
Abstract
The epidemiology of chronic pancreatitis (CP) is incompletely understood. A number of difficulties exist in estimating the prevalence and incidence of CP. Long-term follow-up is often problematic, especially in chronic alcoholics, and obtaining a formal and standardised diagnosis can take years. The available studies are reasonably consistent in their estimation of the incidence of CP but few studies have attempted to estimate prevalence. Although life expectancy in CP is diminished compared with control populations, median survival lies in the range of 15–20 years. Such a survival would suggest a prevalence of CP rather higher than that determined from the survey studies. A recent epidemiological study in France found an annual incidence of 7.8 per 100,000. Assuming a survival of 15–20 years, the annual prevalence should be between 120 to 143 per 100,000. Overall, our understanding of the epidemiology of CP is poor compared with other illnesses. We consider that both prevalence and the rate of pancreatic insufficiency and of CP are currently underestimated. There is a distinct need for more studies to remedy this lack of knowledge.
Introduction
Chronic pancreatitis (CP) is a serious disorder which can have a severe impact on quality of life 1 in addition to life-threatening long-term sequelae.2,3 As well as pain, pancreatic exocrine insufficiency can result in malnutrition (in a population apt to neglect their nutrition). Longer-term complications include diabetes mellitus and pancreatic cancer.2,3
While understanding of this illness is improving, there are a number of aspects where knowledge is lacking. In particular, the epidemiology of CP is far from perfectly described. Difficulty in the formal diagnosis that requires long-term follow-up (a time necessary for the development of ductal abnormalities or pancreatic calcifications), and high variability in severity of the illness and evolution profile directly impact the quality of epidemiological studies that are scarce and limited.
While many patients with CP enter the health care system via a gastroenterologist or surgeon due to an acute manifestation such pancreatitis or pain, much of their long-term care is conducted in the community by general practitioners or diabetologists and is consequently less visible to epidemiological studies performed in the gastroenterological milieu. However, studies in which the incidence of CP is estimated from the number of cases presenting to gastroenterologists or surgeons make the assumption that acute pancreatitis or onset of chronic abdominal pain are always early manifestations of CP, an assumption which is in part false.
Most cases of CP are associated with heavy alcohol intake and cigarette smoking, and the associated stigma makes longitudinal follow-up of these non-compliant patients by the same physician difficult to accomplish. Thus, the incidence of CP is easier to estimate than is its prevalence.
In the context of this imperfect understanding of the epidemiology, and particularly of the prevalence of CP, the objective of the present review is to assess the current state of knowledge of the epidemiology of CP and of pancreatic exocrine insufficiency.
Problems in the diagnosis of chronic pancreatitis
The problems encountered by epidemiological studies are further compounded by the difficulty in rigorously diagnosing CP. No simple and reliable diagnostic test exists for early CP, and definitive diagnosis can take years to obtain.
Because histology is usually not available, the diagnosis of CP is primarily based on the demonstration of pancreatic ductal or parenchymal morphological and/or functional changes that typically develop over time in the course of the disease. 4 Diagnosis of CP is thus mainly based on imaging procedures (magnetic resonance cholangiopancreatography (MRCP), computed tomography (CT) scan, endoscopic ultrasound (EUS)). Functional testing of the exocrine secretion in this context may be of help in cases with inconclusive morphological findings, but this is rarely used in clinical practice since values are often in the normal range, at least at the beginning of the disease. Functional testing gives positive results only when endocrine or exocrine secretory capacities are largely decreased, which is late in the course of the disease. 5
Due to gas interposition and a low sensitivity for detecting mild to moderate changes in the disease, abdominal ultrasound is far from an appropriate method for the diagnosis of this illness in clinical practice. 6 This method, widely used for the diagnostic workup of patients with abdominal pain, will consequently miss the majority of patients with CP except those with advanced disease. While CT is an accurate method for detecting pancreatic calcifications and main duct dilation, it is not effective for earlier pancreatic changes such as mild parenchymal changes due to fibrosis. 6
MRCP, with or without secretin-induced stimulation of pancreatic secretion, associated with diffusion-weighted magnetic resonance imaging (MRI) or contrast (gadolinium)-enhanced MRI allows accurate evaluation of pancreatic ductal and parenchymal changes, together with a semi-quantitative evaluation of the pancreatic exocrine secretion.7,8 MRCP and MRI are therefore useful methods for the diagnosis of CP.
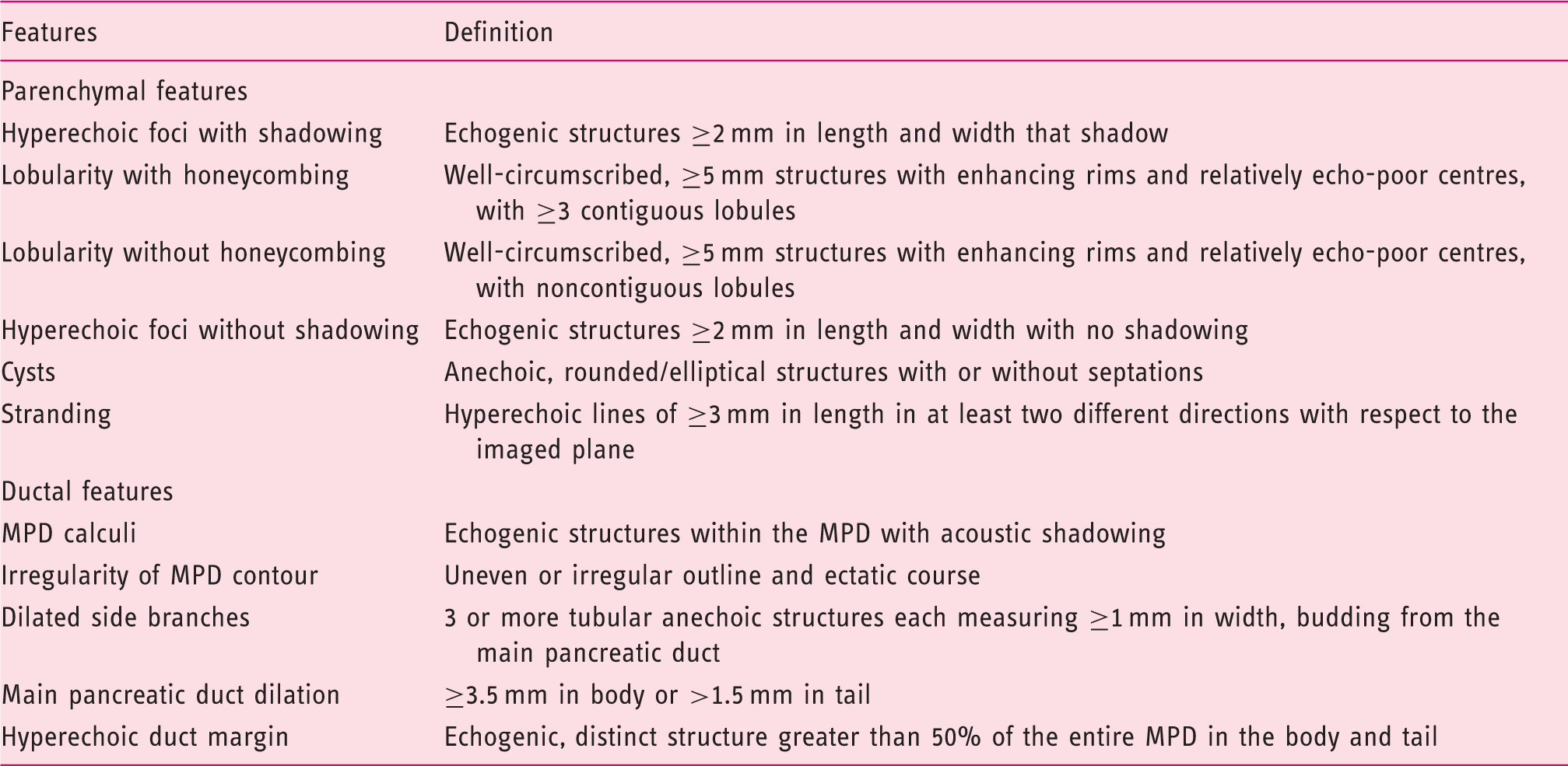
Endoscopic ultrasound criteria of chronic pancreatitis (Modified from Catalano et al. 12 )
Based on the scenario described above, it is easy to understand that the diagnosis of CP in clinical practice is a far from simple task. In practice, most cases of CP are identified from their clinical context (e.g. recurrent acute pancreatitis in heavy alcoholics) and confirmed several years later by abnormal duct imaging or the occurrence of pancreatic calcifications. Diagnosis of CP is even more difficult in the context of epidemiological studies, where simple, accurate and non-invasive tests are required. These considerations strongly suggest that CP is an under-diagnosed disease. In this context, clinical guidelines for the diagnosis and treatment are clearly required; some have been initiated or are in development in several countries.14–18
Epidemiology of chronic pancreatitis
While incidence provides information on the risk of developing a disease within a specified period of time, prevalence provides information on how widespread the disease is in the population. When the incidence is about constant over time, prevalence can be estimated as the product of disease incidence and average disease duration, typically the median life expectancy in cases of chronic disease. Incidence is generally easier to ascertain, especially in diseases starting on an acute mode, than prevalence as it relies on first manifestations. Depending on the disease, the diagnosis can be accurately obtained from medical, radiological, surgical or pathological departments.
Estimates of the prevalence of a chronic disease might be obtained from different sources if available such as national or regional registries (e.g. cystic fibrosis registries), population or hospital surveys, hospital discharge data or, in the absence of a direct measure, could be estimated using mathematical models based on available incidence and survival data.
Only scarce data are available on the prevalence and incidence of CP, while few reports on the long-term outcome and survival of selected series of patients with CP have been published.
Incidence of chronic pancreatitis
Some studies suggest that the role of alcohol as an aetiological factor may be less marked in, for example, Japanese or American populations, than it is in European populations. 27 Other studies emphasise the role of smoking, not only as a significant aetiological co-factor in CP,28–31 but also as a habit that accelerates the evolution and increases the mortality of CP. 32
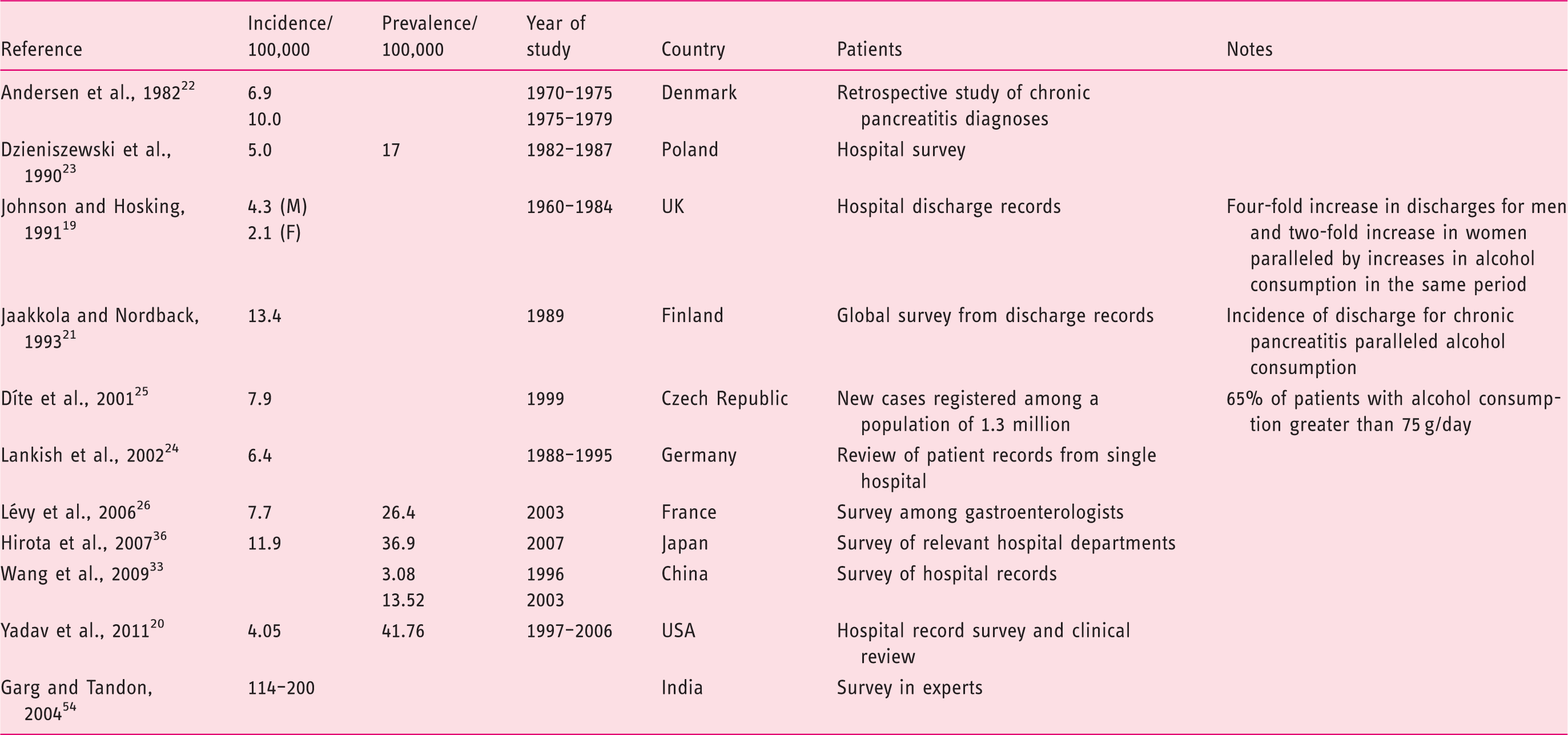
Certain trends are common to all the studies: there is a significant gender difference; men have a higher incidence of CP than women, at least twice as high. There is a trend for the most recent studies to show a higher incidence of CP. In the study of Jaakkola et al. in Finland, for example, incidence increased by 26% between 1977 and 1989. A study in China showed a marked increase in the prevalence of CP between 1996 and 2003 (from 3.08/100,000 to 13.52/100,000). It is noteworthy in this study that, in contrast to other studies from the Asia-Pacific regions, the majority of cases were among middle-aged patients and that the areas most affected by the increase were in the most westernised part of China. 33 Given this historical trend towards increasing incidence of CP and the lack of recent epidemiological studies, it is likely that the literature (as represented in Table 2) underestimates the current true rate of CP. In those studies where alcohol consumption was measured, a correlation between the increase in alcohol consumption and CP was a universal finding. 21 However, most of these studies were done in a period of generally rising alcohol consumption. In many countries in Europe, alcohol consumption has ceased to rise, (or has even begun to fall somewhat, particularly in southern Europe) but remains relatively high compared with the rest of the world. 34
The most recent epidemiological study (2006) in Europe in CP was conducted by one of the authors of this review (Lévy et al.). 26 This study recruited a significant fraction of all gastroenterologists in France and was methodologically rigorous. It was a cross-sectional epidemiological study that examined both the prevalence and incidence of CP. French gastroenterologists were asked to report the number of consultations undertaken for CP during a 3-month period and the number of new cases diagnosed during the same period.
A notable feature of this study was the apparent discrepancy between the incidence and prevalence of CP. This study estimated the prevalence at 15,830 cases and the incidence at 4646 per year (crude annual incidence: 7.8/100,000). Using the accepted epidemiological formula, these results would imply duration of illness of around 3.4 years. An older study in Poland (in a hospital setting) determined both incidence and prevalence and, while both were lower than in the recent study in France, the ratio of prevalence to incidence suggests a duration of illness of less than 4 years, which is also far from clinical experience. 23
This discrepancy needs explanation. CP patients typically attend, or are referred to, a gastroenterologist or a surgeon for their first bouts of illness as it has a more acute presentation (including acute pancreatitis and abdominal pain) than later (where pain is not usually a feature, or is at least masked by treatments and acute pancreatitis is rarer). After 5 or 10 years of chronic illness, the main problems encountered are pancreatic exocrine insufficiency and diabetes mellitus, and such long-term care is normally in the hands of a general practitioner or diabetologist. Quantifying the number of patients being followed by general practitioners/diabetologists and no more by gastrointestinal specialists is difficult, but can be crudely approximated from the preliminary study by Lévy et al.: 41% of the general practitioners in the preliminary survey declared they saw at least one patient with CP on a regular basis in the last year, with a mean of 2.7 patients. Given there are approximately 56,000 general practitioners in France, this implies that 24,000 of them saw at least one patient, an average of around 65,000 CP patients. Some 30% of these patients (around 20,000) were not under the simultaneous care of a gastroenterologist and therefore invisible in the prevalence calculations of this study. A similar calculation applied to the patients under the care of diabetologists yields approximately a further 2500 patients invisible to surveys of gastroenterologists as a whole. These figures provide a prevalence estimate that is much more consistent with the incidence data collected by Lévy et al. Using the incidence figure of 4646 (from this study with a more reasonable life expectancy figure of 20 years (see following discussion)), implies a prevalence of CP of 92,920 patients in France. This figure can be considered an outer limit of the number of CP patients, since their life expectancy is known to be somewhat impaired compared with the population as a whole. 35
This conclusion is confirmed by another recent epidemiological study performed in Japan in 2007. 36 A large survey of 3027 hospital departments resulted in 1100 responses describing 6339 patients treated and 2217 new patients during the 1-year index period. The estimated incidence and prevalence were 11.9 and 36.9 per 100,000. Although comparing the incidence and prevalence of CP across populations with significant genetic and cultural differences is fraught with difficulty, it is noteworthy that the duration of illness implied in the Japanese study is very similar to that in the French study (3.1 vs. 3.4 years, respectively), and so far from clinical and investigational experience.
A recent study of the incidence and prevalence of CP in Olmstead County, USA, made use of unusual arrangements for the provision of medical care in its methodology. 20 In this US county, nearly all medical care is provided by a central hospital (renowned for keeping large longitudinal databases of patient records) and a single primary care centre. This permits more complete capture of epidemiological data than it is possible in the gastroenterologist-gatekeeper scenario. Interestingly, this study provided estimates of incidence (4.05/100,000) and prevalence (41.8/100,000), more in line with longevity estimates for patients with CP.
Natural history of chronic pancreatitis
CP is an illness whose natural history can be grossly divided into three phases with huge overlap.
The progression and duration of these phases are highly dependent on the causative factors and vary from one patient to another. Further, the sequence of events is not canonical, i.e. the various symptoms (pain, calcifications/stones, diabetes mellitus, exocrine insufficiency) can occur in all possible sequences. 37 The rate and severity of progression are influenced by the continuation or otherwise of alcohol and tobacco usage. 38 Smoking is currently proposed to be the driving force behind the progression of pancreatitis. Fibrosis, which progresses as a consequence of a repeated inflammatory response, develops, with a corresponding reduction in exocrine and endocrine tissues. 39
The relevance of the natural history of CP has two important implications for epidemiological studies. Gastroenterologists are most likely to become involved in the care of patients with CP during the early phase of the disease, in which pain and surgical interventions are principle features of the illness. Thus, surveys of gastroenterologists can yield useful incidence data, since the gastroenterologist acts as a gatekeeper through whom many patients with acute manifestations pass. However, the gatekeeper role of the gastroenterologist might be bypassed in those patients whose illness does not follow the ‘classical’ course, or in whom disease is already advanced and does not need digestive specialist care. Such patients would not be visible to surveys of gastroenterologists.
Duration of disease in chronic pancreatitis
Long-term survival of patients with chronic pancreatitis
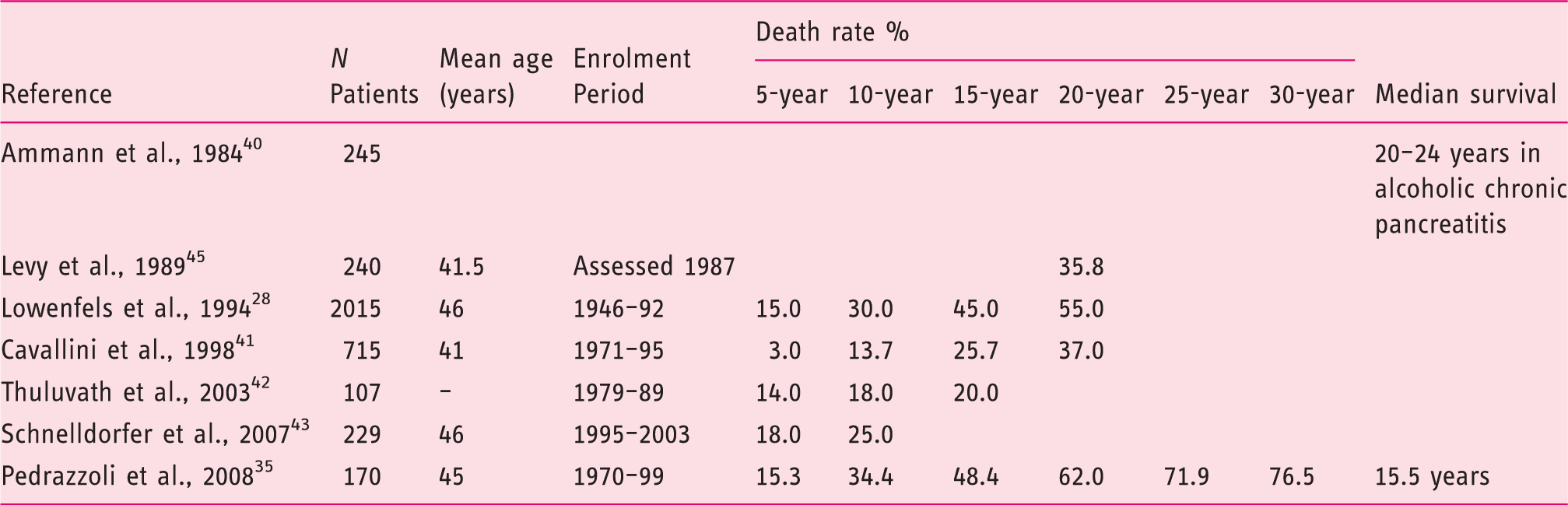
In all these studies, it is noteworthy that the majority of death (60–75%) is due to extrapancreatic consequences of alcohol and smoking over use (e.g. lung or oesophageal cancer, liver cirrhosis, heart attack) rather than CP by itself.
Only a single study has compared the mortality of CP with that of the population as a whole; a study in France compared the mortality and causes of mortality in 240 CP patients with that of matched control group from the general population. The mean age at onset of CP was 41.5 years and the mean age at death for the 57 patients who died during 8.7 years of follow-up was 52.3 years. The excess mortality compared with a matched French population was 35.8% over a 20-year course of illness. 45
From these reports (summarised in Table 3), it emerges that the median survival of CP patients is between 15 and 20 years from onset, and moreover, diagnosis is often delayed for several years from the start of the disease. In the studies by Thuluvath et al. 42 and Schnelldorfer et al., 43 for which follow-up was shorter, 82% and 75% of patients, respectively, were still alive after 10 years. We should keep in mind that the majority of patients with CP are heavy smokers, and are therefore exposed to the additional hazard of smoking. As a long-term follow-up of 34,439 male British doctors 46 demonstrated, on average, cigarette smokers die about 10 years younger than non-smokers, so we should expect that the life expectancy of patients with CP should be at least 10 years shorter than that of the general population. In the context of the most recent epidemiological data, 26 life expectancy at age 51 (median age of patients in this study) in France is 29.18 years for men and 34.92 for women (INED) 47 ). Thus, the life expectancy of patients with CP, for whom smoking is a major determinant of death, 28 is likely to be diminished significantly compared with the population at large. Clinical wisdom suggests a median survival in the range 15–20 years.
Pancreatic exocrine insufficiency
A large subset of patients with CP will suffer from pancreatic exocrine insufficiency and consequent malnourishment due to impaired digestion of nutrients, in particular fats, micronutrients and proteins. Although a proportion of patients present initially with abnormal pancreatic exocrine function, it is commonly associated with several years of evolution. Pancreatic function tests have therefore been used over decades for the diagnosis of the disease. 5 With this aim, only the secretin-pancreozymin test and the endoscopic test are sensitive enough. These tests are both invasive and cumbersome for routine use in clinical practice. The use of other functional tests such as the quantification of the coefficient of fat absorption and the 13 C-mixed triglyceride breath test are limited to just a few teams.5,48 Measurement of faecal fat output is complex, requires complete stool collection over at least 2 days and a lipid-rich diet for 4–5 days. In daily practice, it is very rarely performed nowadays. Faecal elastase is useful for detecting moderate to severe reduction of pancreatic secretion in patients with CP.5,49 This test has the advantages of being simple, non-invasive and easily applicable to routine clinical application, but sensitivity for the diagnosis of patients with non-advanced CP is limited. Other tests used in the past (e.g. Lundh test, N-benzoyl-tryosyl para-aminobenzoic acid test, pancreolauryl test, amino acid consumption test) are often no longer available for clinical practice.
A comprehensive meta-analysis of non-invasive pancreatic function tests concluded that none of the available methods possessed sufficient validity to diagnose mild to moderate pancreatic exocrine insufficiency. 50
Prevalence of pancreatic exocrine insufficiency in patients with chronic pancreatitis
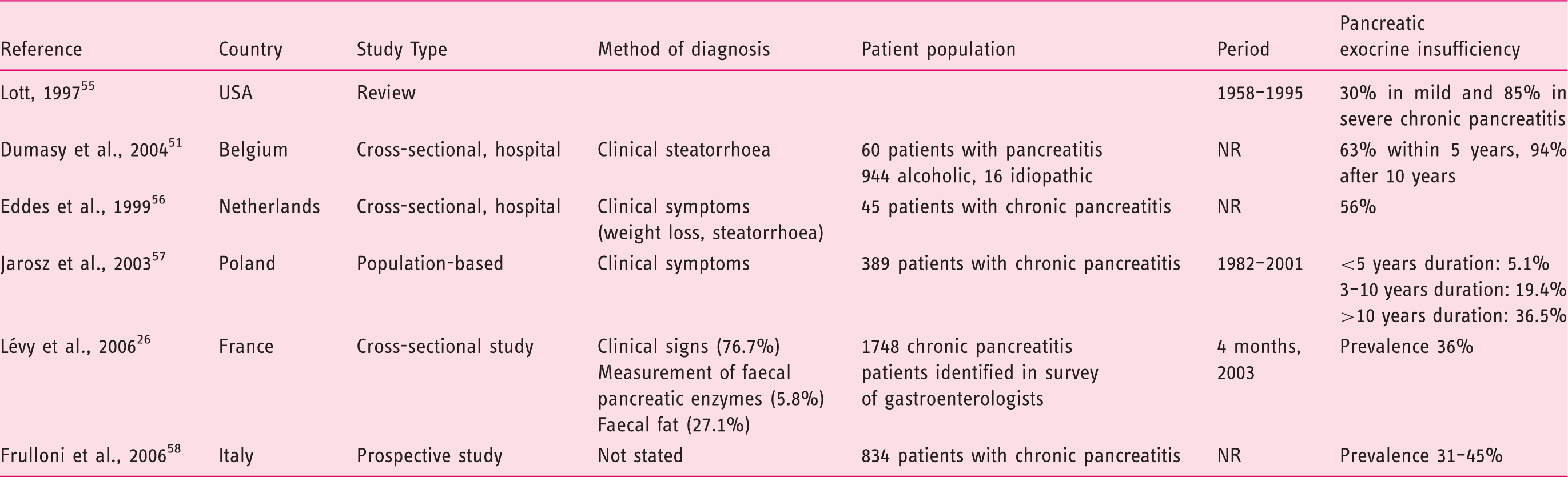
A cross-sectional study of patients with alcoholic and idiopathic CP suggests that pancreatic exocrine insufficiency is considerably more widespread than is generally assumed. Using acid steatocrit and triolein breath tests, this study identified malabsorption in 72% of patients, of whom only around one-third complained of clinical steatorrhoea. Exocrine dysfunction was present in 63% of patients after 5 years of CP and 94% of those with disease lasting 10 years or more. 53 Around 10% of CP patients with exocrine insufficiency have no pain and their diagnosis derives from investigation of either diabetes or steatorrhoea.
In summary, these studies (summarised in Table 4) suggest that the prevalence of pancreatic exocrine insufficiency among patients with CP varies widely from low/moderate (11–20%) to very high (85–94%). It is reasonable to reckon that pancreatic exocrine insufficiency is a feature in 35–50% of patients 10 to 15 years after clinical onset, and generally increases thereafter. However, cross-sectional, especially hospital or gastroenterologist-based surveys, face the same difficulties in studying the epidemiology of pancreatic exocrine insufficiency as they do in estimating the prevalence of CP. Pancreatic exocrine insufficiency is predominantly a feature of late-stage CP, and most of these patients are invisible to hospital- and gastroenterologist-based surveys since they are treated in the community.
Conclusion
Understanding of the epidemiology of CP has not improved in the last decade. The 2003 study by Levy et al. found an incidence of 7.8/100,000. This implied a prevalence of 90,000 patients in France (120–143/100,000), assuming a life expectancy of 20 years from onset of CP. The authors consider that the prevalence of the disease is probably underestimated for a variety of reasons, not least of these being the unreliability of alcohol-dependent patients in attending either hospital outpatient clinics or general practitioner facilities. More accurate incidence and prevalence data may in future be identified by greater utilisation of improved diagnostic approaches such as EUS. Coordination of data recording on CP patients by specialists in gastroenterology, diabetes, nutrition, surgery, psychiatry and general practice is needed to learn more about this disease in order to further medical knowledge.
Footnotes
Funding
Assistance with the preparation of the manuscript was provided by Dr JF Stolz and funded by Abbott.
Conflict of interest
P Levy has received honoraria and reimbursement grants for congress registration and travel from Solvay and Abbott and Mayoly Spindler on an irregular basis; M Lohr has received honoraria from Solvay and Abbott; E. Domínguez-Munoz has acted as advisor and speaker for Solvay and Abbott; C Imrie has received honoraria from Solvay and Abbott for consultancy and lecturing activities.
Acknowledgements
This review is based on the proceedings of the Chronic Pancreatitis Epidemiology Expert Working Group that was convened by Abbott in 2011. The Expert Working Group comprised the authors of this manuscript.