
Abstract
Background
Predicting severe acute pancreatitis (AP) in the early clinical stage is important for low morbidity and mortality. Delta neutrophil index (DNI) is used to detect infection and inflammation, but no previous studies have evaluated the usefulness of DNI as an early predictor of progression to severe AP (SAP).
Methods
The medical records of patients who were diagnosed with AP at the emergency department (ED) of Wonju Severance Christian Hospital from January 2012 to August 2016 were retrospectively reviewed. The initial DNI obtained in the ED was compared with other inflammatory markers to predict SAP. Multivariate logistic regression was used for statistical analysis.
Results
Of the 209 cases included in the analysis, 13 were classified as SAP. Compared to the DNI of the mild to moderately SAP group, that in the SAP group was considerably higher. The DNI showed a positive correlation with the Atlanta classification and bedside index of severity in AP. Using multivariate logistic regression analysis, DNI was an independent predictor of early SAP detection (odds ratio 1.122, 95% CI 1.045–1.205, p = 0.001). Among the biomarkers, DNI had the highest predictive value for SAP.
Conclusions
The DNI measured in the ED at presentation is a potentially useful adjunctive marker to predict SAP.
Key summary
Delta neutrophil index (DNI) strongly correlates with manual immature granulocyte count and precedes change in absolute white blood cell (WBC) or neutrophil count because the course of granular leukocyte differentiation in infectious and inflammatory conditions begins with immature granulocyte formation. In this study of 209 patients, DNI had the highest predictive value for severe acute pancreatitis (SAP) among the biomarkers, including WBC and C-reactive protein. Therefore, DNI measured in the emergency department upon presentation has potential as an adjunctive marker for prediction of SAP.
Introduction
The incidence of acute pancreatitis (AP) has been increasing, and the primary problem in affected patients is inflammation, which results in a variety of clinical outcomes. 1 Over 200,000 patients are hospitalized each year for AP in the United States. 2 AP usually presents in a mild form, and most patients have an uneventful recovery without organ dysfunction. However, about 10–20% of patients with AP progress to a severe form, which can be life-threatening. 3 AP patients may deteriorate and ultimately require critical care in the intensive care unit (ICU) within the first 24–48 hours of hospitalization. 4 Therefore, an initial indicator of disease severity is important to predict the clinical course of AP, because recognizing severe AP (SAP) in the early clinical phase can lower mortality by adequately applying proper critical care.5,6
There are several scoring systems to screen patients at risk for SAP.7–10 The Atlanta classification, a global representative classification of AP, was revised in 2012 based on an international consensus.7–11 C-reactive protein (CRP), procalcitonin and interleukin-6 have been studied as possible biomarkers to predict the severity of AP at the initial clinical phase.12–14 However, simple and accurate biomarkers for early recognition of SAP are still needed. A convenient and cost-effective serum biomarker that predicts disease severity within the initial 24 hours of symptom onset is desirable.15–17
The delta neutrophil index (DNI) identifies the difference in leukocyte subfractions through a cytochemical myeloperoxidase reaction and a nuclear lobularity assay through blood cell analysis.18,19 DNI strongly correlates with manual immature granulocyte count. 19 The DNI can represent changes in absolute white blood cell (WBC) or neutrophil count because the course of granular leukocyte differentiation in inflammatory and infectious conditions starts with formation of immature granulocytes. 20 Therefore, DNI has been studied by several research groups as a serum biomarker in infectious and inflammatory conditions.19–21 In addition, DNI may serve as an efficient test to represent inflammation and infection in patients in the emergency department (ED) because DNI can be included with routine complete blood counts.22–24 No past studies have assessed the clinical efficacy of DNI as an initial biomarker of SAP in the ED. Therefore, we studied the clinical usefulness of DNI as an early indicator of disease progression to SAP in the ED.
Materials and methods
Study design
This is a retrospective observational study of patients with AP in the ED between January 2012 and August 2016. The study protocol was approved by the Institutional Review Board of Wonju Severance Christian Hospital (CR 317113) and follows the ethical guidelines of the Declaration of Helsinki (1975) and its later amendments. Patients’ medical records and information were anonymously collected before analysis, so the need for informed consent was waived.
Computerized hospital records were reviewed, and patients with a discharge code of “acute pancreatitis” according to the Tenth Revision of the International Statistical Classification of Diseases coding were considered for the initial study selection. Diagnosis of AP required that at least two of the following three criteria were met: (a) typical abdominal pain at presentation; (b) elevated serum amylase and/or lipase levels at least three times higher than the upper range of normal; and (c) characteristic imaging compatible with AP. 11 A total of 313 patients were diagnosed with AP in the study period. Upon diagnosis in the ED, AP was treated with patient fasting, intravenous fluids and pain control.
The study exclusion criteria were as follows: (a) age less than 18 years (n = 12); (b) acute exacerbation of chronic pancreatitis (n = 21); (c) AP caused by malignancy (n = 23); (d) post-endoscopic retrograde cholangiopancreatography pancreatitis (n = 19); (e) hematologic disorders; other concomitant infections and inflammations (n = 2); (f) transfer to other hospitals after evaluation in the ED (n = 26); and (g) insufficient data (n = 1).
Data collection
The following patient data was collected: age, sex, past medical history (hypertension, diabetes mellitus and liver cirrhosis), smoking, etiology of AP (gallstone, alcohol, hypertriglyceridemia and idiopathic), ICU admission, duration of hospital stay and mortality. Inflammatory markers (WBC, CRP (Cobas 8000, Roche, Basel, Switzerland) and DNI (ADVIA 2120i, Siemens Healthcare Diagnostics, Eschborn, Germany)), sodium, potassium, blood urea nitrogen, creatinine, hematocrit and arterial blood gas were measured in the ED. DNI was calculated automatically as the sum of immature granulocytes using parameters measured by the ADVIA 2120i: DNI = (% neutrophil + % eosinophil) – % polymorphonuclear leukocytes. 19
Scoring systems such as bedside index of severity in acute pancreatitis (BISAP) and acute physiology and chronic health examination (APACHE) II score were determined during the initial 24 hours of hospitalization.8,10 Parameters to calculate APACHE II score were extracted from the worst laboratory and vital sign measurements acquired from the first 24 hours of admission.
The revised Atlanta 2012 criteria were used to define the severity of AP. No sign of organ failure or systemic or local complication was classified as mild AP. A moderately SAP was diagnosed when transient organ failure resolved within 48 hours. Finally, persistent organ failure was classified as SAP in two or more of three organ systems (respiratory, cardiovascular and renal systems). Local complications comprised acute peripancreatic fluid collection, pancreatic pseudocyst, acute necrotic collection and walled-off necrosis. Aggravation of prior co-morbidities, such as coronary artery disease or chronic obstructive pulmonary disease, triggered by the AP was considered a systemic complication.
Study endpoints
The primary endpoint for this study was efficacy of DNI to predict SAP, as classified by the revised Atlanta classification, in patients in the ED.
Data analysis
Continuous variables are expressed as means and standard deviations or medians and interquartile ranges. Categorical variables are expressed as frequencies and percentages. For continuous variables, the significance of differences in AP severity according to variables of interest was assessed with the independent t-test or the Mann–Whitney U test. The chi-square test or Fisher’s exact test was utilized for categorical variables. Normality was assessed by the Shapiro–Wilk test. To assess the correlations between DNI and other scoring systems, Spearman’s correlation analysis was performed. After adjustments for confounding factors, the odds ratios for SAP were evaluated using univariate and multivariate logistic regression analyses. The accuracy of prediction power of SAP was determined by the area under the curve (AUC) using receiver operating characteristic (ROC) curves. AUC values were determined to compare the predictive abilities of all inflammatory markers evaluated in this study. Optimal cut-off values of the variables were estimated using ROC curves. The p-values < 0.05 were considered statistically significant. Analyses were performed using SPSS version 23 (IBM, Armonk, NY, USA) and MedCalc Statistical Software version 17.5.3 (MedCalc Software, Ostend, Belgium).
Results
Characteristics of the study participants
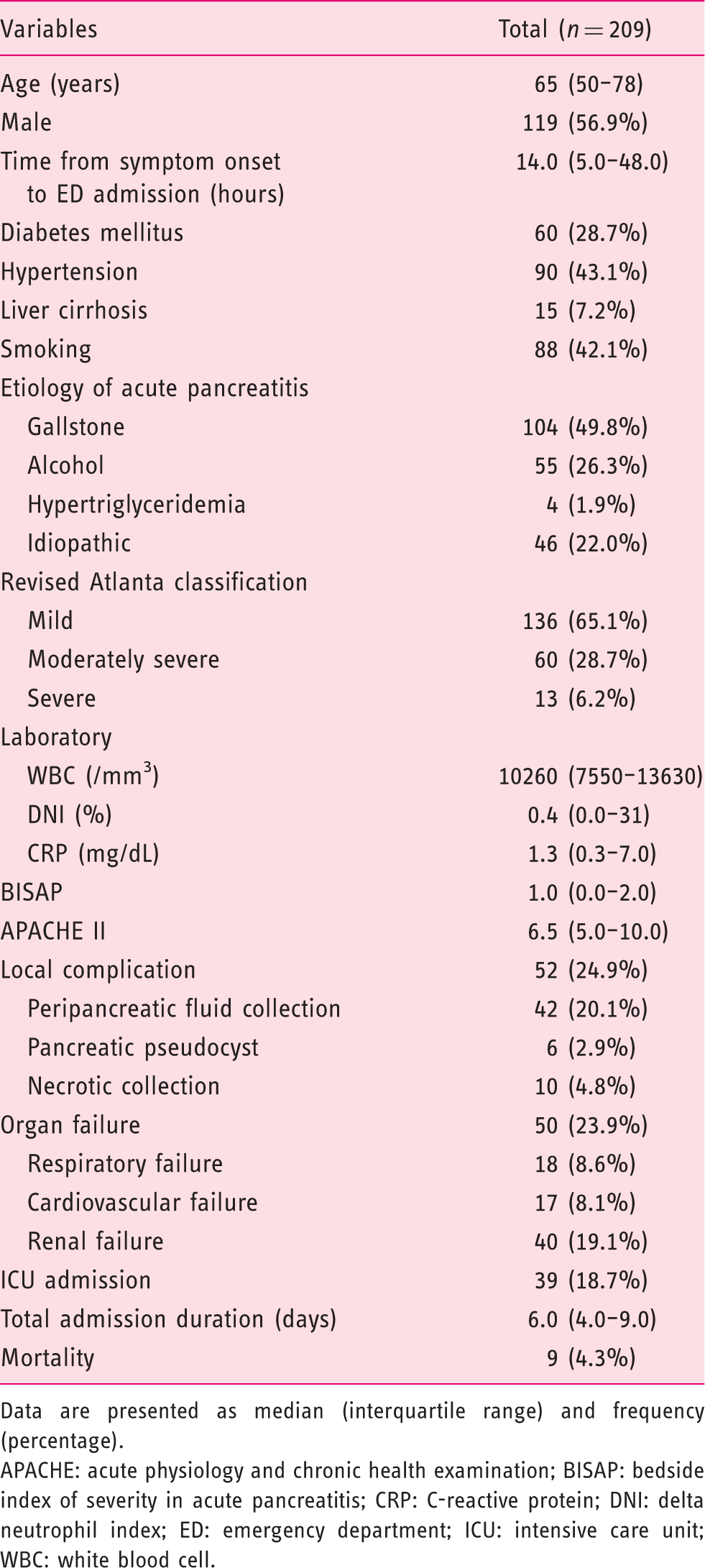
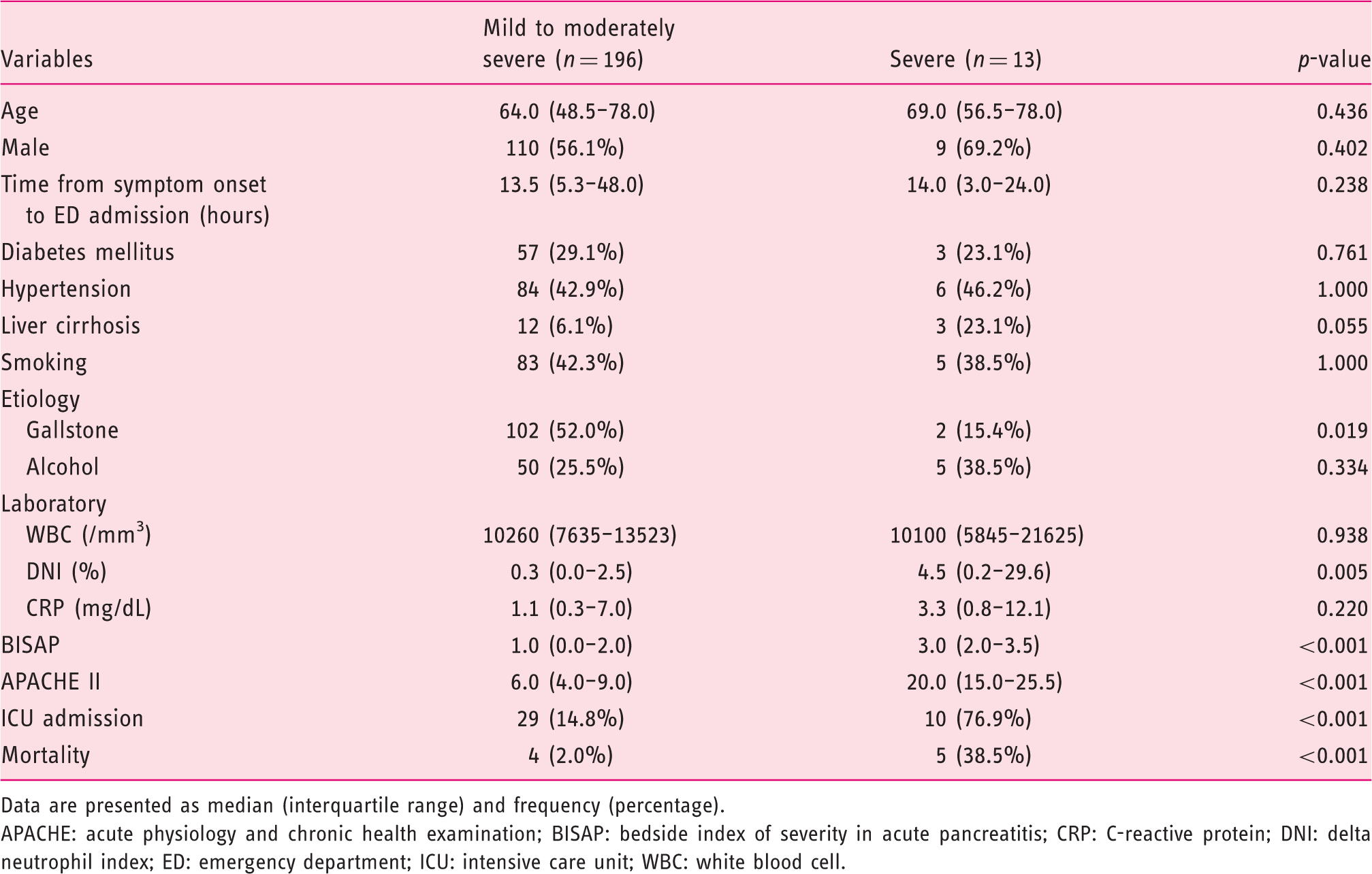
A total of 209 cases were included in this study. The median patient age was 65 years, and 56.9% of the participants were male. Ninety patients (43.1%) had hypertension, and 28.7% of the patients had diabetes mellitus. Gallstones (49.8%) were the most common etiology for AP, and alcoholic AP accounted for 26.3% of the total cases. SAP was diagnosed in 6.2% of patients. Median APACHE II and BISAP scores were 1.0 and 6.5, respectively. Median DNI and CRP values were 0.4% and 1.26 mg/dL, respectively. Nine patients (4.3%) died (Table 1). Patients in the SAP group had higher BISAP and APACHE II scores than patients in the mild to moderately SAP group. The SAP group had a significantly higher DNI than the mild to moderately SAP group (4.5 versus 0.3, p = 0.005) (Table 2 and Figure 1).
Box plot of white blood cell (WBC) counts, C-reactive protein (CRP) concentrations and delta neutrophil index (DNI) values by severity status of acute pancreatitis (AP). Baseline characteristics of patients with acute pancreatitis. Data are presented as median (interquartile range) and frequency (percentage). APACHE: acute physiology and chronic health examination; BISAP: bedside index of severity in acute pancreatitis; CRP: C-reactive protein; DNI: delta neutrophil index; ED: emergency department; ICU: intensive care unit; WBC: white blood cell. Comparison of clinical outcomes of patients with acute pancreatitis according to the severity of pancreatitis. Data are presented as median (interquartile range) and frequency (percentage). APACHE: acute physiology and chronic health examination; BISAP: bedside index of severity in acute pancreatitis; CRP: C-reactive protein; DNI: delta neutrophil index; ED: emergency department; ICU: intensive care unit; WBC: white blood cell.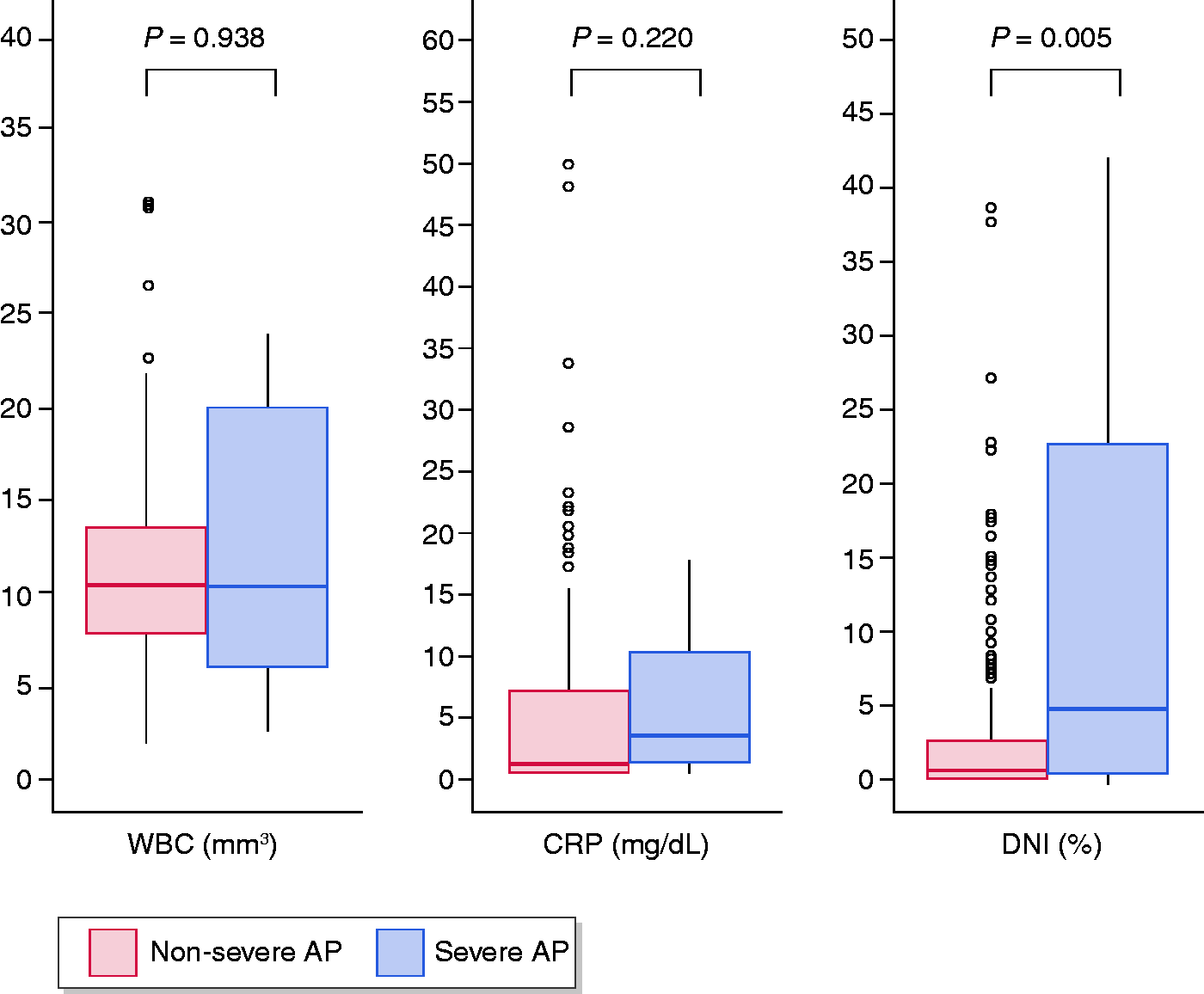
Predictive value of DNI in AP
Correlation between the delta neutrophil index and scoring systems.

Spearman’s correlation analysis was used.
APACHE: acute physiology and chronic health examination; BISAP: bedside index of severity in acute pancreatitis; CRP: C-reactive protein; DNI: delta neutrophil index.
Predictive factors for severe acute pancreatitis.
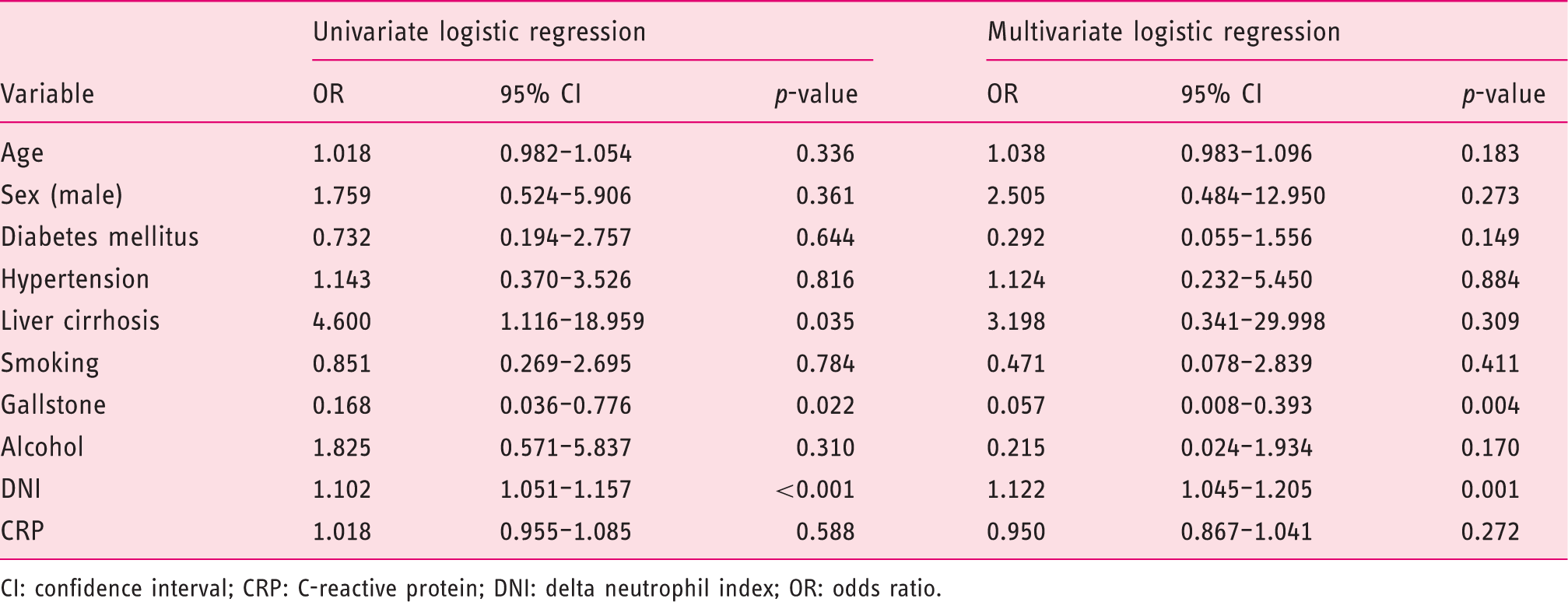
CI: confidence interval; CRP: C-reactive protein; DNI: delta neutrophil index; OR: odds ratio.
Diagnostic value of DNI in detecting subjects with SAP
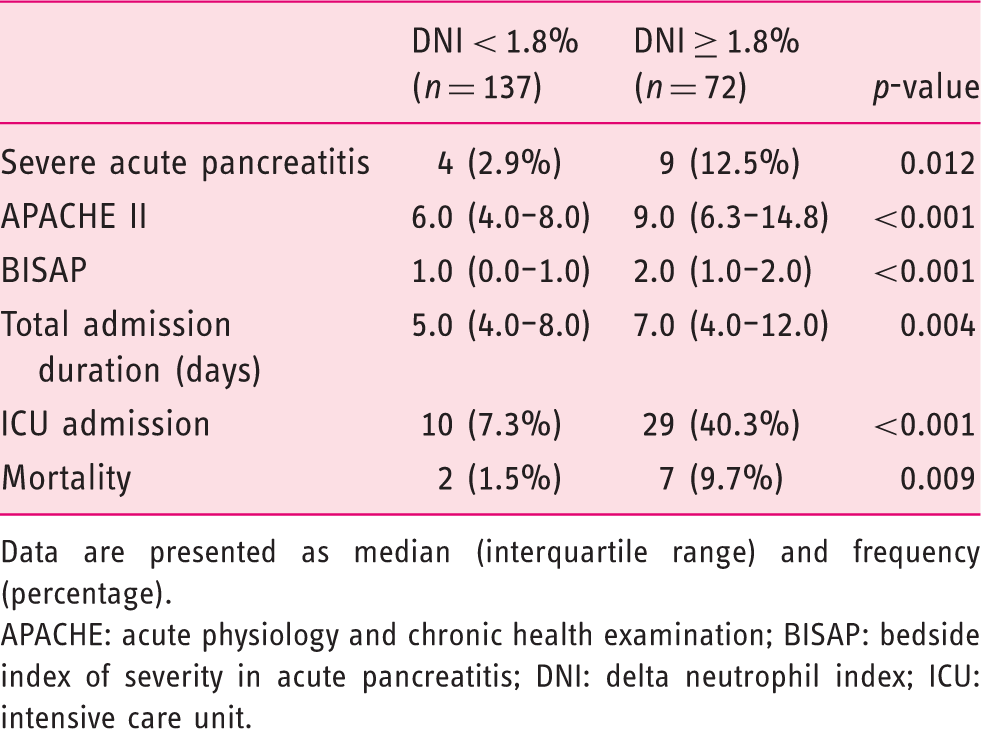
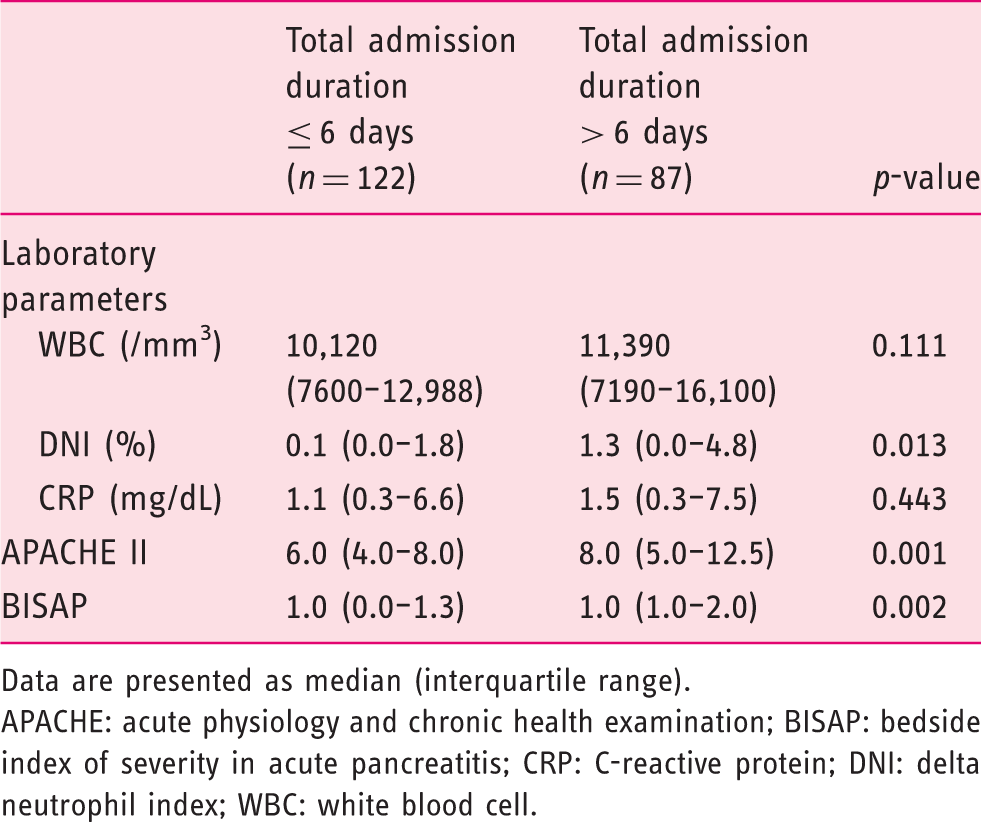
ROC curves were used to assess the predictive ability of WBC, DNI and CRP for SAP. The marker with the highest predictive ability was DNI (AUC 0.880, 95% CI 0.828–0.921, p < 0.001) (Figure 2). The optimum cut-off values for DNI and CRP were 1.8% (sensitivity 69.2%, specificity 67.8%) and 2.2 mg/dL (sensitivity 69.2%, specificity 61.2%), respectively. Further analysis of the relationships between DNI cut-off value and clinical variables was conducted. APACHE II and BISAP scores, total days of hospitalization, number of ICU days and mortality were considerably greater in the higher DNI group (DNI ≥ 1.8%) than the lower DNI group (DNI < 1.8%) (Table 5). Since the length of hospital stay is an important parameter in AP, the relationships between total duration of hospitalization and other markers/score systems were analyzed. DNI and APACHE II and BISAP scores were significantly higher in the longer total hospital stay group (> 6 days) than in the shorter total hospital stay group (≤ 6 days) (Table 6).
Receiver operating characteristic curve for predicting severe acute pancreatitis. The areas under the curve and 95% confidence intervals for indicators were 0.821 (0.762–0.870) for C-reactive protein (CRP), 0.880 (0.828–0.921) for delta neutrophil index (DNI) and 0.812 (0.752–0.863) for white blood cell (WBC). The model was adjusted for age, sex, diabetes mellitus, hypertension, liver cirrhosis, smoking status, gallstones and alcohol. The relationship between delta neutrophil index cut-off value and clinical parameters. Data are presented as median (interquartile range) and frequency (percentage). APACHE: acute physiology and chronic health examination; BISAP: bedside index of severity in acute pancreatitis; DNI: delta neutrophil index; ICU: intensive care unit. The relationship between total admission duration and inflammatory markers and scoring systems. Data are presented as median (interquartile range). APACHE: acute physiology and chronic health examination; BISAP: bedside index of severity in acute pancreatitis; CRP: C-reactive protein; DNI: delta neutrophil index; WBC: white blood cell.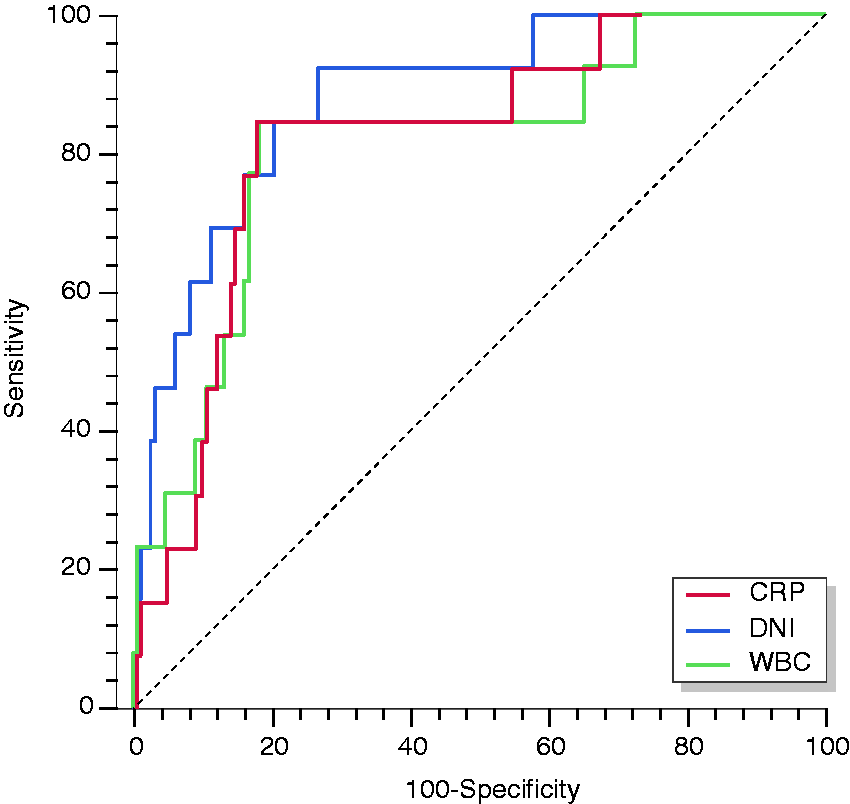
Discussion
We demonstrated that initial DNI obtained in the ED was an independent predictor of SAP. Among the biomarkers evaluated in this study, DNI had the highest predictive value for SAP. To the best of our knowledge, this study is the first to predict SAP using DNI.
There are multiple etiologies of the inflammation observed in AP. Activation of intra-acinar trypsinogen causes an acinar injury in the initial phase of AP. However, local and systemic inflammation occur independently in AP. 25 In addition, the inflammatory response and inflammatory mediators have important pathophysiologic roles in the clinical course of AP. 26 Autodigestion causes excessive transfer of leukocytes to the pancreas. 27 The leukocyte’s significant role is to release pro-inflammatory cytokines and oxygen-derived free radicals, which cause necrotic changes of the acinar.25,28 If these reactions continue, activated proteolytic enzymes and various inflammatory cytokines induce an acute respiratory failure, systemic inflammatory response syndrome, septic shock and multi-organ dysfunction.28,29 If the disease process resolves after the local inflammatory process, the disease will regress to mild AP.27,30 Thus, leukocytes are an important contributor to disease pathogenesis, progression and severity, and changes in DNI precede changes in absolute leukocyte count. 20 Therefore, DNI is a useful biomarker to predict SAP in early phase of AP.
The APACHE II scoring method is the most sensitive method currently available for assessing AP severity.31,32 However, it is complicated and time-consuming because it is composed of more than 14 items. Although the BISAP score is easier to use, 10 it has the disadvantage of not distinguishing between patients with temporary organ dysfunction and those with long-term organ dysfunction, and it can overestimate severity. The Atlanta classification is laborious and requires clinicians to reassess many factors 48 hours after the initial assessment. Therefore, early prediction of patients with higher risk of developing SAP is difficult with the conventional scoring systems. 11 However, DNI is easy to calculate in the ED since it can be simultaneously obtained with routine complete blood counts to evaluate inflammatory and infectious diseases. 24 DNI is a single, cost-effective, accurate and fast serum biomarker that can be used in the ED to identify patients in the early phase of pancreatitis with a higher risk of developing SAP.
CRP, which is produced by hepatocytes after inflammatory stimulation or stimulation by interleukin 1 and 6, has been shown to be a potential predictor of AP severity. 12 However, CRP is only reliable 48 hours after symptom onset because it has a delay of up to 72 hours. Comparing the time of symptom onset to presentation in the ED, there is no significant difference between patients with SAP and those with mild to moderately SAP. Therefore, CRP has the potential weakness of not reliably detecting SAP in its early stages.33,34 The DNI can predict initial change in leukocytes. Among various serum inflammatory markers analyzed in this study, only DNI was a predictor of SAP. From the study conducted by Huh et al., serum CRP, when measured during the early stages of AP, is not an independent predicting factor to detect SAP. 16
There were several limitations in this study. First, because of the retrospective design and single-center study setup, some data, such as subjective symptoms and physical examinations, were missing and/or inaccurate. Additionally, a selection bias could have resulted from patient exclusion. To reduce possible bias, we included all patients with AP who visited the ED and were admitted to this hospital because the DNI was available for all these patients. Second, DNI values were not serially assessed after admission, so we were unable to assess the meaning of changes in DNI for predicting treatment response. Third, we did not investigate serum procalcitonin, which is a relatively accurate and simple biomarker for predicting SAP.35,36 We did not use Ranson’s criteria because they include several factors that have to be measured, and severity cannot be determined until 48 hours after admission, limiting their use in the ED. 31 We also did not calculate computed tomography severity index, which can be evaluated by Balthazar grade and presence of necrosis. 9 However, this index focuses on local complications and does not represent a systemic inflammatory response. Despite these limitations, this study has strengths. This is the first study to evaluate the predictive value of DNI in AP. Because DNI can be quickly and conveniently calculated, it can easily be used in an ED setting. However, future prospective studies are needed to confirm the outcomes.
In conclusion, DNI measured at presentation in the ED has the potential to function as an adjunctive marker for prediction of SAP. Intensive care and careful management should be considered for AP patients with a DNI value greater than 1.8% upon presentation to the ED.
Supplemental Material
Supplemental material for Delta neutrophil index as an early predictive marker of severe acute pancreatitis in the emergency department
Supplemental Material for Delta neutrophil index as an early predictive marker of severe acute pancreatitis in the emergency department by Tae Y Kim, Sun J Kim, Yoon S Kim, Jong W Lee, Eung J Park, Seok J Lee, Kyong J Lee and Yong S Cha in United European Gastroenterology Journal
Footnotes
Declaration of conflicting interests
The authors have no conflicts of interest to disclose.
Ethics approval
The study protocol was approved by the International Review Board for Human Research (approval no. CR 317113) of Wonju Severance Christian Hospital.
Funding
This study was supported by the National Research Foundation (NRF) of Korea funded by the Korea government (Ministry of Science, ICT and Future Planning) (grant nos. NRF-2016R1C1B1007909 and NRF-2017R1C1B5017695).
Informed consent
The need for informed consent was waived due to the retrospective nature of this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.