
Abstract
Background and objective
The 2016, United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU) provided evidence-based recommendations for the management of chronic pancreatitis and allowed for the objective evaluation of the quality of care in several domains of disease management through assessment of guideline adherence. Therefore, the aim of this study is to evaluate the current level and the variety of care for chronic pancreatitis patients in the Netherlands using the HaPanEU guidelines as a reference standard. The majority of these patients were diagnosed before the publication of these guidelines. Therefore, in most patients, the results of the present study with respect to those recommendations regarding the diagnostic process of chronic pancreatitis represent guideline correspondence and not adherence.
Methods
A subgroup of patients from the Dutch nationwide chronic pancreatitis registry (CARE) was included in a retrospective cross-sectional observational cohort study. A total of 39 recommendations concerning the non-invasive management of chronic pancreatitis were appointed as quality indicators (QIs). Per patient, the number of relevant QIs was determined and guideline adherence was assessed. Data were analyzed to identify factors associated with guideline adherence.
Results
Overall, 97 patients with chronic pancreatitis from 11 hospitals were included. Per patient, a mean number of 26 relevant QIs was applicable, with an average adherence rate of 53%. In 45% of the patients, guideline adherence was less than 50%. The majority of suboptimal managed QIs concerned the management of chronic pancreatitis complications. Guideline adherence was not associated with hospital type, sex, age or etiology of pancreatitis.
Conclusion
In the Netherlands, adherence to the HaPanEU recommendations for the management of chronic pancreatitis is moderate to low for all non-invasive domains, which may indicate suboptimal care for these patients. Closer guideline adherence could improve the level of care and the clinical outcomes of these patients. A nationwide approach to increase awareness of the key guideline recommendations among clinicians and patients is needed.
Keywords
Key summary
What is the established knowledge on this subject?
Chronic pancreatitis is a severely debilitating disease and it is associated with a markedly reduced life expectancy and reduced quality of life. Lack of an evidence-based national guideline in the past has most likely led to a variety in the type and level of practice for chronic pancreatitis patients in the Netherlands. In 2016, the United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU) were introduced across Europe. Publication of the HaPanEU guidelines allows for the evaluation of quality of care and variety in practice in several domains of disease management for chronic pancreatitis in the Netherlands.
What are the significant findings in this study?
Adherence to the HaPanEU recommendations for the management of chronic pancreatitis is moderate to low for all non-invasive domains, which may indicate suboptimal care for patients with chronic pancreatitis in the Netherlands. Health care issues showing the lowest adherence were evaluation of current smoking status and alcohol consumption, annual screening for pancreatic exocrine insufficiency and deficiencies of fat-soluble vitamins, screening for and the prevention of bone health diseases and structured evaluation of abdominal pain and quality of life. Suboptimal adherence to guideline recommendations, demonstrated in the present study, could not be explained by etiology, sex, age and hospital setting.
Introduction
Chronic pancreatitis (CP) is a relatively rare debilitating disease with a complex and diverse etiology and clinical presentation.1,2 It is associated with a markedly reduced life expectancy of roughly eight years and a decreased quality of life (QoL) as compared with healthy population controls and with patients with other chronic conditions.3–6 CP is an incurable, chronic inflammatory disease, which leads to permanent tissue damage and loss of pancreatic function. Treatment is mainly focused on preventing further disease progression and disease-related complications. 7 Like in other chronic diseases, QoL is a crucial indicator of treatment success. Mokrowiecka et al. identified pancreatic pain as one of the most important independent predictors of QoL in these patients.8–11 Pain is reported in around 90% of the CP patients and about half of those patients will continue to have pain, despite therapy, adversely influencing their QoL.12,13 Other factors that negatively influence QoL are a lower body weight, longer disease duration, pancreatic exocrine- and endocrine-insufficiency, systemic inflammation, persistent smoking and unemployment.7,11,14,15
Management of CP is difficult and involves many domains of health care. 12 Due to the lack of an evidence-based national guideline in the past, clinical decision-making in CP was mostly based on the experience, beliefs and disbeliefs of the local clinician, presumptively leading to a large variation in the level of care delivered to patients in the Netherlands. 16
Despite a well-organized health care system, our management of CP can most likely be improved. Sikkens et al. concluded that there is substantial undertreatment of exocrine-insufficient patients with pancreatic enzyme replacement therapy, which is suggestive of suboptimal care for these patients in the Netherlands. 17 To be able to improve the management of CP, it is of paramount importance to get insight into the current situation in the Netherlands to identify the domains of and factors associated with suboptimal care. In 2016, the working group on ‘Harmonizing diagnosis and treatment of CP across Europe’, in collaboration with United European Gastroenterology, published the United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU) guidelines. 18 These guidelines provide evidence-based recommendations to harmonize the diagnosis and treatment of CP across Europe, and allow for the objective evaluation of the quality of care in several domains of disease management through the assessment of guideline adherence. The aim of the present study is to evaluate the current level and variety of care for CP patients in the Netherlands using the HaPanEU guidelines as the ‘standard level of care’, to define areas for improvement and to determine factors associated with the current level of guideline adherence.
Methods
Study design and data collection
We performed a retrospective cross-sectional cohort study. Patients with CP from 11 Dutch hospitals were identified using the Dutch CP registry (CARE). 19 CARE is a prospective cohort that was established in 2011 by the Dutch Pancreatitis Study Group to provide information on the level of care for CP patients in the Netherlands. CP patients from the 11 participating hospitals with a diagnosis of CP or a first presentation to the hospital with symptoms of CP between 1 January 2010 and 31 December 2017 were eligible for inclusion. Only patients who still received active treatment in a participating hospital at time of enrollment were included. Active treatment was defined as at least one outpatient clinic visit to a physician (gastroenterologist or abdominal surgeon) for the treatment of CP < 12 months prior to data extraction.
To provide a full and complete dataset, all patients’ original medical records were reviewed on site. In some cases, relevant information was extracted from the CARE registry to prevent missing data. The collected data, representing a maximum period of 24 months, were extracted in May 2018. The majority of the Dutch CP patients were diagnosed before publication of the HaPanEU guidelines. Therefore, in most patients, the results of the present study with respect to those recommendations regarding the diagnostic process of chronic pancreatitis represent guideline correspondence and not adherence.
Among the participating hospitals were four university hospitals and seven teaching hospitals. This approach was chosen to obtain a broad impression of the level of care that was provided in different health care settings. Adherence to the HaPanEU recommendations of the non-invasive management of CP was our main outcome. Secondly, adherence scores for each domain of the non-invasive management and for the individual components of care within each domain were assessed. Therefore, a dataset was designed using the recommendations of four main domains concerning the non-invasive management of CP as mentioned in the HaPanEU guidelines; etiology, diagnosis of CP with imaging, complications of CP and therapy of complications of CP. This resulted in a list of 39 ‘quality indicators’ (QIs), graded as strong recommendations and as high-quality evidence according to the Grading of Recommendations Assessment, Development and Evaluation system. 20 Not all QIs were applicable to every patient. For example, the QIs concerning treatment of complications were not applicable in the absence of these complications. At first, the number of relevant QIs according to these guidelines for each domain per patient was determined. All the relevant QIs of each domain were added up to assess adherence to the key recommendations of the overall management of CP. Subsequently, the number of relevant QIs fulfilled by the treating clinician per domain was confirmed. Guideline adherence for every patient was assessed by determining the ratio between the number of fulfilled QIs and the total number of relevant QIs in the overall non-invasive management and for each domain, to define areas of suboptimal care.
Statistical analysis
In this study, descriptive statistics were applied to describe the study population and to provide the mean HaPanEU guidelines adherence rate in percentages in the overall non-invasive management of CP and for each domain. To test for factors influencing guideline adherence, the study population had to be divided into subgroups based on patients’ age, sex, hospital setting and etiology of CP. Two subgroups based on age of almost equal size were derived by dividing the study population into ≤61 years versus >61 years (i.e. this cut-off was based on the median age of 61 years in our study population). To compare the mean differences in adherence to the recommendations of the HaPanEU guidelines between the etiology of CP (non-alcoholic pancreatitis versus chronic alcoholic pancreatitis), sex (male versus female), age (≤61 years versus >61 years) and hospital setting (university hospital versus teaching hospital), subgroup analyses were conducted to identify factors associated with the level of adherence and to define the variety of care. Continuous variables were tested for normal distribution by using the Kolmogorov–Smirnov and Shapiro–Wilk tests and were compared using the Student’s t-test. In case of a statistically significant difference between subgroups, multivariable regression analyses were conducted to adjust for potential confounders. A p-value lower than 0.05 was considered as statistically significant. Data were analyzed using IBM SPSS 25.
Results
Patients
The medical records of 261 CP patients from the 11 participating hospitals were reviewed. A total of 97 patients fulfilled the eligibility criteria and were included for further analysis. In one patient, no imaging data were available, whereby it was not possible to determine the adherence rate for the domain ‘diagnosing CP with imaging’ and overall non-invasive management of CP and, therefore, this patient was excluded for further analysis, leaving 96 patients for the final cohort. An overview that summarises patient inclusion is provided in Figure 1.
The baseline characteristics are presented in Table 1. Patients had a median age of 61 years; of those, 68% were male and 51% were treated in a university hospital setting. In 43% of the cases, alcohol was considered as the main etiologic factor.
Demographic and clinical characteristics of patients.
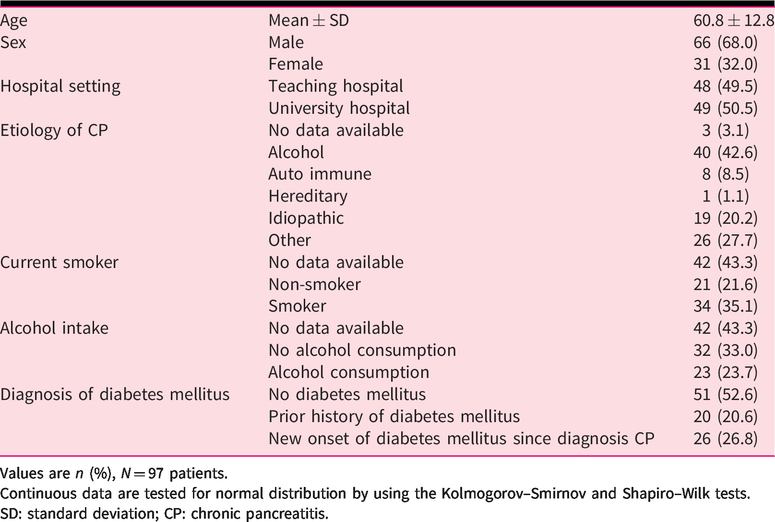
Values are n (%), N = 97 patients.
Continuous data are tested for normal distribution by using the Kolmogorov–Smirnov and Shapiro–Wilk tests.
SD: standard deviation; CP: chronic pancreatitis.
Guideline adherence
A description of all the QIs belonging to the four domains concerning the non-invasive management of CP according to the HaPanEU guidelines is provided in Table 2. In the overall non-invasive management of CP, a minimum of 20 and a maximum of 39 relevant QIs per patient can be fulfilled by the clinician.
An overview of all the QIs of the four domains concerning the non-invasive management of CP and adherence to the HaPanEU guidelines.
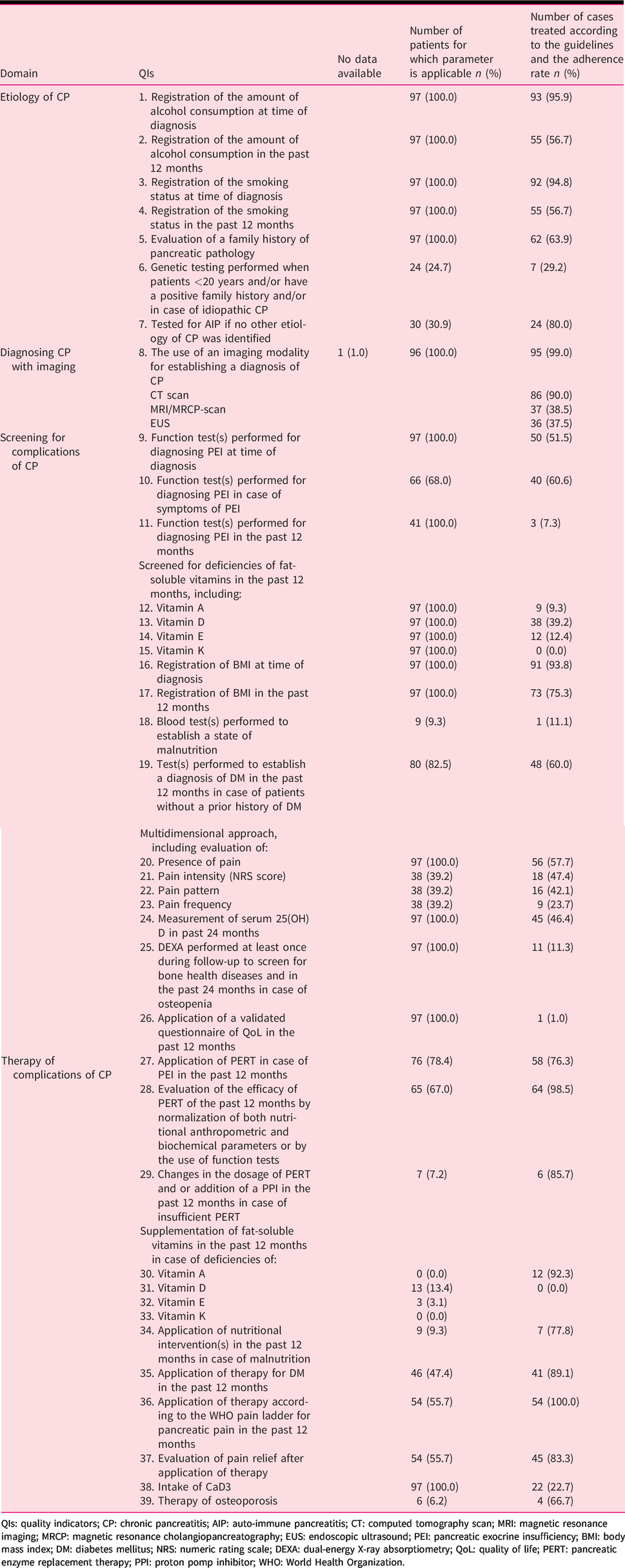
QIs: quality indicators; CP: chronic pancreatitis; AIP: auto-immune pancreatitis; CT: computed tomography scan; MRI: magnetic resonance imaging; MRCP: magnetic resonance cholangiopancreatography; EUS: endoscopic ultrasound; PEI: pancreatic exocrine insufficiency; BMI: body mass index; DM: diabetes mellitus; NRS: numeric rating scale; DEXA: dual-energy X-ray absorptiometry; QoL: quality of life; PERT: pancreatic enzyme replacement therapy; PPI: proton pomp inhibitor; WHO: World Health Organization.
Figure 2 represents the adherence to the HaPanEU guidelines with regard to all the relevant QIs in the overall non-invasive management of CP for the 96 included patients. The mean number of relevant QIs per patient was 26 ± 3. The mean guideline adherence was 53% ± 13%. In 43 patients (45%), the adherence rate was ≤50%.
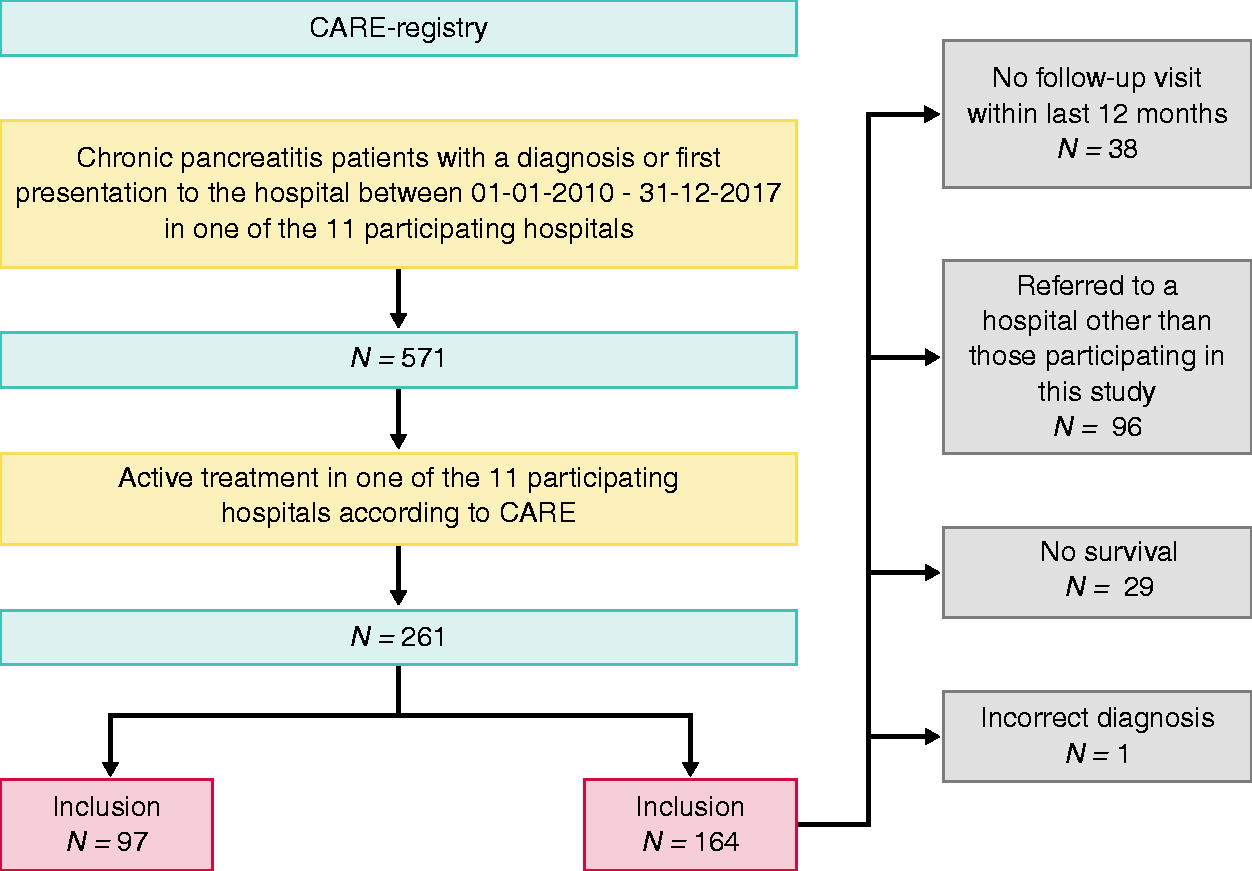
Flow chart of patient inclusion for this study.
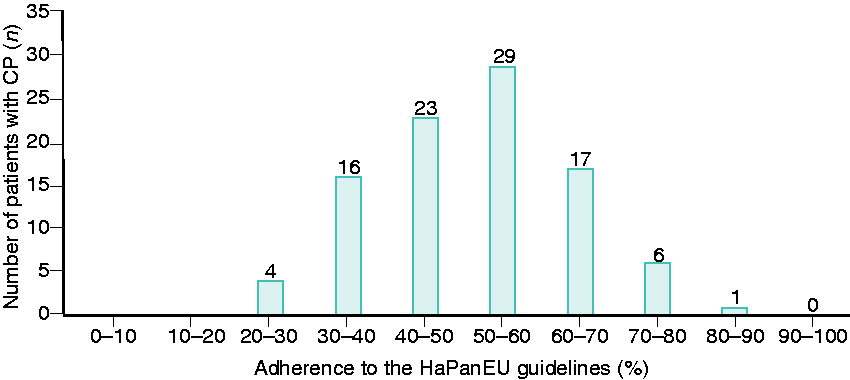
Guideline adherence in the overall non-invasive management of CP.
The subgroup analyses are presented in Table 3. Etiology of CP was not associated with the low adherence rate. In addition, no statistically significant differences were observed in guideline adherence among different hospital settings. In Table 4, an overview is given of the mean guideline adherence per participating center and the variety of care between the different participating hospitals.
Differences in guideline adherence between age, sex, hospital setting and etiology of CP.
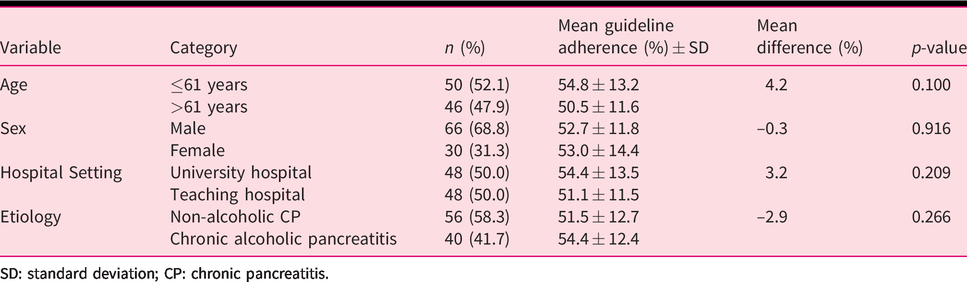
SD: standard deviation; CP: chronic pancreatitis.
Mean adherence rate (%) of all the participating university and teaching hospitals.
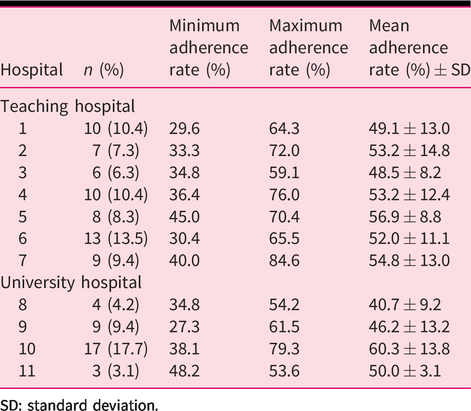
SD: standard deviation.
Defining the areas of suboptimal care
An overview of the mean number of relevant QIs per patient, the mean adherence rate and total number of patients with an adherence rate of less than 50% for each domain of the non-invasive management of CP is given in Table 5. In 95 patients (99%) a computed tomography scan, magnetic resonance imaging/magnetic resonance cholangiopancreatography or endoscopic ultrasound was performed to establish a diagnosis of CP. The items with the lowest guideline adherence were screening for pancreatic exocrine insufficiency (PEI) and deficiencies of fat-soluble vitamins, structured evaluation of abdominal pain and QoL (1%) and screening for and the prevention of bone health diseases (11% and 23%, respectively). A function test to screen for PEI was performed in 52% of the cases at time of diagnosis and in 61% in case of symptoms of PEI. A function test was performed in only 7% of the cases in the past 12 months. Screening for vitamin D deficiency in the past 12 months occurred in 39% of the cases. Screening for deficiencies of other fat-soluble vitamins was performed less often. Presence of pain was evaluated in 58% of the cases (56 patients); 54 patients reported abdominal pain, and all of them received pain therapy according to the steps of the World Health Organization analgesic ladder. In 45 cases, pain relief after application of therapy was evaluated. All those items were part of the domain concerning ‘Therapy of complications of CP’ (Table 2).
Mean number of relevant QIs per patient, the mean adherence rate and total number of patients with an adherence rate ≤50% for each domain of the non-invasive management of CP.
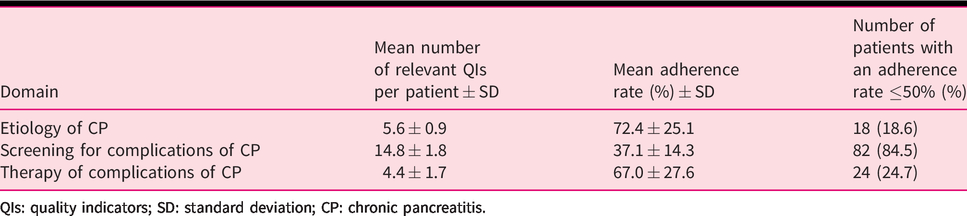
QIs: quality indicators; SD: standard deviation; CP: chronic pancreatitis.
Discussion
This study assessed the current level of care for patients with CP in the Netherlands using the HaPanEU guidelines as a reference standard. We found an average adherence rate of 53%, which could not be explained by etiology of CP, sex, age or hospital setting. This low adherence rate accounted for all domains of care, but, most prominently, for the domain concerning management of CP complications. An adherence rate of 37% was achieved within this domain of care. The main health care issues that proved to be suboptimal in the present study were evaluation of current smoking status and alcohol consumption during follow-up, annual screening for PEI and deficiencies of fat-soluble vitamins, evaluation of abdominal pain and QoL and screening for and the prevention of bone health diseases. The items that scored high in guideline adherence were evaluation of the amount of alcohol consumption and smoking behavior at time of diagnosis, the registration of the body mass index at time of diagnosis and the use of an appropriate imaging modality for establishing CP. In general, it is assumed that adequate longitudinal follow-up of alcoholic CP patients is difficult to accomplish because of the associated stigma that these patients are non-compliant. 21 On the other hand, from a patient’s perspective, these patients often suffer from the feeling that their health care professional accuses them of being addicted. 22 Fortunately, no statistical difference in adherence rate was found between non-alcoholic and alcoholic CP patients. The same applies for CP patients from different health care settings, which means the level of care provided by teaching hospitals was, therefore, comparable with those of patients who were treated in a university hospital setting.
This is the first nationwide study that evaluates the quality of care for CP patients by quantifying guideline adherence. Therefore, we compared our results with the most recently published literature concerning guideline adherence of other gastro-intestinal diseases in the Netherlands. One study evaluated adherence to the national guideline for adjuvant therapy for high-risk stage II and III colorectal cancer. Within their study population, an average guideline adherence of 66% and 84% was found, respectively, which is remarkably higher than in our present study. 23 Van Rijssen et al. evaluated national compliance to selected QIs from a Dutch evidence-based multidisciplinary guideline on pancreatic and periampullary carcinoma. According to their findings, compliance varied between 39% and 64%, which is more in accordance with our results. 24 A potential difficulty in extrapolating these results is the difference in standardization and registration of care between patients with malignant disease and patients with chronic benign diseases.
CP patients have a substantially impaired QoL. No studies so far have investigated the relationship between quality of care and QoL within this population. We found a moderate to low adherence to the HaPanEU guidelines, which may indicate suboptimal care. Future research needs to address the effect of guideline non-adherence in the management of CP on the QoL among these patients.
Adherence to the HaPanEU guidelines is used to indicate current quality of care, as these recommendations are considered to be the ‘standard level of care’. Even though, strictly speaking, guideline adherence could only be evaluated for the domain ‘management of CP complications’, we believe our results are representative for how these guidelines are implemented into current practice. It is possible that the current adherence rate is higher, because of an increasing awareness among clinicians. 25 However, the majority of these recommendations have previously been published in international guidelines with respect to a select domain of disease management (e.g. pain or PEI). Nevertheless, according to our findings, they are still not being applied efficiently in the Netherlands.17,26 Furthermore, all patients were selected from the CARE registry. This cohort is set up to collect information about current practice to investigate natural disease course, disease-related complications and efficacy and timing of treatment strategies. These patients are probably treated more frequently according to the HaPanEU recommendations, because of a higher awareness among their treating physicians, which could indicate that our results are probably too optimistic. However, there are currently 30 centers involved in the CARE registry and all Dutch CP centers are represented. It is true that in our health care system general practitioners care for patients to quite a large extent, which could mean that guideline adherence for the individual patient might be better than displayed in our study. However, most CP patients suffering from disease-related complications will be referred to a specialist and, considering the limited number of CP patients per general practitioner, we believe this will not significantly affect our results. For the reasons mentioned previously, we assume that our results could be considered as representative of the current adherence rate to the HaPanEU guidelines.
Despite the fact that the Netherlands has one of the most well-organized health care systems across the whole of Europe according to the Euro Health Consumer Index of 2017, current care for patients with CP is not in compliance with the HaPanEU guidelines. Therefore, we would assume that improvements in disease management and guideline adherence could be of relevance for many if not all European countries. Therefore, raising guideline awareness among both clinicians and patients is important. Online education should be provided. Given the extensity and complexity of the HaPanEU guidelines, an easy-viewed best-practice protocol is desirable to increase consciousness. Audit and feedback sessions can be used to evaluate guideline implementation. 27 A higher adherence to the HaPanEU guidelines will most likely improve the level of care and QoL of these patients.
Strengths and limitations
A strength of this study is the method of data collection, whereby original patients’ charts were reviewed in detail by the same researcher. Data were, therefore, reliable since no misclassification of data at time of collection could occur with a low number of missing values. Adjustment for potential confounders were made to minimize their influence in case of a statistically significant difference in subgroup analyses. This was not possible for current smoking status and alcohol consumption since no data were available in 43% of the cases. Another strength of this study is the inclusion of different health care settings, whereby a broad impression of the level of care in the Netherlands is obtained.
There are also limitations to our study. Firstly, the current study comprises a relatively small sample of the Dutch CP population. Furthermore, identifying patients by only using the CARE registry and the large number of excluded patients may have caused selection bias. However, all Dutch CP centers are represented in CARE and the characteristics of our population match the ratios described in previously published CP studies. Therefore, we believe this is a representative sample of the Dutch CP population. Secondly, the retrospective cross-sectional design of this study could have caused a distorted evaluation of data. Guideline adherence could reflect variations in the adequacy of documentation by clinicians. Therefore, both information from questionnaires of CARE and from patient charts were combined to reduce information bias.
Conclusion
In this audit of 97 patients with CP, a suboptimal adherence rate of 53% was found using the recommendations graded as strong and as high-quality evidence as a reference standard. This low adherence rate could not be explained by sex, etiology, hospital setting and age. There appears to be significant room for improvement in the identification and management of persistent smoking and drinking, and in the prevention, diagnosis and management of complications of CP. A nationwide approach is preferred to provide education to both clinicians and patients and to implement quality initiatives with the aim to raise guideline awareness and adherence. These quality initiatives are most likely to improve the level of care and clinical outcomes of these patients, which could positively influence their QoL.
Footnotes
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Ethics approval
The study protocol of the CARE registry has been reviewed and was approved by the medical ethical committee of the University Medical Center Utrecht on 17 March 2010 (ID: AvG/rc/10/05699). The protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki. All participants provided written informed consent before enrollment and were asked explicitly for permission to obtain relevant data from their medical records for present and subsequent studies.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The CARE registry has been previously funded by an unrestricted grant from Abbott Pharmaceuticals (AMR number: IB154001) and by The Dutch Pancreas Patients’ Association (Alvleeskliervereniging).
Informed consent
All participants in the study were voluntary and expressed written informed consent prior to their inclusion for the CARE registry.