
Abstract
Background
Current risk stratification models for early invasive (T1) colorectal cancer are not able to discriminate accurately between prognostic favourable and unfavourable tumours, resulting in over-treatment of a large (>80%) proportion of T1 colorectal cancer patients. The tumour–stroma ratio (TSR), which is a measure for the relative amount of desmoplastic tumour stroma, is reported to be a strong independent prognostic factor in advanced-stage colorectal cancer, with a high stromal content being associated with worse prognosis and survival. We aimed to investigate whether the TSR predicts clinical outcome in patients with non-pedunculated T1 colorectal cancer.
Methods
Hematoxylin and eosin (H&E)-stained tumour tissue slides from a retrospective multi-centre case cohort of patients with non-pedunculated surgically treated T1 colorectal cancer were assessed for TSR by two independent observers who were blinded for clinical outcomes. The primary end point was adverse outcome, which was defined as the presence of lymph node metastasis in the resection specimen or colorectal cancer recurrence during follow-up.
Results
All 261 patients in the case cohort had H&E slides available for TSR scoring. Of these, 183 were scored as stroma-low, and 78 were scored as stroma-high. There was moderate inter-observer agreement (κ = 0.42). In total, 41 patients had lymph node metastasis, 17 patients had recurrent cancer and five had both. Stroma-high tumours were not associated with an increased risk for an adverse outcome (adjusted hazard ratio = 0.66, 95% confidence interval 0.37–1.18; p = 0.163).
Conclusions
Our study emphasises that existing prognosticators may not be simply extrapolated to T1 colorectal cancers, even though their prognostic value has been widely validated in more advanced-stage tumours.
Introduction
With the introduction of population-based screening programmes, a growing number of early invasive colorectal cancers (T1 CRC) are being diagnosed. 1 These tumours can be cured by local resection, as long as they have a favourable prognosis, that is, a relatively low risk of lymph node metastases (LNM) or disease recurrence. Current risk-stratification strategies are mainly based on histological features (i.e. deep submucosal invasion, poor differentiation, lymphovascular invasion and high-grade tumour budding 2 ), which are associated with an increased risk of LNM and CRC recurrence. 3 , 4 However, the sensitivity of these features is relatively low. As a result, a large proportion of patients (>80%) with T1 CRC are inadvertently classified into the high-risk category and undergo unnecessary treatment. 5 Thus, there is a need for more accurate discrimination between prognostically favourable and unfavourable T1 CRCs.
A widely studied prognostic parameter is the tumour–stroma ratio (TSR), which is a measure for the relative amount of desmoplastic tumour stroma. 6 Scoring of the TSR is a relatively simple and fast procedure with a low inter-observer variation, as shown by multiple independent studies.7–11 The TSR has been reported to be a strong independent prognostic factor in several solid malignancies, including breast cancer, 8 , 9 hepatocellular carcinoma, 11 non–small cell lung cancer 12 and oesophageal cancer, 7 , 10 with a high stromal content being associated with worse prognosis and survival. For CRC, the prognostic value of the TSR has also been confirmed by multiple studies (hazard ratio (HR) of ∼2.0–2.5 for stroma-high tumors13–18), but it should be noted that these studies only included a small proportion (<10%) of T1 CRC patients. As considerable heterogeneity in stromal composition can exist between different stages of the same tumour type, 19 extrapolation of aforementioned findings to T1 CRCs may be hampered. To date, no TSR studies have been performed in large cohorts consisting exclusively of T1 CRC patients.
Therefore, the aim of our study was to investigate the association between TSR and clinical outcome in patients with non-pedunculated T1 CRC.
Methods
Study design and patients
We evaluated hematoxylin and eosin (H&E)-stained tumour tissue slides from a retrospective multi-centre case cohort of patients with non-pedunculated surgically treated T1 CRCs selected from the Dutch T1 CRC Working Group database. The inclusion process has been described in detail elsewhere. 20 In short, all patients with non-pedunculated T1 CRCs treated between 2000 and 2014 with known lymph node status after surgical resection were included in the baseline cohort (exclusion criteria: hereditary predisposition for CRC, inflammatory bowel disease, synchronous CRC, non-CRC related death within one year, non-adenocarcinoma, neo-adjuvant radiotherapy and missing reports). The final case-cohort consisted of a random 50% sample from the baseline cohort. Patients outside this random sample who reached the primary end point were also included in the final case cohort. The primary end point was adverse outcome, which was defined as the presence of LNM in the surgical resection specimen and/or (local or distant) CRC recurrence during follow-up. The left hemicolon was defined as the descending or sigmoid colon, and the right hemicolon was defined as the colon proximal to the splenic flexure.
This study was approved by the Medical Ethics Committee of the Leiden University Medical Centre (reference number G17.078, date of approval 20 December 2017). Informed consent of the participating patients was waived by the Medical Ethics Committee of the Leiden University Medical Centre (reference number G17.078, date of approval 20 December 2017). The study was performed in accordance with the Declaration of Helsinki, and conforms to the STROBE 21 guidelines.
Histology review
All tumours were classified according to the tumour-node-metastasis staging system. 22 T1 CRC was defined as histological tumour invasion through the muscularis mucosa and into, but not beyond, the submucosa. Size measurements of the invasive part and assessment of all conventional high-risk factors (submucosal invasion, poor differentiation, lymphovascular invasion and high-grade tumour budding 2 ) were performed by at least one pathologist (M.M.L. and/or G.J.A.O.) with special expertise in gastrointestinal pathology, as described previously. 20 High-grade tumour budding was defined as ≥Bd2. 23 Deep submucosal invasion was defined as an invasion depth ≥1000 µm or a Kikuchi level ≥Sm2. 24
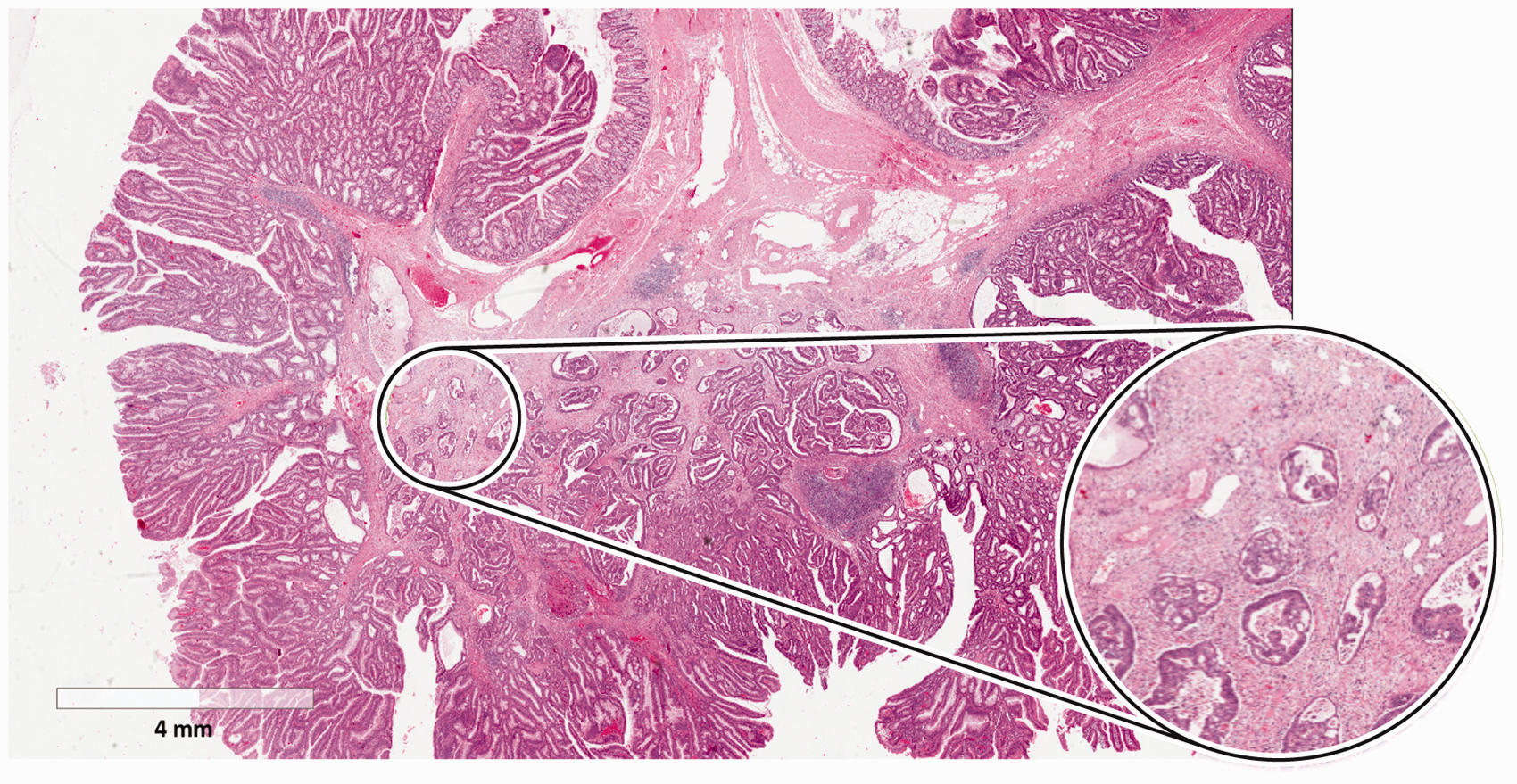
Scoring of the TSR was performed according to the standard procedure described by Van Pelt et al. 25 In short, tissue samples consisting of 4 μm H&E slides from the invasive part of the primary tumour were scanned at 40× magnification using a NanoZoomer-XR (Hamamatsu Photonics, Hamamatsu, Japan) and digitalised; saved images were viewed using Aperio Imagescope v12.2 (Leica Microsystems, Wetzlar, Germany). The proportion of stroma was determined within an annotation of which the area was comparable to the field of vision when using a 20 mm ocular of a conventional microscope (3.14 mm2). Invasive tumour cells had to be present at all borders of the image field within the annotation (see Figure 1) to ensure that desmoplastic tumour stroma was included. Mucinous tissue within a field that matched the scoring criteria was visually excluded from scoring. The image field with the highest stromal proportion was decisive, that is, if there was only one field with a stroma-high score (which also met the aforementioned criteria), the tumour was scored as stroma-high. TSR scores were divided into ‘stroma-high’ (>50% stroma) and ‘stroma-low’ (≤50% stroma) as determined a priori to maximise the discriminative power. 13 Two investigators (H.D. and G.v.P.) assessed the TSR independently from each other. In case of an inconclusive score without consensus after discussion, a third observer was decisive (W.M.). All observers were blinded for the clinical characteristics and study outcomes.
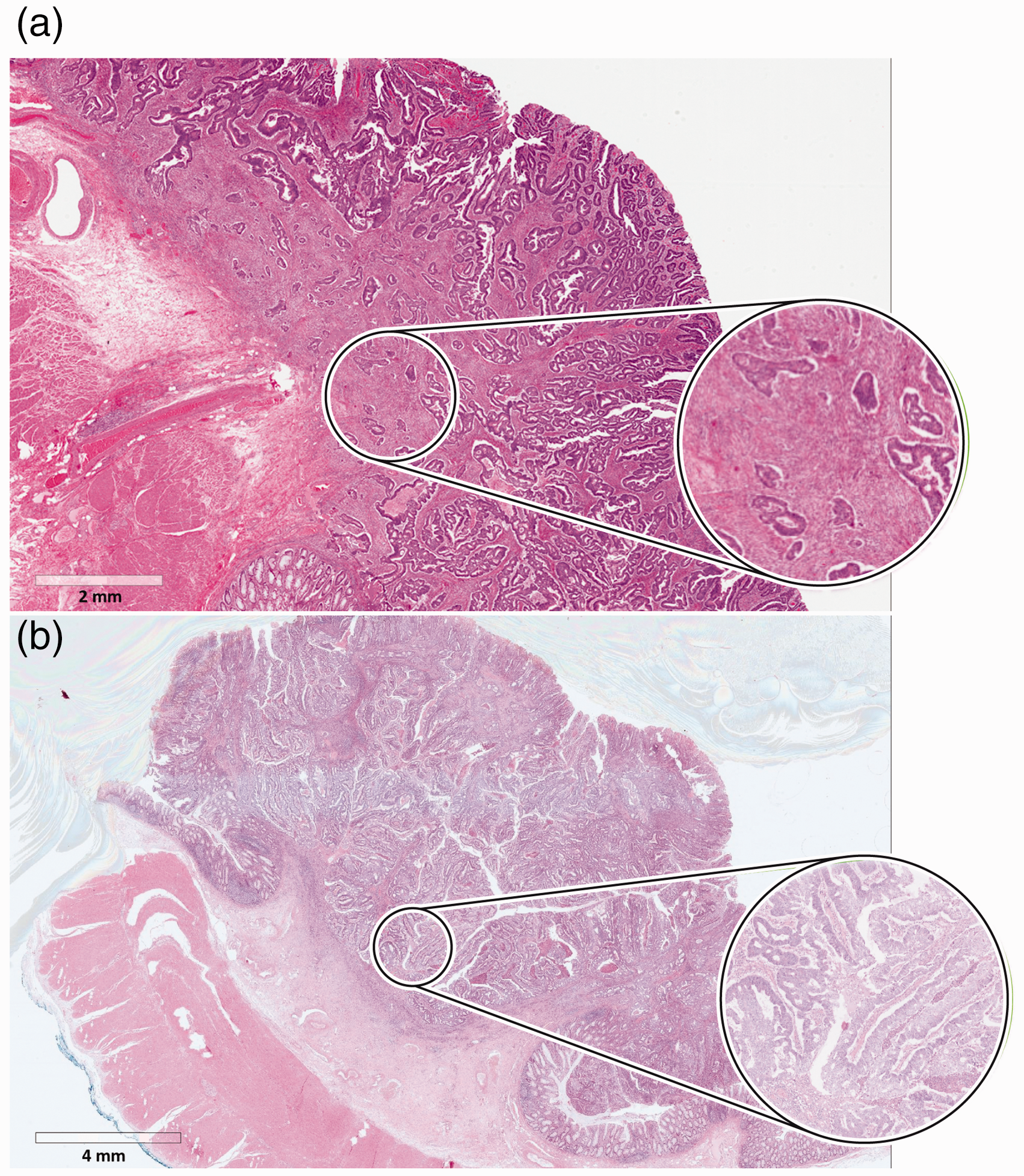
Representative images of the tumour–stroma ratio (TSR) scoring procedure, with examples of a stroma-high (a) and stroma-low (b) tumours.
Statistical analysis
Nominal and ordinal variables were expressed as frequencies and percentages, and continuous variables as medians and interquartile ranges (IQR). Pearson’s chi-square or Fisher’s exact test was used to compare categorical data, as appropriate. Continuous variables were compared using the Mann–Whitney U-test. Inter-observer agreement was expressed using Cohen’s kappa coefficient, with a κ-value of 0 being considered as complete disagreement, 0.0–0.2 as slight agreement, 0.21–0.40 as fair agreement, 0.41–0.60 as moderate agreement, 0.61–0.80 as substantial agreement and 0.81–1.00 as almost perfect agreement. 26
Kaplan–Meier survival curves were plotted to visualise survival estimates. A Cox proportional hazard approach weighted by Prentice’s method to account for the case-cohort sampling 27 was used to evaluate the association between the TSR and the primary end point. The Cox regression model was adjusted for the four aforementioned conventional risk factors. 2 Results of these models are reported as hazard ratios and 95% confidence intervals (CI).
R v3.6.2 (R Foundation for Statistical Computing, Vienna, Austria) and GraphPad Prism v8.01 (GraphPad Software, Inc., San Diego, CA) were used for statistical analysis and to draw figures, respectively. A two-sided p-value of <0.05 was considered statistically significant.
Results
TSR scoring
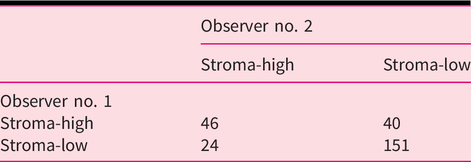
All 261 patients in the final case cohort had digitalised H&E slides available for TSR scoring, and were included in the analyses. In total, 183 (70.1%) were scored as stroma-low and 78 (29.9%) as stroma-high. Scores of 197 (75.5%) tumours were in concordance between the two assessors (Table 1). Consensus was reached after discussion in 51 (19.5%) cases; the third decisive observer was consulted in the remaining 13 (5.0%) cases. Cohen’s kappa coefficient revealed a moderate inter-observer agreement in classification (κ = 0.42).
Cross-table of the tumour–stroma ratio scores given by the two independent assessors.
Clinical characteristics of stroma-low and stroma-high T1 CRCs
Due to enrichment of the final case cohort with patients who reached the primary outcome, the random 50% sample from the baseline cohort was used to describe the characteristics of the two TSR groups. The clinical characteristics of this sub-cohort (n = 223) are shown in Table 2. The median age at the time of diagnosis was 70 years (IQR 65–77 years). The median tumour size was 25 mm (IQR 17–40 mm); most tumours were located in the left hemicolon (54.3%). A total of 49 (22.0%) patients underwent endoscopic tumour resection prior to surgery. The median number of retrieved lymph nodes was nine (IQR 4–12).
Clinical characteristics of the random 50% sample from the baseline cohort.
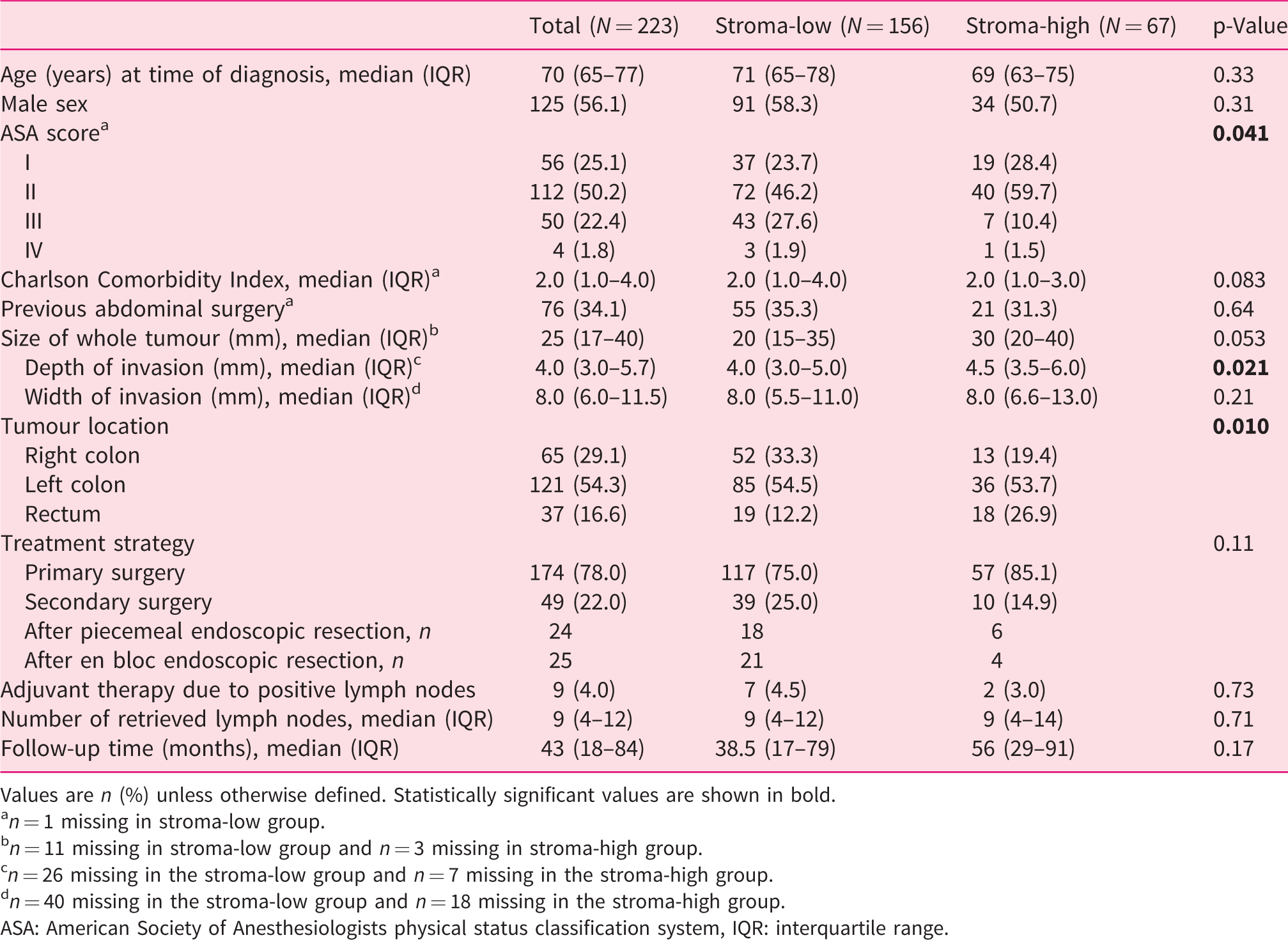
Values are n (%) unless otherwise defined. Statistically significant values are shown in bold.
an = 1 missing in stroma-low group.
bn = 11 missing in stroma-low group and n = 3 missing in stroma-high group.
cn = 26 missing in the stroma-low group and n = 7 missing in the stroma-high group.
dn = 40 missing in the stroma-low group and n = 18 missing in the stroma-high group.
ASA: American Society of Anesthesiologists physical status classification system, IQR: interquartile range.
The distribution of TSR scores in the random sub-cohort (stroma-low 70.0% vs. stroma-high 30.0%) was similar to that of the final case-cohort. Compared with stroma-low T1 CRCs, stroma-high tumours were more often located in the rectum (p = 0.010). The invasion depth of stroma-high T1 CRCs was also greater than that of stroma-low tumours (median depth 4.5 vs. 4.0 mm; p = 0.021).
The association between TSR score and the four conventional high-risk factors is shown in Figure 2. Due to an incomplete invasive front, tangential cutting or coagulation artefacts, the differentiation grade could not be determined in two patients, invasion depth could not be determined in 24 patients, lymphovascular invasion could not be determined in three patients and tumour budding could not be determined in 10 patients. High-grade tumour budding was more often found in stroma-high tumours (stroma-high 37.5% vs. stroma-low 22.1%; p = 0.075). No statistically significant association was found between TSR scores and the other three conventional histological high-risk factors.
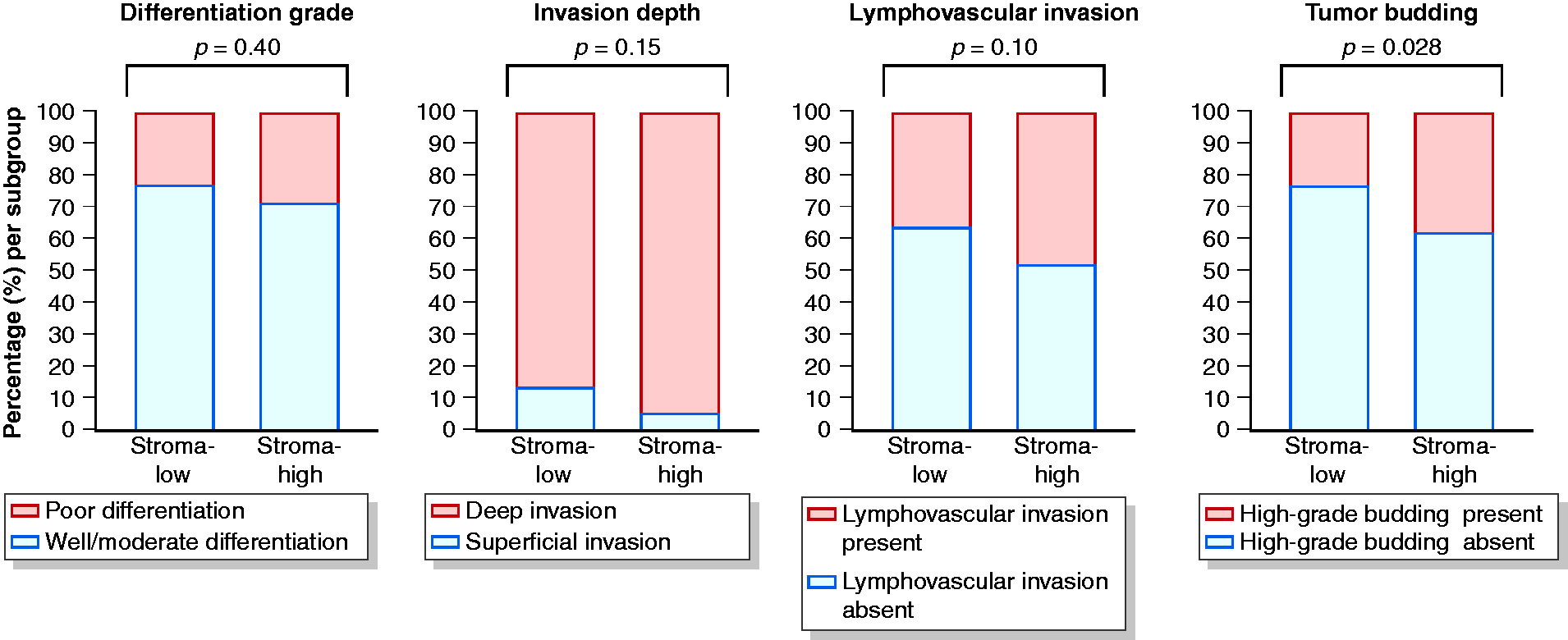
Association between TSR scores and conventional histological high-risk factors.
Association with adverse outcome in the final case-cohort
In total, 47/183 (25.7%) stroma-low (30 LNM, 14 recurrence, 3 both) and 16/78 (20.5%) stroma-high patients (11 LNM, 3 recurrence, 2 both) had an adverse outcome (see Figure 3 for Kaplan–Meier curve). Prentice’s weighted Cox regression showed that stroma-high tumours were not significantly associated with an increased risk for an adverse outcome (HR = 0.73, 95% CI 0.42–1.29; p = 0.28). A comparable risk was observed when adjusting for the aforementioned histological high-risk factors (HR = 0.66, 95% CI 0.37–1.18; p = 0.16).
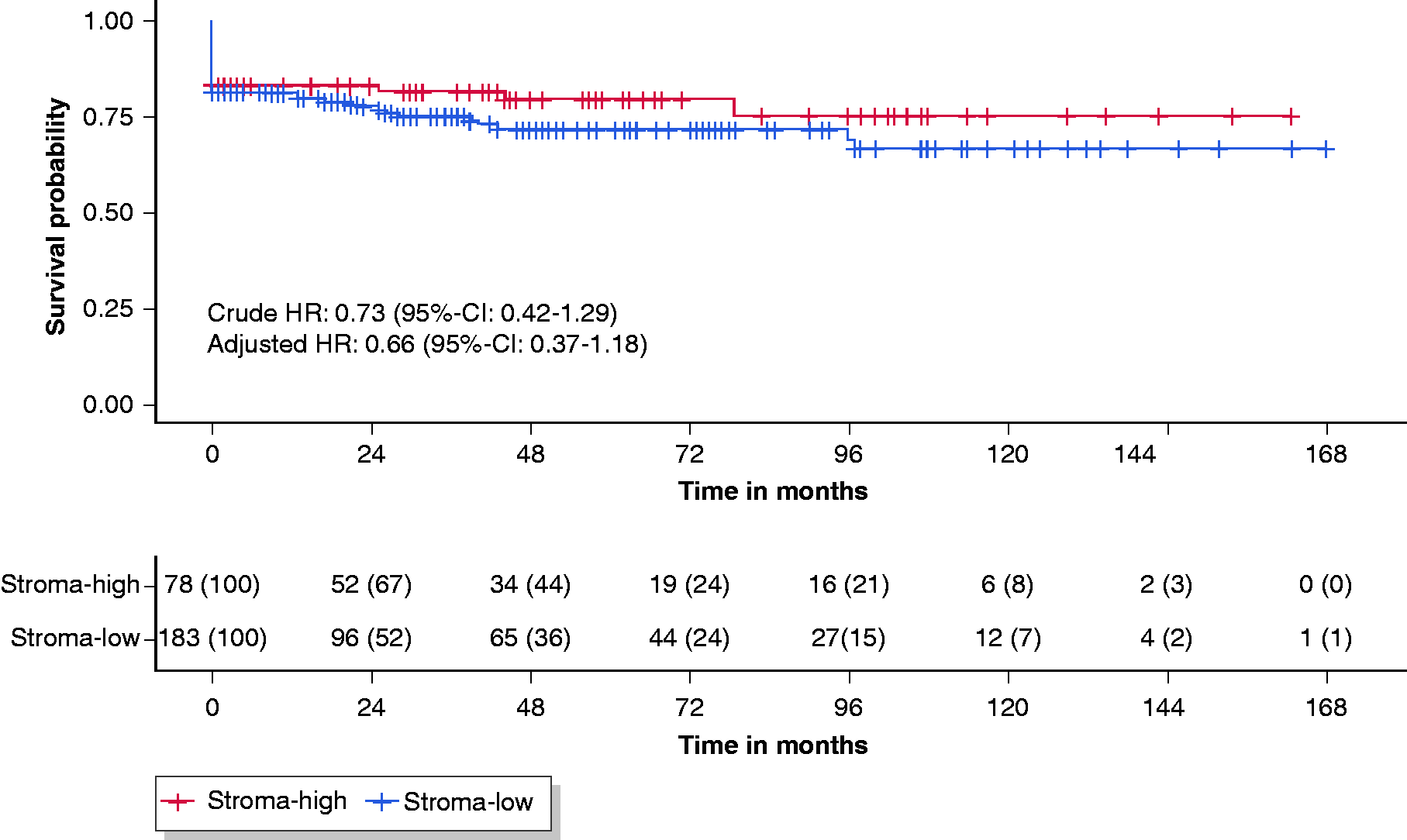
Kaplan–Meier survival curves of the stroma-low and stroma-high group. For calculation of the hazard ratios (HR), the reference group was stroma-low T1 colorectal cancers (CRCs).
Discussion
With the increasing number of T1 CRCs being detected due to the introduction of CRC screening programmes, the need for more accurate discrimination between prognostically favourable and unfavourable tumours is increasing. To our knowledge, this is the first study to evaluate the prognostic value of the TSR in a large multi-centre case cohort of T1 CRC patients. However, in contrast to previous studies in more advanced (>T1) stages of CRC,13–18 we found no statistically significant association between TSR scores and adverse outcome, indicating that the TSR did not have prognostic value in T1 CRC patients.
A biological explanation for our finding could be that in T1 CRCs, the TSR not only measures desmoplastic tumour stroma, but also takes into account reactive stroma which was not tumour associated. Under physiological conditions, the intestinal epithelium is subject to various mechanical (peristalsis, faecal stream) or erosive (invasive bacteria, chemical agents) stimuli which can damage the structural integrity of this layer. These injuries can initiate a wound-healing response 28 – a process which very much resembles the formation of desmoplastic tumour stroma. 29 We hypothesise that stromal expansion in T1 CRCs can be caused by physiological and tumour-induced processes, as superficially invasive tumours are more prone to the aforementioned stimuli compared to more deeply invasive CRCs. This hypothesis may be reflected by our finding that stroma-high T1 CRCs were more often located in the rectum, where mechanical forces caused by accumulation of faeces play an important role. Unfortunately, it is not possible to discriminate between physiological and tumour-induced stromal expansion on histology. As a result, TSR scores in T1 CRCs may overestimate the amount of desmoplastic stroma, leading to a considerable decrease of the prognostic value of the TSR. Considering the estimated hazard ratio of <1, this overestimation even seems to be so substantial that the prognostic effect of a high stromal content – as reported in patients with more advanced desmoplastic CRCs – could be completely reverted in T1 CRC patients. In line with our hypothesis, post hoc analyses stratified on anatomical location showed that overestimation of the amount of desmoplastic stroma appeared to be more pronounced in rectal T1 CRCs (adjusted HR = 0.28, 95% CI 0.06–1.30; p = 0.10) than in colonic T1 CRCs (adjusted HR = 0.69, 95% CI 0.35–1.35, p = 0.28).
Interestingly, several studies have shown that similar to the TSR, other parameters known to be strongly prognostic in patients with advanced-stage CRC (Immunoscore, CMS classification, MSS/MSI status, molecular testing of KRAS, BRAF and TP53 etc.) were also of limited use in predicting prognosis in T1 CRC patients. 20 , 30 , 31 These results suggest that caution should be taken in extrapolating such prognosticators to this specific patient group, possibly due to several distinct biological characteristics of T1 CRCs. In order to improve risk stratification in T1 CRC patients, we suggest that T1 CRC-tailored prognosticators should be developed through translational studies in T1 CRCs.
It is believed that the prognostic power of the TSR is mainly explained by the fact that it accurately reflects the probability of having certain subsets of stromal cells, which are mechanistically involved in cancer progression. 6 Numerous studies have shown that stromal cell populations – and in particular cancer-associated fibroblasts (CAFs), the major component of the tumour stroma – can affect CRC progression. This occurs via mechanisms such as the secretion of growth factors that affect cell motility or by facilitating escape to lymphatic or blood vessels through remodelling of the extracellular matrix. 19 , 32 , 33 Moreover, CAF-based biomarkers can also predict disease outcome in the advanced stages of CRC: several studies have shown that a small number of genes expressed in CAFs is sufficient to identify patients with a poor prognosis.34–38 Considering the aforementioned issues and findings, we hypothesise that an in-depth analysis of stromal cell populations/CAFs in T1 CRC may lead to identification of more accurate prognosticators. For example, unbiased single-cell profiling of these populations may be used to distinguish CAFs which are mechanistically involved in cancer progression from fibroblasts which are mainly involved in the physiological wound-healing response. These ‘physiological’ fibroblasts could resemble one or more of the normal fibroblast subsets described by Kinchen et al., which were enriched for extracellular matrix–related processes. 39 Due to the stage-dependent phenotypic heterogeneity of CAFs 19 , 32 and the lack of studies on CAFs in T1 CRCs, it is difficult to speculate on which (subsets of) CAFs may be present in the T1 CRC stroma and may exhibit prognostic potential.
One of the limitations of our study was that a considerable number of patients had fewer than 10 surgically retrieved lymph nodes, which is associated with an increased risk of recurrence. 40 To circumvent this issue, we therefore used a composite outcome which includes both LNM at baseline and (local or metastatic) CRC recurrence during follow-up. Second, several limitations of the TSR scoring procedure in T1 CRCs should also be acknowledged. For example, stroma-high tumours may have been misclassified into the stroma-low category due to the relatively small size of the invasive component of T1 CRCs. With commonly used (18–22 mm) oculars in conventional microscopy, the field of vision in which the TSR is scored has a diameter of around 2 mm. However, for a considerable proportion of our T1 CRC cohort, the depth or width of the invasive component of the tumour was barely larger than the diameter of the field of vision. This may have resulted in fewer fields of vision which meet one of the scoring criteria (i.e. including tumour cells at all four borders of the selected image field; see Figure 4). Another point of concern is the relatively low level of inter-observer agreement (κ = 0.42; mostly reported to be >0.8). 6 Explanations for this finding are unlikely to be related to one of the observers, as analyses stratified on the scores of each individual observer yielded comparable non-significant results (data not shown). A more likely explanation relates to the criterion that only one image field with a stroma-high score was sufficient for a tumour to be scored as stroma-high. Although it is unclear how often this occurs in more advanced-stage tumours and to what extent it influences the inter-observer variability, our data show that disagreement occurs more often in stroma-high tumours which were scored based on this criterion (23/39 (59.0%) vs. 9/39 (23.1%), p = 0.003). In addition, in 17/33 (51.5%) cases with inter-observer disagreement which were eventually scored as stroma-low, the underlying reason for disagreement was a supposed stroma-high field which turned out not to meet the scoring criteria after discussion. Unfortunately, the aforementioned issues cannot be easily solved because a priori adjustments of the standardised TSR scoring procedure 25 require validation in independent cohorts, whereas a posteriori adjustments can introduce bias to the study results and thus require extensive validation even more.
Representative example of a T1 CRC, which was scored as stroma-high based on one image field with a stroma-high score.
Conclusion
In conclusion, we did not find a statistically significant association between the TSR and adverse outcome in a large multi-centre case cohort of patients with non-pedunculated T1 CRCs. Our study further emphasises that existing prognosticators may not be simply extrapolated to T1 CRCs, even though their prognostic value has been widely validated in more advanced-stage tumours.
Supplemental Material
sj-pdf-1-ueg-10.1177_2050640620975324 - Supplemental material for Tumour–stroma ratio has poor prognostic value in non-pedunculated T1 colorectal cancer: A multi-centre case-cohort study
Supplemental material, sj-pdf-1-ueg-10.1177_2050640620975324 for Tumour–stroma ratio has poor prognostic value in non-pedunculated T1 colorectal cancer: A multi-centre case-cohort study by Hao Dang, Gabi W van Pelt, Krijn JC Haasnoot, Yara Backes, Sjoerd G Elias, Tom CJ Seerden, Matthijs P Schwartz, Bernhard WM Spanier, Wouter H de Vos tot Nederveen Cappel, Jeroen D van Bergeijk, Koen Kessels, Joost MJ Geesing, John N Groen, Frank ter Borg, Frank HJ Wolfhagen, Cornelis A Seldenrijk, Mihaela G Raicu, Anya N Milne, Anja UG van Lent, Lodewijk AA Brosens, G Johan A Offerhaus, Peter D Siersema, Rob AEM Tollenaar, James CH Hardwick, Lukas JAC Hawinkels, Leon MG Moons, Miangela M Lacle, Wilma E Mesker, Jurjen J Boonstra and on behalf of the Dutch T1 CRC Working Group in United European Gastroenterology Journal
Footnotes
Acknowledgements
The original case cohort was funded by a grant from the Dutch Digestive Diseases Foundation (reference number MG/2015-040).
Declaration of conflicting interests
J.J.B. is a consultant of Boston Scientific. All other authors declare no potential conflicts of interest.
Ethics approval
▪
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethics approval
This study was approved by the Medical Ethics Committee of the Leiden University Medical Centre (reference number G17.078, date of approval 20 December 2017).
Informed consent
Informed consent of the participating patients was waived by the Medical Ethics Committee of the Leiden University Medical Centre (reference number G17.078, date of approval 20 December 2017).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.