
Abstract
Although pregnancy is rare in women with cirrhosis, it is increasingly prevalent in an era of modern assisted conception techniques and improved awareness, monitoring and management of underlying liver disease. After overcoming the difficulties of subfertility and becoming pregnant, women undergo a ‘high-risk’ pregnancy which can be complicated by variceal haemorrhage (≤50%) and hepatic decompensation (≤25%). Management of these complications are similar to non-pregnant individuals. However, there are a few caveats to consider. These pregnancies are associated with adverse maternal and foetal outcomes, such as mortality (0–8%) and prematurity (19–67%) in the newborn, and mortality (0–14%), pregnancy-induced hypertension (5–22%) and post-partum haemorrhage (5–45%) in the mother. Pre-pregnancy counselling, use of predictive scores and appropriate variceal screening during pregnancy can stratify patients and improve outcomes. This review focusses on the complications that can occur during pregnancy in women with cirrhosis.
Keywords
Physiological changes during pregnancy
Portal hypertension (PHTN) is characterised by a hyper-dynamic circulation with low systemic vascular resistance and elevated portal venous pressures (≥10 mmHg). This process is exaggerated during pregnancy. Rapidly increasing blood volume during the second trimester because of renin–angiotensin system activation results in increased aldosterone production and sodium/water retention. Due to maternal blood volume expansion, augmented cardiac output and increased compression of the gravid uterus on the inferior vena cava, portal pressures rise and peak during the second trimester, thus increasing the risk of VH. 1
Progesterone and oestrogen rise progressively during pregnancy and influence hepatic metabolism, synthesis and excretory functions, for example several anticoagulant factors decrease, while certain procoagulant factors increase during pregnancy. Pregnancy also influences immunological tolerance and hepatic blood flow.
Most liver parameters remain stable during pregnancy, other than alkaline phosphatase and alpha-fetoprotein which rise during pregnancy because of foetal/placental production. Albumin tends to reduce during pregnancy. 1
Infertility in cirrhosis
Fertility is decreased in women with cirrhosis due to disruption of the hypothalamic–pituitary axis combined with impaired hepatic metabolism of sex hormones, porto-systemic shunting of weak androgens and peripheral aromatisation of androgens. Menstrual irregularities can lead to unexpected pregnancies in these women. Others may seek assisted conception, for example in vitro fertilisation, which is not without risk. 2
Pre-pregnancy counselling
Deaths secondary to chronic pre-existing medical conditions account for 58% of maternal deaths in the UK, albeit the proportion directly related to liver disease is low. 3 Nonetheless, guidance recommends that women with pre-existing conditions have multidisciplinary input during intra-partum care.
Women with cirrhosis should therefore receive pre-pregnancy counselling with a team of experts, for example a midwife, obstetrician, obstetric-physician and hepatologist. This facilitates tailored medication regimens and triage of patients by risk profile (Table 1) in addition to pre-emptive anticipation of complications. 4
Key effects of common medications used in cirrhosis during pregnancy.
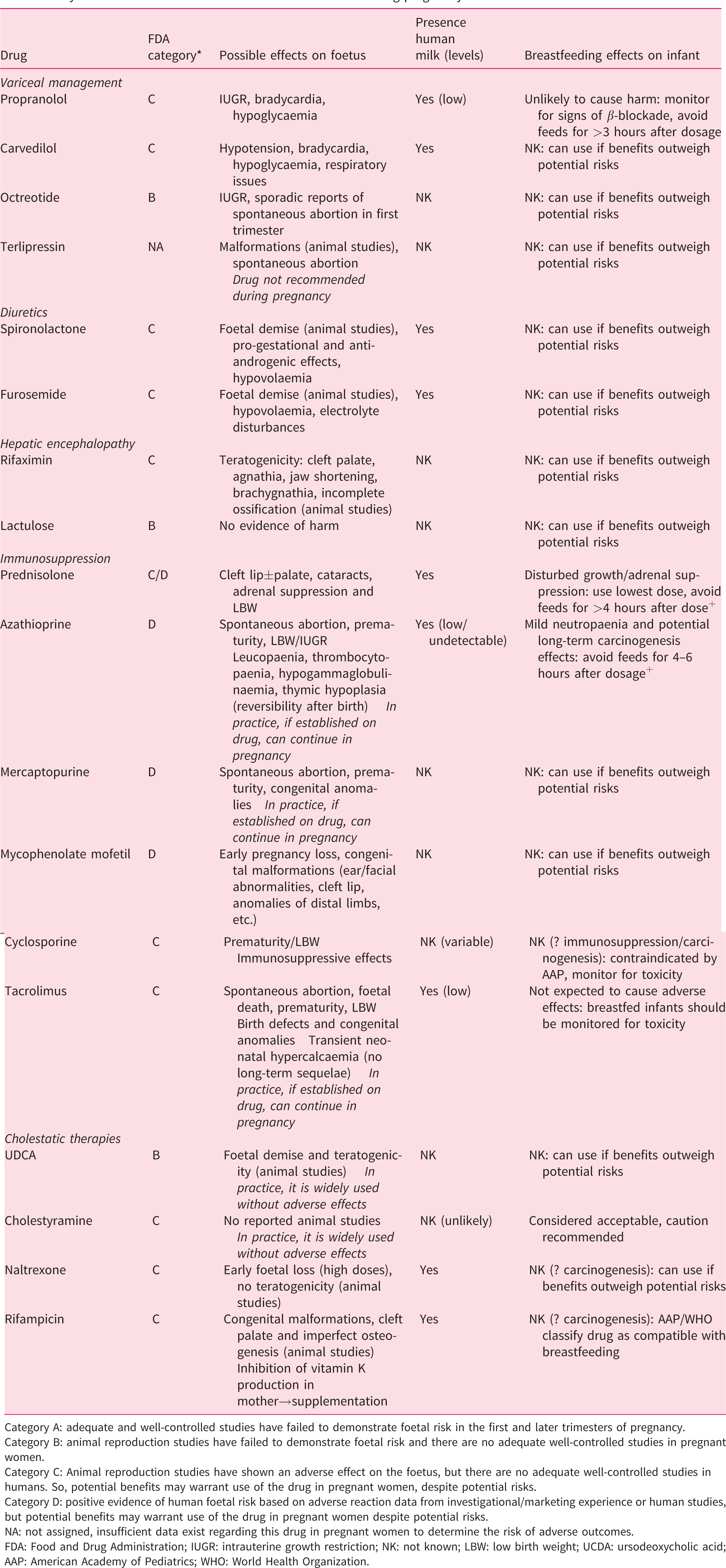
Category A: adequate and well-controlled studies have failed to demonstrate foetal risk in the first and later trimesters of pregnancy.
Category B: animal reproduction studies have failed to demonstrate foetal risk and there are no adequate well-controlled studies in pregnant women.
Category C: Animal reproduction studies have shown an adverse effect on the foetus, but there are no adequate well-controlled studies in humans. So, potential benefits may warrant use of the drug in pregnant women, despite potential risks.
Category D: positive evidence of human foetal risk based on adverse reaction data from investigational/marketing experience or human studies, but potential benefits may warrant use of the drug in pregnant women despite potential risks.
NA: not assigned, insufficient data exist regarding this drug in pregnant women to determine the risk of adverse outcomes.
FDA: Food and Drug Administration; IUGR: intrauterine growth restriction; NK: not known; LBW: low birth weight; UCDA: ursodeoxycholic acid; AAP: American Academy of Pediatrics; WHO: World Health Organization.
Risk stratification
Pregnancy outcomes are related to the severity of underlying maternal liver disease. Therefore, prognostic scoring systems utilised in clinical practice are valuable in assessing materno-foetal risk during pregnancy. Pre-conception MELD scores <6 predict positive outcomes with minimal complications, whilst MELD scores >10 predict hepatic decompensation during pregnancy. 5 These patients should be carefully counselled about the possible risks of decompensation, liver transplantation (LT) and death during pregnancy. Furthermore, a pre-conception albumin–bilirubin (ALBI; log10 bilirubin (µmol/L) × 0.66) ± (albumin (g/L)×–0.0852) score of <–2.7 (ALBI grade 1) has been demonstrated to predict live birth, and a pre-conception aspartate aminotransferase (AST)-to-platelet ratio index (APRI; AST (IU/L)/upper limit of normal/platelet count (109/L) × 100) of 0.84 (APRI grade 1) predicts term pregnancies (≥37 weeks). 4
The American College of Gastroenterology recommends variceal screening in the second trimester in pregnant women with suspected PHTN. 6 Some experts also advocate pre-conception surveillance. Platelets <110 × 109 cells/L may predict the presence of varices in the second trimester. 5 In patients with significant PHTN and intra-abdominal varices, magnetic resonance imaging may reveal pelvic varices, which is important to know when considering mode of delivery. Patients with cirrhosis are often malnourished. If there are concerns regarding nutrition pre-pregnancy or antenatally, early referral to a dietician can prove beneficial.
Maternal complications
Hepatic decompensation
Up to 25% of women with cirrhosis may experience decompensation (mostly VH) during pregnancy. 5 , 7 , 8 However, a recent retrospective population-based study from North America suggests that the rate may be lower at 1.6%. History of pre-pregnancy hepatic decompensation may significantly increase the risk (∼13%) of decompensation during pregnancy. 8
VH
VH has been reported in up to one third of pregnant women with cirrhosis and half with PHTN. 5 ,9–12 Associated mortality was up to 50% in older studies, although recent series suggest rates <20% (Table 2). 5 ,11–14 Although VH does occur during pregnancy in women with non-cirrhotic PHTN, mortality is only 2–6% (better liver function). 9 , 15
Summary of studies evaluating materno-foetal outcomes of pregnancies in women with cirrhosis.
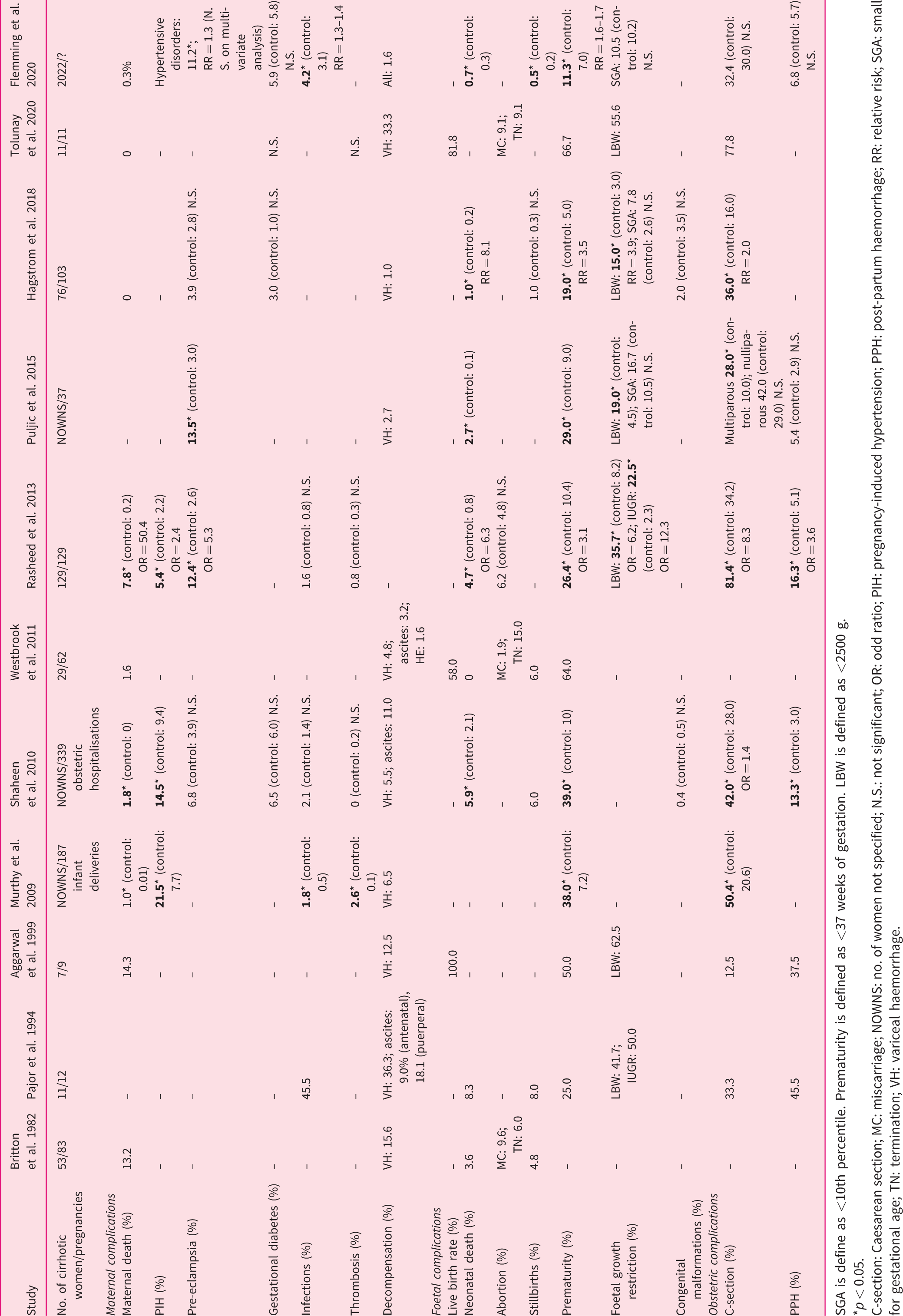
SGA is define as <10th percentile. Prematurity is defined as <37 weeks of gestation. LBW is defined as <2500 g.
*p < 0.05.
C-section: Caesarean section; MC: miscarriage; NOWNS: no. of women not specified; N.S.: not significant; OR: odd ratio; PIH: pregnancy-induced hypertension; PPH: post-partum haemorrhage; RR: relative risk; SGA: small for gestational age; TN: termination; VH: variceal haemorrhage.
Endoscopy
With a few stipulations, OGD can be performed safely in pregnant women. 6 , 16 In late pregnancy, aorto-caval compression in the supine position can cause reduced venous return, cardiac output and uteroplacental blood flow. Left lateral positioning avoids this. Despite a Food and Drug Administration (FDA) pregnancy category of D, in practice, midazolam is used widely during endoscopy in pregnant women, without significant consequences. 16 Over-sedation (benzodiazepines/opiates) can cause materno-foetal hypotension/hypoxia. Guidelines suggest that meperidine (pethidine) and propofol can be used with relative safety in pregnant women. 6
Management
In acute VH during pregnancy, broad-spectrum antibiotics should be initiated. Use of terlipressin is controversial; its vasoconstrictive properties may induce uterine contractions, with decreased uterine blood flow leading to ischaemia, which can subsequently result in spontaneous abortion and placental abruption. 7 , 17 It should only be used in cases when endoscopic therapy has failed. Octreotide may be a suitable alternative (Table 1).
EBL remains the mainstay of therapy for acute VH. 18 Sclerotherapy has previously been used successfully, but potential shunting of toxic material to the placenta remains concerning. 10 , 19 Prospective studies comparing these two methods in pregnancy are lacking, although EBL is superior in the non-pregnant population.
In those with refractory bleeding despite optimal endoscopic therapy, rescue trans-jugular intrahepatic portosystemic shunt (TIPSS) insertion can successfully control bleeding. 20 In this situation, the benefits of performing this procedure are likely to outweigh the risks. Each case should be individually evaluated in a multidisciplinary setting. Historically, a surgical shunt (splenorenal/portocaval) was an option to manage life-threatening VH. TIPSS has superseded the requirement for surgical intervention.
Portal-vein flow usually increases during pregnancy, although the impact of pregnancy on TIPSS function is unknown. 21 In women with previous TIPSS, regular (frequency unclear) ultrasound monitoring of the shunt during pregnancy is recommended. A few case reports have described ongoing TIPSS patency during pregnancy, with possible increased flow velocity in the portal vein, stent and hepatic artery. 22 , 23
If varices are identified, prophylactic EBL to prevent VH remains controversial, but is practiced in some centres. 24 Primary prophylaxis with non-selective beta-blockers may be beneficial but should be balanced with risks (Table 1).
Hepatic encephalopathy
Similar principles apply to managing hepatic encephalopathy (HE) during pregnancy, although certain medications should be avoided where possible (Table 1). At delivery, the presence of HE may influence the administration of anaesthesia, as certain drugs may precipitate hypotension and worsen HE.
Ascites
Ascites is relatively rare (7–11%) during pregnancy. 14 , 25 If present, diuretics and paracentesis should be avoided, depending on the risk–benefit balance. If spontaneous bacterial peritonitis is confirmed, management includes antibiotics and human albumin solution. It is important to consider alternative aetiologies of intra-abdominal infection, as secondary peritonitis increases the risk of premature delivery and placental abruption. Prophylactic antibiotics (norfloxacin/ciprofloxacin) should be avoided during pregnancy if possible, but can be used safely during breastfeeding, provided the infant is monitored for side effects (diarrhoea/candidiasis).
Splenic artery aneurysm rupture
Spontaneous rupture of a splenic artery aneurysm (SAA) is rare. Risk is greatest in pregnant women with cirrhosis and PHTN in the third trimester due to increased splenic blood flow from a hyper-dynamic circulation. 26
Symptoms of rupture include abdominal pain and syncope. A curvilinear calcification in the left upper quadrant on imaging may represent a SAA. 27 Up to 25% of patients experience the ‘double rupture phenomenon’: warning symptoms from an initial small self-contained rupture, which hours later results in significant rupture with rapid intra-abdominal bleeding and haemorrhagic shock. Materno-foetal mortality rates are high (70–95%) in these cases. 7 , 27
Trans-catheter embolisation is now the mainstay of treatment in cases of rupture, with surgical intervention (ligation±splenectomy) reserved for failed therapy or when interventional radiology is unavailable. Prophylactic intervention can be considered if a SAA has previously ruptured or if a large aneurysm (>2–3 cm) has been identified pre-conception.
Malignancy
Hepatocellular carcinoma (HCC) in pregnancy is rare. Hyperoestrogenaemia and increased vascularity has been postulated to accelerate HCC progression during pregnancy, but data are inconsistent. 28 Due to foetal production, alpha-fetoprotein cannot be used as a diagnostic/surveillance marker of HCC during pregnancy. HCC in pregnancy has been associated with poorer obstetric outcomes, with a 12.5% risk of spontaneous rupture and inferior maternal survival rates. 29 , 30 Trans-arterial embolisation, radiofrequency ablation and surgery are all possible during pregnancy, although careful consideration of risk versus benefit must occur in a multidisciplinary setting. 30
Maternal outcomes
Death rates in pregnant women with cirrhosis range from 0% to 14%; older studies report higher rates, while newer ones report rates <2%. 5 , 8 , 9 , 12 , 14 , 25 ,31–33 Women with cirrhosis are more likely to have pre-pregnancy co-morbidities (e.g. diabetes, hypertension, obesity and dyslipidaemia) when compared to the general population. 8
Rates of pregnancy-induced hypertension (PIH) range widely between 5.4% and 21.5% in various studies. Comparisons with control groups suggest higher rates than the general population. 14 , 25 , 32 It is difficult to interpret whether rates (3.9–13.5%) of pre-eclampsia are greater in pregnant women with cirrhosis. 11 , 14 , 25 , 33 Angiotensin-converting enzyme inhibitors, calcium channel blockers and certain beta-blockers should be avoided where possible. Studies have shown no significant difference in rates of gestational diabetes in pregnant women with cirrhosis compared to background risk. 12 , 14 , 33
Intrahepatic cholestasis of pregnancy (ICP) is more common in women with cirrhosis, with one study suggesting a relative risk of 10.6 when compared to the general population. 8 , 34
Specific liver diseases
Hepatitis B virus
In selected women (hepatitis B virus (HBV) DNA >200,000 IU/mL), antiviral therapy from 24 to 28 weeks of gestation (to 12 weeks post delivery) can reduce the risk of vertical transmission in addition to HBV immunoglobulin and vaccination at birth. 35 Tenofovir has a FDA pregnancy category of B, with no evidence of foetal harm if used during pregnancy. Alternatively, entecavir has a FDA pregnancy category of C and should be avoided where possible.
Hepatitis C virus
Mother-to-infant transmission occurs in ∼5–10%, although this varies in the presence of human immunodeficiency virus co-infection and high hepatitis C virus (HCV) viral load. Prolonged rupture of membranes has been associated with increased risk of perinatal transmission. The second stage of labour should therefore be brief in these women. Obstetric outcomes amongst HCV-infected pregnant women are variable. One large cohort study reported an association between HCV infection and gestational diabetes, low birth weight (LBW) and admission to neonatal intensive care. 36 ICP is also more common in these women. 34 Direct-acting antiviral therapies are not currently recommended in HCV-infected pregnant women, although pilot studies are evaluating safety and efficacy.
AIH
Disease activity usually improves during pregnancy. However, flares can occur antenatally or post-partum. 37 , 38 The best outcomes occur in those who have well-controlled disease pre-conception. 38 Immunosuppression (except mycophenolate mofetil) should be continued during pregnancy (Table 1). A flare during pregnancy can usually be managed with augmentation of immunosuppression. Rarely, a flare may precipitate an episode of decompensation (±LT). Irrespective of cirrhosis status, pregnant women with AIH have increased rates of foetal loss, prematurity and LBW. 37 , 38
Primary biliary cholangitis
Disease course during pregnancy is variable. Ursodeoxycholic acid (UDCA) can be continued safely during pregnancy, with cautious use of anti-pruritics for symptomatic or de novo pruritus (Table 1). Rates of ICP and prematurity are increased in these pregnancies. 39 Post-partum, liver enzymes can deteriorate. 40
Primary sclerosing cholangitis
Course of disease during pregnancy depends on the presence of cirrhosis/PHTN. UDCA can be continued/escalated during pregnancy. Complications during pregnancy include pruritus, jaundice and cholangitis secondary to gallstones or biliary strictures. If imaging during pregnancy reveals obstructed stones or a dominant stricture, an endoscopic retrograde cholangiopancreatography can be considered. These pregnancies are associated with increased risk of preterm birth and ICP. 39
Wilson’s disease
This condition can affect fertility. Increased rates of spontaneous abortion have also been reported. 41 During pregnancy, treatment must be continued, as disruption can lead to liver failure. Penicillamine has a FDA pregnancy category of D, with evidence of possible teratogenicity and congenital cutis laxa. Trientine has a FDA pregnancy category of C, with evidence of possible teratogenicity. However, satisfactory outcomes have been reported with both chelating agents during pregnancy. 41 The American Association Study of Liver Diseases recommends reducing penicillamine/trientine to 25–50% of the pre-pregnancy dose. This reduces foetal risk, in addition to improving wound healing following a Caesarean section (C-section). 42 There is no evidence of harm with zinc therapy during pregnancy. However, it is not recommended during breastfeeding due to potential zinc-induced copper deficiency in the infant.
Foetal outcomes
Live birth rates in pregnancies of women with cirrhosis are poorly reported, with rates varying between 58% and 100%. 5 , 12 , 31 Rates of neonatal death are between 0% and 8.3%, and are believed to be greater than the general population. 5 ,9–11, 14 , 25 , 33 A proportion of these deaths are likely to be related to prematurity/LBW. Stillbirth rates range between 1% and 8%. 5 , 9 , 10 , 14 , 33 Congenital malformation rates (0.4–2%) are comparable to the general population. 14 , 33
Prematurity in pregnant women with cirrhosis is common, although reported rates vary widely between 19% and 67%. 5 ,10–12, 14 , 25 ,31–33 In association, 15–63% of neonates have LBW (<2500 g).10–12, 25 , 31 , 33 Birth weight is dependent on gestational age and is not a true reflection of pathological growth. Assessment of intrauterine growth restriction (IUGR), the definition of which has changed over years, is a more accurate method of evaluation.
Flemming et al. have recently demonstrated that pregnancies in women with cirrhosis are independently associated with induction of labour, puerperal infections, preterm delivery, large for gestational age infants and neonatal respiratory distress. 8
Delivery
An area of controversy in women with PHTN is approach to delivery. Concerns arise from excessive straining and repeated Valsalva manoeuvres during labour, which change intra-abdominal/portal pressures and may precipitate VH. There are no recent studies evaluating the impact of vaginal delivery on the risk of VH. Consequently, many experts recommend an elective C-section, which is not without risk.
In pregnant women with cirrhosis, C-section rates (12–81%) vary widely.10–12, 14 , 25 ,31–33 Patient/institutional preference and temporal trends in obstetric practice may explain these discrepancies. Where appropriate, a C-section may require corrective products and pre-emptive surgical planning to avoid intra-abdominal/pelvic varices. Furthermore, women with cirrhosis may experience poor wound healing and infection. Our institutional preference is to reserve C-sections for obstetric indications only. Assisted vaginal deliveries with a shortened second stage of labour, to avoid excessive elevations in intra-abdominal pressures, are also suitable.
Post-partum haemorrhage (PPH) occurs in 5–45% of women with cirrhosis. 8 , 10 , 11 , 14 , 25 , 31 This is due to a combination of factors: thrombocytopaenia, imbalance of coagulation factors and aberrant variceal formation. Management includes blood/coagulation factors, uterine contractile agents, ligation of bleeding vessels and, if all fails, hysterectomy.
Post-partum
Women with cirrhosis should be able to breastfeed, provided they are not on contraindicated medications (Table 1). Early advice on contraception should be given. Women with compensated cirrhosis have no limitations in their contraceptive options. However, those with decompensated cirrhosis are restricted to barrier methods and copper intrauterine devices. 43 Other methods can be considered on an individualised basis after specialist discussion. A caveat to consider is the use of copper intrauterine devices in Wilson’s disease, as the manufacturers list this condition as a contraindication. 44
Conclusion
Pregnancy in women with cirrhosis is not without risk, with increased rates of maternal mortality, VH, PIH and PPH, and increased rates of neonatal mortality, prematurity and LBW. Women should be offered PPC, which not only better informs the patient, but also allows the opportunity to prognosticate and predict outcomes, with the initiation of individualised therapies/monitoring during pregnancy. Unfortunately, data are limited in the field, making accurate counselling problematic. However, valuable registry data will be available in the upcoming years through the UK Obstetric Surveillance System and European pregnancy registries, which will better educate the hepatology and obstetric communities.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
No formal ethics review was required for this publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: M.A.H. is supported by an European Association for the Study of the Liver (EASL) Registry Grant (Liver Disease in Pregnancy), The King’s College Hospital NHS Trust Charity (Orpin Bequest) and The Kelly Group.
Informed consent
No informed consent was required for this review.