
Abstract
Background
Pancreatic function testing and imaging are used to inform the diagnosis of chronic pancreatitis, but most of these methods are time- and cost-consuming or lack diagnostic accuracy.
Objective
We investigated the utility of pancreas-specific plasma amylase for assessment and diagnosis of chronic pancreatitis.
Design
This was a prospective study of 121 consecutive patients with chronic pancreatitis and a reference population of 94 healthy controls. Pancreas-specific plasma amylase level was determined and analysed for its association with exocrine pancreatic insufficiency, diabetes and other clinical variables. Receiver operating characteristic curve analyses were performed to determine the diagnostic utility of plasma amylase for diagnosing chronic pancreatitis and to study associations with disease severity. The findings were validated in a further cohort of 57 patients with chronic pancreatitis.
Results
Significant and independent associations between plasma amylase level and duration of chronic pancreatitis as well as the presence of exocrine pancreatic insufficiency and diabetes were observed (all p < 0.001). An amylase level below 17.3 U/l had a high specificity (94%) and moderate sensitivity (59%) for the diagnosis of chronic pancreatitis. Diagnostic performance was influenced by disease stage with the best performance observed for advanced disease. The findings were replicated in the validation cohort.
Conclusion
Pancreas-specific plasma amylase may provide a clinically useful mean for assessment and diagnosis of chronic pancreatitis.
Keywords
Key summary
Summarise the established knowledge on this subject
Pancreatic function testing and imaging are used to inform the diagnosis of chronic pancreatitis. Most of the current available methods for assessment of chronic pancreatitis are time- and cost-consuming and lack diagnostic accuracy, and some of them invasive and unpleasant for the patient. Accurate, noninvasive and low-cost methods are warranted to aid in the assessment of chronic pancreatitis.
What are the significant and/or new findings of this study?
Significant and independent associations between pancreas-specific plasma amylase level, exocrine pancreatic insufficiency and diabetes were observed. A pancreas-specific plasma amylase level below 17.3 U/l had a high specificity and moderate sensitivity for the diagnosis of chronic pancreatitis. Diagnostic performance was influenced by disease stage with the best performance observed for advanced chronic pancreatitis.
Introduction
Chronic pancreatitis (CP) is a fibro-inflammatory disease that causes irreversible injury to the pancreatic tissue resulting in atrophy and fibrosis. 1 As the disease progresses, significant impairment of exocrine and endocrine pancreatic function evolves, compromising digestion and absorption of nutrients. 2 Pancreatic function testing and various imaging modalities are used to inform the diagnosis of CP and provide the cornerstone of previous and recent diagnostic criteria.3–5 However, most of these diagnostic modalities are time- and cost-consuming and some of them are invasive and unpleasant for the patient. Therefore, accurate, noninvasive and low-cost methods are warranted to aid in the diagnosis and assessment of CP.
Decreased plasma or serum levels of pancreatic enzymes have long been observed in patients with CP,6–10 but the observation has not been implemented in previous or recent diagnostic criteria or guidelines.11,12 This is possibly because of limited awareness of the clinical significance of a low plasma enzyme level, while an increased level of pancreatic enzymes is universally accepted as a criterion for acute pancreatitis. 13 Two recent studies investigated the diagnostic utility of plasma amylase and lipase in the context of CP. Kwon et al. found a high specificity (94%) but low sensitivity (39%) using a receiver operating characteristic curve (ROC)-derived threshold of plasma amylase level of 27.5 U/l for the diagnosis of calcific CP. 14 This finding was largely replicated in a later study by the same group that also included non-calcific pancreatitis patients. 15 However, both studies used a non–pancreas-specific amylase, which may compromise diagnostic accuracy because of modifications of plasma levels from extrapancreatic amylase sources. 16 Further, none of the studies investigated the association between amylase level, pancreatic exocrine and endocrine function, and clinical disease stage. This is important information as pancreatic enzyme levels are likely linked to the fibro-inflammatory process with decreasing amylase levels observed with prolonged disease duration as pancreatic atrophy and fibrosis evolves.8,17
To bridge this gap of knowledge and to inform future diagnostic criteria for CP more accurately, we investigated pancreas-specific plasma amylase levels and its association with endocrine and exocrine pancreatic function in two cohorts of patients with CP and a reference population. We hypothesised that the diagnostic accuracy of amylase levels for the diagnosis of CP would be influenced by the clinical disease stage. The aims of the study were: 1) to investigate pancreas-specific plasma amylase levels in CP patients and a reference population; 2) to study its association with diabetes (DM), exocrine pancreatic insufficiency (EPI) and other clinical variables; 3) to investigate the diagnostic performance of pancreas-specific plasma amylase for the diagnosis of CP, 4) to investigate the influence of clinical disease stage, as assessed by the M-ANNHEIM system, 5 on diagnostic performance, and 5) to validate findings in an independent cohort of patients with CP.
Participants and methods
This was a prospective, cross-sectional, two-centre study conducted at the Centre for Pancreatic Diseases, Department of Gastroenterology and Hepatology, Aalborg University Hospital, Denmark and Department of Clinical Cancer Medicine, Institute of Translational Medicine, The University of Liverpool, United Kingdom (UK).
The blood samples used to form the discovery cohort were collected at Aalborg University Hospital, Denmark, and drawn on a clinical indication and solely as a routine part of patient diagnostics and treatment. Because no study-related procedures were undertaken, the study did not require ethical approval according to the North Denmark Region Committee on Health Research Ethics and the informed consent requirement was consequently waived. Approval for data collection and storage was obtained from the Danish Data Protection Agency, Northern Denmark Region (2008-58-0028, project ID 2018-19).
The blood samples used to form the validation cohort were obtained from patients with proven or suspected CP under clinical review at the Royal Liverpool University Hospital. These patients were identified, recruited and consented during routine outpatient appointment visits. Once consent for inclusion in the Liverpool CP biobank and database was obtained, patients voluntarily provided a research blood sample taken simultaneously with any clinically indicated blood tests requested as part of standard clinical practice. Clinical and demographic data were also collected and stored on the CP database. The Liverpool CP biobank and database has been through full regional ethics committee (REC) review and has been granted favourable ethical opinion (REC refs 10/WNo03/46 and 16/WA/0057).
This study is reported according to the Standards for Reporting of Diagnostic Accuracy Studies 2015 guidelines. 18 However, a study protocol was not registered prior to study start.
Discovery cohort
Consecutive patients with clinical suspicion of CP referred to the Centre for Pancreatic Diseases, Department of Gastroenterology and Hepatology at Aalborg University Hospital between 2013 and 2017 were screened for inclusion. Inclusion criteria were age 18–75 years and a diagnosis of definitive or probable CP according to the M-ANNHEIM classification system. 5 Definitive CP was defined as patients fulfilling one or more of the following criteria: i) pancreatic calcifications, ii) marked pancreatic ductal changes according to the modified Cambridge classification, iii) marked and persistent exocrine insufficiency defined as pancreatic steatorrhea markedly reduced by enzyme replacement therapy and iv) histological evidence of CP. A diagnosis of probable CP was established if the patients fulfilled one or more of the following criteria: i) mild ductal alterations (according to the modified Cambridge classification), ii) recurrent or persistent pseudocysts, iii) pathological test of pancreatic exocrine function and iv) endocrine pancreatic insufficiency (DM). Patients with definitive and probable CP were included to cover the full disease spectrum of CP. 19 Exclusion criteria were patients with evidence of pancreas-specific plasma amylase or creatinine level above the upper limit of normal (ULN) and patients with a prior history of pancreatic surgery. Excluded patients were included in a secondary intention-to-test analysis.
Validation cohort
Seventy patients with CP were recruited for the validation cohort from the Department of Pancreato-Biliary Surgery at the Royal Liverpool University Hospital, Liverpool, UK, between 2011 and 2017. The in- and exclusion criteria were those utilised for the discovery cohort; 13 patients were excluded from the validation analysis because of pancreas-specific plasma amylase or creatinine level above the ULN. Hence, the final validation cohort comprised 57 patients.
Reference population
The reference population comprised 94 healthy blood donors from Aalborg University Hospital with no known history of pancreatic, gastrointestinal or renal diseases. All participants in the reference population had pancreas-specific plasma amylase and creatinine levels within the normal range.
Demographic and clinical characteristics of patients with CP
Information on patients' demographics (gender and age) and clinical characteristics including aetiology and duration of CP, EPI, DM and presence of pancreatic calcifications were recorded on standardised case report forms based on patient interviews, review of medical records, biochemistry and imaging data (computed tomography and/or magnetic resonance cholangiopancreatography, MRCP).
Exocrine pancreatic function was characterised by the faecal elastase-1 concentration test or faecal fat collection as deemed appropriate by the referring physician. In case the exocrine pancreatic function had not been investigated prior to study inclusion, the faecal elastase-1 concentration test was used and the test result was registered when available. Exocrine pancreatic insufficiency was defined as a fat excretion (aliphatic carboxylate (C14–C26)) above 25 mmol per 24 hours or faecal elastase-1 level below 200 µg/g. 20
The patents' clinical disease stage was determined based on a modified M-ANNHEIM clinical staging score: clinical stage I; no evidence of EPI or DM, clinical stage II; evidence of EPI or DM, clinical stages III and IV; evidence of EPI and DM. 5 Stage III patients (painful complete pancreatic insufficiency) and stage IV (nonpainful complete pancreatic insufficiency) were grouped to ensure a sufficient number of patients for statistical analysis.
Pancreas-specific plasma amylase
Pancreas-α-amylase (Amy-P) was analysed using Cobas 8000 C 502 according to the manufacturer's instructions (Roche Diagnostics GmbH, Mannheim, Germany). Amy-P is a routine in vitro test for the quantitative determination of pancreatic α-amylase in human serum, plasma and urine. The measuring range is 3 to 1500 U/l with linearity within the whole range. After inhibition of salivary α-amylase by monoclonal antibodies, the pancreatic α-amylase is determined with an enzymatic colorimetric method measuring cleavage of the substrate 4,6-ethylidene-(G7)-1,4-nitrophenyl-(G1)-α-D-maltoheptaoside (ethylidene-protected substrate) by pancreatic α-amylase followed by hydrolysis of all the degradation products to p-nitrophenol with the aid of α-glucosidase (100% chromophore liberation). The results of this method correlate with those obtained by high-performance liquid chromatography. This assay follows the recommendation of the International Federation of Clinical Chemistry and Laboratory Medicine. Precision over a 50-day period showed a coefficient of variation percentage (CV%) of 2% at 41 U/l and a CV% of 1% at 103 U/l. All biochemical analyses were conducted at Aalborg University Hospital; the test and the laboratory at this institution are accredited by the Danish Accreditation Fund (DANAK), the national accreditation body in Denmark (International Organisation for Standardisation 15189 quality standards).
Statistics
All data are reported as means ± SD unless otherwise indicated. The primary analysis was performed in the per-protocol population. Demographics and clinical characteristics and plasma amylase levels between patient subgroups were compared by chi-squared tests, analysis of variance or Kruskal–Wallis tests as appropriate. Uni- and multivariate linear regression models were used to analyse the association between plasma amylase level, disease duration and clinical assessment variables (EPI, DM, calcifications and aetiology of CP).
The diagnostic accuracy, sensitivity, specificity and post-test probabilities (likelihood ratios) of plasma amylase levels for diagnosing CP were calculated using area under the receiver operating characteristics curve (AUC). Optimal cut-off values were determined by maximising the Youden index. A prediction plot was constructed from a logistic regression model with plasma amylase level as continuous predictor. In addition to the primary analysis of diagnostic performance, a sensitivity analysis based on the intention-to-test population was performed. The software package STATA version 15.1 (StataCorp LP, College Station, TX, USA) was used for statistical calculations.
Results
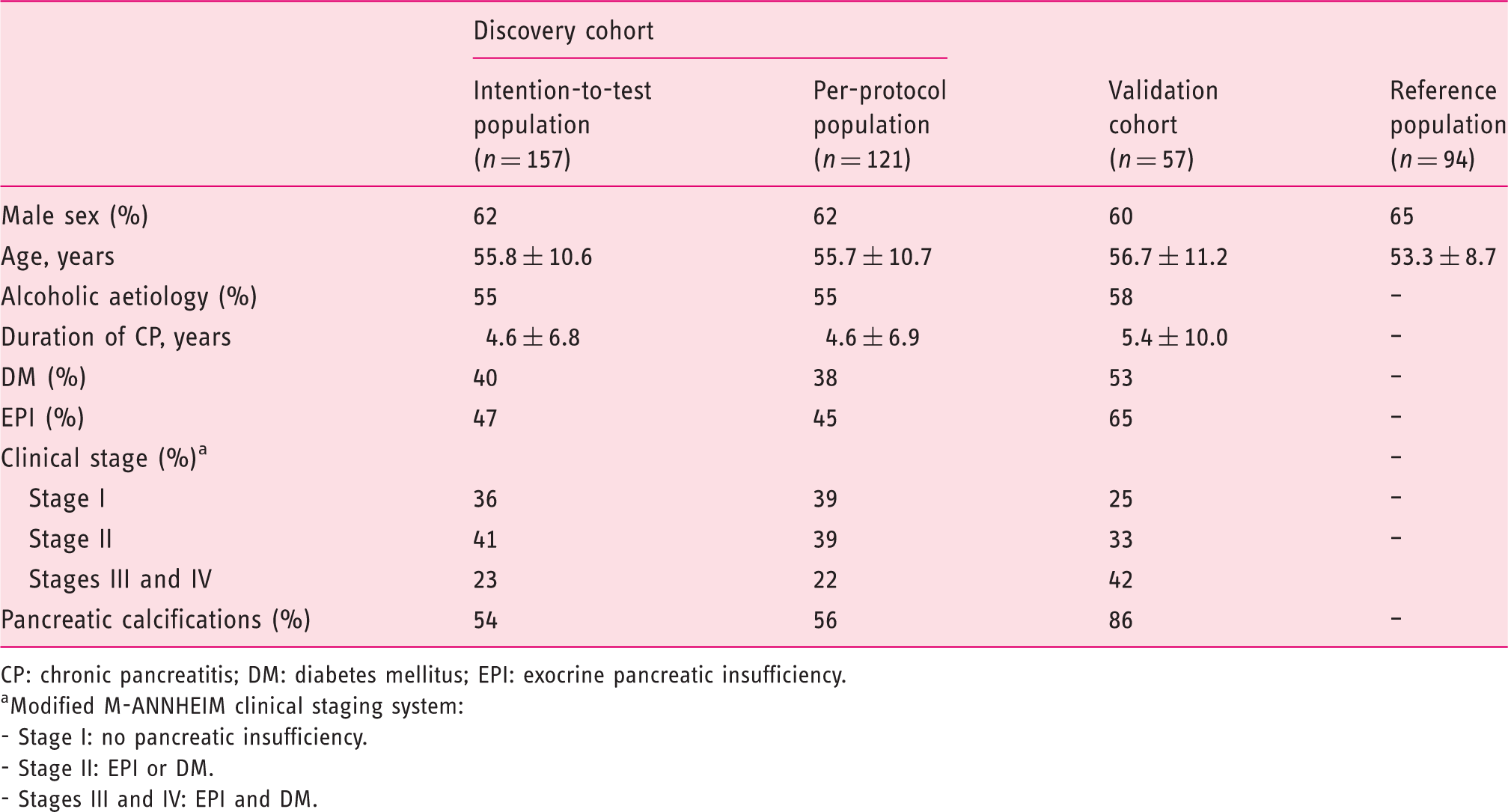
Between November 1, 2013 and February 30, 2017, we prospectively screened 182 patients with suspected CP for inclusion in the discovery cohort, of whom 157 were included in the intention-to-test population and 121 were included in the per-protocol population (Figure 1). The validation cohort was composed of 57 patients and the reference population of 94 healthy individuals who all had blood creatinine and amylase levels within the normal range. Mean age and gender distributions were comparable between the patient cohorts and the reference population (Table 1).
Study flow diagram. CP: chronic pancreatitis; ULN: upper limits of normal. Clinical and demographic characteristics of patients with chronic pancreatitis (discovery and validation cohorts) and the reference population. CP: chronic pancreatitis; DM: diabetes mellitus; EPI: exocrine pancreatic insufficiency. Modified M-ANNHEIM clinical staging system: - Stage I: no pancreatic insufficiency. - Stage II: EPI or DM. - Stages III and IV: EPI and DM.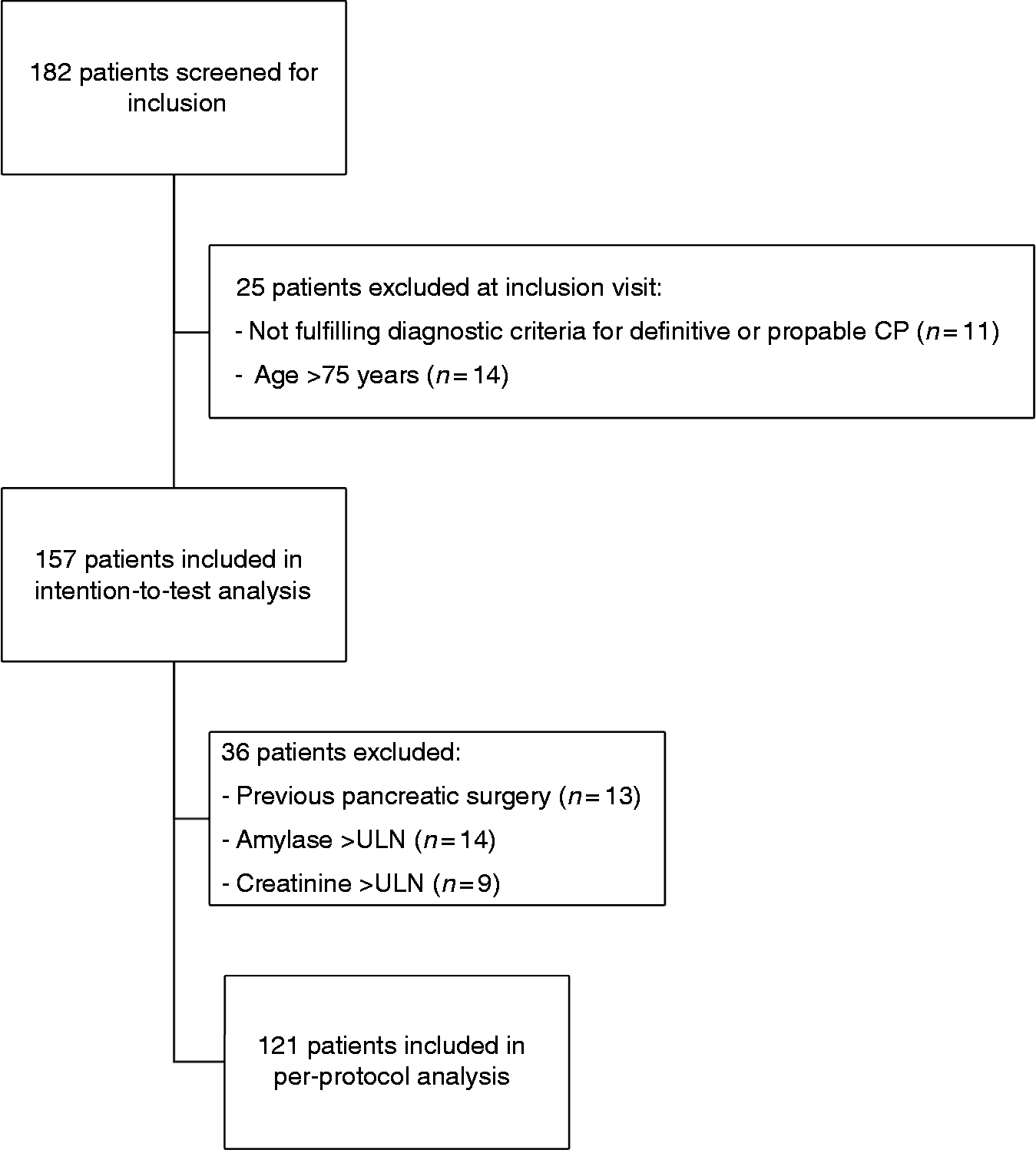
Amylase levels in the reference population and patients with CP
The median (interquartile range, IQR) amylase level was significantly decreased in patients with CP compared with the reference population (15.0 U/l (6.0–24.0) vs 26.7 U/l (21.7–34.2); p < 0.001) (Figure 2).
Pancreas specific plasma amylase levels in the reference population and in the discovery cohort of patients with chronic pancreatitis (CP), by pancreatic exocrine and endocrine function. HV; healthy volunteers. EPI; pancreatic exocrine insufficiency. DM; diabetes mellitus.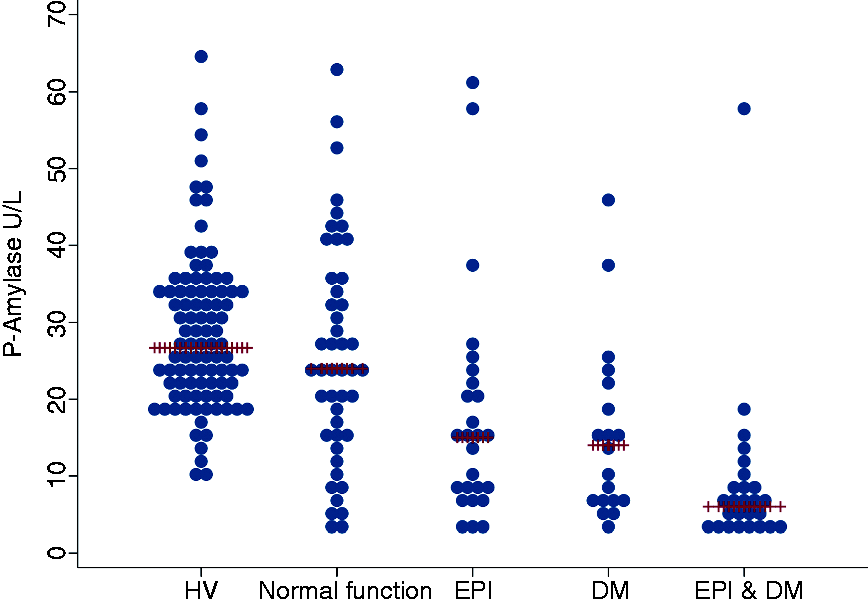
Amylase levels in patients with CP and associations with clinical characteristics
The median (IQR) amylase level was significantly decreased in patients with EPI compared with their exocrine-sufficient counterparts (8.0 U/l (5.0–16.0) vs 20.5 U/l (10.0–32.0); p < 0.001) (Figure 2). Also, patients with DM had decreased amylase levels compared with non-DM patients (7.0 U/l (5.0–15.0) vs 20.0 U/l (10.0–31.0); p < 0.001) (Figure 2).
A negative association between amylase level and duration of CP was observed (coefficient (ln-amylase) –0.04 ± 0.01 U/l; p < 0.001).
No difference in median (IQR) amylase levels between patents with or without pancreatic calcifications was observed (15.0 U/l (7.0–25.0) vs 15.0 U/l (6.0–24.0); p = 0.72). Likewise, no difference in median (IQR) plasma amylase levels was observed between patients with alcoholic and nonalcoholic aetiology (15.0 U/l (6.0–24.0) vs 15.0 U/l (6.0–24.0); p = 0.87).
Multivariate analysis of clinical parameters associated with plasma levels of pancreas-specific amylase in patients with chronic pancreatitis.
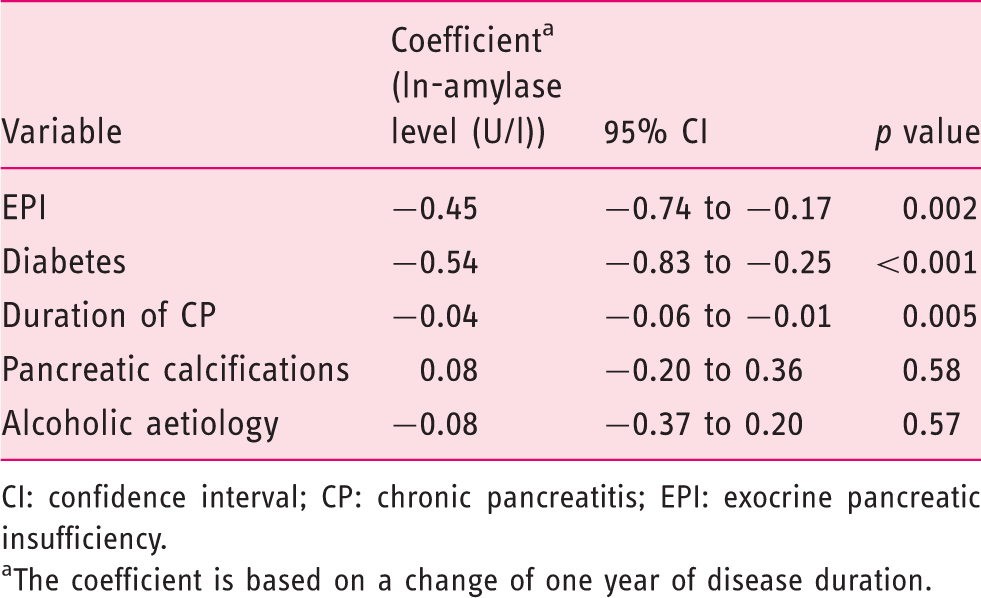
CI: confidence interval; CP: chronic pancreatitis; EPI: exocrine pancreatic insufficiency.
The coefficient is based on a change of one year of disease duration.
Diagnostic performance of plasma amylase level to diagnose CP
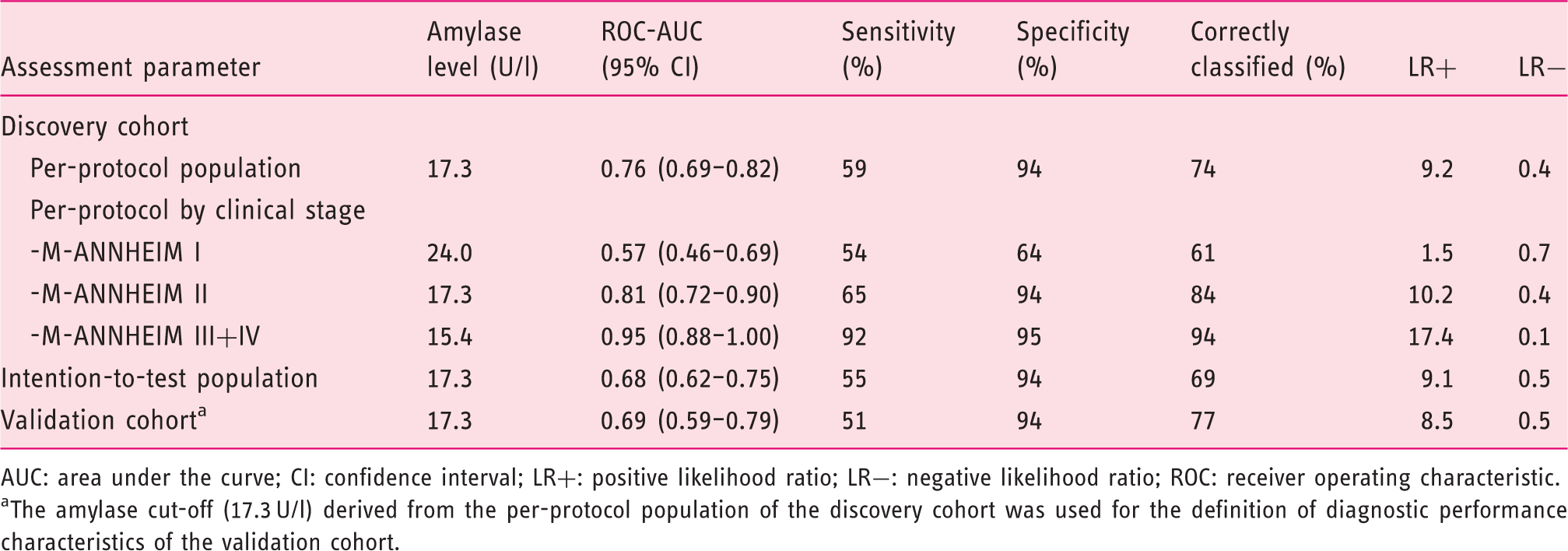
The optimal plasma amylase level cut-off for diagnosing CP was 17.3 U/l with a corresponding ROC-AUC of 0.76 (95% confidence interval (CI), 0.69–0.82), accuracy 0.74, sensitivity 0.59 and specificity 0.94 (Table 3). To aid in the interpretation of amylase levels, we created a prediction plot to determine the probability of CP as a function of plasma amylase levels (Figure 3).
Risk-prediction plot to evaluate the probability of chronic pancreatitis as a function of pancreas specific plasma amylase level. CP: chronic pancreatitis. Diagnostic performance of amylase level to diagnose chronic pancreatitis in the discovery and validation cohorts. AUC: area under the curve; CI: confidence interval; LR+: positive likelihood ratio; LR−: negative likelihood ratio; ROC: receiver operating characteristic. The amylase cut-off (17.3 U/l) derived from the per-protocol population of the discovery cohort was used for the definition of diagnostic performance characteristics of the validation cohort.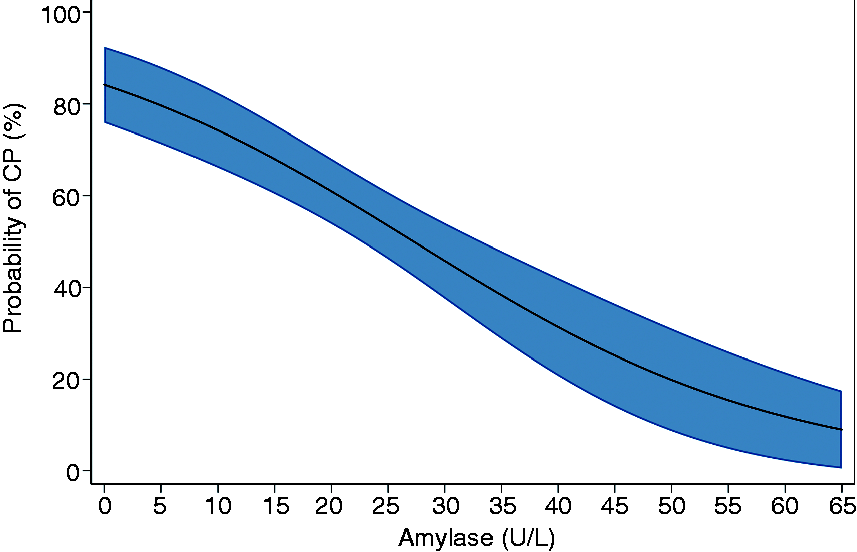
A stratified analysis of diagnostic performance of amylase levels by modified M-ANNHEIM clinical stage was performed to evaluate the influence of disease stage on diagnostic performance; overall, the diagnostic performance increased with advancing severity of CP (Table 3 and Figure 4).
(Upper panel) Sensitivity and specificity curves of pancreas specific plasma amylase levels to differentiate between healthy subjects and chronic pancreatitis patients, by M-ANNHEIM clinical stage. Optimal cutoff values for amylase levels to differentiate patients from controls are shown as vertical lines (M-ANNHEIM I; 24.0 U/l, M-ANNHEIM II; 17.3 U/l, M-ANNHEIM III-IV; 15.4 U/l. (Lower panel) ROC-curves of pancreas specific plasma amylase levels to differentiate between healthy subjects and chronic pancreatitis patients, by M-ANNHEIM clinical stage. ROC: receiver operating characteristic.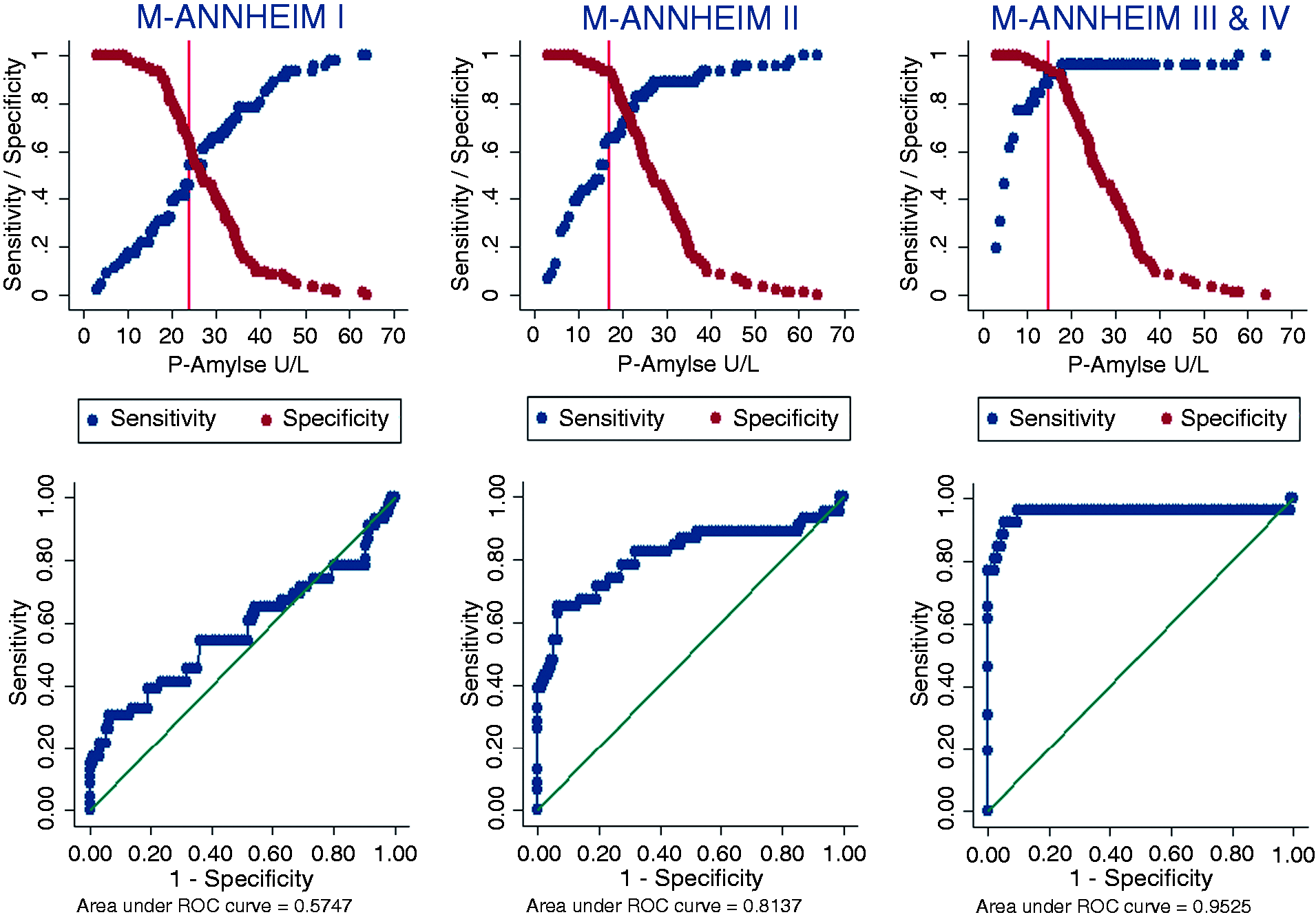
To further evaluate the stability of our results, we performed a sensitivity analysis in the intention-to-test population using the per-protocol amylase level cut-off value (17.3 U/l). The intention-to-test analysis had a negative effect on diagnostic performance; ROC-AUC 0.68 (95% CI, 0.62–0.75), classification accuracy (69%) and sensitivity (55%), whereas the specificity (94%) was comparable to that observed in the per-protocol analysis (Table 3).
Validation cohort
Plasma amylase levels stratified by the presence of EPI and diabetes are shown in Supplementary Figure 1. The median (IQR) amylase level was significantly decreased in patients with EPI compared with their exocrine-sufficient counterparts (11.8 U/l (6.2–19.9) vs 28.0 U/l (20.0–38.7); p < 0.001). Also, patients with DM had decreased amylase levels compared with non-DM patients (10.9 U/l (5.8–19.2) vs 26.4 U/l (16.3–40.2); p < 0.001).
The diagnostic performance characteristics of plasma amylase for the diagnosis of CP were replicated in the validation cohort. Using the plasma amylase level cut-off for diagnosing CP from the discovery cohort (17.3 U/l), the ROC-AUC in the validation cohort was 0.69 (0.59–0.79) with a corresponding accuracy of 77%, sensitivity of 51% and specificity of 0.94% (Table 3).
Discussion
We investigated the diagnostic utility of pancreas-specific amylase for assessment of CP; a plasma amylase level below 17.3 Ul had a high specificity and moderate sensitivity for the diagnosis of CP. However, the diagnostic performance was influenced by disease stage with the best performance observed for advanced CP. In line with this, we demonstrated significant and independent associations between plasma amylase level and duration of CP as well as the presence of EPI and DM. The main findings were validated in a second independent cohort of patients; in particular a high specificity for the diagnosis of CP was again observed. Our findings may have important clinical implications: First, we suggest that low plasma amylase is included in future diagnostic criteria for CP as a specific, albeit insensitive, biomarker of CP. Second, we propose that patients with a low serum amylase are systematically evaluated for EPI and diabetes.
Plasma amylase levels and associations with EPI, DM and disease duration
Many previous studies have investigated plasma and serum levels of pancreatic enzymes in the context of pancreatic disorders including CP; while high amylase levels are typically seen in patients with acute pancreatitis, 13 low enzyme levels have consistently been reported across studies in patients with CP and pancreatic cancer and these observations are in line with our findings.6,14,15,8 However, most previous studies were based on analysis of plasma amylase that was not specific for pancreas, used outdated laboratory technologies and disease classification systems, and did not systematically investigate the associations among plasma amylase levels, EPI and DM.
We documented that EPI and DM were independently associated with plasma amylase levels, and these associations were not solely driven by disease duration, as both EPI and DM remained significantly and independently associated with plasma amylase levels in multivariate analysis. This is an important observation with direct clinical implications as the presence of a low plasma amylase level should prompt further investigation for DM and EPI. The mechanism underlying these associations cannot be determined from the present study, but it is plausible that the quantity and functional state of acinar cells in the pancreas account for the association between plasma amylase and EPI. Accordingly, the fibro-inflammatory process that characterise CP gradually replaces functional acinar cells with fibrotic tissue as the disease evolves.4,17,19 This process is further dependent on various accelerators such as genetic susceptibility as well as smoking and drinking habits, which have all been shown to be independently associated with disease progression.4,21,22 As such, it is not surprising that the association between EPI and amylase level was independent of disease duration, as patients with CP may develop acinar dysfunction and EPI on various time points during their disease course depending on the aforementioned parameters.4,21,22
The mechanisms accounting for the association between DM and plasma amylase levels are more puzzling. Cross-talk between acinar cells, endocrine pancreatic cells and the gut, mediated via paracrine and incretin effects, have been well characterised and seem to be central for normal pancreatic endocrine and exocrine function. 23 Hence, abnormal or decreased insulinotrophic effects on acinar cells may lead to impaired exocrine function and possible lowering of plasma amylase levels. However, as the association between DM and plasma amylase levels was found to be independent of EPI, other mechanisms are likely also involved.
The association between pancreatic enzyme levels and disease duration has previously been investigated in patients with CP. Successive decreases in serum elastase, lipase and trypsin were observed during the course of CP, while no changes in amylase levels were observed during a nine-year follow-up study. 8 This is in contrast to the present study, in which a significant association between disease duration and plasma amylase levels was seen. A possible explanation for this discrepancy may be found in the test used for assessment of amylase levels. In our study, a pancreas-specific amylase was used, which is less sensitive to influence from extrapancreatic amylase sources such as the salivary gland, liver and female reproductive organs. 16
Calcifications and aetiology of CP were not associated with plasma amylase levels in our study. This is in line with previous observations and emphasises that a low plasma amylase level is a common characteristic both of calcific and noncalcific CP and independent of aetiology.14,15
Diagnostic performance of plasma amylase for assessment of CP
The diagnostic performance of plasma amylase levels to diagnose CP was improved compared to that reported in recent published reports, with a high specificity (94%) and moderate sensitivity (59%).14,15 This underlines that the finding of a low plasma amylase can mainly be used to rule in a diagnosis of CP, while the presence of a normal amylase cannot be used to rule out the disease. The improvement in diagnostic utility of pancreas-specific amylase was mainly confined to better sensitivity compared to previous reports. This may be explained by the use of pancreas-specific amylase as discussed above, and the characteristics of the patient population, which comprised a broader spectrum of CP patients than in previous reports.
An important observation of this study was the association between disease stage and diagnostic performance. In agreement with previous reports, we found that the diagnostic performance improved with worsening of CP disease stage. However, we used a clinically based classification score that was solely based on the characterisation of pancreatic function and symptoms (M-ANNHEIM clinical staging of CP 5 ). This is in contrast to previous reports that based their classification of disease severity on morphological parameters. 15 As morphology is not closely associated with symptoms and disease burden in CP, the classification system employed in the present investigation probably reflects more clinically meaningful disease staging.24,25 Accordingly, the observed association between diagnostic performance and disease stage was a direct reflection and consequence of the aforementioned associations among plasma amylase level, EPI and DM. An important clinical consequence of this observation is that pancreas-amylase is not particular useful for assessment of early CP, for which methods such as endoscopic ultrasound, secretin-enhanced MRCP or even direct pancreatic function testing seem to be the most accurate. 12
Study strengths and limitations
This study was undertaken in a large group of well-characterised patients with CP encompassing the full disease spectrum. This allowed for a better characterisation of the influence of disease stage than has previously been undertaken.14,15 In addition, the large sample size and detailed characterisation of patients allowed for stratification and analysis of factors associated with abnormalities in plasma amylase levels that have not previously been explored systematically. Another strength of our study was the use of a pancreas-specific iso-amylase, which diminished bias and influence from extrapancreatic sources of amylase. 16
There are several limitations to our study: First, our findings need replication and validation in further independent cohorts before any certain conclusions can be made. Two, the study was undertaken at tertiary centres in patients with probable or definitive CP and the reference population comprised healthy volunteers with no known pancreatic or extrapancreatic diseases that could influence the plasma amylase level. Thus, the prevalence of CP was artificially set at a fixed point (56% in the discovery cohort), which precluded calculation of valid predictive values. In forthcoming studies, the diagnostic utility of plasma amylase for the assessment and diagnosis of CP should be evaluated in ‘low prevalence populations’ in primary and secondary settings with inclusion of clinically relevant control groups. Third, future studies should validate the utility of pancreas-specific amylase against more conventional methods (e.g. serum lipase activity or total plasma amylase levels) to better elucidate its diagnostic performance. 7 Finally, pancreas-specific iso-amylase is not entirely specific for pancreatic-derived amylase as it may also be derived from the gut during, for example, intestinal obstruction or perforation. However, in the current study we carefully selected patients with no evidence of extrapancreatic gastrointestinal diseases and consequently we find it unlikely that the amylase levels would have been significantly influenced by extrapancreatic sources in our study. 16
Conclusions
Pancreas-specific plasma amylase level is associated with EPI and DM and provides a clinically useful mean for assessment and diagnosis of CP (ruling in disease rather than ruling out). Diagnostic performance is influenced by disease stage, with the best performance observed for advanced CP. If these findings are confirmed and validated in independent studies, we suggest that pancreas-specific amylase may be included in future diagnostic criteria for CP.
Supplemental Material
Supplemental material for Pancreas-specific plasma amylase for assessment and diagnosis of chronic pancreatitis: New insights on an old topic
Supplemental material, Supplemental Material for Pancreas-specific plasma amylase for assessment and diagnosis of chronic pancreatitis: New insights on an old topic by Søren Schou Olesen, Henrik Krarup, Jakob Lykke Poulsen, Jeppe Hagstrup Christensen, Andrea Rhiannon Glynne Sheel, Robert Sutton, William Greenhalf, Christopher Halloran and Asbjørn Mohr Drewes in United European Gastroenterology Journal
Footnotes
Declaration of conflicting interests
None declared.
Ethics approval
Because no study-related procedures were undertaken, this study did not require ethical approval according to the North Denmark Region Committee on Health Research Ethics. Approval for data collection and storage was obtained from the Danish Data Protection Agency, Northern Denmark Region (2008-58-0028, project ID 2018-19).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
The informed consent requirement was waived by the North Denmark Region Committee on Health Research Ethics.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.