
Abstract
Background
Diabetes mellitus is a common complication of chronic pancreatitis. It is traditionally considered to develop as a consequence of beta cell loss, but there might be additional factors. Recent studies have highlighted the importance of type 2 diabetes-related risk factors in this context and population-based studies show increased risk of diabetes following acute pancreatitis. The aim of this study was to explore multiple risk factors for diabetes in patients with chronic pancreatitis.
Methods
We conducted a multicentre, cross-sectional study of patients with definitive chronic pancreatitis according to the M-ANNHEIM criteria. We used multivariable logistic regression models to determine risk factors independently associated with diabetes.
Results
The study included 1117 patients of whom 457 (40.9 %) had diabetes. The mean age was 52.8 ± 14.2 years and 67% were men. On multivariate analysis, parameters indicative of beta cell loss (pancreatic calcification, exocrine insufficiency, pancreatic resection) were confirmed as independent risk factors for diabetes (all p ≤ 0.02). In addition, type 2 diabetes-related risk factors (dyslipidaemia and overweight/obesity) were associated with the presence of diabetes (all p ≤ 0.002). Patients with a history of pancreatic fluid collections (indicative of previous attacks of acute pancreatitis) had a marginally increased risk of diabetes (p = 0.07).
Conclusion
In patients with chronic pancreatitis the presence of diabetes is associated with multiple risk factors including type 2 diabetes-related factors. Our observations attest to the understanding of this entity and may have implications for treatment.
Key Summary
Summarise the established knowledge on this subject:
Diabetes mellitus (DM) is a common complication of chronic pancreatitis. Factors indicative of beta cell loss are well-established risk factors for DM. Type 2 DM-related risk factors and a history of acute pancreatitis may increase the risk of DM.
What are the significant and/or new findings of this study?
We confirmed risk factors for DM indicative of beta cell loss (pancreatic exocrine insufficiency, pancreatic calcifications, and pancreatic resection). Type 2-related risk factors (overweight/obesity and dyslipidaemia) conveyed an independent risk of DM. A history of acute pancreatitis only marginally influenced the risk of DM.
Introduction
Chronic pancreatitis (CP) is a fibro-inflammatory disease characterized by progressive replacement of the pancreatic parenchyma with fibrotic tissue. 1 Development of pancreatic exocrine insufficiency (EPI) and diabetes mellitus (DM) are foreseeable complications of CP and affects a large proportion of patients. 2 Whereas EPI typically develops as a result of acinar cell destruction and/or obstruction of the pancreatic duct, the mechanisms underlying DM in the context of CP are incompletely understood and likely involve a number of mechanisms in addition to reduced beta cell mass following destruction of islet cells.3,4
Recent studies have highlighted the importance of type 2 DM-related risk factors in patients with CP.3,5 Accordingly, Bellin et al. characterized a number of risk factors for diabetes in a large multicentre cohort study of CP patients from North America. 3 The risk factors included classic CP-related parameters such as EPI, calcifications and pancreatic resection (indicative of beta cell loss), and type 2 DM-related risk factors such as a family history of diabetes, dyslipidaemia as well as overweight or obesity (indicative of beta cell dysfunction and/or insulin resistance). In keeping with these findings, another study showed that genetic risk scores based on validated single nucleotide polymorphisms for type 2 DM were similar in CP and type 2 DM patients, but distinct from genetic risk scores in a non-diabetic control population. 5 As such, beta cell dysfunction and insulin resistance may be important mechanisms of DM in patients with CP in addition to beta cell loss. 6
Population-based studies have shown that patients with a history of acute pancreatitis (but without CP) have a more than two-fold increased risk for developing DM compared with the background population.7,8 As many patients with CP have a history of recurring acute pancreatitis, the mechanisms underlying DM following acute pancreatitis may also be relevant in patients with CP.9,10 However, previous studies have not explored this hypothesis, and the mechanisms underlying DM in patients with CP are probably multifactorial but incompletely understood (Figure 1).
Putative risk factors and implicated mechanisms for diabetes mellitus in patients with chronic pancreatitis.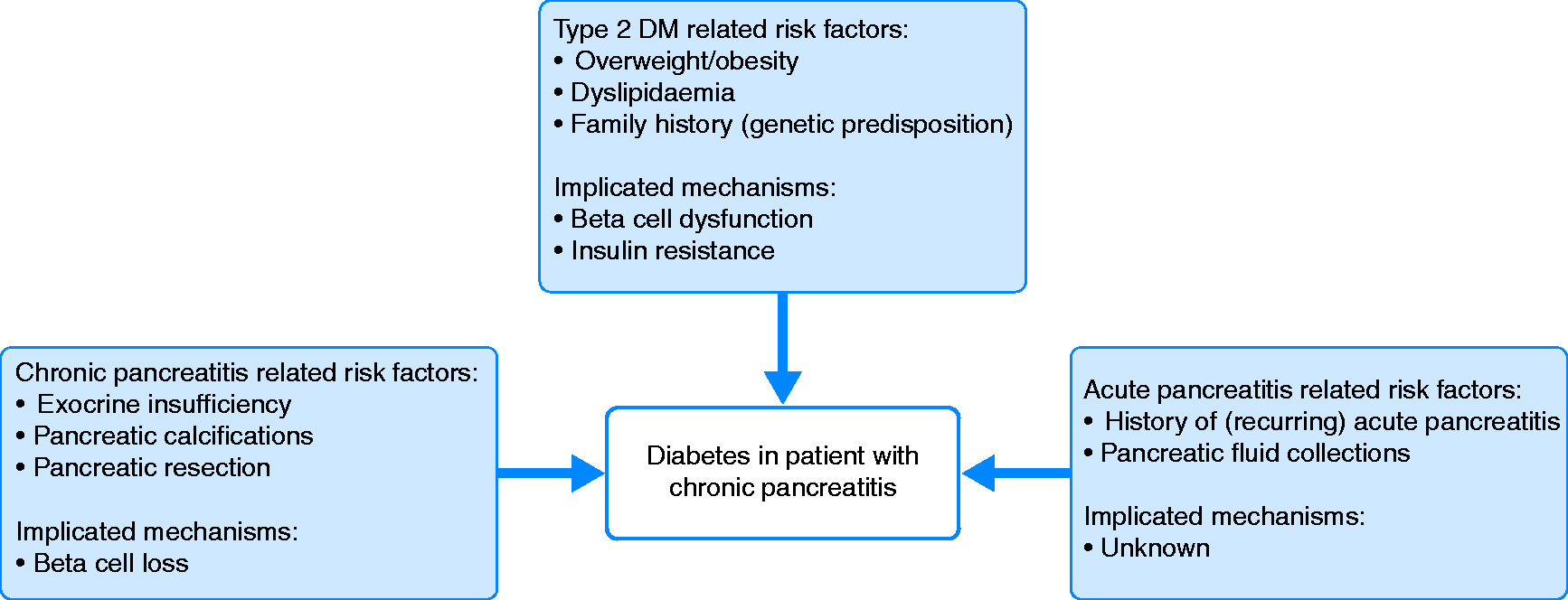
We investigated risk factors for DM in a multicentre cohort of more than 1100 patients with CP. We hypothesized that type 2 DM-related risk factors and a history of recurring acute pancreatitis would be associated with an increased risk of DM independently of classic CP-related diabetes risk factors. The aims of the study were: a) to determine the point prevalence of DM in a well-characterized Northern European cohort of CP patients and b) to define risk factors for DM using multivariable statistical modelling in combination with comprehensive assessment of acute and CP-related parameters as well as type 2 DM-related risk factors.
Methods
This was a cross-sectional, multicentre study based on the Scandinavian Baltic Pancreatic Club (SBPC) database. This database include data from a multicentre prospective registration of patients with CP initiated on 1 February 2016, 11 we derived data for the present study as of 12 August 2019. The dataset included registrations from 11 centres in eight countries, a detailed description of the methodology and study protocol of the SBPC database is provided in a previous publication.11,12 The M-ANNHEIM classification system was used to define CP and only patients with a definite diagnosis of CP (histology and/or pancreatic calcifications and/or marked pancreatic duct pathology (Cambridge grade 3 or 4)) were included. 13 These criteria were chosen to ensure a uniform characterization of our study cohort and to exclude patients with DM following acute pancreatitis (but without definite evidence of CP). 7
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki. The Centre for Pancreatic Disease at Aalborg University Hospital, Denmark served as the coordinating center. In agreement with Danish law and recommendations from the North Denmark Region Committee on Health Research Ethics, our study did not require written or informed consent because this was a register-based study and no study-related procedures were undertaken. Approval for data collection and storage was obtained from the Danish Data Protection Agency, Northern Denmark Region (2008-58-0028, project ID 2018–19).
Study assessment parameters
We retrieved information on patients’ demographics, aetiology and duration of CP, presence of EPI and DM, medical treatment as well as history of recurring acute pancreatitis based on review of medical records and patient interviews. Weight and height were measured and body mass index (BMI) calculated as weight divided by height squared. The World Health Organization classification for BMI was adopted for categorization of BMI into four subgroups: underweight BMI (BMI <18.5 kg/m2), normal BMI (18.5–24.9 kg/m2), overweight BMI (25.0–29.9 kg/m2) and obese BMI (>30 kg/m2). 14 The treating physician designated the most likely aetiological risk factor(s) according to the M-ANNHEIM system, no absolute risk-thresholds for smoking and alcohol consumption were adopted in this process. 13 A diagnosis of DM was based on the criteria commenced by the American Diabetes Association. 15 We used the faecal elastase concentration test, C13 mixed triglyceride breath test or faecal fat collection to characterize exocrine pancreatic function according to local practice at the individual sites. We defined EPI according to previously published criteria. 16 We reviewed imaging studies as part of routine clinical practice and information on pancreatic calcifications and pancreatic duct pathology was registered on the database. We retrieved information on endoscopic and surgical treatment from patient interviews and reviews of medical records. The following endoscopic procedures were registered: a) drainage procedures of pancreatic fluid collections (indicative of previous attacks of acute pancreatitis); b) common bile duct stenting and stone clearance; and c) stenting and stone clearance of the pancreatic duct. Surgery included: a) drainage procedures; b) pancreatic resection; and c) combined drainage and resection procedures.
Statistical analysis
We present data as numbers (%) for categorical variables and means (standard deviations (SD)) for continuous variables. We inspect QQ plots to determine if continuous variables are normally distributed and compare patient demographics and disease characteristics for CP patients with and without DM using Student’s t-test for continuous variables and Fisher’s exact test for categorical variables (univariate analysis). We use multivariable logistic regression with backward selection to assess the variables independently associated with the presence of DM and the TRIPOD recommendations are adopted in the design of statistical modelling. 17 Variables are included and removed one at a time according to their significance level (p < 0.15) until a final model is reached. In case a variable is considered to have clinical relevance, it is forced back into the model (history of recurring acute pancreatitis). The interaction between BMI categories and the presence of EPI is determined using a nested log-likelihood test, comparing a model containing the variables as single terms with a model also including the interaction term. 18 Results from multivariate analyses are presented as odds ratios (ORs) with 95% confidence intervals (CI). A significance threshold of p < 0.05 is used. The software package STATA version 16.0 (StataCorp LP, College Station, Texas, USA) is used for all statistical analyses.
Results
Patient and disease characteristics of the study cohort (n = 1107).
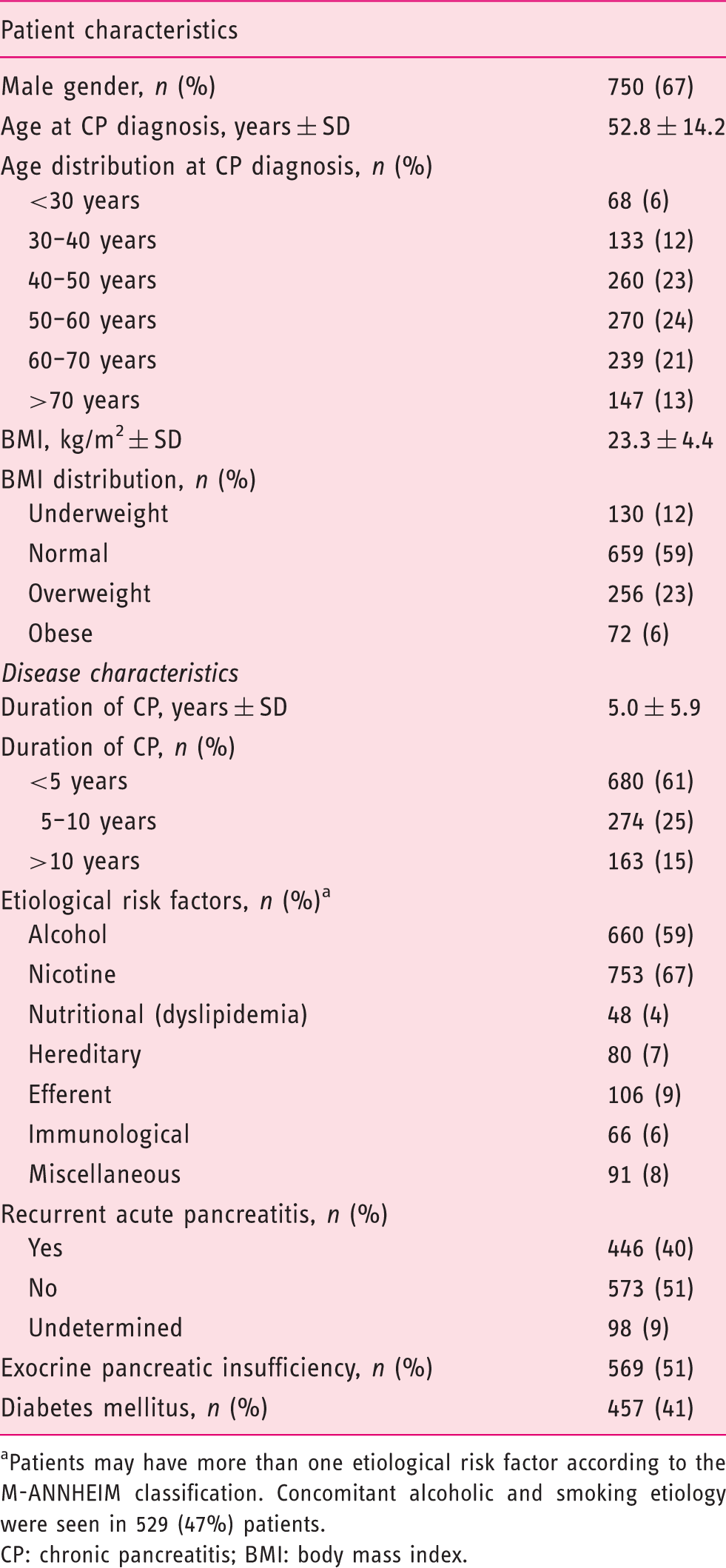
Patients may have more than one etiological risk factor according to the M-ANNHEIM classification. Concomitant alcoholic and smoking etiology were seen in 529 (47%) patients.
CP: chronic pancreatitis; BMI: body mass index.
Chronic pancreatitis related treatment modalities in the study cohort.
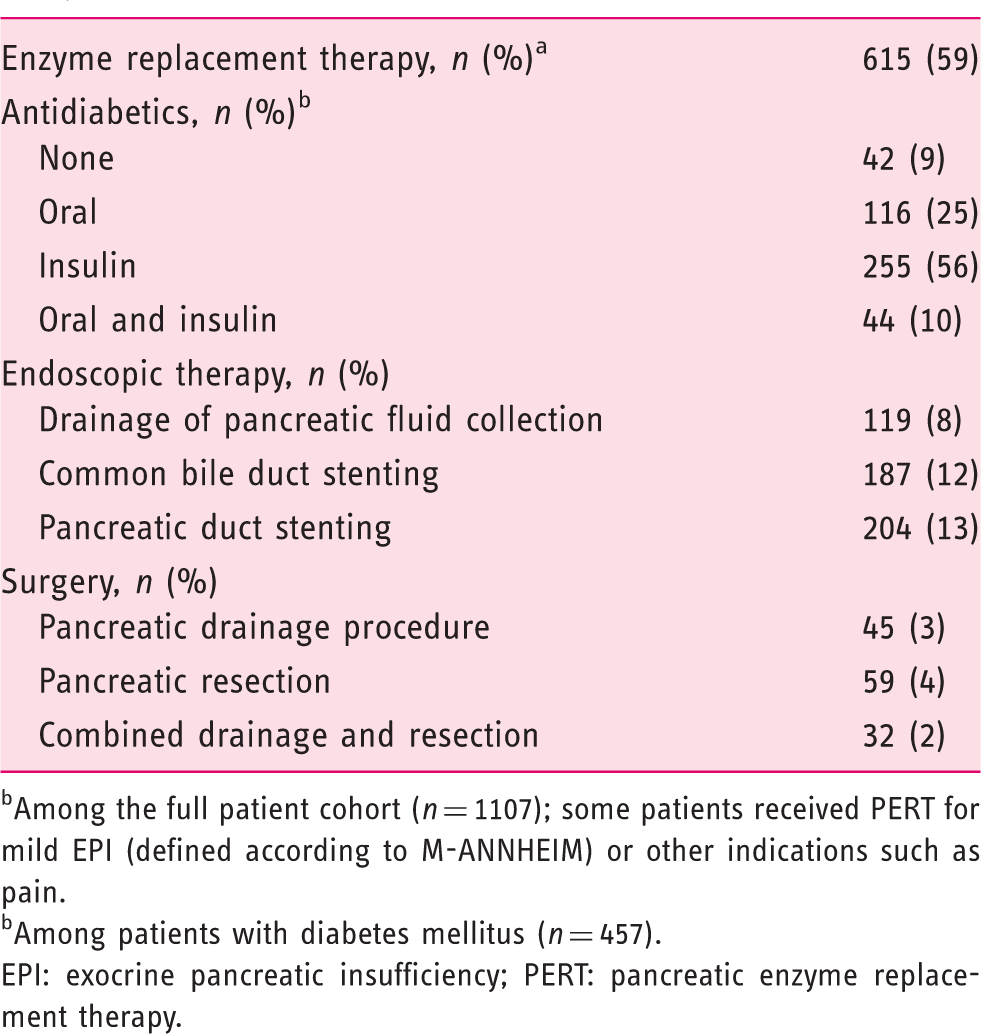
Among the full patient cohort (n = 1107); some patients received PERT for mild EPI (defined according to M-ANNHEIM) or other indications such as pain.
Among patients with diabetes mellitus (n = 457).
EPI: exocrine pancreatic insufficiency; PERT: pancreatic enzyme replacement therapy.
Prevalence of DM and antidiabetic treatment
DM was evident in 457 of the 1117 included patients, which corresponds to a point prevalence of 40.9% (95% CI, 38.0–43.9%). The majority of patients with DM were treated with insulin-based therapies (56%) or oral antidiabetics (25%), with 10% of diabetics receiving both oral antidiabetics and insulin (Table 2). A small proportion of patients with DM (9%) were managed without antidiabetic drugs; some of them were newly diagnosed with DM and consequently had not yet received treatment.
Single parameters associated with DM (univariate analysis)
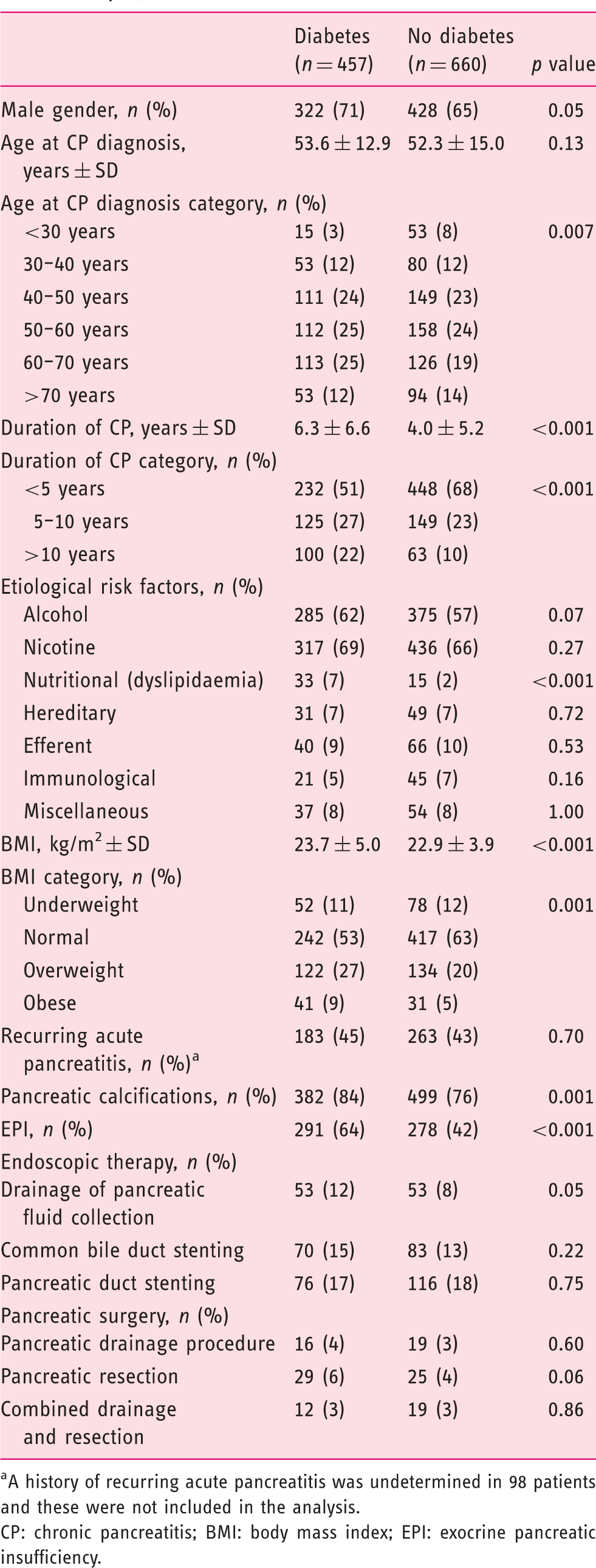
Results of the univariate analysis are reported in Table 3. Patients with DM were more likely to be diagnosed with CP at an older age compared with their non-diabetic counterparts (p = 0.007). Likewise, patients with long-lasting CP were more likely to have DM compared with patients with short-lasting disease (p < 0.001). Patients with dyslipidaemia (p < 0.001) as an aetiological risk factor were more likely to have diabetes, whereas no differences were observed for the remaining aetiological risk factors. In addition, patients with a BMI in the overweight or obese categories were more likely to have DM (p < 0.001). The presence of EPI was more frequently observed in patients with diabetes (p < 0.001) and conveyed an elevated risk for DM across all BMI categories (Figure 2). Likewise, pancreatic calcifications was associated with an increased DM risk (p = 0.001), whereas the number of patients with a past history of recurring acute pancreatitis (p = 0.70), pancreatic resection (p = 0.06) and endoscopic drainage of pancreatic fluid collections (p = 0.05) was proportionate between patients with and without DM.
Prevalence of diabetes mellitus by body mass index (BMI) category and the presence or absence of exocrine pancreatic insufficiency. Percentages of patients with diabetes are shown in the figure for the individual subgroups. Patient and disease characteristics in chronic pancreatitis patients with and without a diagnosis of diabetes mellitus (univariate analysis). A history of recurring acute pancreatitis was undetermined in 98 patients and these were not included in the analysis. CP: chronic pancreatitis; BMI: body mass index; EPI: exocrine pancreatic insufficiency.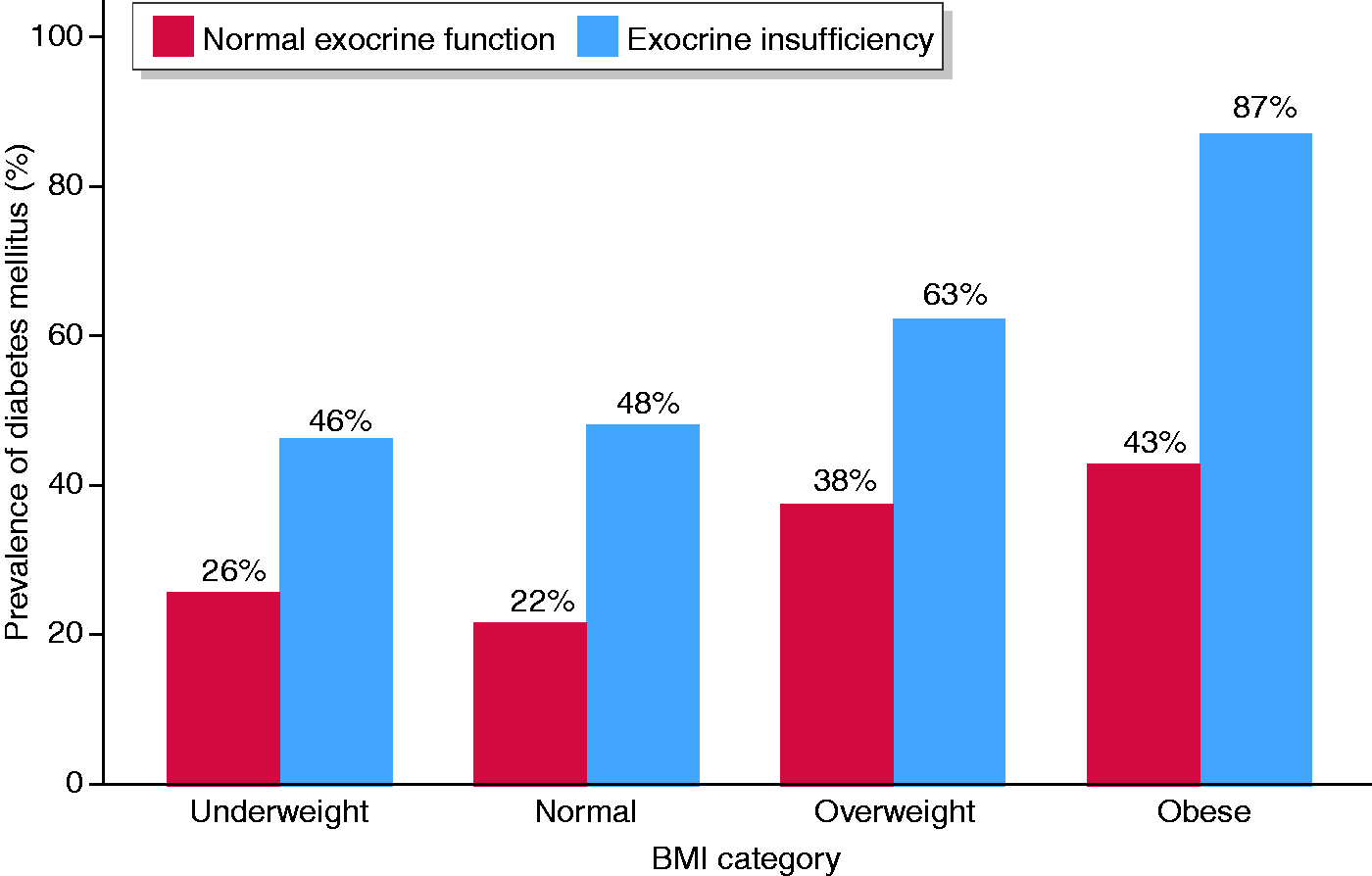
Independent parameters associated with DM (multivariate analysis)
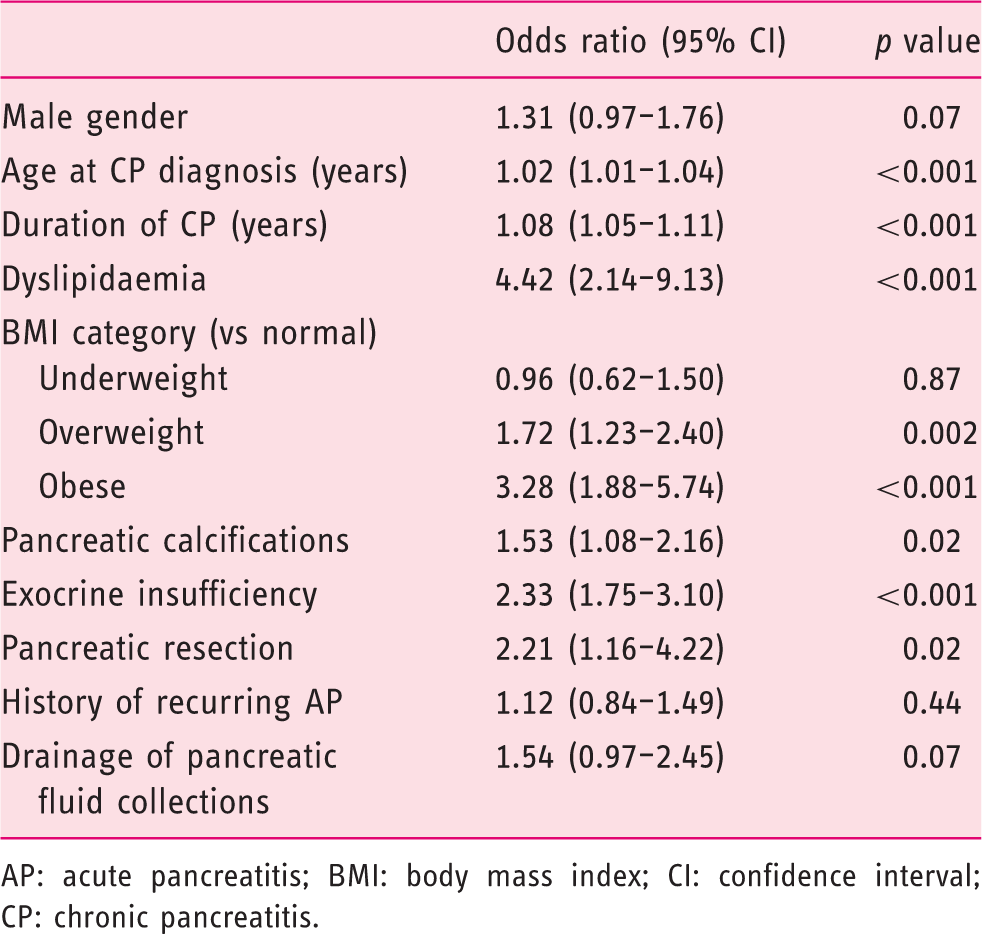
Results of the multivariate analysis are reported in Table 4 and illustrated in Figure 3. On multivariate analysis, age at diagnosis (p < 0.001), duration of CP (p < 0.001), dyslipidaemia (p < 0.001), overweight or obese BMI categories (p ≤ 0.002), pancreatic calcifications (p = 0.02), pancreatic resection (p = 0.02) and EPI (p < 0.001) were confirmed as significant and independent risks factors for DM. In contrast, risk factors indicative of a history of acute pancreatitis only marginally influenced the risk of DM and did not reach statistically significant associations (Table 4).
Forest plot of risk factors for diabetes mellitus in patients with chronic pancreatitis (CP) obtained from multivariable logistic regression modelling. Whiskers represent 95% confidence intervals. Multivariable analysis of patient and disease characteristics and the odds of having diabetes mellitus. AP: acute pancreatitis; BMI: body mass index; CI: confidence interval; CP: chronic pancreatitis.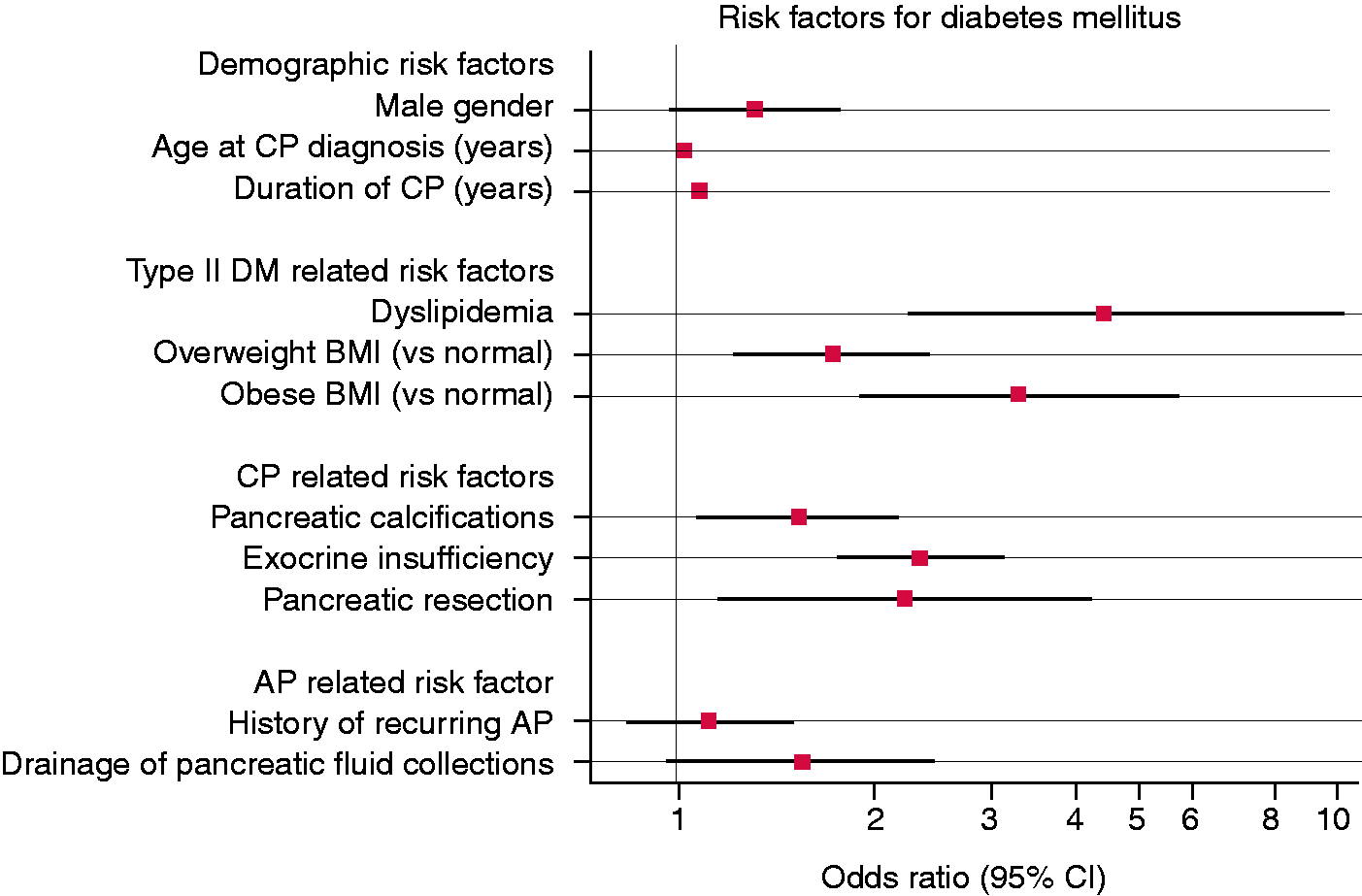
Discussion
We investigated the prevalence of DM and associated risk factors in a multicentre cohort of more than 1100 patients with a definite diagnosis of CP from a restricted geographical area. We found 40% of patients had DM and a number of risk factors were identified including classic CP-related risk factors indicative of beta cell loss (EPI, pancreatic resection and calcifications). In addition, we investigated factors relating to type 2 DM and acute pancreatitis. Although type 2 DM-related risk factors (dyslipidaemia and overweight/obesity) conveyed an increased and clinically relevant risk for DM independently of the classic CP-related risk factors, only marginal effects were observed from the risk factors associated with acute pancreatitis (previous history of recurring acute pancreatitis and pancreatic fluid collections). Taken together, these findings underline the heterogeneous mechanisms underlying DM in CP and may have implications for the treatment of this entity.
Prevalence of DM
The point prevalence of DM was approximately 40% in our cohort. This number is higher than that observed in the North American Pancreatitis Study (NAPS 2) cohort where 282 out of 1171 (29%) had DM. 3 The reason for the higher DM proportion in our cohort compared with the NAPS 2 study may be explained by different inclusion criteria and longer disease duration of the patients included in our study. Hence, prospective studies have shown the incidence of DM increases with prolonged duration of CP and approximately 50% of patients have diabetes 10 years after a diagnosis of CP has been established. 4 In contrast, some patients may develop DM after a relatively short period of CP as illustrated by our data where the mean duration of CP was only 5 years for the overall cohort; similar observations apply for the NAPS 2 study. 3 Taken together, these data emphasize that DM is a common complication of CP and not restricted to patients with longstanding disease.
Risk factors for DM
In keeping with findings from many previous studies we confirmed CP-related parameters (pancreatic calcifications, resection and EPI) as independent risk factors for DM.3,4,19,20 These parameters are mostly indicators of end-stage CP and the mechanism underlying the increased risk of DM are likely explained by beta cell loss, with gradual destruction of the islet cells as the fibro-inflammatory process evolves. Importantly, this process also affects the other endocrine cells in the pancreatic islets with concomitant destruction of alpha cells (glucagon), delta cells (somatostatin) and pancreatic polypeptide cells. 21 The clinical correlate of this process is a ‘brittle diabetes’ with patients experiencing highly fluctuating blood glucose levels and increased risk of hypoglycaemic episodes due to the lack of hormonal counterregulation. 22 This clinical phenotype is, however, only seen in a subset of patients that implies other DM-related mechanisms are likely operative.
In addition to the classic CP-related risk factors for DM, we confirmed the recent findings that type 2 DM-related risk factors also convey an increased risk of diabetes in patients with CP.3,5 Hence, overweight or obese patients and those with dyslipidaemia had increased risk of DM compared with their normal-weight and normolipidemic counterparts. Interestingly, the risk estimates (ORs) were even higher for the type 2-related risk factors compared with the CP-related parameters. Hence, the longstanding view of DM as a consequence of beta cell loss following fibrosis and atrophy may need to be revisited and reconsidered in a broader context including genetic risk of beta cell dysfunction and insulin resistance. Indeed, more than 400 single nucleotide polymorphisms have been identified and associated with an increased risk of type 2 DM, where the majority of disease-associated variants exert their effects through pancreatic islet dysfunction.6,23 Hence, it is conceivable that many patients with CP have a genetic predisposition for DM and together with a gradual loss of beta cells resulting from pancreatic fibrosis and atrophy, this may ultimately lead to the development of DM.
A novel aspect of our study was the inclusion of acute pancreatitis-related parameters (previous history of recurring acute pancreatitis and pancreatic fluid collections) as putative risk factors for DM.7,8 We observed marginal (and borderline significant) associations for the presence of pancreatic fluid collections and DM risk, but no association was observed for previous attacks of acute pancreatitis. This implies the mechanism underlying the two-fold increased risk of DM in patients with acute pancreatitis (but without CP) observed in population-based studies does not seem to be operative in the majority of patients with CP.7,8 Hence, it may be speculated that DM in the setting of acute pancreatitis is mediated through diverse and hitherto unrecognized mechanisms compared with the mechanisms involved in the development of DM in patients with CP.
Implications for treatment
The finding that type 2 DM-related risk factors are present in many patients with CP and diabetes may have implications for treatment. Currently there are no international guidelines for the management of pancreatogenic diabetes (type 3c DM), but most expert opinions recommend that patients are started on metformin in the presence of mild hyperglycaemia and shifted to insulin-based therapies in the absence of adequate glycaemic control.16,22,24 This is in keeping with the treatment modalities observed in our study where the majority of patients were on insulin treatment. As our understanding of the mechanisms involved in pancreatogenic diabetes evolves, it is most likely that additional antidiabetics, currently restricted for use in type 2 DM, may be useful in CP as well.
Our study was not designed to investigate if the presence of diabetes was associated with an underlying pancreatic malignancy. Recent high-quality studies have shown that hyperglycaemia is an early marker of pancreatic ductal adenocarcinoma.25,26 This knowledge should be incorporated in the management algorithms of patients with CP who have a nearly seven-fold increased risk of pancreatic cancer compared with the background population. 27 Hence, it is suggested to do a cross-sectional imaging study in CP patients with newly diagnosed (or severely dysregulated) DM to rule out the presence of an underlying malignancy. However, the cost effectiveness of such an approach will need validation in well-designed prospective studies.
Study limitations
A number of limitations of our study need to be mentioned. First, the cross-sectional study design precludes inference of causality between the observed associations. However, type 2 DM-related risk factors have previously been observed in patients with CP and population-based studies support an independent association between diabetes risk and previous attacks of acute pancreatitis.3,5,7,8 Second, the increased prevalence of type 2 DM-related risk factors (overweight/obesity and dyslipidemia) in our cohort may simply reflect that a proportion of patients had classic type 2 DM given the high prevalence of type 2 DM in the general Western population. 28 However, within the limitations of this large epidemiologic study, it was not feasible to employ testing to distinguish type 2 DM from pancreatogenic diabetes. Along this line, we did not assess whether beta cell autoimmunity (type 1 DM) was a contributor to diabetes development in our cohort, but overall the prevalence of type 1 DM is below 1% and thus this is less likely to influence our findings. Third, we did not collect data on genetic risk for DM (family history or biomarkers). However, the aforementioned studies from the NAPS 2 consortium have investigated this thoroughly in previous studies and findings from these studies support our conclusions.3,5 Finally, our observations are restricted to a population dominated by alcohol and smoking related CP mostly from the Northern European countries and thus need further validation in populations with different aetiological risk factor profiles and in paediatric populations.29,30
Conclusion
DM in patients with CP is associated with multiple risk factors including parameters associated with loss of beta cell mass, but also classic type 2 DM-related risk factors including overweight/obesity and dyslipidaemia. These findings attest to the understanding of DM as a complex and multifactorial complication of CP and have implications for management.
Supplemental Material
sj-pdf-1-ueg-10.1177_2050640620901973 - Supplemental material for Multiple risk factors for diabetes mellitus in patients with chronic pancreatitis: A multicentre study of 1117 cases
Supplemental material, sj-pdf-1-ueg-10.1177_2050640620901973 for Multiple risk factors for diabetes mellitus in patients with chronic pancreatitis: A multicentre study of 1117 cases by Søren S Olesen, Jakob L Poulsen, Srdan Novovic, Camilla Nøjgaard, Evangelos Kalaitzakis, Nanna M Jensen, Trond Engjom, Erling Tjora, Anne Waage, Truls Hauge, Stephan L Haas, Miroslav Vujasinovic, Giedrius Barauskas, Aldis Pukitis, Imanta Ozola-Zālīte, Alexey Okhlobystin, Mikael Parhiala, Johanna Laukkarinen and Asbjørn M Drewes in United European Gastroenterology Journal
Footnotes
Acknowledgement
Study design and data collection: SSO, JLP, SN, CN, EK, NMJ, TE, ET, AW, TH, SLH, MV, GB, AP, IOZ, AO, MP, JL and AMD. Data management and statistical analysis: SSO and JLP. Drafting of the manuscript: SSO, JLP and AMD. Data interpretation, review of manuscript for important intellectual content and final approval of the manuscript: all authors.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
The study was approved by Institutional Review Boards at each participating centre in agreement with local law and requirements.
Informed consent
Informed consent was obtained as per request by Institutional Review Boards at each participating centre.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.