
Abstract
Background and objective
Tumor size is an important prognostic factor in cancers. This study aims at investigating the interaction between gender status and tumor size to evaluate cancer-specific survival (CSS) in hepatocellular carcinoma (HCC).
Methods
In this study, we searched Surveillance, Epidemiology, and End Results (SEER) population-based data and identified 38,368 patients diagnosed with HCC between 1988 and 2012. Patients diagnosed between 1998 and 2007 were distributed into a training set (n = 19279), and the rest were assigned as a SEER validation set (n = 19089). Definition of cut-off value of tumor size stratified by gender was determined by the “X-Tile” program. The five-year CSS data were found. Long-term survival outcomes and risk factors were analyzed by the Kaplan–Meier methods and the multivariable Cox regression models.
Results
There were significant differences among these different tumor size subgroups with regards to five-year CSS (p < 0.001). When applying cutoff points of 38 mm and 75 mm tumor size in men, and 38 mm and 55 mm in women, the most significant difference was observed by the X-Tile program, respectively (p < 0.001). The five-year CSS was 27.5% for women and 25.7% for men in the training set, and 33.9% for women and 31.1% for men in the validating set (p < 0.001). Further analysis showed that this significant difference existed in localized, regional, and distant-stage patients.
Conclusions
These results demonstrated that women with HCC appeared to exhibit better survival rates than men. The sex-related discrepancies should be emphasized, particularly for HCC patients with 39 to 75 mm tumors.
Key summary
1. Summarize the established knowledge on this subject:
Hepatocellular carcinoma (HCC) is the fifth most common malignancy worldwide and the third leading cause of cancer-related death globally. HCC displays a markedly sex disparity and mainly affects men more than women. 2. What are the significant and/or new findings of this study?
Tumor size is an important prognostic factor in HCC. Women with HCC appear to have better survival rates than men. Patients with 39 to 75 mm tumors have different prognoses in different genders.
Introduction
Liver cancer (including hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma as well as other rare types) was predicted to be the sixth most common malignancy and the fourth leading cause of cancer death in 2018. 1 HCC is closely associated with a history of chronic hepatitis caused by hepatitis B or C virus (HBV or HCV).2–4 Over the last few years, trends in HCC have shown significant increases. 5 In 2013, an estimated 7920 women and 22,720 men in the United States (US) were diagnosed with primary liver cancer. 6 This malignancy displays a significant gender disparity and mainly affects men more than women.7,8 The male-to-female ratio averages between 2:1 and >4:1 in different analyses. 9 Recently, the role of estrogen has gained considerable attention, and it has also provided new insight into HCC development. 10 In addition, cirrhosis progress to HCC is thought to occur more frequently in men and postmenopausal women, suggesting that sex hormones might play an important role in the gender difference in the incidence of HCC. 11
Tumor size is a known independent prognostic factor for HCC.12–14 Hence, most staging systems are based on tumor size, and increased tumor size is closely correlated with decreased cancer-specific survival (CSS). 15 In particular, tumor size correlates with survival in men and women may be different. Given the growing importance of sex-related discrepancies in tumor size, we used date from the Surveillance, Epidemiology, and End Results (SEER) program to identify the impact of gender and tumor size on HCC prognosis.
Materials and methods
Patients
The SEER database provides information on 18 population-based cancer statistics in an effort to reduce the cancer burden among the US population. According to the Site Recode Classifications, we extracted cases of invasive liver cancer (C22.0) from the SEER database. These cases were diagnosed between 1988 and 2012. Then, we expanded morphology codes for liver cancer. Those patients without histological type, incomplete staging or follow-up were excluded. Meanwhile, we also assessed variables for these patients including age, race, sex, stage, histologic type, tumor grade and size, as well as CSS rates between age 18 and 85 years at diagnosis. The primary end point of the study was five-year CSS rate. We obtained access to the SEER database public data file numbered 10504-November 2014.
Statistical analyses
Data are expressed as mean ± SEM, or as absolute number or percentage for categorical variables.
We used different ways to analyze and evaluate different targets: the chi-squared (χ2) test for evaluating the relationship between gender categories and clinicopathological parameters, the Student t-test for comparing continuous variables, the Kaplan–Meier method for generating survival curves, the log-rank test for analyzing differences between the curves, and the Cox proportional-hazards model for assessing survival outcomes and risk factors. P values ≤0.05 were considered significant. All statistical analyses were performed using the statistical software package SPSS for Windows, version 17 (SPSS, Inc).
Results
Patient characteristics
Characteristics of patients from SEER database by gender.
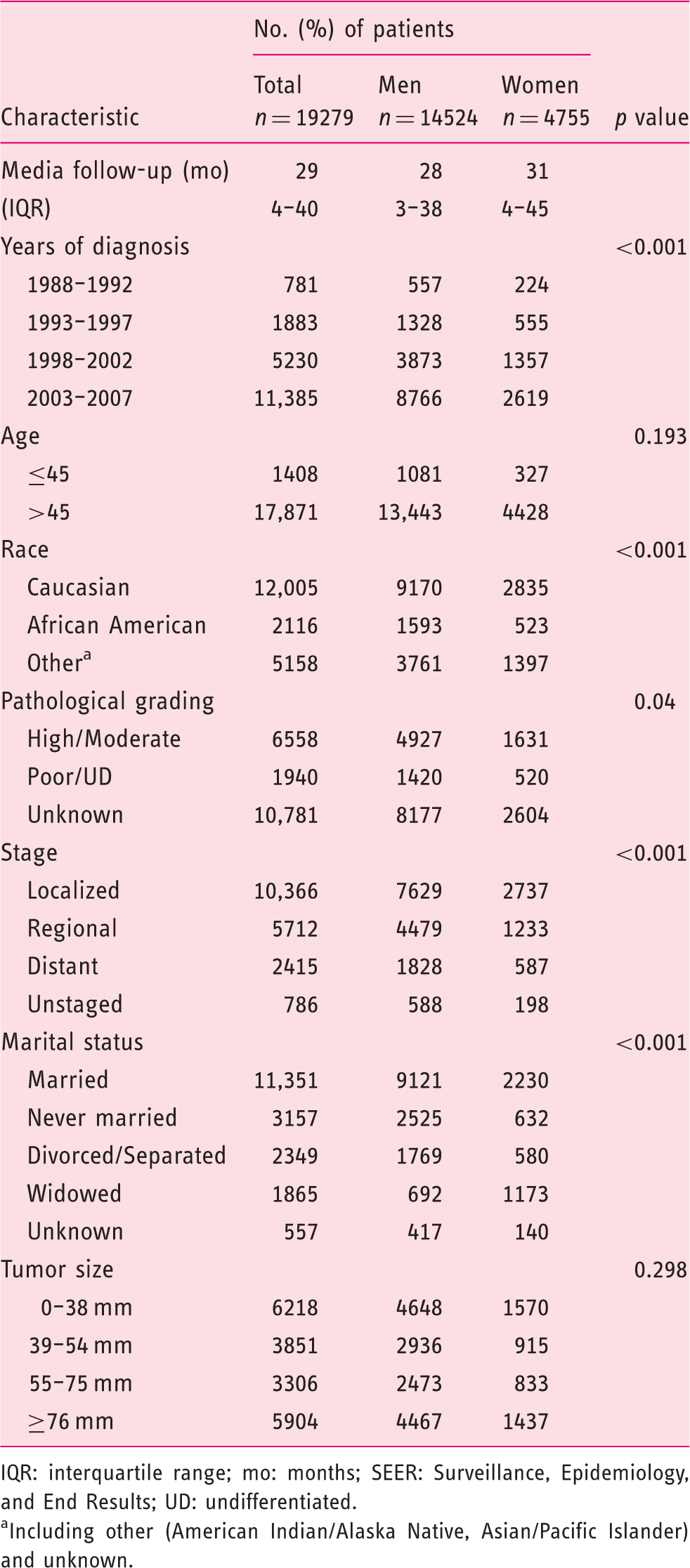
IQR: interquartile range; mo: months; SEER: Surveillance, Epidemiology, and End Results; UD: undifferentiated.
Including other (American Indian/Alaska Native, Asian/Pacific Islander) and unknown.
Identification of cutoff points of tumor size stratified by gender
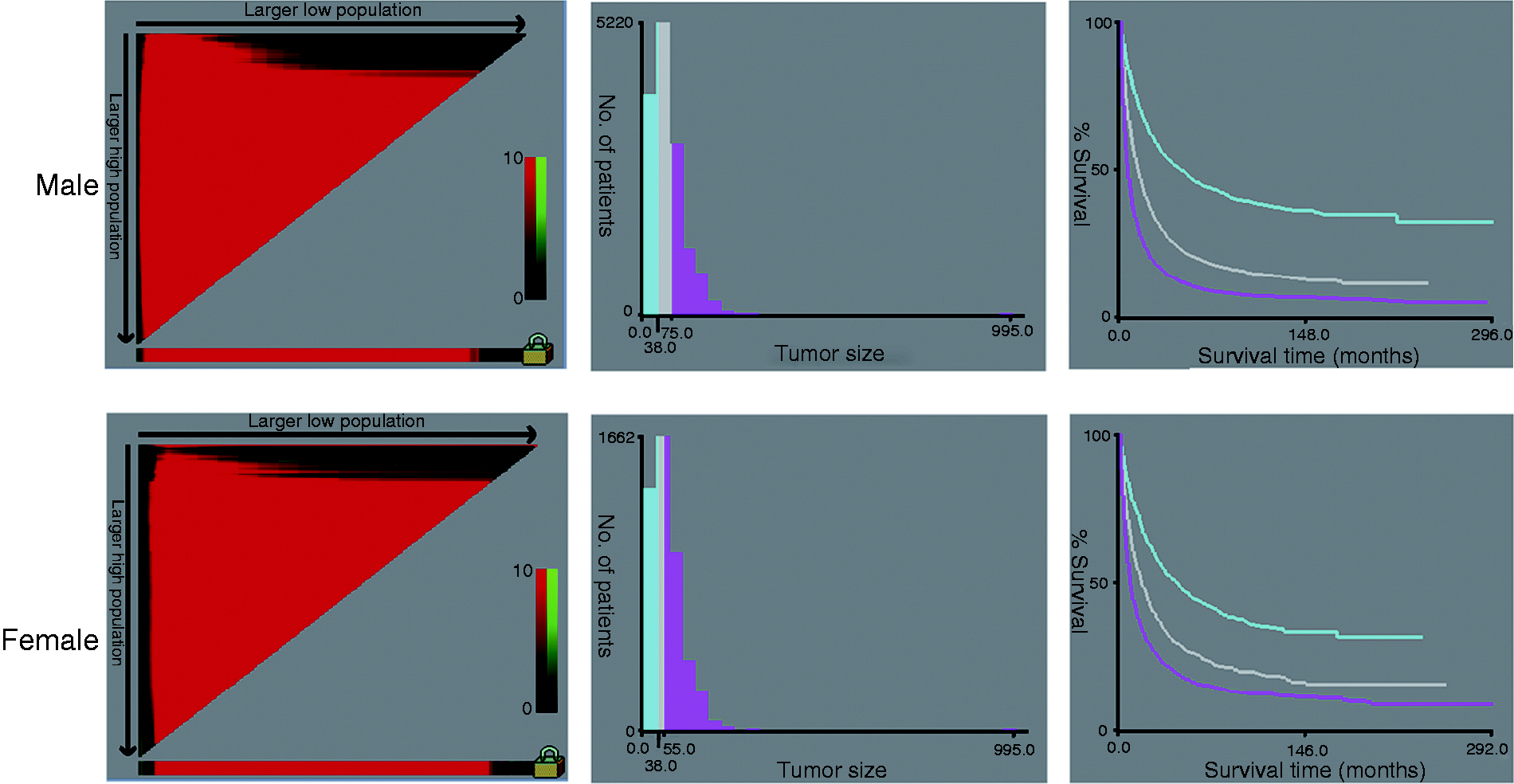
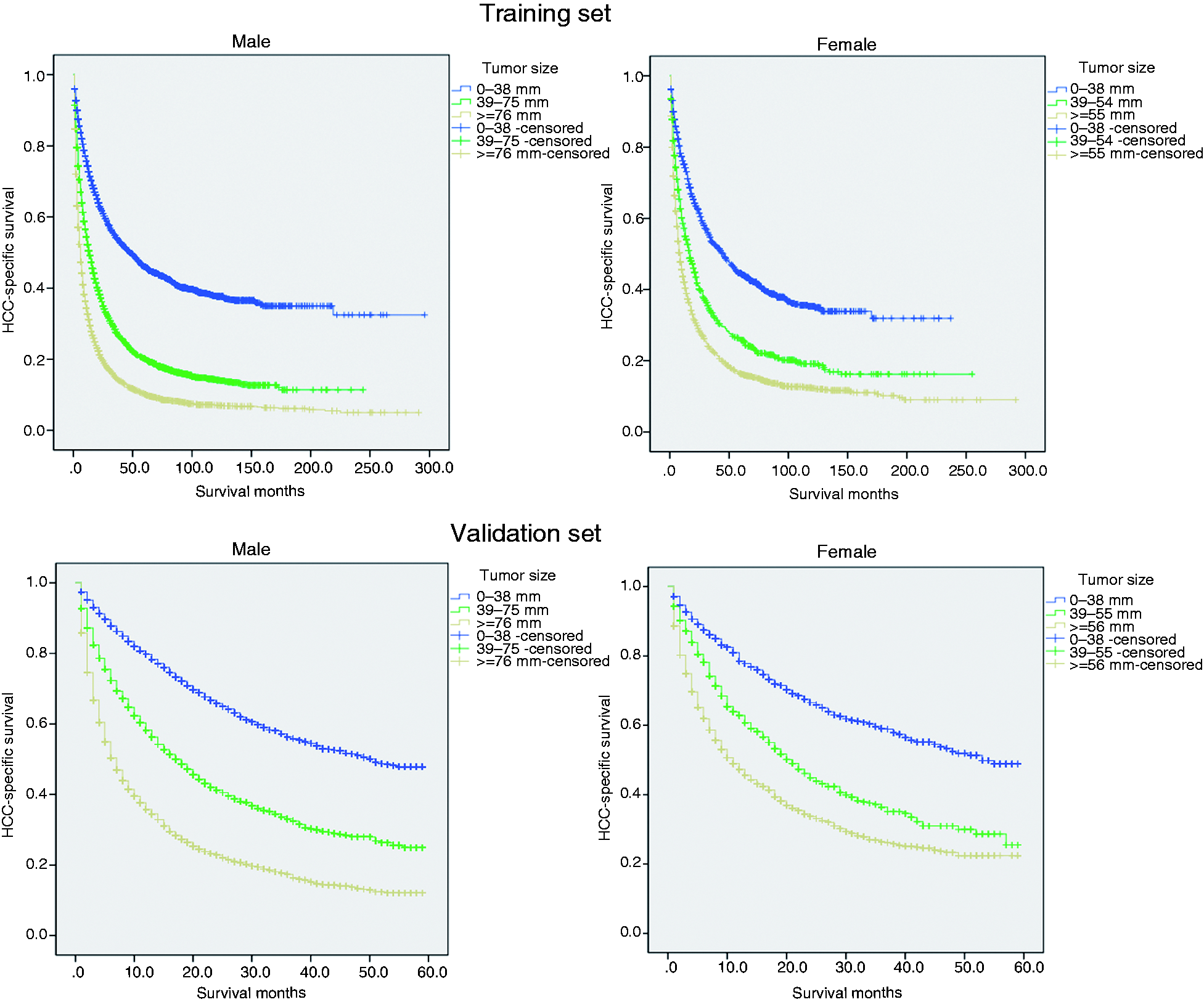
By using the X-Tile program, our results showed that the maximum chi-squared points of 2173.432 and 454.299 were achieved when applying 38 mm and 75 mm tumor size as the optimal cutoff point in men (survival rate 45.9%, 20.2% and 10.2% for patients with 0–38 mm, 39–75 mm and ≥76 mm tumors, respectively; p < 0.001); and 38 mm and 55 mm in women (survival rate 44.5%, 25.8% and 16.3% for patients with 0–38 mm, 39–55 mm and ≥56 mm tumors, respectively; p < 0.001) (Figures 1 and 2(a)). By using the abovementioned cutoff points, we can divide the HCC patients into three subgroups in terms of five-year CSS.
Effect of gender on CSS
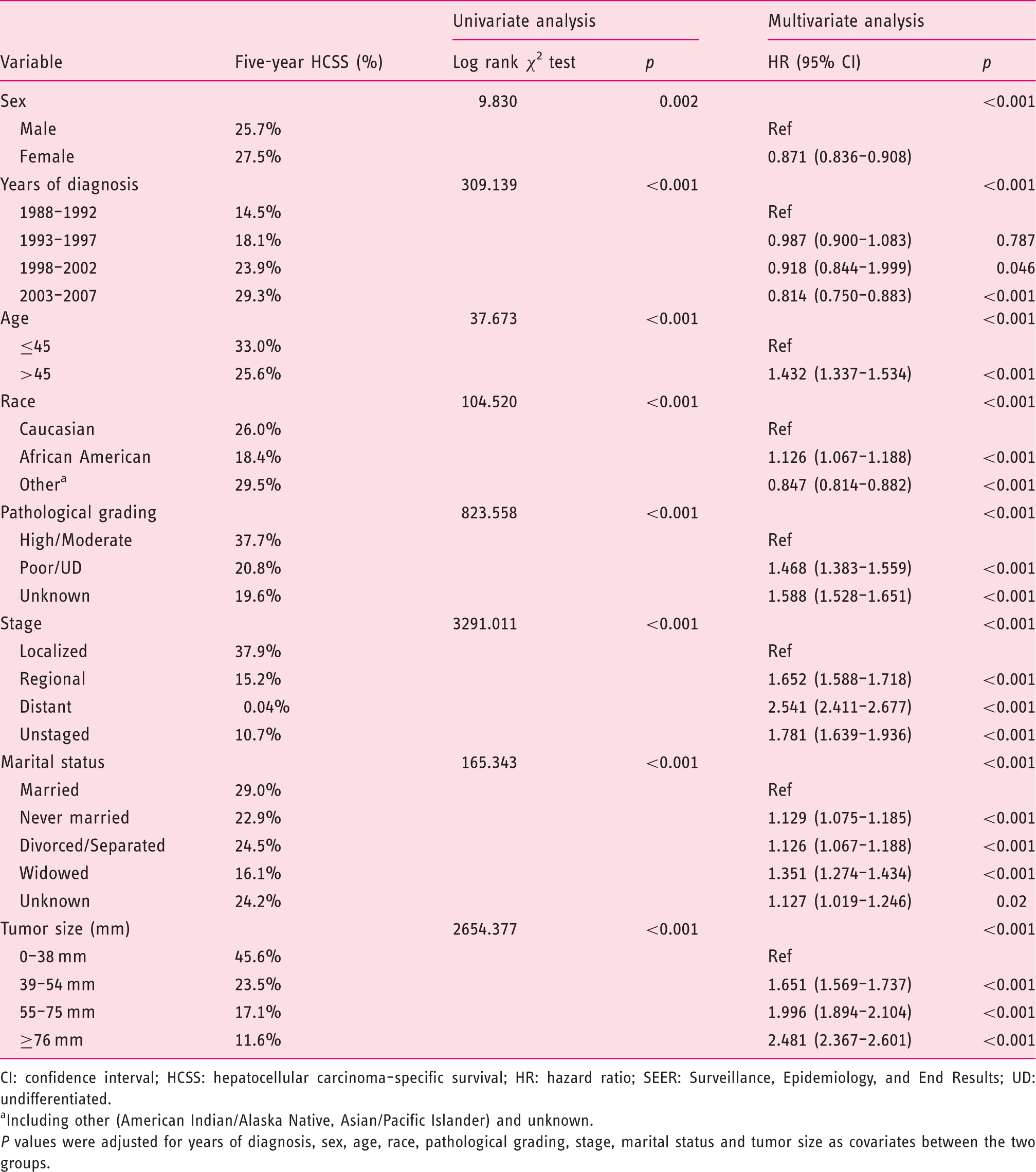
The five-year overall (p < 0.001) and CSS (p = 0.002) rates were 19.1% and 25.7% in men; and 21.4% and 27.5% in women (Figure 3(a)). Additionally, in men (p = 0.002), univariate analysis found that larger tumor size, the widowed group, higher stage, poor/undifferentiated tumor grade, African American race, age older than 45 years, an early year of diagnosis as well as being men were considered significant risk factors. Additionally, the following eight factors were found to be independent prognostic factors when multivariate analysis with Cox regression was performed (Table 2): (female, HR 0.871, 95% confidence interval (CI) 0.836–0.908), year of diagnosis (1993–1997, HR 0.987, 95% CI 0.900–1.083; 1998–2002, HR 0.918, 95% CI 0.844–1.999; 2003–2007, HR 0.814, 95% CI 0.750–0.883), age (>45, HR 1.432, 95% CI 1.337–1.534), race (African American, HR 1.126, 95% CI 1.067–1.188; others, HR 0.847, 95% CI 0.814–0.882), pathological grading (poor/undifferentiated, HR 1.468, 95% CI 1.383–1.559; unknown, HR 1.588, 95% CI 1.528–1.651), stage (regional, HR 1.652, 95% CI 1.588–1.718; distant, HR 2.541, 95% CI 2.411–2.677; unstaged, HR 1.781, 95% CI 1.639–1.936), marital status (never married, HR, 1.129, 95% CI, 1.075–1.185; divorced/separated, HR, 1.126, 95% CI, 1.067–1.188; widowed, HR, 1.351, 95% CI, 1.274–1.434; unknown, HR 1.127, 95% CI 1.019–1.246) and tumor size (39–54 mm, HR 1.651, 95% CI 1.569–1.737; 55–75 mm, HR 1.996, 95% CI 1.894–2.104; ≥ 76 mm, HR 2.481, 95% CI 2.367–2.601).
Univariate and multivariate survival analysis for evaluating the influence of tumor size on cause-specific survival in the SEER database. CI: confidence interval; HCSS: hepatocellular carcinoma–specific survival; HR: hazard ratio; SEER: Surveillance, Epidemiology, and End Results; UD: undifferentiated. Including other (American Indian/Alaska Native, Asian/Pacific Islander) and unknown. P values were adjusted for years of diagnosis, sex, age, race, pathological grading, stage, marital status and tumor size as covariates between the two groups.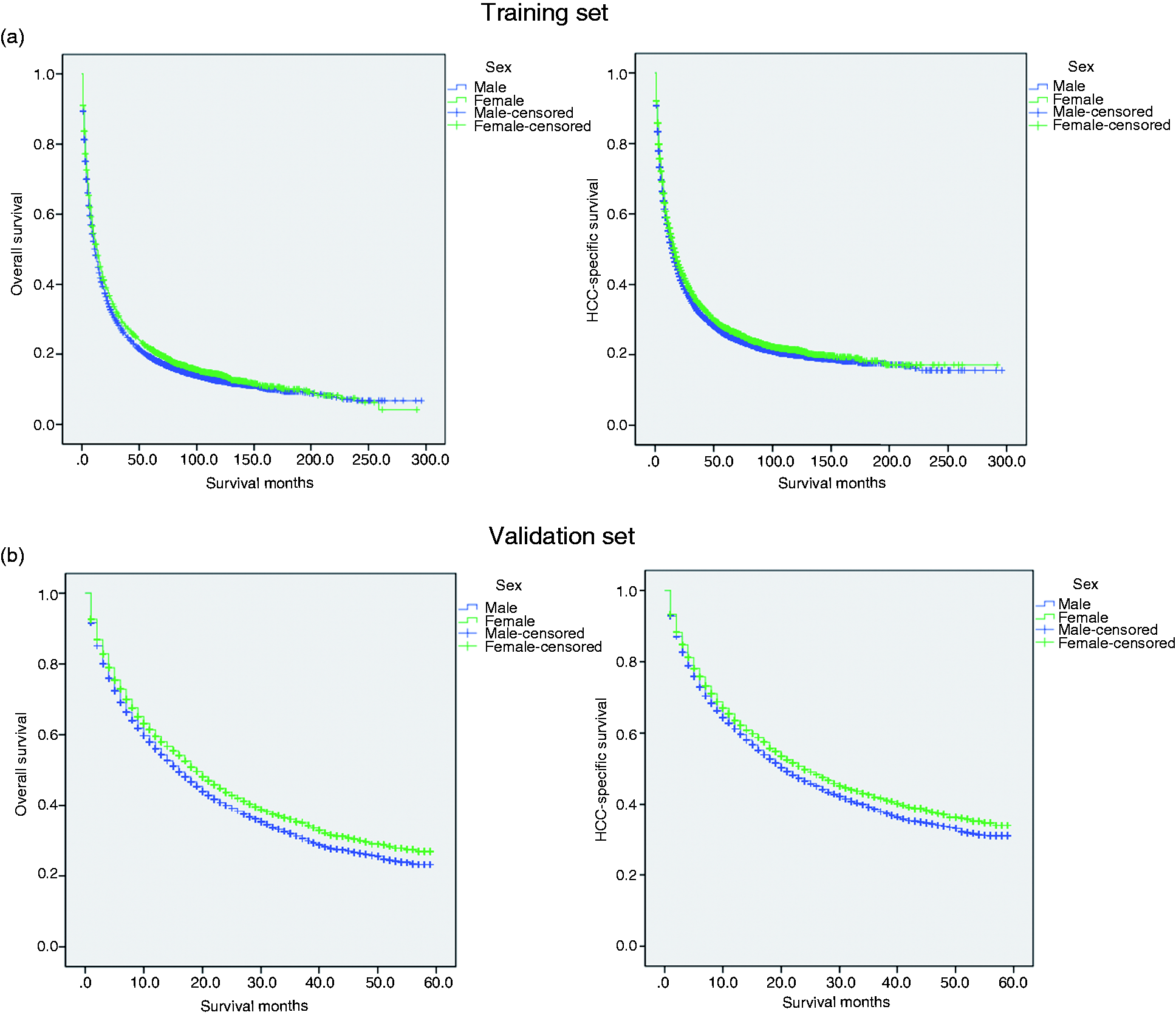
Interaction by gender in the training set
Pairwise comparisons between different combinations of tumor size and gender relative to HCSM.
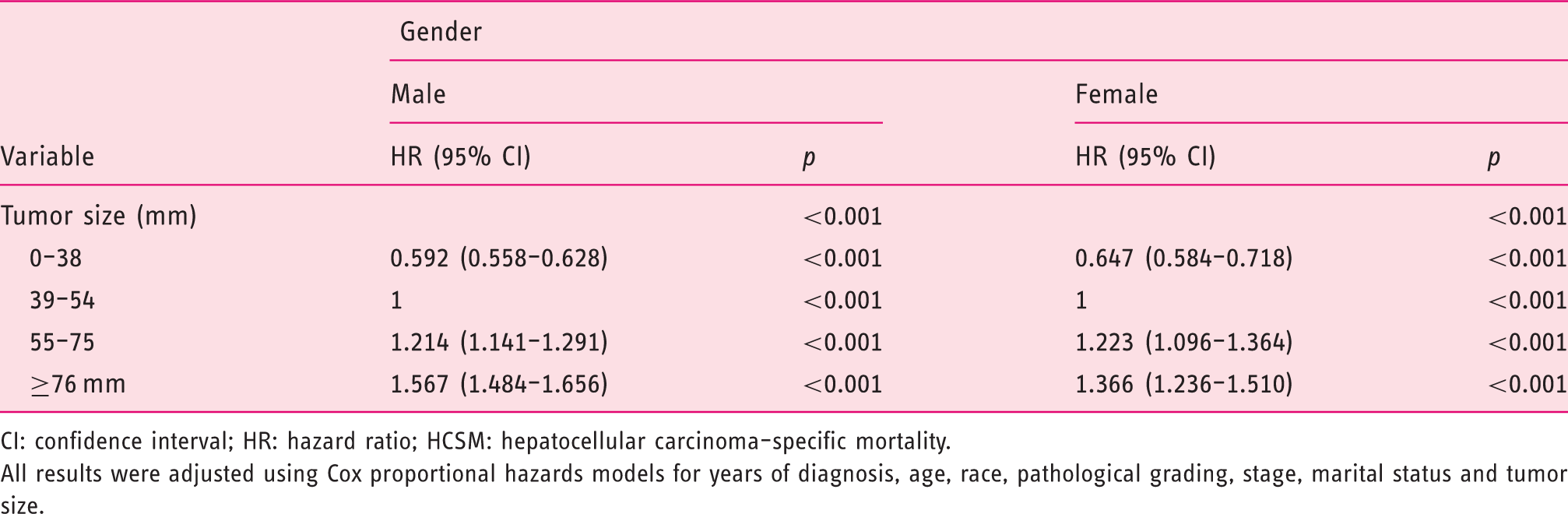
CI: confidence interval; HR: hazard ratio; HCSM: hepatocellular carcinoma–specific mortality.
All results were adjusted using Cox proportional hazards models for years of diagnosis, age, race, pathological grading, stage, marital status and tumor size.
Subgroup analysis for evaluating the effect of tumor size based on different stages
Univariate and multivariate analyses for evaluating tumor size influencing CSS in HCC based on different cancer stage.
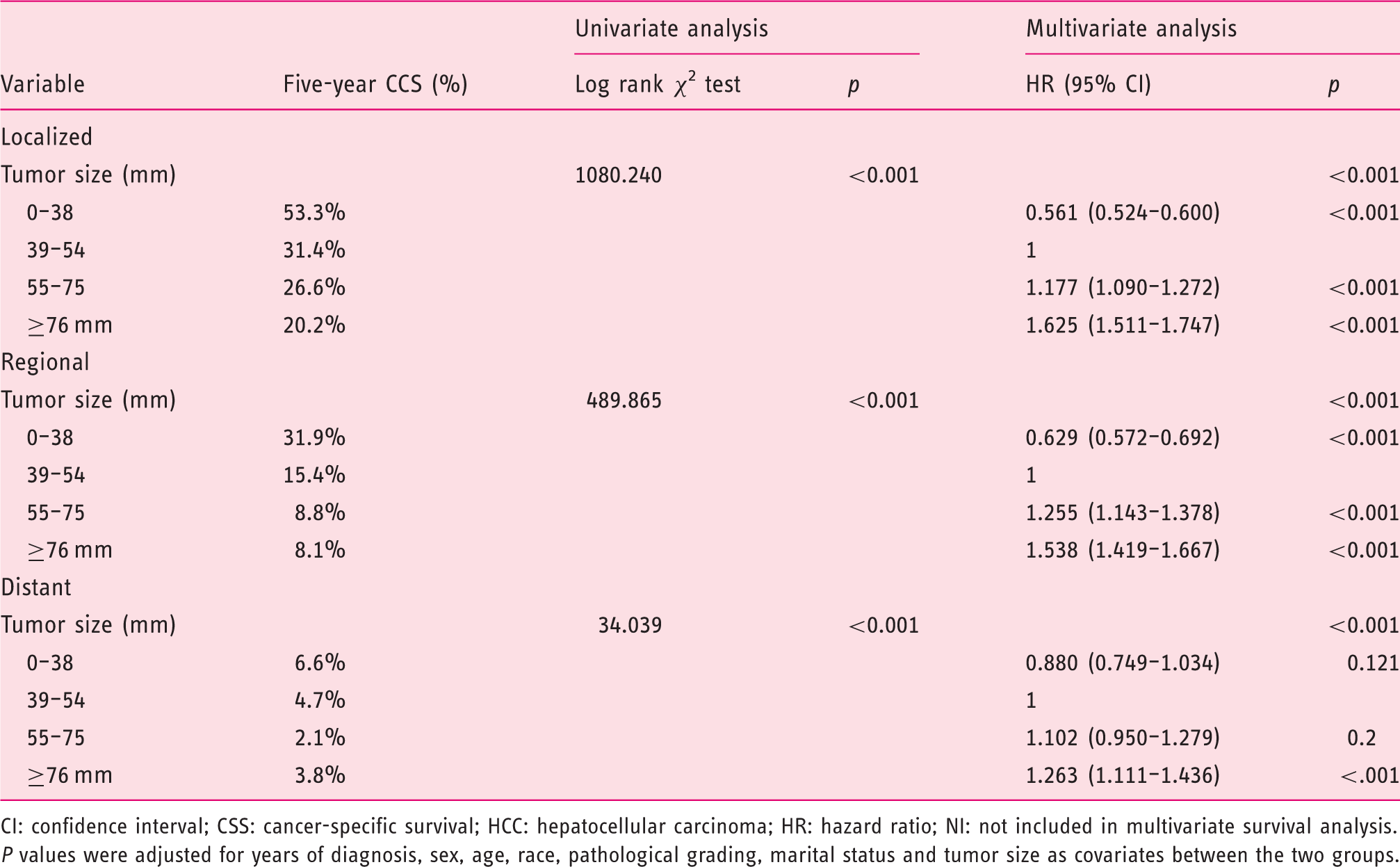
CI: confidence interval; CSS: cancer-specific survival; HCC: hepatocellular carcinoma; HR: hazard ratio; NI: not included in multivariate survival analysis.
P values were adjusted for years of diagnosis, sex, age, race, pathological grading, marital status and tumor size as covariates between the two groups.
Validation of outcomes
The external validation was performed in another SEER validation set. By using the optimal cutoff value, the validation patients could also be divided into three subsets in terms of five-year CSS rates (Figure 2(b)). The five-year overall (p < 0.001) and CSS (p < 0.001) rates were 23.3% and 31.1% in men, and 27.0% and 33.9% in women (Figure 3(b)). Multivariate analysis showed gender was an independent prognostic factor for HCC, validating that women with HCC had better survival (Table S1). Meanwhile, small tumor size groups also had survival benefits across several subgroups (Tables S2 and S3).
Discussion
Despite the prognosis of HCC patients improving recently because of advances in early diagnosis and treatment, the incidence is still increasing. 16 A more comprehensive understanding of cancer biology could increase our knowledge of HCC and individualized treatments. Regardless of predisposing factors, there is a remarkable sex disparity in HCC incidence, with a solid predominance for men. 7 Epidemiological studies showed that elevated testosterone levels in male HBsAg carriers were correlated with the increased risk of HCC.17,18 Meanwhile, antiandrogen agents can prevent HCC development in male rodents. 19 In addition to the tumor-promoting activity of androgen, estrogen in women seems to protect them from hepatocarcinogenesis. Postmenopausal females are at high risk of HCC, as are early-oophorectomy patients. 20
Tumor size is also a known risk factor for poor survival of HCC.13,21 Both the Barcelona Clinic Liver Cancer classification and the American Joint Committee on Cancer staging system include tumor size as an important variable. However, the cutoff value for tumor size varies among different staging systems and the prognostic significance of tumor size in patients with HCC is controversial.12,14 Pawlik et al. reported that tumor size could predict vascular invasion and histologic grade. 22 However, Zhang and colleagues found tumor size did not affect long-term survival of solitary HCC without macroscopic vascular invasion. 23 Owing to the sex-related discrepancies, the application of the proper tumor size cutoff value stratified by gender in HCC patients in predicting the survival rates has been a controversial issue.
In this study, we analyzed the SEER data of 19,279 HCC patients and identified 38 mm and 75 mm tumor size as the optimal cutoff value in male patients, and 38 mm and 55 mm in female patients. The five-year CSS rates were 45.9%, 20.2% and 10.2% in the 0–38 mm, 39–75 mm and ≥76 mm tumors in men, and 44.5%, 25.8% and 16.3% in the 0–38 mm, 39–55 mm and ≥56 mm tumors in women. Among these patients, regardless of gender, 0–38 mm tumors always exhibited the best survival whereas ≥76 mm tumors had the worst survival in male and female patients, indicating that 39–75 mm tumors was essentially heterogeneous. Meanwhile, a piecewise relationship between large tumor size and HCSM was observed. In patients with ≥76 mm tumors, women had a lower HCSM compared with men, which was consistent with epidemiology results that estrogen protects women from HCC. Moreover, female patients with HCC had certain clinicopathological features and prognostic factors different from those in male patients. The percentage of patients with HCC at high/moderate grade was 33.9% in men compared with 34.3% in women. In addition, the female patients also had a higher percentage of localized stage compared with males (57.5% vs 52.5%). Further subgroup analysis demonstrated that HCC patients with 0–38 mm tumors exhibited an increased five-year CSS across several subgroups. These results were further validated in another validation set.
Our results might affect clinical practice. As a result of the sex-related discrepancies, patients with 39 to 75 mm tumors have different prognoses in different genders. These HCC patients should be treated with a personalized treatment strategy, especially those HCC patients with 39 to 75 mm tumors.
This population-based surveillance study also has several limitations. First, HCC predisposing factors such as hepatitis virus and steatohepatitis were not included in the SEER database. Second, despite being based on a large, multicenter study population, individual subgroups became small after stratifying by tumor size, yielding limited statistical power. Third, the SEER database is retrospective rather than prospective, which might introduce unaccounted biases and affect the analysis. Fourth, although we observed that men and women have different cutoff points of tumor size, a real and precise association between tumor size and CSS in different genders needs to be further confirmed. Despite these limitations, the SEER database provides the opportunity to analyze a large number of patients with significant follow-up, rendering our results more convincing.
In conclusion, our study demonstrated that women appeared to have better survival rates than men in HCC, which correlated with more favorable tumor characteristics. Sex-related discrepancies should be emphasized and salvage therapy should be individualized, particularly in patients with 39 to 75 mm tumors.
Supplemental Material
Supplemental material for Differences in the prognostic value of tumor size on hepatocellular cancer-specific survival stratified by gender in a SEER population-based study
Supplemental Material for Differences in the prognostic value of tumor size on hepatocellular cancer-specific survival stratified by gender in a SEER population-based study by Wenjie Zhang, Kangpeng Jin, Fei Wang, Guangyan Zhangyuan, Weiwei Yu, Yang Liu, Haitian Zhang, Ping Zhang and Beicheng Sun in United European Gastroenterology Journal
Footnotes
Acknowledgments
We would like to thank the SEER database for its open access.
Author contributions
W.Z., P.Z. and B.S.: conceptualization, methodology, validation, investigation, writing–original draft, writing–review and editing, and visualization. W.Z., K.J. and B.S.: data curation and writing–review and editing. W.Z., G.Z. and W.Y formal analysis, investigation, and writing–review and editing. Y.L.: investigation, resources, writing–original draft, and writing–review and editing. WJZ, PZ and B.S.: formal analysis, writing–original draft, writing–review and editing, visualization, and supervision. K.J. and G.Z.: investigation, resources, writing–original draft, and writing–review and editing. W.Y. and Y.L.: formal analysis, investigation, resources, and writing–review and editing. H.Z., P.Z and B.S.: conceptualization, methodology, software, validation, formal analysis, investigation, resources, data curation, writing–original draft, writing–review and editing, visualization, and supervision. B.S. is Yangtze River Scholars Distinguished Professor.
Declaration of conflicting interests
None declared.
Funding
This work was supported by grants from the National Key Research and Development Program of China (grant number: 2016YFC0905900 to B.S.); the State Key Program of National Natural Science Foundation (grant number: 81430062 to B.S.); Innovative Research Groups of National Natural Science Foundation (grant number: 81521004 to B.S.); The National Natural Science Foundation of China (grant number: 81702344 to W.Z.), and the TianQing Liver Disease Research Fund (grant number: TQGB20180095 to W.Z.).
Ethics approval
Approval from the ethical board for this study was not required because of the public nature of all the data.
Informed consent
This study did not involve personal identifying information or interact with human individuals. Therefore, informed consent was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.