
Abstract
Background
The safety and diagnostic accuracy of colonoscopy depend on the quality of colon cleansing. The adenoma detection rate is usually used as a quality measurement score.
Objective
We aimed to introduce and evaluate three new parameters to determine polyps and adenomas segmental localization and their distribution in association with different bowel preparation levels during colonoscopy. We introduce the multiple adenoma detection rate (the percentage of patients with >2 adenomas diagnosed during colonoscopy), the zonal adenoma detection rate (the percentage of patients with >2 adenomas diagnosed during colonoscopy in different colon areas (rectum, sigmoid, descending, transverse, ascending and cecum colon)), and multi-zone adenoma detection rate (the percentage of patients with >2 adenomas diagnosed during colonoscopy in different colon areas with at least a segment between them with or without lesions (i.e. rectum and descending colon with or without lesions in the sigmoid)).
Methods
We prospectively enrolled outpatients who underwent colonoscopy from January 2013 to October 2014. The bowel preparation quality, according to the Aronchick modified scale, number and location of lesions, Paris classification and histology, were recorded. The multiple adenoma/polyp detection rate, zonal adenoma/polyp detection rate, and multi-zone adenoma/polyp detection rate were determined.
Results
In total, 519 consecutive patients (266/253 M/F; mean age 55.3 ± 12.8 years) were enrolled. The adenoma and polyp detection rates were 21% and 35%, respectively. Multiple adenomas were detected in 28 patients. Adenoma and polyp detection rate and new parameters were statistically significantly higher in the optimal as compared with the adequate bowel preparation.
Conclusions
An optimal level of bowel preparation was strongly associated not only with a higher adenoma detection rate, but also with a higher chance of detecting multiple clinically relevant lesions in adjacent or discrete segments of the colon.
Introduction
Colorectal cancer (CRC) is a major cause of morbidity and mortality. 1 Colonoscopy is highly effective in detecting advanced neoplasia, and CRC prevention by endoscopic polypectomy reduces disease-specific incidence and mortality. 2 As such, its use as a preferred screening and diagnostic strategy is supported by official guidelines. 3
The long-term efficacy of colonoscopy in preventing CRC incidence and/or mortality has been addressed in cohort and case-control studies.4–6 Although the majority of these studies showed a very high CRC prevention rate, some studies showed a suboptimal CRC protection rate.7,8 This appeared to be related to an unexpectedly high risk of post-colonoscopy CRC in the early years after colonoscopy.
Quality of endoscopy has been strongly related to the risk of post-colonoscopy CRC.4,9 In large administrative cohort or case-control studies, the risk of early post-colonoscopy cancer appeared to be independently predicted by a relatively low adenoma/polyp detection rate (ADR/PDR). 10 This has been recently confirmed in a randomized controlled trial on sigmoidoscopy screening, in which the risk of distal interval cancer was significantly increased for patients of examiners with a low distal ADR. 11
A major determinant of the quality of colonoscopy is represented by an adequate level of bowel preparation (BP). 12 Indeed, a suboptimal level of cleansing has been consistently related to a higher rate of interval cancer. An inadequate level of cleansing has already been related to a decrease in the ADR, which by itself has been related to a higher risk of interval cancer. 13
The level of cleansing has been shown to differ according to the various parts of the colon. Thus, it cannot be excluded that even in those with inadequate preparation but in whom an adenoma has been detected, additional adenomas may have been missed in other segments with worse level of cleansing. This would expose these patients to a higher risk of subsequent neoplasia, even if apparently classified as adenoma-bearing patients.
The aim of our study was to assess whether an inadequate level of BP was associated not only with a lower ADR, but also with a reduced number of adenomas per patient, taking into account the spatial distribution of these lesions.
Materials and methods
Patient population and colonoscopy characteristics
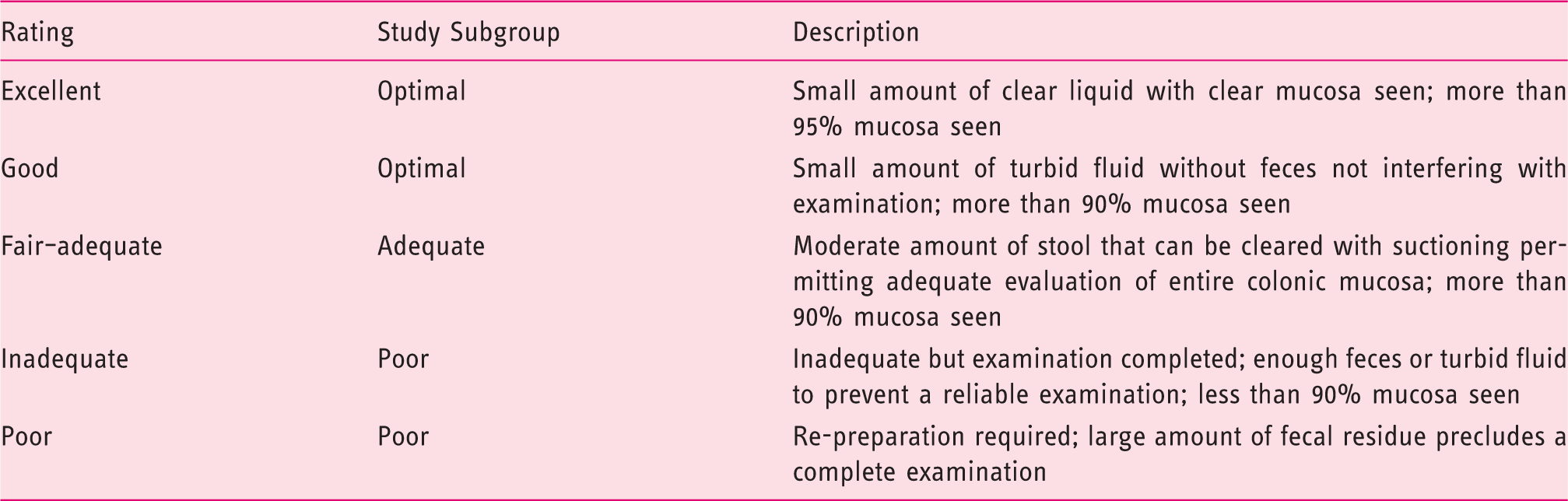
Subgroup subdivision according to the Modified Aronchick scale 14 classification.
Definition of study variables: ADR, mADR, zADR, mzADR, PDR, mPDR, zPDR and mzPDR
ADR, defined as the number of colonoscopies in which one or more adenomas was detected, divided by the total number of colonoscopies performed and PDR, defined as the number of colonoscopies in which one or more polyps was detected, divided by the total number of colonoscopies performed, were calculated. 11
In order to bypass some spatial limitations of ADR, we aimed to test new parameters, namely: the multiple Adenoma Detection Rate (mADR), the zonal Adenoma Detection Rate (zADR) and multi-zone Adenoma Detection Rate (mzADR), developed in order to maximize segmental evaluation during endoscopy. In detail, mADR was defined as the percentage of patients with ≥2 adenomas diagnosed during colonoscopy, the zADR as the percentage of patients with ≥2 adenomas diagnosed during colonoscopy in different colon areas (rectum, sigmoid, descending, transverse, ascending and cecum colon), and the mzADR as the percentage of patients with ≥2 adenomas diagnosed during colonoscopy in different colon areas with at least a segment between them with or without lesions (i.e. rectum and descending colon with or without lesions in the sigmoid). The corresponding values were also assessed for polyps, namely mPDR, zPDR, mzPDR.
In our study, we also assessed the correlation among the proposed new parameters and the modified Aronchick scale. For this purpose, the study group was divided into three subgroups, according to the quality of BP, namely optimal (Aronchick 1–2), adequate (Aronchick 3), and poor preparation (Aronchick 4–5).
Statistical analysis
The statistical analysis of the results was performed with SPSS version 20.0. The chi-square test and Student t-test were used as appropriate. Values of p < 0.05 were considered statistically significant.
Results
Study population
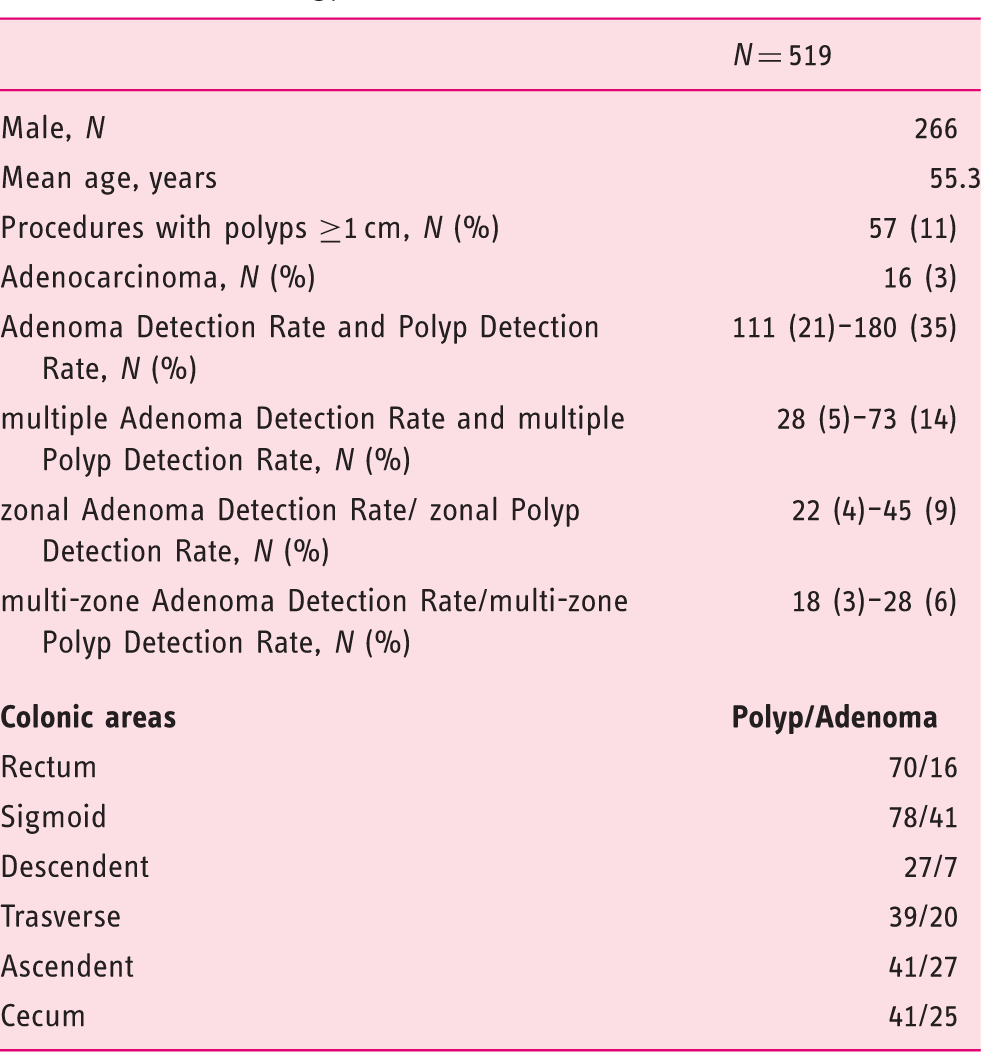
During the study period, 519 patients (226/253 M/F; median age = 55.3 + 12.8; range = 23–86) were enrolled. In a per patient analysis, the adenoma and polyp detection rates were 21% (111/519) and 35% (180/519), respectively. In a per polyp analysis, the overall mean of adenomas and polyps detected per patient were 1.38/patient and 1.61/patients. Regarding localization, 175/296 (59%) and 64/136 (47%) polyps and adenomas were in the distal colon, respectively, while 121/296 and 72/136 were in the proximal colon. Regarding size, 135/296 (46%) polyps and 99/136 (73%) adenomas were equal or superior 6 mm. Adenocarcinomas (ADK) were diagnosed in 16 patients, also in association with hyperplastic polypoid (37%) and adenomatous (19%) lesions (Table 2).
New study variables
In a per-patient analysis, multiple adenomas were detected in 28 patients, corresponding to a 5% mADR rate. The corresponding value for polyps (i.e. mPDR) was 14% (73/519). Adenomas in different segments (i.e. at least two different segments) were detected in 22 patients, corresponding to a 4% zADR rate. The corresponding value for polyps (i.e. zPDR) was 9% (45/519). Adenomas in different discrete segments were detected in 18 patients, corresponding to a 3% mzADR rate. The corresponding value for polyps (i.e. mzPDR) was 6% (28/519) (Table 2).
Distribution of the study variables according to the quality of preparation
The number of diagnosed colic lesions, their location, diameter and histology.
Statistical analysis for data acquired in the study group divided according to the different bowel preparation degrees.
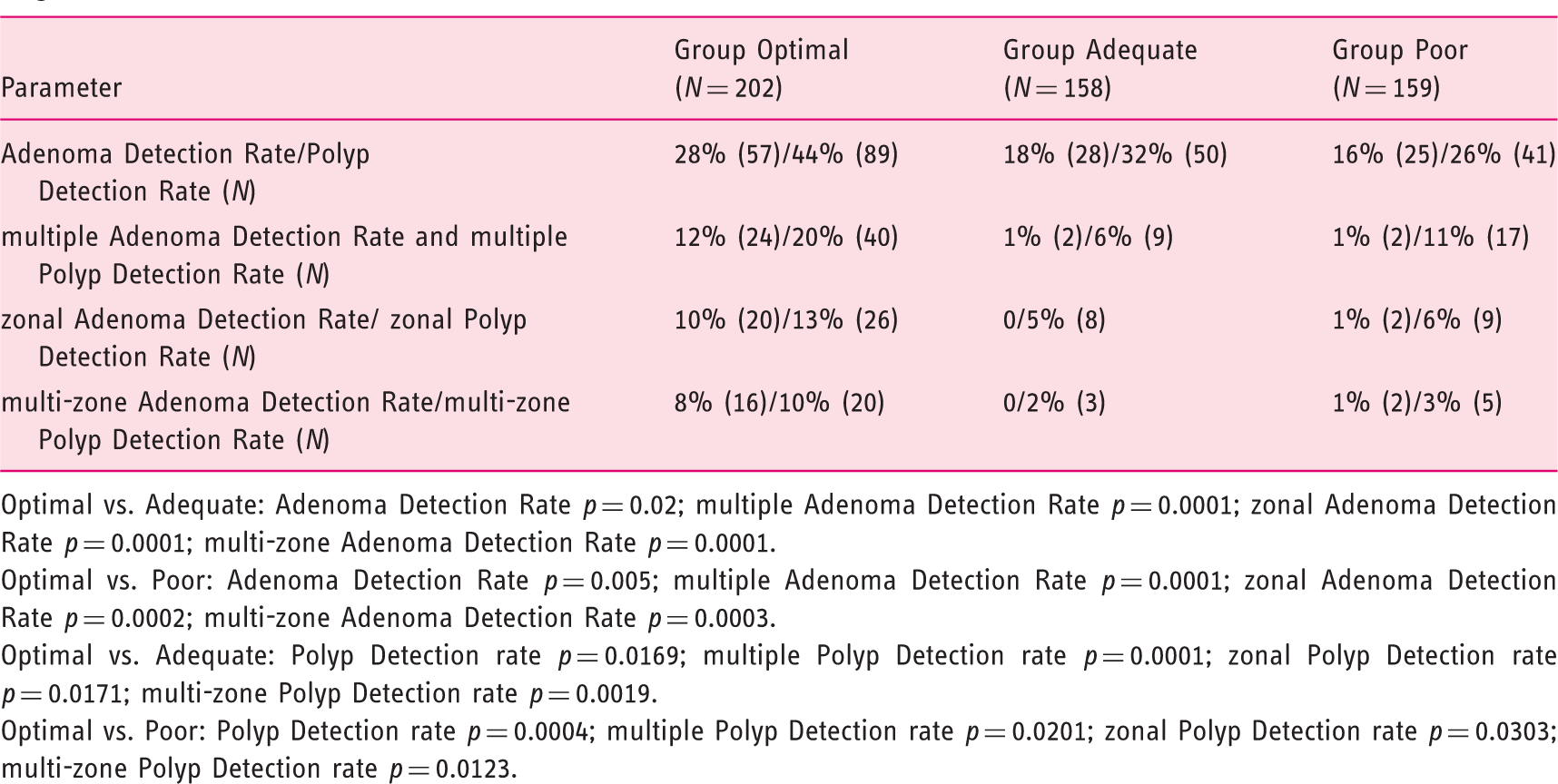
Optimal vs. Adequate: Adenoma Detection Rate p = 0.02; multiple Adenoma Detection Rate p = 0.0001; zonal Adenoma Detection Rate p = 0.0001; multi-zone Adenoma Detection Rate p = 0.0001.
Optimal vs. Poor: Adenoma Detection Rate p = 0.005; multiple Adenoma Detection Rate p = 0.0001; zonal Adenoma Detection Rate p = 0.0002; multi-zone Adenoma Detection Rate p = 0.0003.
Optimal vs. Adequate: Polyp Detection rate p = 0.0169; multiple Polyp Detection rate p = 0.0001; zonal Polyp Detection rate p = 0.0171; multi-zone Polyp Detection rate p = 0.0019.
Optimal vs. Poor: Polyp Detection rate p = 0.0004; multiple Polyp Detection rate p = 0.0201; zonal Polyp Detection rate p = 0.0303; multi-zone Polyp Detection rate p = 0.0123.
Discussion
ADR represents the most reliable tool to evaluate the impact of BP on polyp detection. In a recent study, Chokshi et al. 16 reviewed all the colonoscopies performed between 2004 and 2009 in their diagnostic centre, in which BP was judged poor, inadequate or unsatisfactory, according to the Aronchick scale. Among a series of 373 patients, 91 missed lesions were found, reaching an adenoma miss rate of 47.9%. The initial ADR was 25.7% (32% in men and 21.1% in women); among the 373 initial patients, 133 underwent a second colonoscopy, and in 33.8% of these patients at least one adenoma missed at previous colonoscopy was detected, reaching an ADR of 42.9% in men and 27.1% in women. A colonoscopy performed with an optimal BP allowed the detection of missed lesions, increasing ADR both in men and in women.
However, there is uncertainty on whether a suboptimal BP reduces only the per patient detection rate of adenomas/polyps or also the identification of patients with multiple lesions in the same or different segments of the colon.
Although a retrospective study and meta-analysis17,18 suggest that the ADR in colonoscopies with an intermediate-quality BP does not differ to ADR in those with a high-quality preparation, no interobserver or intraobserver agreement studies have been conducted on the evaluation of BP. In fact, even supporters of the Boston Bowel Preparation Scale (BBPS) 19 developed an educational programme to improve the classification variability. 20 For these reasons, a point of debate regarding the evaluation of intermediate levels of BP should be deepened. Our study differs from the previous ones by defining a diagnostic advantage especially in the presence of excellent or good levels of BP (Aronchick 1 and 2).
Moreover, the primary aim of this study was to propose new parameters to assess the impact of BP on the detection of colorectal lesions, improving and complementing ADR/PDR, by assuming a possible difference in the effect of bowel preparation according to the various colonic segments. According to the study data, the parameters related to number and location of detected polyps during colonoscopy changed considerably according to the level of BP. In particular, we showed that an optimal level of BP was not only associated with a higher ADR/PDR, but also with a higher chance to diagnose multiple lesions in the same area (mADR/PDR) or in different segments (mzADR/PDR). On the other hand, no main differences in any of the study variables, including ADR/PDR, were detected between the discrete and poor BP groups. The results of our study are relevant for several reasons. First, we showed that a suboptimal BP is likely to be associated not only with a reduced rate of identification of patients with at least one adenoma, but also with a suboptimal characterization of all the lesions in those patients who have at least one lesion. This would indicate that even those patients with a positive diagnosis would still remain at a lower degree of CRC protection, as compared with the corresponding patients with an optimal degree of BP. Second, our findings may indirectly justify the anticipation of post-polypectomy surveillance in patients with inadequate BP. Indeed, endoscopists were already aware of the higher risk of missing multiple adenomas in those presenting with at least one adenoma and incomplete BP. Third, the strong association between an optimal degree of BP and higher detection rates was not found for an adequate degree of BP, according to the adopted BP scale. This could suggest that an optimal rather than a simply adequate level should be the target of the optimization of BP. Fourth, the ADR assessment needs both endoscopic and histological diagnoses, and this represents a drawback to the routine by use of this parameter.21–24 A study performed by Bernard et al. in 2010 22 underlined how PDR could effectively replace ADR in the evaluation of the effectiveness of colonoscopy in clinical practice, and showed how these two quality indicators are well correlated to each other, with 37 expert endoscopists performing 6631 colonoscopies within a colorectal screening programme. However, this correlation is less evident at the level of the distal colon, where hyperplastic polyps (HP) cause an overestimation of PDR vs. ADR. In our study, 78% of HP were found in distal colon, but their “weight” was minimized in zPDR and mzPDR.
There are limitations to the present analysis. We did not use a split regimen of BP, since all the colonoscopies were scheduled in the early morning period, justifying the relatively high rate of inadequate BP in our series. However, the split regimen is likely to affect the relative rate of adequate preparation, rather than the association between each degree of BP and the detection rate. Secondly, our study is monocentric, so that larger studies are needed to further confirm the validity of the study variables. Finally, a more accurate assessment of BP may be obtained by BBPS. However, this method, while adding a segmental evaluation, requires an equal ability to complete washing and suction manoeuvres during colonoscopy. Thus, we preferred not to add this additional element of subjectivity in the evaluation of BP.
An optimal level of BP was strongly associated not only with a higher ADR, but also with a higher chance of detecting multiple clinically relevant lesions in adjacent or discrete segments of the colon.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.