saharan Africa (see http://www.meningvax.org/index.php). From a global perspective, reductions in serogroup C and A disease are observed wherever these vaccines have been introduced at a population level. This has resulted in IMD becoming a relatively rare condition in many countries.
The meningococcus is carried by individuals in the oropharynx. Identification of carriers through carriage studies is of interest in studies of transmission dynamics. However, such studies pose many challenges and are not essential from a public health perspective. Furthermore, identifying carriers does not mean either that they will develop IMD or that they will transmit the organism to someone else. The factors that result in disease and transmission are poorly understood, but in addition to social factors, antecedent viral infection may be important [Tuite et al. 2010].
Whilst good immune responses against capsular polysaccharides of serogroups A, C, W and Y meningococcus have allowed for the development of glycoconjugate vaccines, the poor immunogenicity of the capsule along with heterogeneity in the genetic and antigenic makeup of serogroup B meningococcus has meant that serogroup B vaccines to date have been very limited in their coverage. So far they have been aligned to cover prevalent strains in New Zealand, Normandy, Norway, Cuba and Brazil by use of outer membrane vesicle (OMV) vaccines. The heterogeneity of serogroup B meningococci means that a serogroup B vaccine with the potential to cover a broad range of global strains must in itself have redundancies in its makeup.
The multicomponent 4CMenB serogroup B meningococcal vaccine Bexsero® was developed by screening large numbers of potential targets inferred from the whole-genome sequence of the organism, a process known as reverse vaccinology. This novel approach reversed the usual approach of empirically identifying protective antigens, then arriving at their amino acid and genetic sequence in order for the antigen(s) to be synthesized. This ‘inverted’ strategy was enabled by means of advances in computing and genetics [Fleischmann et al. 1995; Saunders et al. 1998; Pizza et al. 2000; Tettelin et al. 2000] that made it possible to sequence the entire meningococcal serogroup B genome.
Many investigators have worked on the development of Bexsero. Many stand to benefit from the fruits of their labour. This is the story of (i) the invention of 4CMenB, (ii) the development of 4CMenB and (iii) the evidence for broad coverage of this vaccine. A number of observations are also made about (iv) the changing global epidemiology of IMD, (v) particularly vulnerable individuals and (vi) some general issues surrounding meningococcal vaccination.
Invention of 4CMenB
The process of reverse vaccinology commences at the genome level, in order to identify potential antigens that are likely to elicit an immune response in the form of the production of bactericidal antibodies [Pizza et al. 2000; Tettelin et al. 2000; Rappuoli, 2001; Giuliani et al. 2006; de Gregorio and Rappuoli, 2014]. The process allows for the identification of vaccine candidates that may not be evident through the use of traditional techniques. Following complete sequencing of the Neisseria meningitidis genome, bioinformatics analysis was performed to analyse unassembled DNA fragments and to identify open reading frames that potentially encoded novel surface-exposed or exported proteins. Protein expression was then performed in Escherichia coli. Promising proteins were purified and mice were vaccinated with these. The sera obtained were used to confirm surface exposure of the proteins by enzyme-linked immunosorbent assay (ELISA) and fluorescence-activated cell sorting (FACS) analysis, and bactericidal activity was confirmed. The accepted measure of this bactericidal activity is complement-mediated in vitro killing of bacteria, a test known to correlate with vaccine efficacy in humans. Final candidates were selected for further vaccine development.
The proteins so discovered and included in 4CMenB are: factor H binding protein (fHbp), Neisserial adhesin A (NadA) and Neisserial heparin-binding antigen (NHBA) [Comanducci et al. 2002; Madico et al. 2006; Serruto et al. 2010]. These proteins are involved in bacterial adhesion, carriage, invasion and survival. Added to these is the NZ PorA 1.4: porin A, a major OMV protein from the New Zealand outbreak strain which has demonstrated effectiveness as a single-component vaccine.
The final formulation of 4CMenB in each 0.5 ml dose consists of 50 µg of each of the proteins (fHbp, NadA, NHBA) and 25 µg of OMV, and the excipients aluminium hydroxide 0.5 mg, sodium chloride 3.125 mg, sucrose 10 mg, histidine 0.776 mg and water for injection up to 0.5 ml.
Development of 4CMenB
Due to the relative rarity of IMD, performing a fully powered efficacy study is not feasible. Instead, a correlate of protection, namely a protective antibody level measured by serum bactericidal antibody titres of ≥4 or 5 with human complement (the hSBA) is utilized [Frasch et al. 2009].
Immunogenicity in infants
Following standard phase I and phase II trials [Findlow et al. 2010; Snape et al. 2010], pivotal phase IIb/III immunogenicity trials were performed. Table 1 summarizes the two large European phase IIb/III immunogenicity trials, both of which commenced in 2008 [Gossger et al. 2012; Vesikari et al. 2013; O’Ryan et al. 2014]. The immunogenicity results are shown in Figure 1. 4CMenB was shown to be highly immunogenic following three doses in infancy, with an excellent booster response after a fourth dose. There were no clinically important interactions with the routine infant immunisations co-administered.
Vaccination schedules for the 4CMenB pivotal trials.

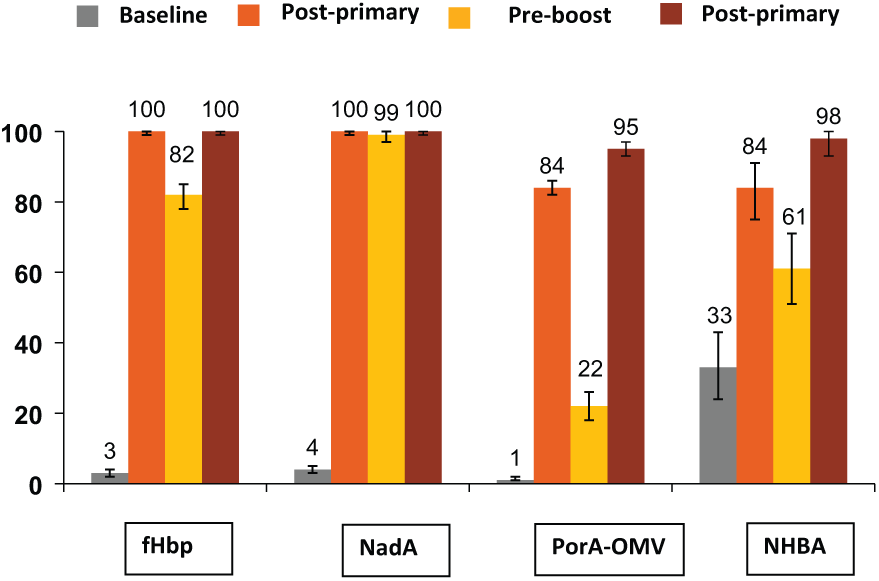
Immunogenicity in response to four doses of 4CMenB in infants.
Immunogenicity in adolescents and adults
4CMenB was also studied in adolescents aged 11–17 years (see also Table 1) [Santolaya et al. 2012, 2013; O’Ryan et al. 2014]. The immunogenicity results are shown in Figure 2. Again, the vaccine was highly immunogenic, as early as after the second dose, supporting a 2-dose schedule with doses administered between 1 and 6 months apart. Persistence of the immune response was demonstrated 18–24 months after the last vaccination. The vaccine is also immunogenic in adults [Kimura et al. 2011].

Immunogenicity in response to two doses of 4CMenB given 1 month apart in adolescents.
Safety and reactogenicity
The safety findings in infants are summarized in Table 2. The rates of solicited local and systemic adverse events amongst infants who received 4CMenB concomitantly with routine vaccines in the 2/4/6 month or 2/3/4 month schedules were similar, but were higher than those experienced by infants who received routine vaccinations alone or routine vaccinations concomitantly with the meningococcal C conjugate vaccine [Vesikari et al. 2013; O’Ryan et al. 2014]. The local and systemic reactions were transient and mostly of mild to moderate severity. Overall, the most frequent injection site reaction was tenderness (87% of 4CMenB recipients, 29% of which was reported as severe). By comparison, tenderness was reported in 79% of PCV7 recipients, 24% of which was reported as severe. Importantly, the rates and severity of such reactions did not increase after the subsequent administration of 4CMenB [Vesikari et al. 2013].
Summary of safety findings for 4CMenB pivotal trials.
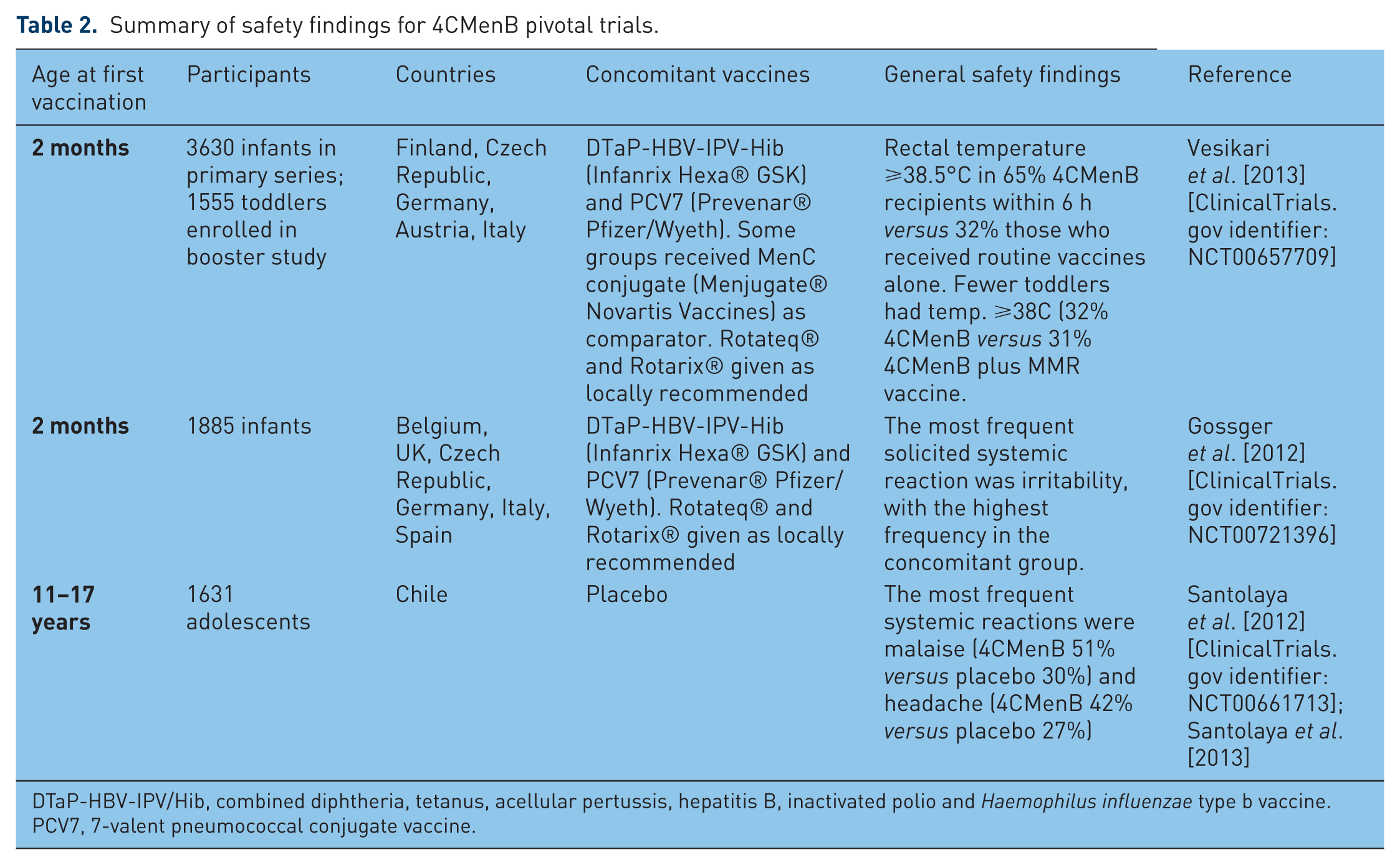
DTaP-HBV-IPV/Hib, combined diphtheria, tetanus, acellular pertussis, hepatitis B, inactivated polio and Haemophilus influenzae type b vaccine.
PCV7, 7-valent pneumococcal conjugate vaccine.
Rare events which could possibly have been related to 4CMenB included one case of pyrexia, two cases of seizure associated with fever, one case of seizure affecting the lower limbs, one case of seizure affecting an upper limb and four cases of Kawasaki disease [Vesikari et al. 2013]. Analysis of observed versus predicted cases has shown no evidence of increased incidence of Kawasaki disease.
In the study by Gossger and colleagues [Gossger et al. 2012], fever ≥39°C after any vaccination occurred in 15–17% of those receiving concomitant vaccines or those receiving the 2/3/4 month schedule. In the groups that received 4CMenB and routine vaccinations in the 2/4/6 month schedule (either concomitantly or at the intervening months, such fever occurred in 6–12% of recipients. Severe local tenderness at the injection site was reported in 12–16% of 4CMenB recipients in both the concomitant and the 2/3/4 month groups [Gossger et al. 2012].
Paracetamol administration does not affect the immunogenicity of 4CMenB either when 4CMenB is administered alone or with concomitant vaccines, nor is the immunogenicity of the concomitant vaccines impacted [Prymula et al. 2014] (study code V72P16). Whilst the occurrence of fever was higher in infants co-administered with 4CMenB compared with those given a comparator vaccine (MenC conjugate), the fever was significantly decreased by the use of prophylactic paracetamol.
Rare events which could possibly have been related to 4CMenB included six recipients who were hospitalized for fever within 2 days of vaccination, four cases of seizures and one case each of aseptic meningitis, hypotonic hyporesponsive episode, Kawasaki disease, retinal dystrophy (thought to be congenital), hearing loss and transient synovitis of the right hip [Gossger et al. 2012].
Regarding adolescents, the vaccine was generally well tolerated [Santolaya et al. 2012; Santolaya et al. 2013; O’Ryan et al. 2014]. The safety results are summarized in Table 2. The most common local reactions were pain (86% in the 4CMenB group versus 60% in the placebo group). Events judged as possibly and probably related to 4CMenB vaccination occurred in 16% of subjects. Two cases of juvenile arthritis, assessed as possibly and probably related were reported 170 and 198 days after a third dose, respectively.
Evidence for broad strain coverage of 4CMenB
The Meningococcal Antigen Typing System (MATS) has been developed to estimate the likelihood of 4CMenB covering a broad range of meningococcal strains, although it is possible that MATS is unduly conservative and may underestimate the true coverage [Donnelly et al. 2010; Frosi et al. 2013]. There are a number of properties of the bacteria which can affect the killing in the SBA: strains may express all, some or none of the vaccine antigens, the level of expression of the antigens may vary, and there is of course the well-known antigenic variation of the organism.
For any given meningococcal isolate, the MATS quantifies the level of expression and antigenic reactivity of each antigen included in 4CMenB, and relates this to the probability that this strain will be killed by the serum of an immunized person. A sandwich immunoassay using rabbit polyclonal antibodies raised against the vaccine antigens fHbp, NadA and NHBA, is used for capture and detection, and reflects both the level of expression and the amount of antigenic variation. In short, MATS determines the minimum amount of recognizable antigen needed to result in bacterial killing for each of the vaccine components. Conventional polymerase chain reaction (PCR) genotyping is used to determine the similarity of the PorA gene sequence in the test strains to that in 4CMenB.
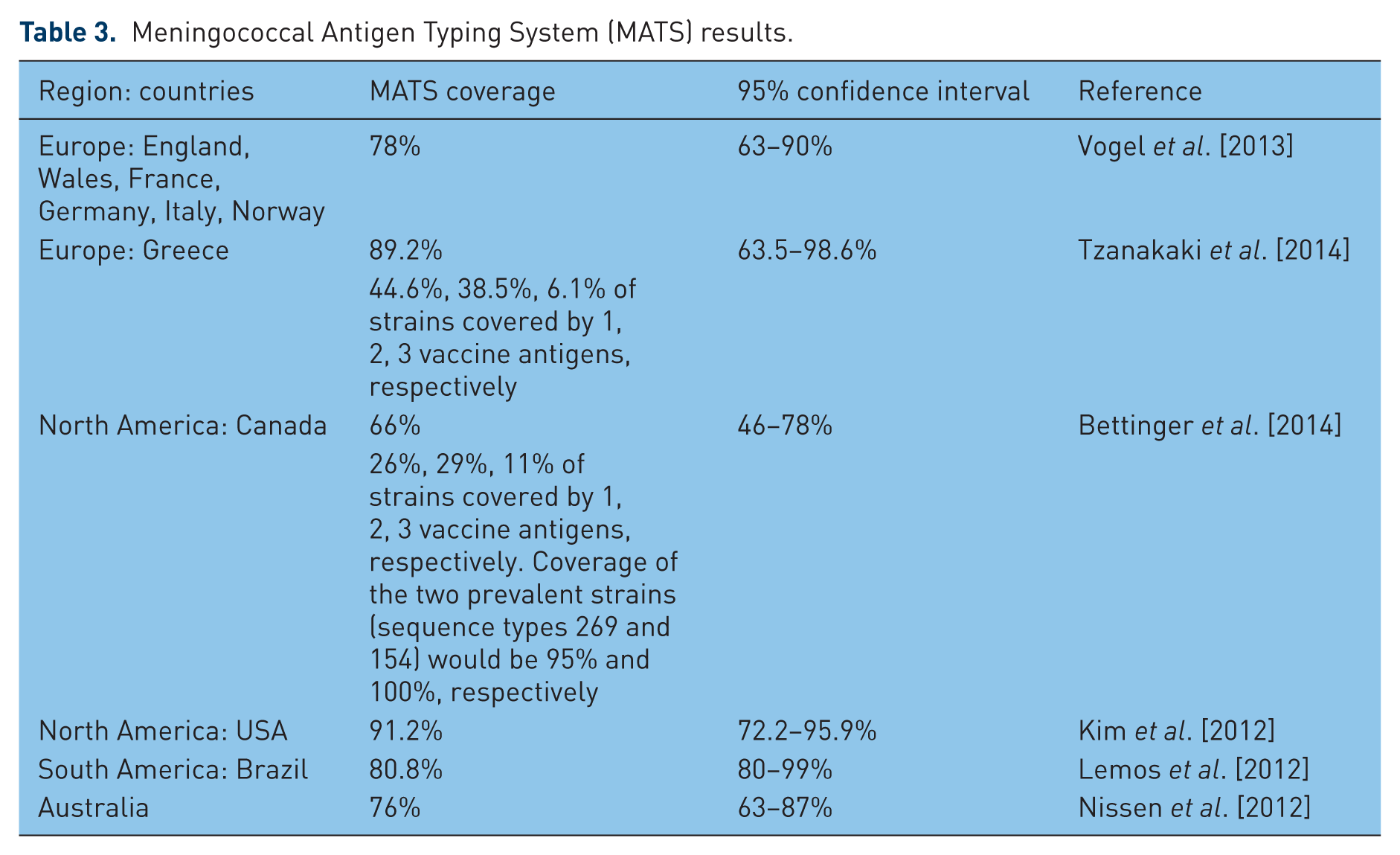
A number of meningococcal laboratories globally are being qualified to perform MATS analysis [Plikaytis et al. 2012]. Although possibly an underestimation, the MATS technique predicts that global coverage of 4CMenB against all serogroup B strains is in the range 66% (Canada) to 91% (USA). MATS analysis has been performed in a number of countries (Table 3).
Meningococcal Antigen Typing System (MATS) results.
Regarding the potentially conservative nature of MATS, a study of unbiased serogroup B meningococcal strains from the UK, when analysed by MATS predicted that 73% of all 528 strains and 70% of 40 selected strains would be killed [Biolchi et al. 2012]. However, this rises to 88 and 88%, respectively, when tested with pooled post-vaccination sera from infants and adolescents.
There is some evidence that 4CMenB may have a degree of coverage against non-B meningococci [Claus et al. 2012]. In this study of 227 representative non-B isolates from England/Wales, France and Germany, the overall predicted strain coverage of 4CMenB among non-B meningococci was 68% (95% confidence interval [CI] 44–79%), with coverage of serogroup C strains of 80% (95% CI 58–88%), coverage of serogroup W strains of 83% (95% CI 44–94%), and coverage of serogroup Y strains of 22% (95% CI 12–38%).
Changing global meningococcal epidemiology
The emergence of serogroup Y disease against a background of serogroup B and C disease, along with outbreaks, is described in detail in a review of the changing epidemiology of meningococcal disease in North America over the period 1945–2010 [Baccarini et al. 2013]. Serogroup B IMD has emerged as a major threat in Ontario, Canada [Dang et al. 2012]. An assessment of the epidemiology of IMD in Latin America over the period, 1945–2010, reveals a varying incidence of different serogroups in different countries [Safadí et al. 2013b]. In the Southern Cone of South America, there has been emergence recently of serogroup W135 disease [Lopez and Debbag, 2012].
An assessment in Asia suggests that IMD is under-recognized, due in part to the absence of proper surveillance in a number of countries, poor bacterial detection methods and social/healthcare barriers to disease reporting [Vyse et al. 2011]. A meeting of the Global Meningococcal Initiative (GMI) convened in India came to the conclusion that meningococcal meningitis was the third most common cause of sporadic bacterial meningitis in children <5 years of age in that country but that the ‘incidence is not reliably known due to suboptimal surveillance and insufficient microbiological support for diagnosis’ [John et al. 2013].
The serogroup A meningococcal conjugate vaccine MenAfriVac has had a profound impact in reducing meningococcal meningitis in the Africa [Altmann et al. 2013; Tartof et al. 2013].
In Europe, serogroup Y disease is gradually emerging [Bröker et al. 2012]. Increased detection, improved surveillance and an expansion of the case definition are thought to be at least partially responsible for the increasing reported incidence rates of IMD in Poland, where the incidence rate of all-serogroup IMD in infants was reported to be 15.7 per 100,000 in 2011 [Skoczynska et al. 2013]. In fact, some authorities are calling for a new case definition of IMD [Safadí et al. 2013a]. In Turkey, serogroup W disease has emerged in association with the Hajj [Ceyhan et al. 2013].
The incidence of serogroup B IMD in Australia remains one of the highest in the world [Lahra and Enriquez, 2012]. The introduction of the meningococcal serogroup C conjugate vaccine into the national immunization programme in 2003, as in other countries, resulted in a dramatic reduction in the incidence of serogroup C disease: in 2002, 41% of IMD cases were due to serogroup C and that rate declined to only 4% (9 out of a total of 241 IMD cases) in 2011, and to 0% in the <19 year age group by 2011 [Lahra and Enriquez, 2012]. Since the introduction of the meningococcal serogroup C conjugate vaccine, the predominant serogroup causing IMD in Australia is now serogroup B: in 2011, 74% (179 of 241 confirmed IMD cases) were identified as being due to serogroup B.
Particularly vulnerable individuals
Whilst there are likely to be a number of ‘social’ factors which predispose individuals to IMD, there are a number of medical conditions such as hyposplenism, membranous glomerulonephritis and immunodeficiency which also increase the risk [Daskas et al. 2007; William et al. 2007a and 2007b; McKeage, 2011; Hill et al. 2012; Isaacs, 2013]. A hallmark of inherited deficiencies in complement pathway proteins is an increased risk for and repeated episodes of meningococcal disease. Treatment with the monoclonal antibody eculizumab, a targeted complement inhibitor, is also associated with the development of IMD.
Complement deficiency is difficult to detect and may have as its first manifestation an episode of IMD caused by any serogroup, including those rarely seen in healthy individuals. Although these individuals are recommended to receive meningococcal vaccine, the effectiveness of vaccination has not been shown and the immunological basis for antibody-mediated killing through fixation of complement and formation of the membrane attack complex suggests that active immunization could be ineffective. Similarly, patients with acquired complement disorders, including patients treated with eculizumab, also may not be directly protected by active immunization, although they are recommended to receive available vaccines.
Protecting such individuals indirectly, by herd effects achieved through universal and catch-up vaccination programmes, may be the most efficient means to protect these cohorts, as well as infants who cannot be vaccinated early enough in life to achieve direct protection. The possibility of cross coverage by proteins contained in 4CMenB provides an opportunity to cover rarely occurring serotypes that threaten cohorts with primary immunodeficiencies.
Some general issues surrounding meningococcal vaccination
There is no evidence that mass meningococcal vaccination, as for example performed with the serogroup A meningococcal conjugate vaccine MenAfriVac, results in capsular switching [Kristiansen et al. 2013]. Although serogroup W is emerging as an important cause of IMD in countries such as France [Gaschignard et al. 2013], this phenomenon occurred before the national serogroup C meningococcal conjugate campaign and is more likely due to clonal expansion of introduced serogroups. Nor is there evidence from anywhere else that widespread use of the meningococcal C conjugate vaccine results in capsular switching.
Pharmacoeconomic analyses have been performed for quadrivalent meningococcal A, C, W, Y vaccine [Hepkema et al. 2013] and are now being performed for serogroup B meningococcal vaccines [Christensen et al. 2013].
4CMenB is approved for use in the following age groups in the European Union (2 months+), Canada (2 months to 17 years), Australia (2 months+) and Chile (2 months+), following clinical evaluation in 4843 infants and toddlers, and 1712 adolescents and adults, in schedules including a three-dose (2, 3, 4 or 2, 4, 6 months) and a two-dose (6–11 months) infant series with a booster in the second year of life, a two-dose series in toddlers (12–23 months) and children (2–10 years) given 2 months apart and a two-dose series in adolescents (11–17 years) given 1–6 months apart. It has been used in two outbreak situations at universities in the USA and has been submitted for licensure in that country.
Another vaccine to prevent serogroup B meningococcal infection is under development, a bivalent fHbp vaccine known as rLP2086 [Richmond et al. 2012]. Until serogroup B meningococcal vaccines are extensively deployed, the residual threat from IMD remains unknown.
Summary and conclusions
The 4CMenB vaccine, invented through the process of reverse vaccinology, and studied extensively for its immunogenicity and safety in infants, adolescents and adults, holds the potential to help decrease further the global burden of IMD. Through the process of MATS, the vaccine appears to be well aligned with global circulating and epidemic strains.
Bullet-point summary
In countries with established programmes for vaccination of infants, toddlers and adolescents with meningococcal conjugate vaccines, serogroup B is left as the major cause of septicaemia and meningitis in the paediatric age group
4CMenB (Bexsero®, Novartis Vaccines) has been approved in the European Union, Canada, Australia and Chile, for the active immunization of individuals 2 months of age and older against invasive serogroup B meningococcal disease, and has been submitted for approval in the USA, Brazil and other countries.
The vaccine was developed using the innovative technique known as reverse vaccinology.
Clinical evaluation in excess of 4843 infants and toddlers, and 1712 adolescents and adults, in schedules including infant two-dose or infant three-dose followed by a booster in the second year of life, toddler two-dose and adolescent two-dose, has found 4CMenB to be highly immunogenic, with protective antibody levels (serum bactericidal antibody titres ≥4 or ≥5, with human complement) in >95% of subjects, against serogroup B strains expressing vaccine antigens.
4CMenB was found to be generally well tolerated, although local and systemic reactions, notably fever in infants, typical of many vaccines, were increased following concomitant administration of 4CMenB with routine vaccines.
When tested, prophylactic paracetamol significantly decreased the frequency and severity of reactions in infants, with no clinically significant impact on immunogenicity of 4CMenB or concomitant routine vaccines.
Although possibly an underestimation, the MATS technique predicts that global coverage of 4CMenB against all serogroup B strains is in the range 66% (Canada) to 91% (USA).
4CMenB is now in clinical use, for example in outbreaks and in at-risk populations, and has been recommended for inclusion in regional and national schedules in a number of countries.
Footnotes
Conflict of interest statement
All authors are or have been employees of Novartis companies
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.