
Abstract
Background
Hepatocellular carcinoma is one of the most lethal cancers worldwide. Novel prognostic and/or predictive biomarkers are urgently needed to improve patient management. Alpha-fetoprotein is a well-established and widely used biomarker for hepatocellular carcinoma. However, diagnostic accuracy of static alpha-fetoprotein values is limited and the clinical potential is a matter of ongoing scientific discussion.
Objective
We here evaluated the prognostic impact of pre-treatment static and dynamic alpha-fetoprotein variables on overall survival of hepatocellular carcinoma patients in a Western cohort.
Methods
Patients with confirmed hepatocellular carcinoma (n = 809) treated at the Johannes Gutenberg-University Mainz between 1998 and 2014 and two available pre-treatment alpha-fetoprotein-values (AFP-slope) were retrospectively analysed. Clinico-pathological baseline parameters, pre-treatment static values and AFP-slope were assessed. Prognostic impact was determined by Kaplan–Meier analyses and Cox regression models.
Results
High static and dynamic alpha-fetoprotein variables prior to therapy were associated with reduced survival rates of hepatocellular carcinoma patients. Several known clinical parameters such as Child–Pugh B (p < 0.01) and C stage (p < 0.001), portal vein thrombosis (p < 0.001) and extrahepatic spread (p < 0.001) were confirmed as independent predictors for overall survival. Addition of static and/or dynamic alpha-fetoprotein variable resulted in higher time-dependent area under the curves. Notably, in patients with more favourable prognosis, AFP-slope prior to therapy was a slightly stronger predictor for overall survival compared with static alpha-fetoprotein values.
Conclusion
Static and dynamic alpha-fetoprotein variables prior to therapy are predictive for overall survival of hepatocellular carcinoma patients. Addition of AFP-slope to established prognostic parameters might improve prognostic classification for a subgroup of hepatocellular carcinoma patients with preserved liver function and without portal vein tumour thrombosis.
Key summary
Alpha-fetoprotein (AFP) is the most commonly used biomarker for hepatocellular carcinomas (HCCs), but accuracy of static and dynamic AFP values is limited and the prognostic significance is under debate. High static and dynamic AFP variables prior to therapy are associated with reduced survival rates of HCC patients across different tumour stages and treatment modalities. In patients with more favourable prognosis, AFP-slope prior to therapy was a better predictor for OS in comparison with static AFP values. Addition of AFP-slope to established prognostic parameters might improve prognostic classification for a subgroup of HCC.
Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver cancer and leading cause of death in cirrhotic patients. 1 HCC is the sixth most common cancer worldwide and shows a rising incidence in the Western world. Between 2005 and 2015 HCCs were the second leading cause of cancer related years of life lost. 2 The majority of HCCs develop on the background of chronic liver injury and, most commonly, liver cirrhosis. Predisposing risk factors include chronic viral hepatitis, alcohol abuse and metabolic disorders. 3 Due to an impaired liver function and late diagnosis, only a minority of patients is amenable to curative treatment such as resection, orthotopic liver transplantation (OLT) or local ablation. More than two-thirds of HCC patients are diagnosed in intermediate and advanced stages of disease, when therapeutic options are limited to loco-regional and systemic therapies.4–6 Despite new approaches in interventional and systemic treatment modalities, prognosis of HCC remains decidedly poor and novel biomarkers for accurate prediction of prognosis as well as selection of optimal treatment strategies are urgently needed to improve patient management. 4 Alpha-fetoprotein (AFP) is the most widely used and validated biomarker for HCCs since the 1970s. Routine clinical use of AFP in HCC diagnosis and surveillance has been under extensive debate over recent years due to a low sensitivity and specificity, especially in detecting small HCCs. 7 , 8 However, due to improved imaging modalities for HCC diagnosis, routine AFP measurements in HCC surveillance are no longer endorsed by HCC guidelines of the American Association for the Study of Liver Diseases (AASLD) 5 and the European Association for the study of the Liver (EASL). 4
However, despite the low accuracy in a diagnostic setting, the value of AFP in prediction of overall survival (OS) has been repeatedly demonstrated and measurement is still implemented in most established prognostic staging algorithms. 5 , 9 Especially with respect to patient allocation for liver transplantation, AFP seems to possess considerable predictive value. 10 Interestingly, several recent studies further delineate a strong impact on both recurrence rates and OS when AFP dynamics rather than static values are assessed prior to liver transplantation.11–15 Unlike single AFP values, AFP trends and changes might better reflect the biological traits of tumours. However, clinical potential of these dynamic AFP-slopes as prognostic and/or predictive markers needs to be more precisely defined. We here evaluated the prognostic role of pre-treatment serum static as well as dynamic AFP variables on OS of 809 patients with HCC in a German cohort and investigated their predictive significance across different treatment modalities including OLT, HCC resection, transarterial chemoembolization (TACE) and systemic therapy.
Materials and methods
Demographics
Patients diagnosed with HCC at the University Medical Centre of the Johannes Gutenberg-University Mainz between 1998 and 2014 were included in this retrospective analysis (Mainz cohort). HCC diagnosis was based on histological or radiologic findings according to AASLD/EASL criteria. 4 , 5 , 16 End of follow-up was 30 June 2017. A total of 1706 patients were identified from our HCC registry. Exclusion criteria were: i) less than two AFP values or ii) an interval between two AFP measurements of less than seven days or more than 365 days, iii) patients with mixed hepato/-cholangio cellular carcinom as (HCC/CCC) (Figure 1). Fifty patients were censored due to loss to follow-up. Baseline parameters concerning patient status (sex, age, performance status), tumour characteristics (tumour size, tumour number, extrahepatic spread, Barcelona Clinic Liver Cancer (BCLC) stage), Child–Pugh score, aetiology of underlying liver disease, presence of portal vein thrombosis, as well as static pre-treatment AFP values and AFP dynamics within one year of the remaining 809 patients were collected from a prospectively maintained database of our clinical registry unit. 17 The study was approved by the responsible ethics committee for the retrospective analysis of clinical data.
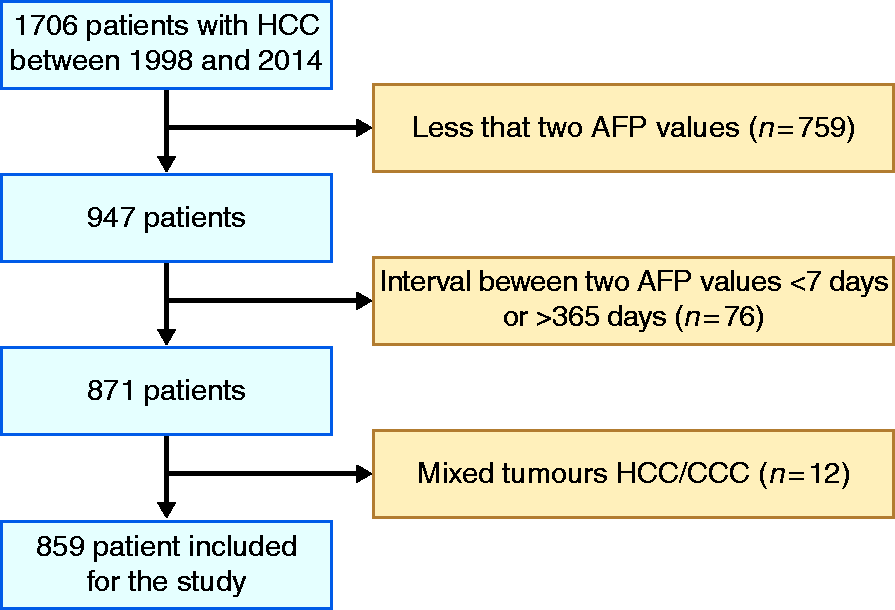
Flow chart of the study.
Tumour characteristics
All patients were classified according to the BCLC classification. 18 Eastern Co-operative Oncology Group performance status and treatment was retrieved from medical records or records from the clinical registry. Tumour size, extrahepatic spread and presence of portal vein thrombosis was documented based on resected specimen or radiological assessment as applicable.
AFP cut-offs and -slope calculation
Laboratory results, including AFP values prior to therapy, were collected from the hospital information system and patient records. Positive AFP values were defined above a cut-off of 8.8 ng/ml. For Cox regression analyses an AFP cut-off over 400 ng/ml was chosen, since this is the most widely used cut-off in existing staging systems. 9 , 19 , 20 Absolute AFP-slope was defined as the difference of two consecutive pre-treatment measurements divided by the time between measurements, thus obtaining daily increment/decline: AFP-slope (ng/ml per day) = (AFP2 – AFP1)/T (time in days between the two AFP measurements).
Statistical analyses
Statistical analyses were conducted with R (The R Project for Statistical Computing, version 3.4.2, Vienna, Austria, www.r-project.org) and SAS 9.4. Univariate and multivariate Cox regression analyses were performed to identify prognostic factors for OS of HCC patients using PROC PHREG from SAS. Survival curves were generated using the Kaplan–Meier method and compared using the log-rank test using Prism Graph Pad. p-values < 0.01 were considered statistically significant.
Results
Study population and pre-treatment AFP levels and dynamics
A total of 809 patients were included in the study after applying the above-mentioned inclusion criteria. Median time of follow-up was 453 (interquartile range 1269) days. Baseline characteristics of patients are presented in Table 1. Patients of the study cohort were mainly men, with a median age of 65 years (range 16–90). The majority of patients (88.4%) presented with liver cirrhosis in Child–Pugh stages A (40%), B (34.5%) and C (13.8). Main aetiology of underlying liver disease was alcohol abuse (39.2%) followed by hepatitis C (24.7%) and hepatitis B infection (12.2%). BCLC stages were represented as 34.9% classified as stage BCLC-A, 22.2% BCLC-B, 28.6% BCLC-C and 14.3% BCLC-D. The majority of patients (94.2%) presented in a good performance status (0–1). A portal vein tumour thrombosis has been found in 20.6% of patients and extrahepatic spread in 8.0%. Predictive impact of static and dynamic AFP variables has been studied across several treatment approaches. Curative therapies included OLT (4.2%), ablation (3.2%) and resection (12.9%) of HCCs. Most patients were treated with TACE (58.7%). Patients with advanced stages of disease received systemic therapy (8.0%) or best supportive care (10.2%). Static AFP values were measured at two different time points, that is, AFP1 and AFP2 prior to therapy. For 717 patients (88.6%) the two values were measured within 7–90 days, for 61 patients (7.5%) within 91–180 days and for 31 patients (3.8%) within 181–365 days (Table 1; Supplemental Material Figure 1(a) online). While AFP1 was collected either during HCC-surveillance or during diagnostic clarification for HCC, AFP2 was collected mainly during diagnostic work-up for HCC (Supplemental Figure 1(b) and (c)). Intervals between each measurement and start of therapy were similar across different treatment modalities (Table 1). Median AFP level at baseline (AFP1) within the study population was 26 ng/ml spanning a wide range from 1 to 411.417 ng/ml as shown in Table 1. Two hundred and forty-seven patients (30.5%) initially presented with AFP values below the internal laboratory thresholds of 8.8 ng/ml. Values below 8.8 are considered negative according to our internal laboratory standard. From the 562 (69.5%) patients with positive AFP values 224 (27.7%) had high AFP values (>400 ng/ml). At the second time point 223 (28.8%) of patients were negative for AFP. Two hundred and fifty-three (31.3%) positive patients had a high AFP value (>400 ng/ml). Dynamic AFP variables are expressed as an AFP-slope calculated by changes of AFP values in ng/ml per day. Median AFP-slope of the study cohort was 0.051 ng/ml per day.
Patient and tumour characteristics.
BCLC: Barcelona Clinic Liver Cancer; ECOG PST: Eastern Co-operative Oncology Group performance status; HBV: hepatitis B virus; HCV: hepatitis C virus; NASH; non-alcoholic steatohepatitis; TACE: transarterial chemoembolization; BSC: best supportive care; AFP: alpha-fetoprotein; OLT: orthotopic liver transplantation.
High static and dynamic AFP variables are associated with poor OS of HCC patients
To describe association of AFP variables with OS of HCC patients uni- and multivariate Cox regression analyses were performed including clinical parameters, such as patient performance status, tumour size, aetiology of underlying liver disease and liver function by Child–Pugh scoring, portal vein tumor thrombosis (PVTT) and extrahepatic spread. Static AFP cut-off was defined at 400 ng/ml.
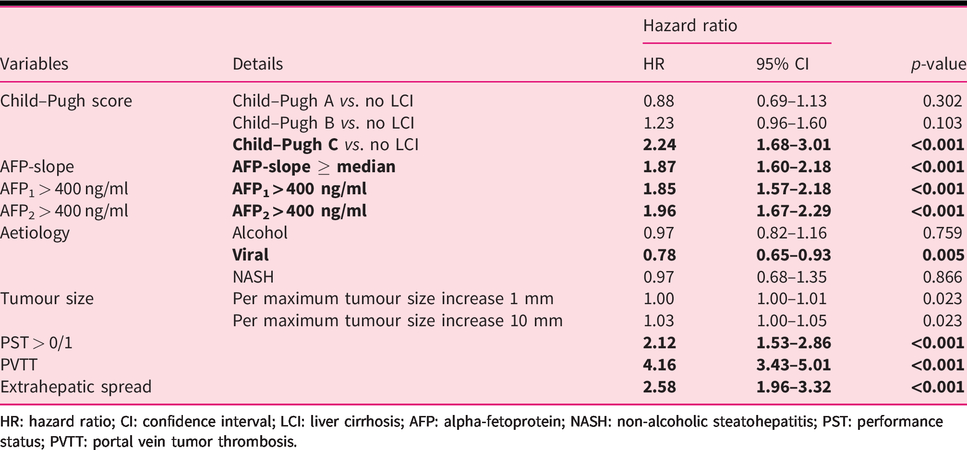
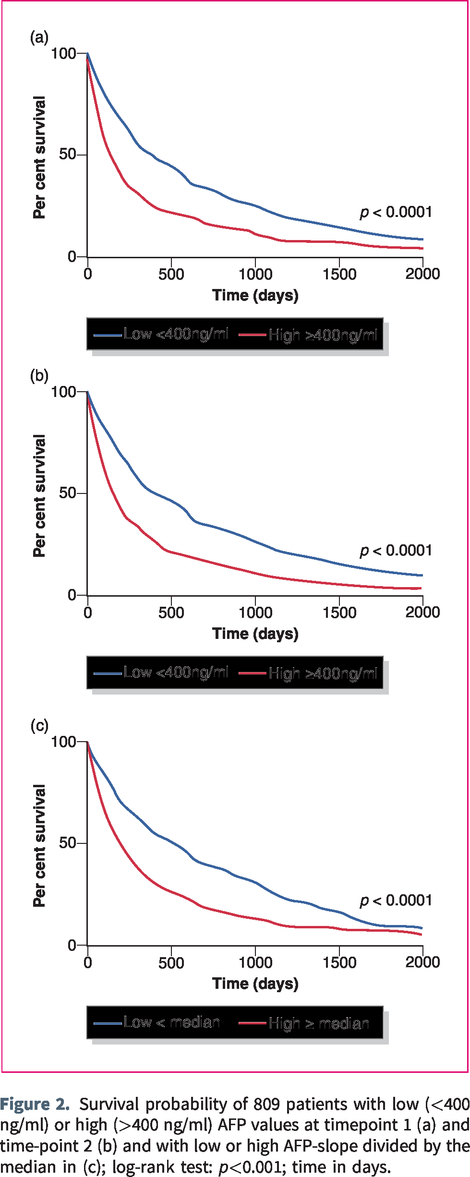
While viral hepatitis was a favourable factor in univariate Cox regression analyses (hazard ratio (HR) 0.78; 95% confidence interval (CI) 0.65–0.93), other known prognostic factors such as a Child–Pugh C liver cirrhosis (HR 2.24; 95% CI 1.68–3.01), a worse performance status >0/1 (HR 2.12; 95% CI 1.53–2.86) as well as extrahepatic spread (HR 2.58; 95% CI 1.96–3.32) and a PVTT (HR 4.16; 95% CI 3.43–5.01) were associated with poor OS for HCC patients. Pre-treatment static AFP values > 400 ng/ml were further highly significantly associated with OS in univariate analyses (AFP1: HR 1.85; 95% CI 1.57–2.18; AFP2: HR 1.95; 95% CI 1.67–2.29) and resulted in significantly reduced survival rates (Table 2 and Figure 2(a) and (b)). Similarly, pre-treatment AFP-slopes dichotomized at median were significantly associated with OS, when AFP2 exceed 20 ng/ml (Table 2 and Supplemental Figure 1). For further analyses the AFP-slope was divided into high and low based on the median (0.051 ng/ml per day) across the cohort. A high AFP-slope was strongly associated with OS (HR 1.87; 95% CI 1.60–2.18) and resulted in significantly reduced survival rates for HCC patients (Table 2 and Figure 2(c)). Time-dependent area under the curves (AUC) for pre-treatment static and dynamic AFP variables of univariate analyses decreased with longer prediction periods; however, AUC of pre-treatment AFP-slope was slightly higher compared with static AFP values (Figure 3 and Supplemental Table 1).
Univariate analyses of prognostic factors for overall survival of hepatocellular carcinoma patients.
HR: hazard ratio; CI: confidence interval; LCI: liver cirrhosis; AFP: alpha-fetoprotein; NASH: non-alcoholic steatohepatitis; PST: performance status; PVTT: portal vein tumor thrombosis.
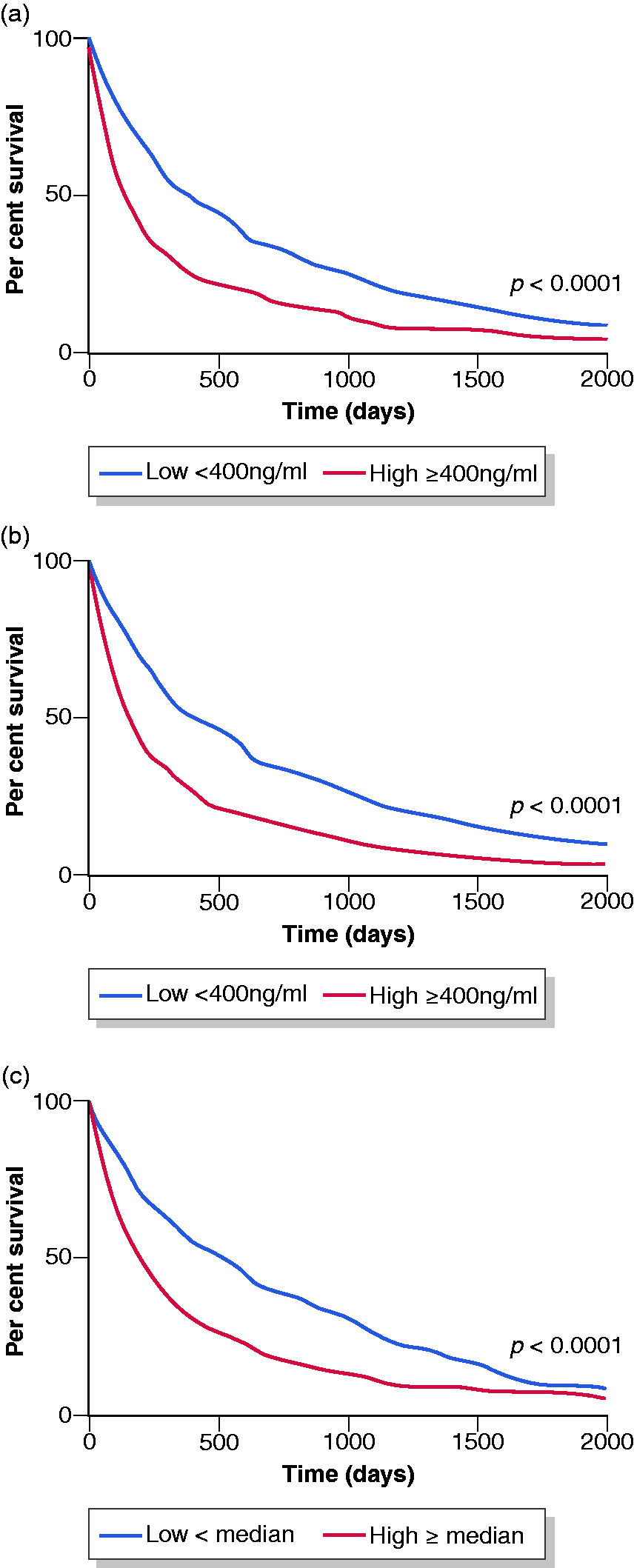
Survival probability of 809 patients with low (<400 ng/ml) or high (>400 ng/ml) AFP values at timepoint 1 (a) and time-point 2 (b) and with low or high AFP-slope divided by the median in (c); log-rank test: p<0.001; time in days.
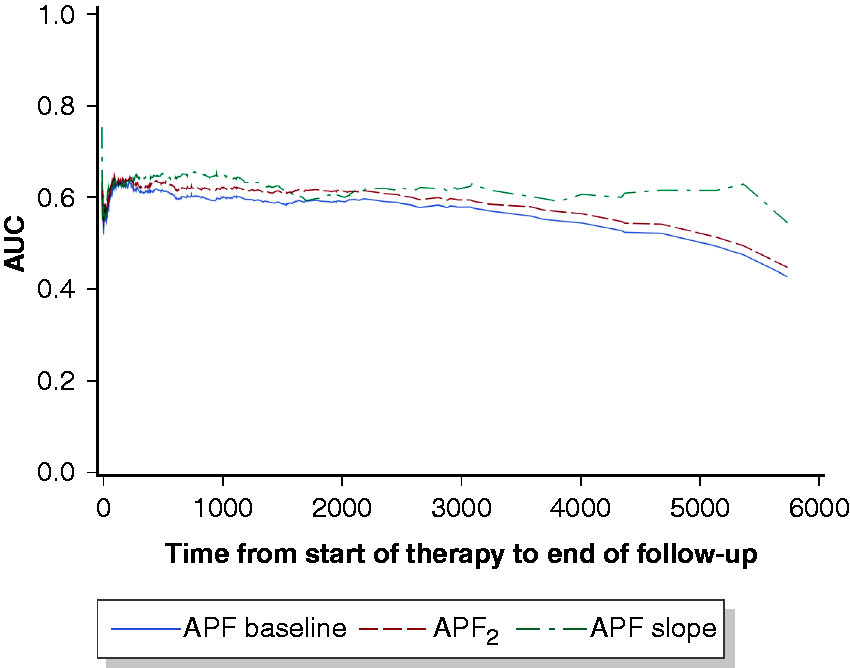
Time-dependent area under the curve for pre-treatment static AFP values of univariate analyses.
AFP-slope improves prediction for subgroup of HCC-patients with preserved liver function and without PVTT
In order to determine whether high static and/or dynamic AFP variables prior to therapy are independent predictors for OS of HCC patients, multivariate analyses were performed including (i) a full model with all parameters as well as models, (ii) without any AFP variable and (iii) with only AFP1, AFP2 or the AFP-slope (Supplemental Tables 2(a) and (b) and 3(a) to (e)).
First we investigated the whole study cohort (N=809). Several well-known clinical parameters such as the Child–Pugh score B (HR 1.49; CI 1.13–2.00, p < 0.01) and C (HR 2.71; CI 1.87–3.97, p < 0.001), portal vein tumour thrombosis (HR 3.67; CI 2.96–4.52, p < 0.001) and extrahepatic spread (HR 1.87; CI 1.39–2.42, p < 0.001) could be confirmed as strong independent factors for OS of patients with HCC in multivariate analyses (Supplemental Table 3(a)). Adding pre-treatment static and/or dynamic AFP variables to the models resulted in higher time-dependent AUCs and higher values for Harrell’s concordance index (HC), indicating an improved predictive ability for OS (Figure 4 and Supplemental Table 2(a) and (b)). However, difference between static and dynamic AFP variables were not remarkable (Supplementary Table 2 (A) and (B): HCAFP1 0.694 ± 0.009; HCAFP2 0.697 ± 0.009; HCAFP-slope 0.702 ± 0.009).
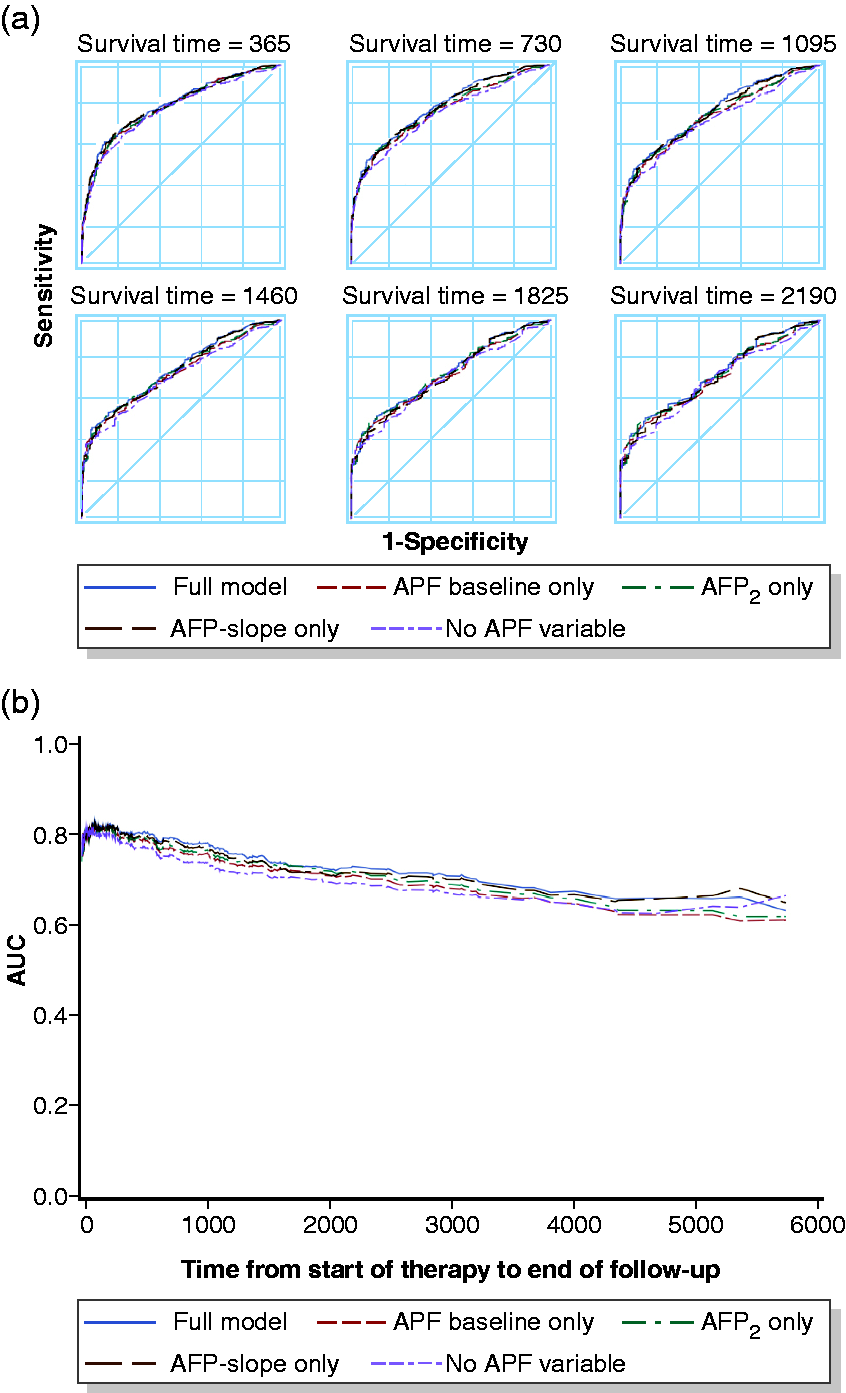
Receiver operating curve (a) and time-dependent area under the curve (b) for analysed models of multivariate analyses including all patients (N = 809).
We next excluded strong independent predictors such Child–Pugh C liver cirrhosis and PVTT in order to analyse patients with more favourable prognoses (n = 569), that is, patients with preserved liver function and without PVTT (Supplemental Table 4(a) and (b) and 5(a) to (e)). In this subgroup of patients, we observed slightly higher time-dependent AUCs for the model including AFP-slope in comparison with models including only static AFP values (Supplemental Table 4(a) and (b); HCAFP1 0.617 ± 0.014; HCAFP2 HC 0.621 ± 0.014; HCAFP-slope HC 0.631 ± 0.014). Therefore, in selected patients an AFP-slope prior to therapy is a stronger predictor for OS compared with static AFP values (Figure 5(a) and (b)).
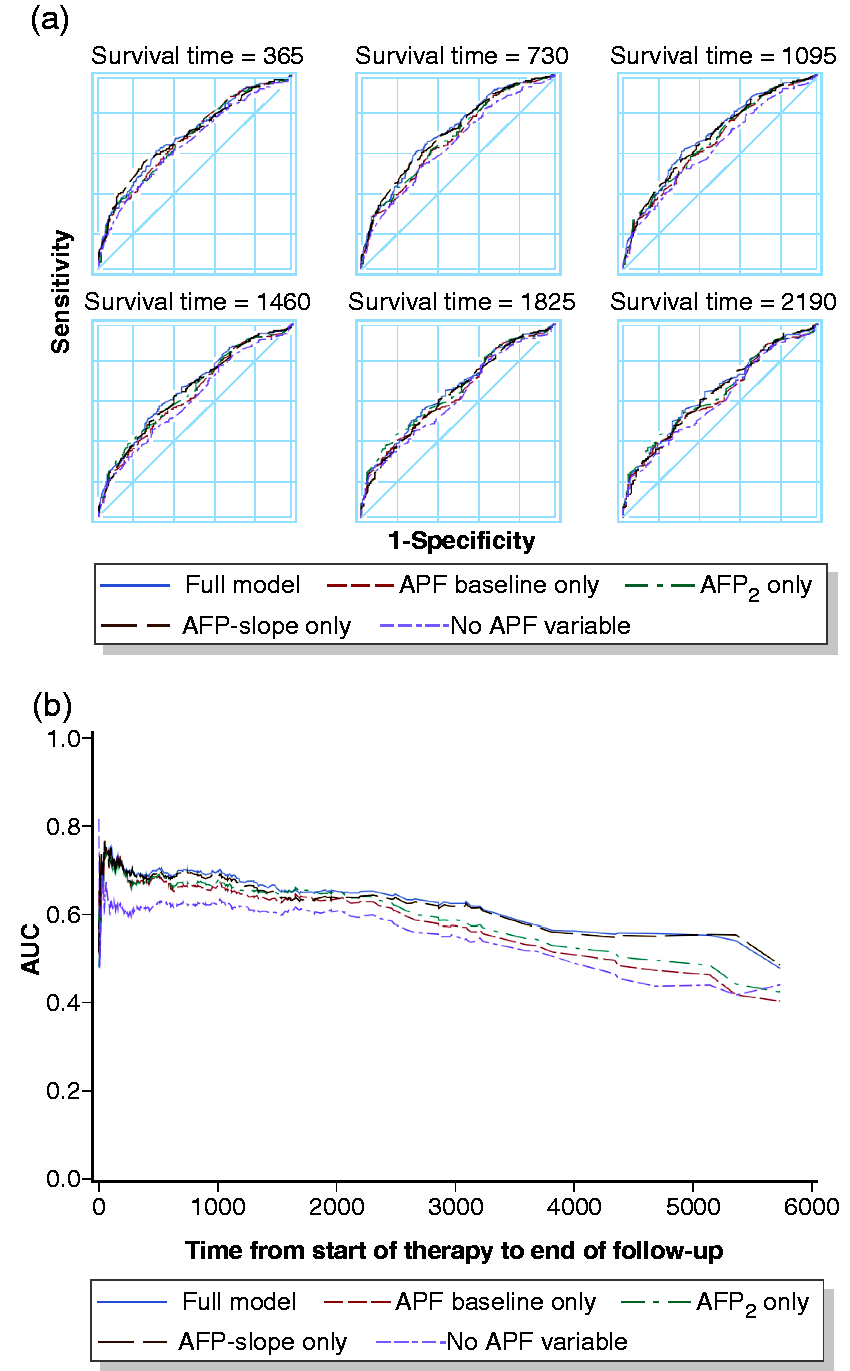
Receiver operating curve (a) and time-dependent area under the curve (b) for analysed models of multivariate analyses including patients with preserved liver function and without portal vein tumor thrombosis (n = 569).
Discussion
In the presented study, we evaluated the predictive value of static and dynamic AFP variables prior to therapy. We demonstrate that across all commonly used treatment modalities covering the full range of BCLC stages, high pre-treatment AFP variables are associated with worse clinical outcome for HCC patients. Notably, integration of AFP-slopes rather than static AFP values in multivariate models are reliable predictors for OS of a subgroup of patients with HCC without PVTT and with preserved liver function.
AFP is a well-established and widely used biomarker for HCC. 21 However, its use in clinical practice for HCC diagnosis and surveillance is still a matter of ongoing discussion due to limited accuracy of static AFP values. 8 , 22 Universal agreements of AFP cut-off values do not exist and the use of AFP is currently not recommended by major clinical associations for surveillance or for treatment stratification. 4 , 5 , 16 , 23
However, over recent years the use of AFP as a predictor for prognosis, recurrence and survival with respect to OLT gained increasing attention. 10 Due to the shortage of liver donors, strong selection criteria are required to stratify patients before OLT. Until now only tumour size and number according to Milan Criteria are used as a selection tool for OLT in most Western countries. 24 However, these criteria inaccurately predict the tumour biology and aggressiveness 25 , 26 and a combination with additional factors might be superior in selecting the most suitable patients. Therefore, identification of novel, non-invasive and reproducible serum biomarkers is highly desirable. 16 Recent studies that focused on AFP demonstrated a shorter OS after OLT for patients with high pre-operative AFP values. However, a wide range from 8.5 ng/ml to 1000 ng/ml has been observed to be associated with OS or recurrence rate and a common threshold has not been established yet.27–31
We here evaluated the prognostic impact of pre-treatment static and dynamic AFP variables across several treatment modalities and disease stages and demonstrate that indeed high static AFP values as well as a dynamic AFP-slope prior to therapy have prognostic value in uni- and multivariate analyses. Patients with high AFP values over 400 ng/ml as well as with high pre-treatment AFP-slopes (>median) had significantly reduced survival rates compared with patients below the cut-offs (Figure 2). We further confirmed the significance of other well-known clinical parameters such as Child–Pugh scoring, PVTT and extrahepatic tumour spread for OS of patients with HCC.
Previously studies mainly on dynamic AFP variables focused only on OLT. Lai et al. recently demonstrated that an AFP-slope greater than 15 ng/ml per month and radiological progression according to mRECIST were unique independent risk factors for HCC recurrence and death after OLT. 14 Survival rates of patients outside the Milan Criteria without risk factors showed similar outcome compared with patients inside the MC without risk factors and were even significantly superior to patients inside the MC with risk factors. The authors conclude that integration of dynamic biological and morphological tumour characteristics into classic HCC staging tools could be more effective to accurately select patients for OLT. 14 Furthermore, Vibert et al. also showed that an AFP progression (>15 ng/ml per month) was more relevant than a static AFP value in predicting OLT outcomes in a cohort of 153 HCC patients. 12 A Canadian study (N=144) confirmed that a rising AFP-slope (>0.1 ng/ml per day) was a faithful and independent predictor of microvascular invasion and HCC recurrence after OLT. 13 Our results are in agreement with the aforementioned studies. We confirmed that an AFP-slope is associated with OS of HCC patients before major therapeutic approaches including OLT, HCC-resection, TACE and sorafenib therapy, that is, across all BCLC stages. To address clinical relevance of static as well as dynamic AFP values, we performed several multivariate models and showed that, if a strong negative predictor such as a Child–Pugh C cirrhosis or a PVTT is present, incorporation of AFP values does only slightly improve the AUC over time (Figure 4 and Supplemental Tables 2 and 3). In this context, AFP-slopes were not superior to static AFP values for patients harbouring a poor clinical outcome. We next investigated a subgroup of patients with more favourable prognosis, that is, preserved liver function without PVTT (Figure 5 and Supplemental Tables 4 and 5). In these selected patients inclusion of AFP-slopes in multivariate models reached higher time-dependent AUCs compared with inclusion of static AFP values in multivariate analyses (Figure 5 and Supplemental Tables 4 and 5). These findings emphasize that a significant AFP progression prior to therapy is a valid marker for an aggressive tumour biology and worse outcome for selected HCC patients. Therefore, dynamic AFP-slope measurements might reflect more faithfully than static AFP values the natural cause of the disease in patients with more favourable prognoses. Notably, consistent with previous studies, the predictive ability of static or dynamic AFP variables alone is limited (AUCs ranging from 0.59 to 0.64). Similar data has been obtained in recent publications with AUCs ranging from 0.557 to 0.727, sensitivities and specificities of 30.8–63% and 58–92.3%, respectively.11–14
Therefore further refinement and combination with other markers seem necessary. But AFP-slopes might be a helpful addition to other established staging tools. The BALAD-score, a new staging system, which is exclusively based on serum markers (bilirubin, albumin, AFP-L3, AFP and des-γ-carboxyprothrombin (DCP)) has recently been introduced. 9 , 20 The score is, therefore, not only highly reproducible and non-invasive, but also objective. Overall, the BALAD-score showed good discriminative ability across different populations of HCC patients. 32 , 33 Nevertheless, our findings as well as aforementioned studies strengthen that changes of biomarkers instead of static values might possess superior classification abilities for selected patient subgroups and should be considered as an integrative classification and/or selection tool to refine existing staging systems.
Of note, the retrospective, single centre design of our study as well as limited numbers of patients in some subgroups are important limitations. Prospective studies performed on independent cohorts are needed to validate AFP-slopes prior to therapy as an improved selection and classification tool for the patient’s prognosis and treatment selection. Implementation of least-squares-based slopes including sequential AFP measurements over time could further refine AFP-slopes and reduce noise of random fluctuations.
In conclusion, we showed that high static AFP values as well as high AFP-slopes prior to therapy are strongly associated with poor prognosis of HCC patients across different treatment modalities and BCLC stages. Importantly, for patients with preserved liver function and without PVTT, a pre-treatment AFP-slope improved prediction for patients’ survival in comparison with static AFP values. Therefore, integration of AFP dynamics might be a promising approach to improve prognostic scoring systems for HCC subgroups and help to refine patient selection for most suitable therapies. Prospective evaluation and validation in independent patient cohorts of the concept and of the ideal interval of the sequential AFP tests without interfering with a timely start of therapy seems warranted.
Footnotes
Acknowledgements
JUM is supported by the Volkswagen Foundation (Lichtenberg Programm). CC is supported by a TransMed Fellowship of the University of Mainz. Aspects of this article are part of the doctoral thesis of LP. Author contribution: collection of data: CC, SK, LP, SH, GO, JM, HL, RK, CD, MFS, MAW, PRG, JUM, AW. Analysed the data: CC, IS, SK, LP, AW, JUM. Wrote the paper: CC, IS, JUM, A.W. All authors discussed the results and critically commented on the manuscript. All authors had access to the study data and reviewed and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The study was approved by the responsible ethics committee for the retrospective analysis of clinical data.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by internal funding of the 1. Department of Medicine, University Medical Centre, University of Mainz, Germany.
Informed consent
No informed consent was requested. The study design was retrospective and all data were anonymized.
Supplemental material
Supplemental material for this article is available online.