
Abstract
Background
Modulating gut microbiota is a potential treatment for irritable bowel syndrome (IBS). This meta-analysis explored whether fecal microbiota transplantation (FMT) is successful in treating IBS.
Methods
A systematic review was performed to find trials on FMT in IBS. Ratios and relative ratios (RR) of improvement for single-arm trials (SATs) and randomized controlled trials (RCTs) were calculated, respectively. Changes in IBS Severity Scoring System (IBS-SSS) and IBS Quality of Life (IBS-QOL) instrument compared to baseline in FMT versus placebo groups were pooled.
Results
In SATs, 59.5% (95% confidence interval (CI) 49.1–69.3) of IBS patients showed significant improvement. In RCTs, there were no differences between FMT and control in improvement (RR=0.93 (95% CI 0.50–1.75)) or changes in the IBS-SSS and IBS-QOL.
Conclusions
FMT was not effective in IBS. Variations in FMT methods and patient factors may contribute to the heterogeneous results of the trials.
Keywords
Introduction
Irritable bowel syndrome (IBS) is a disorder of gut–brain interaction (DGBI) with multifactorial etiology. 1 Motility disturbances, visceral hypersensitivity, altered mucosal permeability, immune activation, or systemic parameters affecting the gut–brain interaction have been considered as underlying mechanisms. 2
Dysbiosis plays an important role in the pathogenesis of IBS. 3 Accordingly, modulation of gut microbiota with agents such as probiotics, prebiotics, symbiotics, luminal antibiotics, and fecal microbiota transplantation (FMT) have been suggested as treatment options for IBS.4,5 FMT is defined as the transfer of gastrointestinal (GI) microbiota from a healthy donor into the GI tract of a patient with dysbiosis. 4 This is a strongly endorsed treatment strategy in refractory or recurrent Clostridioides difficile infection. 4 Although not part of a consensus, FMT has been recommended for other GI disorders, including inflammatory bowel disease and IBS.
Studies on the role of FMT in IBS are limited.6–20 Based on a narrative review, several case series showed favorable results for FMT. 4 Of five randomized controlled trials (RCTs) on IBS, the majority measured the IBS Symptom Severity Scoring System (IBS-SSS) as an outcome. In contrast, the selection criteria and the route and form of FMT were different between the trials. The results of those studies were inconsistent, and there was a lack of statistical power of the performed trials. Notwithstanding, some of the trials suggested that post-infectious IBS (PI-IBS) and the baseline microbiota status in the donors could predict success for FMT in IBS. 4
To overcome the inconsistency of the trials on FMT in IBS, we performed a systematic review and meta-analysis, and the findings are presented in this article.
Methods
In February 2019, two independent reviewers (M.K. and A.D.) searched PubMed, Embase, Google Scholar, and abstract books of Digestive Disease Week 2010–2018 and United European Gastroenterology Week 2010–2018 using (a) “irritable bowel syndrome,” (b) fecal, (c) stool, (d) microbiota, (e) transplant, (f) transfer, (g) “microb*,” (h) “(((((fecal) OR stool) OR microbiota) OR transplant) OR transfer) OR microb*,” and (i) “irritable bowel syndrome AND (((((fecal) OR stool) OR microbiota) OR transplant) OR transfer) OR microb*.” Single-arm trials (SATs) and RCTs on FMT in IBS were retrieved if the diagnosis of IBS was proven by physicians or was based on ROME I, II, III, or IV criteria when other GI disorders were excluded. Whenever an abstract and a full text of a project were published, data from the full text article were included. Figure 1 shows the flow diagram of study selection.
Flow diagram of study selection for the meta-analysis of fecal microbiota transplant (FMT) in irritable bowel syndrome (IBS).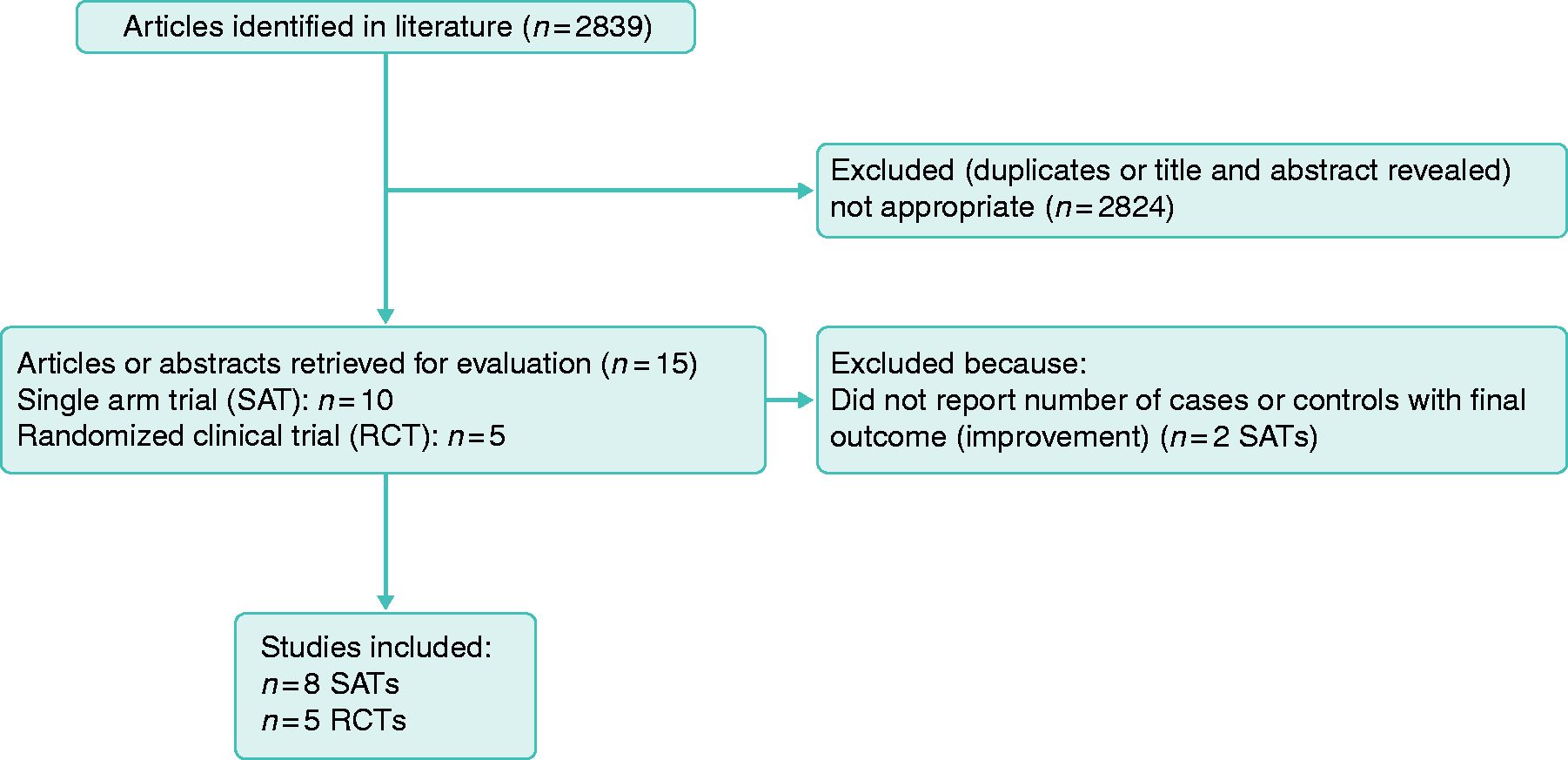
Quality assessment
Quality assessment for RCTs was based on the Jadad Scale, 21 Cochrane Collaboration’s tool for assessing risk of bias, 22 and the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) for level of evidence for the variables. 23
Data extraction
The total number of studied patients, number of patients with symptom improvement, and the M±SD of the IBS-SSS and IBS-QOL at baseline and after FMT were extracted. Whenever data were presented in figures, data points were reconstructed using the image digitizer Graph Grabber v2.0 (Quintessa, Henley-on-Thames, UK). When M ± SD were not reported, they were estimated, as described previously. 24
Statistical analysis
Data analysis was performed using RevMan v5.3 (Cochrane, London, UK) and MedCalc v19 (MedCalc Software, Ostend, Belgium). Response to treatment was defined as number of patients with overall symptom improvement divided by the total number of studied patients and is reported as ratio (R) and 95% confidence interval (95% CI) and relative ratio (RR) and 95% CI for SATs and RCTs, respectively. Changes in IBS-SSS and IBS-QOL in FMT versus control groups were defined as Δ IBS-SSS and Δ IBS-QOL, which were equal to “baseline score” minus “score after treatment.” For Δ IBS-QOL, absolute values were included. IBS-SSS and IBS-QOL were compared using the mean difference (MD) and standard mean difference (SMD) methods, respectively. A positive MD for IBS-SSS indicated a tendency toward better response to FMT compared with placebo (control). Fixed- and random-effects models were used when I2 ≤ 50% and I2 > 50%, respectively. The results are presented as forest plots.
Results
Ten SATs7,11,12,15–18,25–27 and five RCTs10,13,20,28,29 on FMT in IBS were retrieved. Overall, eight SATs7,11,12,16–18,25,26 (n = 90 patients in total) and all five RCTs10,13,20,28,29 (n = 151 patients allocated to FMT and n = 105 controls) were included. One of the RCTs was published in full after the literature review and was later included.6,29 One trial reported separate IBS-SSS for patients treated with frozen or fresh FMT; the mean value for response to both types of FMT was calculated. 13
Summary of results of open-label single-arm trials of FMT in IBS.
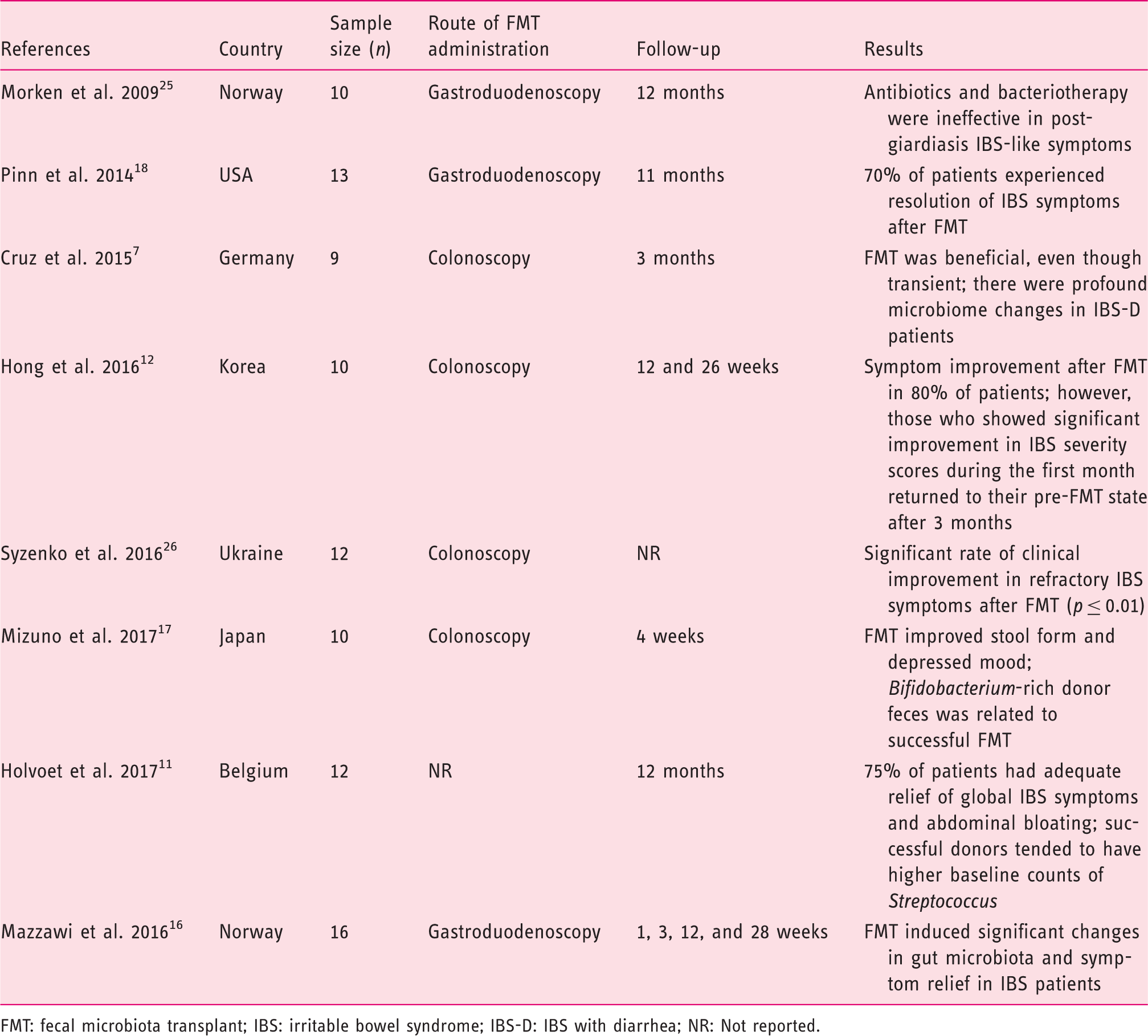
FMT: fecal microbiota transplant; IBS: irritable bowel syndrome; IBS-D: IBS with diarrhea; NR: Not reported.
RCTs of FMT in IBS.
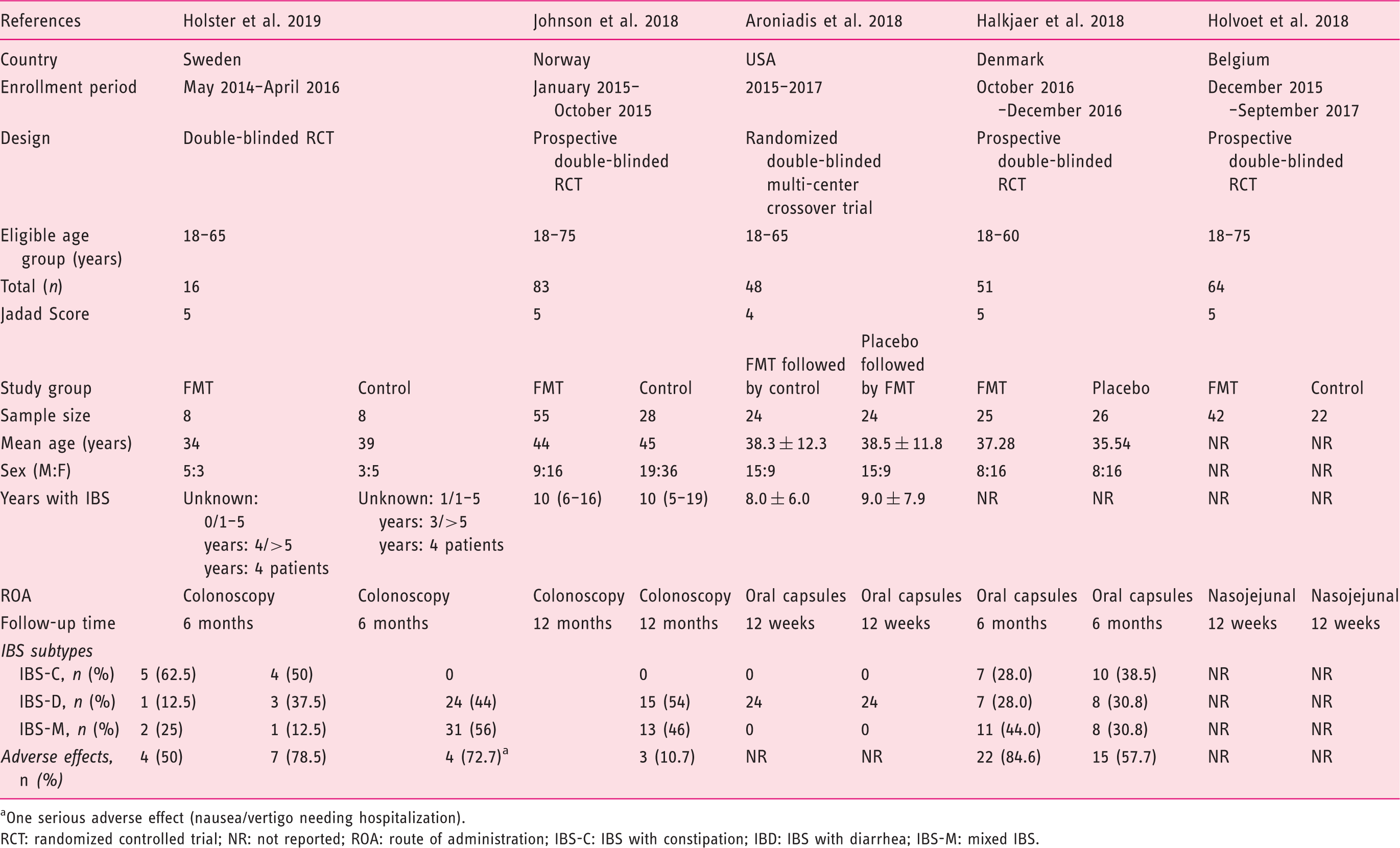
One serious adverse effect (nausea/vertigo needing hospitalization).
RCT: randomized controlled trial; NR: not reported; ROA: route of administration; IBS-C: IBS with constipation; IBD: IBS with diarrhea; IBS-M: mixed IBS.
The quality of the trials according to the Jadad Scale was good (score: five in four trials10,13,20,29 and four in one trial 28 ). The risk of bias of the RCTs is shown in Supplemental Figure S1. The level of evidence based on GRADE was very low (see Supplemental Table S1).
Outcome definitions, number of patients, duration of follow-up, and safety profile of the included studies have been discussed in a previous narrative review by our group. 4
Two RCTs that used oral capsules had real placebo as a comparator.20,28 The three other RCTs used autologous FMT as controls.10,13,29 The duration of the follow-up in the SATs ranged from 3 weeks to 18 months, while in the RCTs, it was up to 24 months.
In the SATs, R = 59.5% (95% CI 49.1–69.3) of IBS patients showed significant improvement of IBS symptoms (Figure 2). For the RCTs, 4-, 8-, 12-, and 24-week outcomes were selected for the analysis of IBS-SSS, and 12-week outcomes were selected for IBS-QOL. Holvoet et al. analyzed self-reported adequate relief of general IBS symptoms and bloating, finding that 49% of donor FMT recipients versus 29% of controls (p = 0.004) reached this outcome.
10
Discomfort, number of stools, urgency for a bowel movement, abdominal pain, and flatulence were significantly reduced by 19%, 13%, 38%, 26%, and 10%, respectively, in the FMT but not in the control group.
10
Aroniadis et al. analyzed the clinical response—defined as a decrease in IBS-SSS by ≥50 points at 12 weeks—and found no differences between the FMT and control groups (48% vs. 63%).
28
In the study by Johnsen et al., 36/55 participants receiving FMT and 12/28 receiving placebo showed a response by a decrease of >75 points in IBS-SSS at three months, favoring the active group (p = 0.049).
13
Meta-analysis of the RCTs showed no differences between the FMT and control groups in IBS symptom improvement, which was defined as self-reported satisfactory relief of IBS symptoms or decrease in IBS-SSS (RR = 0.93; 95% CI 0.50–1.75; Figure 3(a)) As response to treatment was not standardized in the included studies, changes in IBS-SSS from baseline would provide a better information in terms of response to FMT or control.
Meta-analysis of single-arm clinical trials (SATs) on the role of FMT in IBS. Data represent proportion (ratio), which is defined as the number of cases with improvement divided by the total studied cases. Meta-analysis of randomized clinical trials (RCTs) on the role of FMT in IBS. (a) Risk ratio or relative ratio: events indicate number of cases with improvement of symptoms. (b) Changes in IBS Severity Scoring System (IBS-SSS) after treatment at 12 weeks; negative values indicate decrease in IBS-SSS after treatment or improvement. (c) Crude changes in IBS Quality of Life (IBS-QOL) after treatment.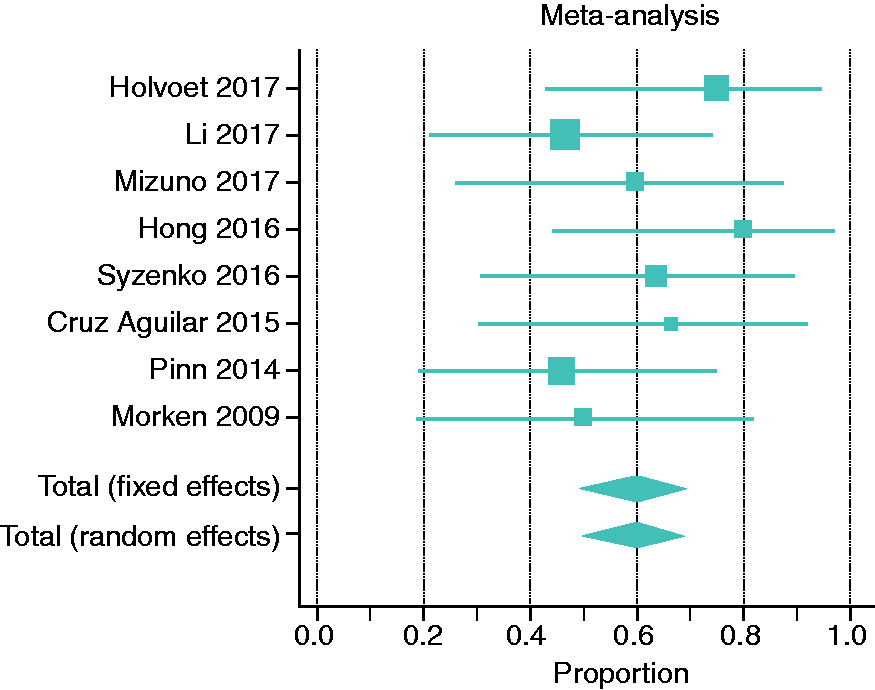
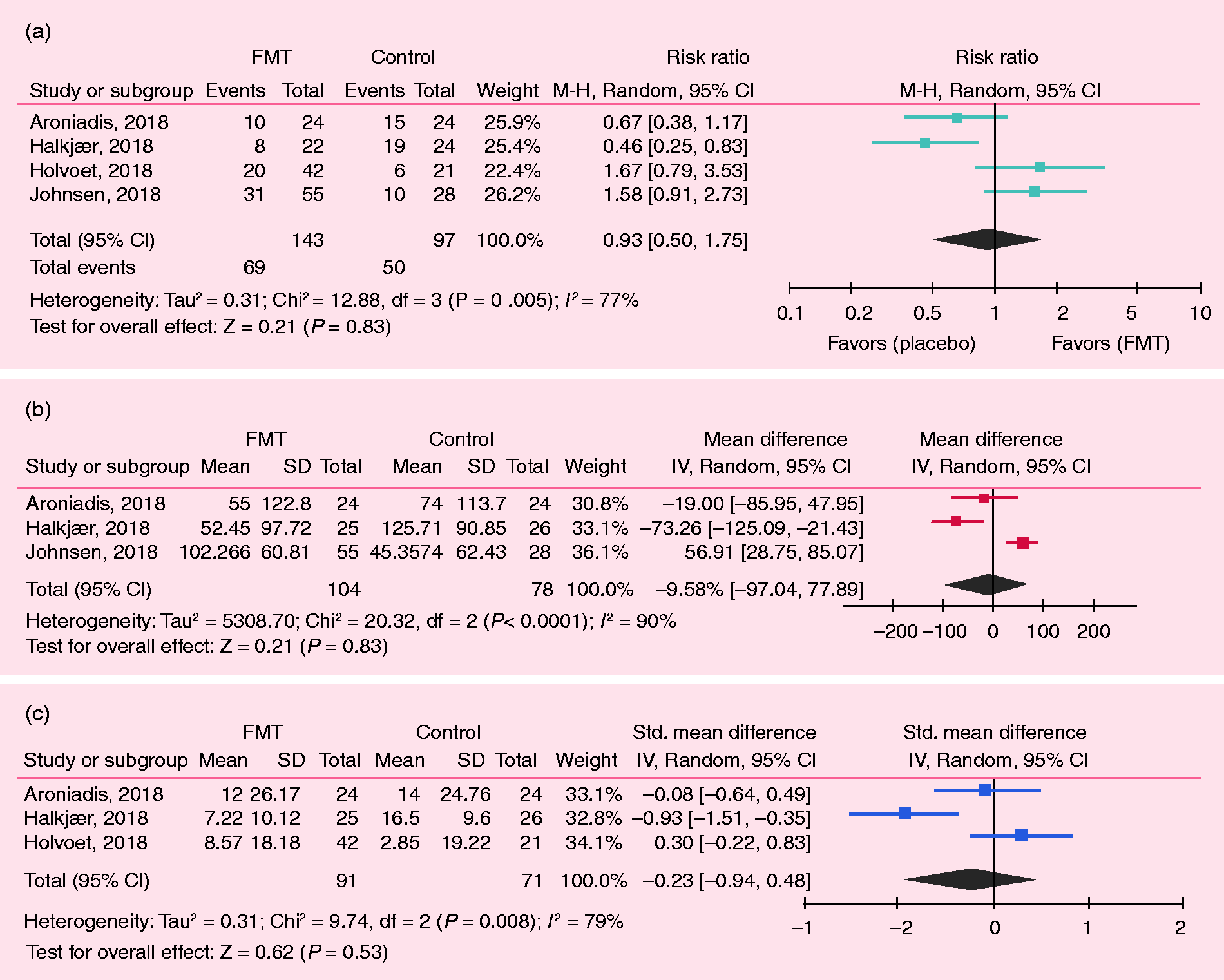
Four RCTs analyzed IBS-SSS.13,20,28,29 Johnsen et al. and Aroniadis et al.’s findings are described above. Halkjaer et al. used the IBS-SSS as the primary endpoint defining a positive effect in the presence of a 50-point reduction in this scale, showing a significant improvement at the three-month visit, favoring control treatment over FMT: M = 125.71 (SD = 90.85) versus M = 52.45 (SD = 97.72), p = 0.012. 20 Holster et al. did not observe a significant difference in IBS-SSS after allogenic and autologous treatments. 29 In the meta-analysis of the changes from baseline in the IBS-SSS, there were no differences in the FMT versus control groups: MD = –9.58 (95% CI –77.89 to 97.04) at 12 weeks (Figure 3(b)), as well as at 4, 8, and 24 weeks (Supplemental Figure S2).
Regarding the IBS-QOL, three studies compared the effect on IBS-QOL at 12 weeks.10,20,28 The first one by Aroniadis et al. found an improvement in IBS-QOL at 12 weeks versus baseline in both groups (FMT: 52 ± 19 vs. 64 ± 18; control: 53 ± 18 vs. 67 ± 17), without any difference between the groups. 28 Halkjaer et al. showed a significant improvement in FMT and control at 12 weeks, favoring control (–16.50 (9.60)) over FMT (–7.22 (10.12)) in the IBS-QOL. 20 Holvoet et al. showed an improvement of the IBS-QOL in the FMT group by 16%, with minimal changes in the control group at 12 weeks. In the meta-analysis of changes of IBS-QOL after treatment, there were no differences between the FMT and control groups (SMD: –0.23; 95% CI –0.94 to 0.48; Figure 3(c)). 10
No serious adverse event was reported in any of the RCTs, except for one case in the FMT group requiring a few hours of hospitalization (Table 2).
Discussion
Dysbiosis has been involved in the pathophysiology of functional GI disorders, now called DGBI, such as IBS. 30 Dysbiosis can be triggered by antibiotics or after an enteric infection, which can trigger PI-IBS. A study found lower Lactobacillus spp. in stool samples of diarrhea predominant IBS (IBS-D), while constipation predominant IBS (IBS-C) had increased Veillonella spp. 31 Kassinen et al. found differences in the genera Coprococcus, Collinsella, and Coprobacillus in IBS versus controls. 32 Carroll et al. revealed differences in the luminal and mucosal microbiota between IBS patients and controls and decreased microbial biodiversity in fecal samples of IBS-D patients. 33 Rajilic-Stojanovic et al. reported an increased ratio of the Firmicutes to Bacteroidetes phylotypes. 34 Tana et al. showed patients with IBS had higher Veillonella and Lactobacillus versus controls. 35 Jalanka-Tuovinen et al. identified an index of fecal microbial dysbiosis, which significantly distinguished PI-IBS from controls. 36 Therefore, currently, the abnormalities in the microbiota–gut–brain axis are considered an important underlying mechanism in the generation of IBS. 37
Bacteriotherapy or FMT, now approved for the treatment of recurrent or refractory C. difficile infection,38,39 has been proposed for the treatment of other disorders such as IBS. 4 To our knowledge, during the past few years, 10 SATs7,11,12,15–18,25–27 and five RCTs,6,10,13,20,28,29 on FMT in IBS have been published. In a previous narrative review, we found that FMT for IBS in the SATs was promising, while the RCTs provided conflicting results. 4 Two RCTs showed an improvement in IBS symptoms with FMT,10,13 and two other studies provided negative results.20,28 Therefore, we conducted this meta-analysis to explore the real efficacy of FMT in IBS. In summary, eight SATs fulfilled the inclusion criteria. In the SATs, 59.5% of IBS patients had significant improvement of symptoms. In contrast, in the RCTs, there were no differences between FMT and control treatment in IBS symptom, severity, or improvement in quality of life.
The inconsistent results on the RCTs could be related to several factors such as placebo effect. The relative placebo responses for IBS symptom severity is roughly 41.4% (range 25–59%), and for quality of life, it is between 20% and 125%. 40 In the RCTs reviewed in this meta-analysis, crude placebo response rates were almost similar to the response to FMT in SATs, suggesting that observations in the SATs would be mainly because of a placebo effect.
The routes and source of FMT could be considered a confounding factor. The two RCTs that used oral capsules did not show an improvement in IBS symptoms compared to placebo.20,28 In contrast, three other trials that used the nasojejunal and colonoscopy approach showed results favoring FMT.10,13,29 Whether FMT into the distal GI tract or the colon is more effective than the oral capsules in IBS needs further investigation. The oral route may result in small intestinal bacterial overgrowth. In addition, the number of bacteria delivered by oral capsules may not be sufficient. Notwithstanding, data from FMT in C. difficile infection have shown that oral capsules are not inferior to FMT delivered by colonoscopy for preventing recurrent infection over 12 weeks. 41 In addition, no difference has been found between frozen and fresh FMT. 42 This has also been observed when FMT was given orally administering a lyophilized microbiota product compared to a frozen product delivered by enemas. 43
Another issue that deserves attention is the effectiveness of FMT according to the IBS subtypes. However, data were not presented based on subtype in the majority of the studies. Although in terms of immunological profile of IBS we did not observe a huge difference between IBS-C and IBS-D,4,44 there is a possibility that a specific IBS subtype would have a better response to FMT.
The presence of dysbiosis might also be important in predicting response to FMT. Recently, Ghoshal et al. showed that treatment directed to manipulate the methanogenic microbiota improved chronic constipation only in the subset of patients colonized by this group. 45 As it is not expected that all patients would have dysbiosis, the inclusion of all unselected patients is not likely to yield a positive result with FMT. Another interfering factor is the donors’ and recipients’ fecal microbiota profile. Using patients’ own fecal material may not be considered as a true placebo. The other parameter is PI-IBS. According to Aroniadis et al., 28 a trend toward greater improvement was observed in PI-IBS patients who received FMT, but again we have to consider that the route of FMT administration in the above-mentioned study did not provide a dramatic improvement compared to those studies that used enemas as the route of FMT.
In conclusion, the current systematic review and meta-analysis does not support FMT as a successful treatment strategy in IBS. To address whether FMT would be helpful in IBS, larger studies with appropriate placebo groups and which take into account recipient and donor factors, including baseline microbiota profile, would be necessary. Stratifying data based on IBS subtypes and the presence of PI-IBS would decrease heterogeneity of the observations.
Supplemental Material
Supplemental material for Fecal microbiota transplantation in irritable bowel syndrome: A systematic review and meta-analysis
Supplemental Material for Fecal microbiota transplantation in irritable bowel syndrome: A systematic review and meta-analysis by Kanchana Myneedu, Abhizith Deoker, Max J Schmulson and Mohammad Bashashati in United European Gastroenterology Journal
Footnotes
Declaration of conflicting interests
M.J.S. received research support from Alfa Wassermann and Takeda Mexico, is a member of the Advisory Board of Alfa Wassermann Mexico, served as a consultant for Commonwealth Diagnostics International Inc., and has been a speaker for Takeda Mexico. K.M., A.D., and M.B. do not have anything to disclose.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.