
Abstract
Background
People with cystic fibrosis (CF) report a variety of gastrointestinal (GI) symptoms, independent of pancreatic enzyme insufficiency (PEI), reminiscent of other chronic GI disorders. There are currently no accepted or validated assessment tools and neither the range, frequency nor severity of GI symptoms has been systematically described in CF. We present results of a cross-sectional study using established tools and compare them to current measures of quality of life (QOL).
Methods
Consecutive patients attending specialist CF appointments were asked to complete questionnaires including the GI Symptom Rating Scale (GSRS); Irritable Bowel Syndrome Symptom Severity Score (IBS-SSS) and Cystic Fibrosis Questionnaire (CFQ-R). Questionnaire terminology was altered to replace references to ‘IBS’ with ‘GI symptoms’.
Results
In total, 107 patients were recruited (mean age, 27.8 ± 9.6 years; 60 female), and 94 (88%) had PEI. Body mass index was 22.1 ± 3.6 kg/m2, forced expiratory volume in one second was 59 + 27.7% predicted. Fifty-three (49.5%) were p.Phe508del homozygous. Overall 69/107 (65%) reported significant GI symptoms independent of PEI or adherence to pancreatic enzyme replacement therapy (PERT), with the four most frequent being attributable to the lower GI tract: bloating/distension, flatulence, abdominal pain and borborygmi (gurgling). There was no numerical correlation between any CFQ-R domain (particularly Digestion domain) and GSRS or SSS.
Conclusion
This is the first systematic study measuring GI symptoms in CF using validated GI tools. Symptoms are not related to PERT or genotype and appear to be captured well by the GSRS. Further research will study longitudinal changes with treatment, and therapeutic trials in CF may use these tools to demonstrate a positive impact on ‘non-respiratory’ symptoms and QOL.
Key summary
As the average age of patients with cystic fibrosis (CF) increases, new symptoms and presentations are becoming apparent. Chronic gastrointestinal (GI) symptoms may contribute significantly to the morbidity of CF, affecting quality of life even when pulmonary disease is well controlled. This article demonstrates a significantly higher prevalence of chronic GI symptoms in adults with CF (reminiscent of those reported in irritable bowel syndrome and inflammatory bowel disease), with ‘lower GI’ symptoms seeming to predominate. Validated symptom scores and tools established in other chronic GI disorders are of value in CF, but further work is required to determine whether they can be used to monitor progress.
Introduction
Mutations in the cystic fibrosis transmembrane regulator (CFTR) gene 1 also modulate the properties of other epithelial ion channels,2,3 which affect the intestinal milieu. A more acidic luminal environment 4 with more viscid mucus 5 ensues, with well-described primary effects including meconium ileus, distal intestinal obstruction syndrome (DIOS) and intussusception. 3
A host of other manifestations have also been reported including dysbiosis of the gut microbiome,6,7 low-grade intestinal inflammation8–10 and increased intestinal permeability.11,12 The recognition of this triad of phenomena has transformed our understanding of other chronic GI disorders, such as irritable bowel syndrome (IBS) and inflammatory bowel disease (IBD). In these conditions, clear mechanistic links can be drawn between GI physiology and the symptoms experienced.13,14 Anecdotally, many of the symptoms reported by patients with CF (bloating, constipation, epigastric discomfort) are highly reminiscent of those reported in these other GI disorders, particularly of the Rome IV criteria for IBS. 15 While it is not yet clear whether the same or similar mechanisms underlie these symptoms in CF, validated tools that assess symptoms in other GI disorders may be of immediate utility.
The influence of pancreatic exocrine insufficiency (PEI) in this setting is unknown, but its symptoms are well characterised and largely effectively treated by pancreatic enzyme replacement therapy (PERT). 16
To date, there are no systematic reports describing the range or impact of chronic GI symptoms in CF, but a validated reporting tool would be of value for academic and clinical purposes. We sought to determine whether tools validated in GI disorders could fulfil this role.
Methods
Setting
This was a prospective study of 107 consecutive patients attending the CF clinics (outpatient and inpatient) at King’s College Hospital, London.
Procedure
Data used in this study were collected using the Integrating Mental and Physical Healthcare: Research, Training & Services (IMPARTS; www.kcl.ac.uk/imparts) programme. IMPARTS is a multidimensional programme to enhance clinical care by integrating mental healthcare as part of routine clinical care in hospital settings. Routine patient-reported outcomes are collected using electronic tablets in clinical services, with real-time feedback to the electronic patient record (EPR).
Clinicians on the Cystic Fibrosis team explained the IMPARTS screening process to patients and that data might be used for research purposes. In this way, specific consent to complete questionnaires was not required, as they were introduced as part of a routine clinical care pathway, but IMPARTS has United Kingdom (UK) national research ethics committee approval to use pseudonymised data for research purposes (IMPARTS Research Database REC reference: 18/SC/0039, with original approval granted 4 June 2013 and renewed for a further five years on 5 June 2018). All research applications arising from use of the database are assessed and approved by a patient-led research oversight committee, in line with ethical requirements. Patients were also given an information sheet and informed that completion was voluntary. As such, this research conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
Upon completion of the measures, results were immediately uploaded and visible to the reviewing clinical team. Patients reporting GI symptoms (as well as those with psychological distress) were managed in the routine clinical service.
Questionnaires were administered in English. Patients with learning difficulties or language comprehension barriers that rendered them unable to use the tablet input method were excluded. Although interpreter services were available through the routine clinical service, there were no instances for which these were required.
Measures
All patients were asked to complete a series of self-reported questionnaires related to quality of life (QOL), anxiety and depression and GI symptoms.
The Patient Health Questionnaire (PHQ-9) 17 and Generalised Anxiety Disorder tool (GAD-7) 18 are well-validated screening tools for depression and anxiety in primary and secondary care settings, with nine and seven questions, respectively, asking about indicators over the past two weeks. Scores of 0–3 are assigned to each response according to frequency of occurrence, then totalled to arrive at a final score. The PHQ-9 was administered initially as the PHQ-2, a shortened version which, if respondents score 3 or more, triggers the nine-item questionnaire. For each, a score of 10 or more identifies a population requiring onward referral for psychological assessment and support.
GI symptoms were measured using the GI Rating Scale (GSRS)19,20 and the IBS Symptom Severity Score (IBS-SSS),20,21 both widely used in IBS studies. In our study, the term ‘IBS’ was removed from questionnaires and replaced with “gut symptoms” in order not to prejudice responses. The GSRS consists of 11 upper- and lower-GI symptoms rated on a four-point Likert scale (0 absent, 1 mild, 2 moderate, 3 severe). The IBS-SSS consists of five items (abdominal pain intensity, abdominal pain frequency, abdominal distension, dissatisfaction with bowel habits, interference of symptoms on life) each scored 0–100 using visual analogue scales, except for the abdominal pain frequency (reported as the number of pain days during the previous 10 days). For the GSRS, the scores for each domain are averaged to produce a final, total score for analysis, while the IBS-SSS domain scores are added to produce a total score out of 500.
QOL was measured using the CF QOL-revised questionnaire (Cystic Fibrosis Questionnaire-Revised (CFQ-R)), 22 a disease-specific tool consisting of questions informing 12 domains, producing an overall score of 0–100, with higher scores indicating higher QOL.
Stool form was measured using the Bristol Stool Form Scale (BSFS) based on retrospective recall of most common stool form. The BSFS consists of seven verbal and pictorial descriptors of stool form (Type 1–2 hard, Types 3–5 normal, Types 6–7 loose). It has been validated as a measure of stool form for use in healthy individuals and in patients with IBS. 23
Demographic and genotype data, as well as detailed questionnaires on PERT dosage and adherence, were collected as part of routine care and extracted from the EPR.
Data analysis
Data were extracted from the IMPARTS database and EPR, merged and pseudonymised. Data in tables are presented as mean and SDs for continuous, and median (minimum to maximum) for categorical variables. Statistical comparisons, conducted in GraphPad Prism v2.0, were by Student t-test or Mann-Whitney U-test dependent on distribution and correlation by Spearman rank coefficient.
Results
Data from 107 consecutive patients, consisting of 94 (88%) with PEI, of whom two were not taking PERT, were analysed. Across the cohort, 53 (49.5%) were p.Phe508del homozygous.
Comparative statistics, stratified for IBS-SSS.
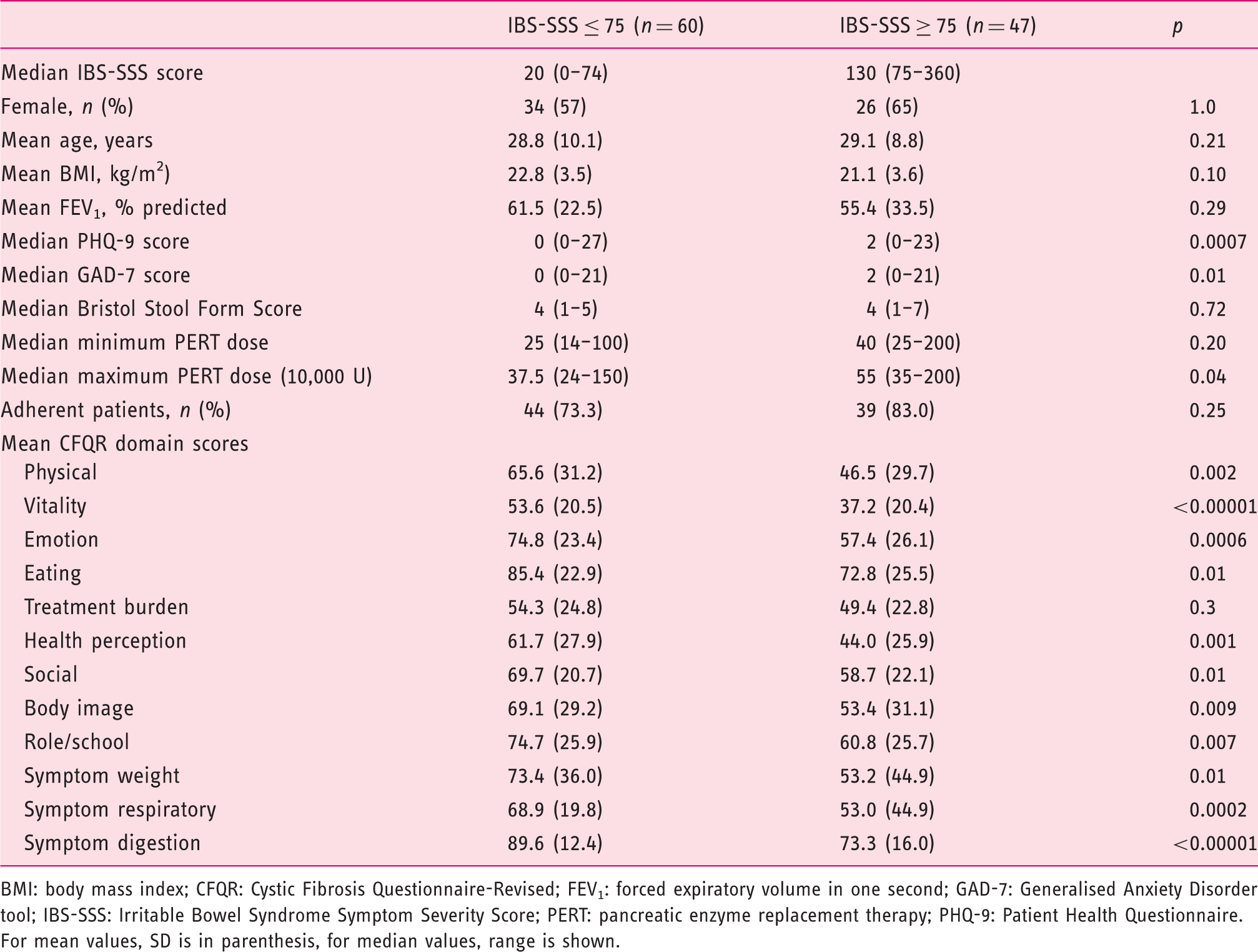
BMI: body mass index; CFQR: Cystic Fibrosis Questionnaire-Revised; FEV1: forced expiratory volume in one second; GAD-7: Generalised Anxiety Disorder tool; IBS-SSS: Irritable Bowel Syndrome Symptom Severity Score; PERT: pancreatic enzyme replacement therapy; PHQ-9: Patient Health Questionnaire.
For mean values, SD is in parenthesis, for median values, range is shown.
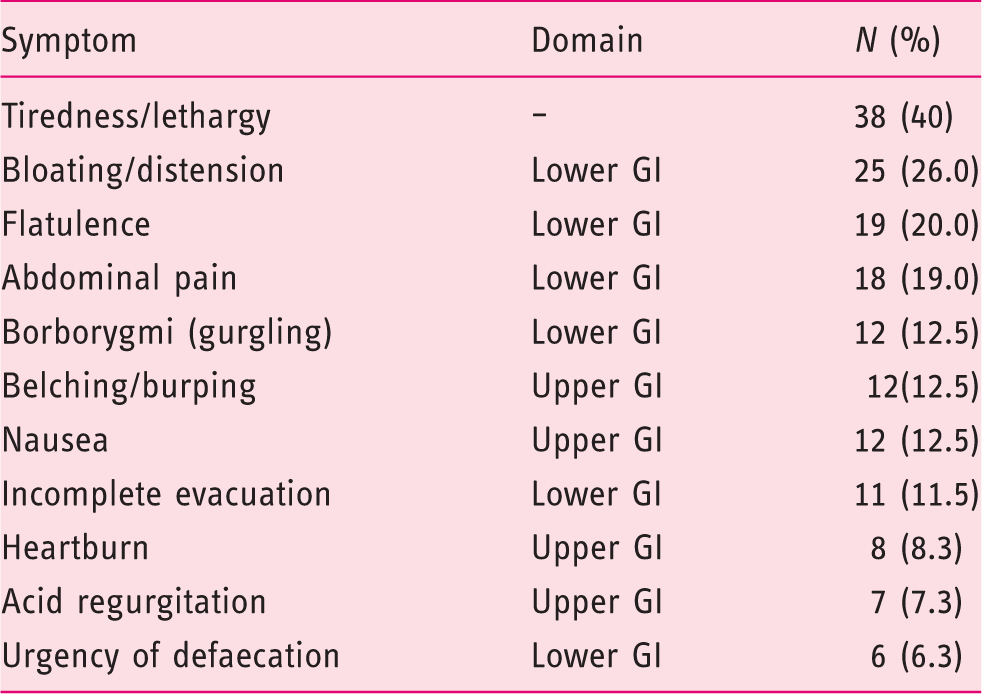
To visually represent the spread of individual GI symptoms, a ‘heatmap’ was devised (Figure 1), graded using absent, mild, moderate and severe for each of the symptoms of the GSRS (numbered 1–11), listed in numerical order for increasing IBS-SSS scores. Only nine (8.4%) patients reported no symptoms at all. Symptoms attributable to the lower-GI tract were more frequently reported as moderate or severe (i.e. clinically relevant), than those attributable to the upper-GI tract (91 reports vs 39, Table 2).
Gastrointestinal (GI) Symptom Rating Scale (GSRS) heatmap. The entire cohort is shown with every row representing an individual patient and his or her responses. Each column is a different domain of the GSRS. Each response is represented by a different colour: “None”=green, “Mild”=yellow, “Moderate”=amber, and “Severe” = red. GSRS symptoms are arranged from left to right “along” the GI tract, showing the majority of moderate and severe symptoms on the right-hand side of the heatmap, corresponding to symptoms that would be attributable to the lower-GI tract. IBS-SSS: Irritable Bowel Syndrome Symptom Severity Score. Reported frequency of moderate or severe symptoms on the Gastrointestinal Symptom Rating Scale in 96 patients reporting any gastrointestinal (GI) symptoms.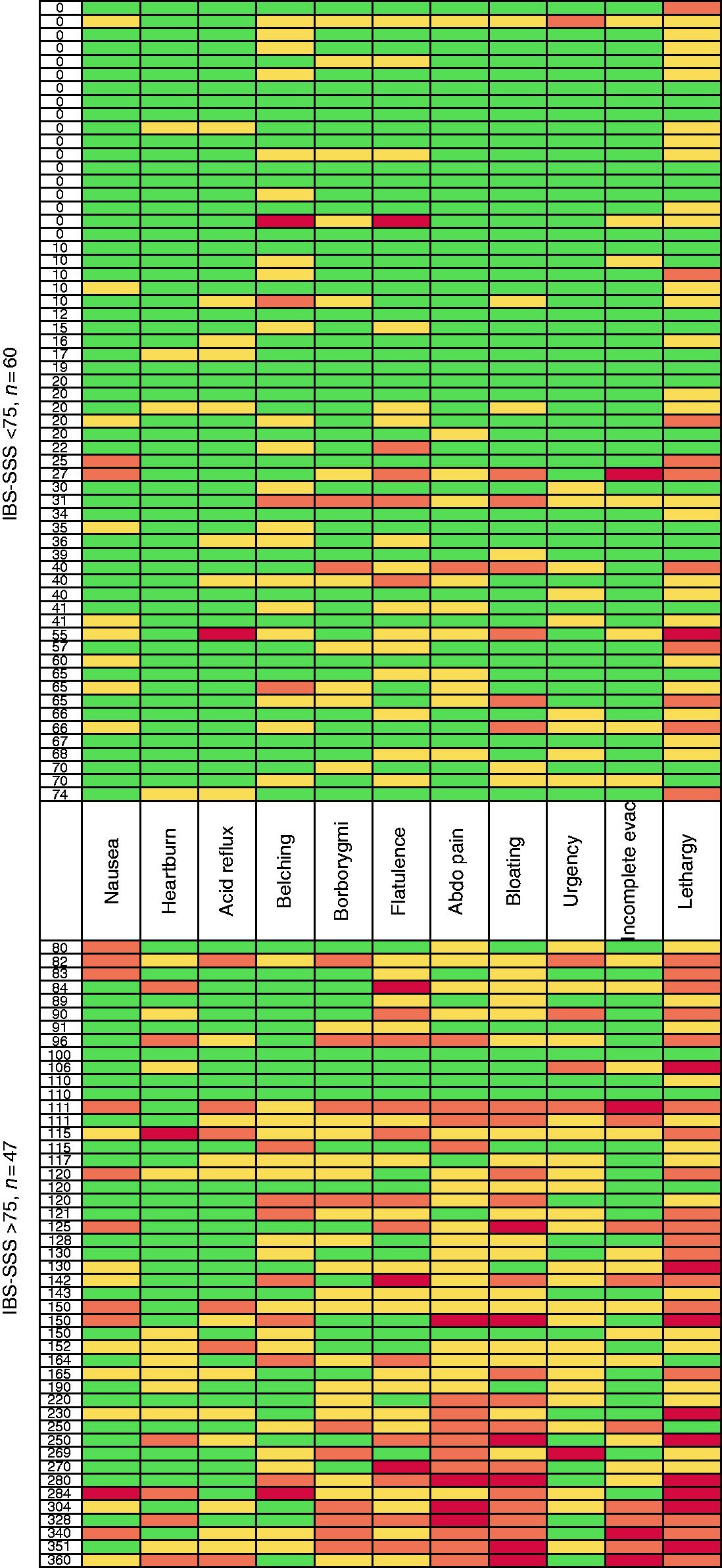
Scores both for PHQ-9 and GAD-7 were higher in patients reporting higher IBS-SSS (Table 1), with 21 (19.6%) and 18 (16.8%), respectively, meeting the criterion for onward referral and 11 meeting criteria on both questionnaires. For PHQ-9, 6/60 respondents requiring onward referral were in the IBS-SSS < 75 group, with 15/40 in the > 75 group (p = 0.0005). For GAD-7, these were 5/60 and 13/40 (p = 0.003), respectively.
Comparative statistics for patients calculating or estimating PERT dosage.
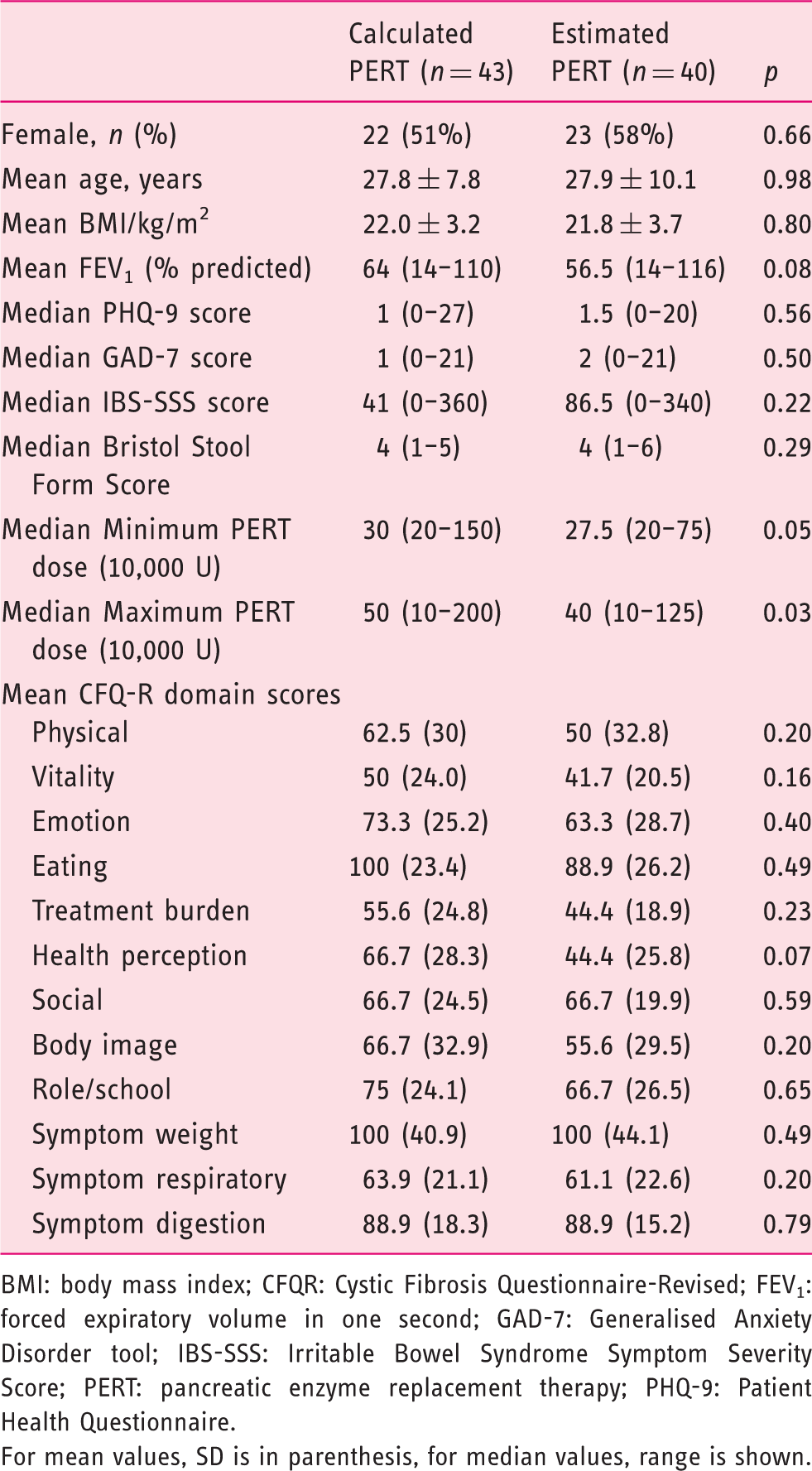
BMI: body mass index; CFQR: Cystic Fibrosis Questionnaire-Revised; FEV1: forced expiratory volume in one second; GAD-7: Generalised Anxiety Disorder tool; IBS-SSS: Irritable Bowel Syndrome Symptom Severity Score; PERT: pancreatic enzyme replacement therapy; PHQ-9: Patient Health Questionnaire.
For mean values, SD is in parenthesis, for median values, range is shown.
Discussion
This is the first study to comprehensively describe the range and impact of chronic GI symptoms in CF in a large cohort of unselected patients. The IBS-SSS was used as, anecdotally, many symptoms reported by CF patients were reminiscent of those seen in IBS. Many more CF patients in our cohort reported symptoms which met the Rome IV criteria for IBS than would be expected in the general population (5.5% in the UK 15 ), and a significant proportion of patients scored highly on the symptom severity tool for this disorder. While the exact mechanisms underlying these symptoms in CF are not yet known, there are clear parallels to other GI disorders. Categorising, but importantly not classifying, CF-GI symptoms in a similar way should allow symptom-directed and personalised intervention as they have in IBS. Tools validated for use in other GI disorders should also be immediately applicable in CF.
To explore this further, we employed a tool that encompasses both upper- and lower-GI symptoms, the GSRS. This demonstrates more patients reporting more severe symptoms, albeit broadly in line with IBS-SSS score. There does exist, however, a group of patients who do not score highly on the SSS but report significant symptoms on the GSRS, suggesting that the latter may be more the appropriate tool in terms of sensitivity, although we did not specifically assess this. Overall, as IBS-SSS increased, patients reported a higher frequency of moderate and severe symptoms on the GSRS, with a predominance of symptoms attributable to the lower-GI tract.
It is challenging to assess adherence (or otherwise) to PERT in routine clinical practice and could confound the assessment of lower-GI symptoms in particular. We asked for self-reporting of adherence in our study, but also whether patients estimated or calculated/counted out their PERT doses according to dietary intake. It is important to note that no patients reported steatorrhoea in our cohort, and although there was no difference in the minimum dose, the maximum PERT dose was actually significantly less for patients reporting SSS < 75 (if ‘underdosed’, patients might be expected to report worse symptoms). Furthermore, although patients estimating their enzyme requirements took significantly less than those calculating the dose, there was no difference in symptom scores in these two groups.. These observations are important as they imply mechanisms other than PEI (and PERT dosing) may also be responsible for the majority of chronic GI symptoms in CF.
The CFQR, while a comprehensive and established measure of QOL in CF, correlated with neither SSS nor GSRS. Furthermore, the Digestion domain of the questionnaire did not adequately capture the range of symptoms reported.
It is important to note, however, that the GSRS is not a ‘true’ patient-reported outcome measure (PROM) in the sense that it is not associated with a weighted score and the symptom descriptors rely on subjective perception using a Likert-type response scale rather than objective measures (for instance, symptom frequency). Validated GI PROMs, for instance, the patient assessment of upper gastrointestinal symptom severity index (PAGI-SYM 24 ) and patient assessment of constipation symptom severity index (PAC-SYM 25 ), could be applicable in this scenario. Each also has the advantage of being associated with a validated QOL tool (PAGI-QOL 26 and PAC-QOL 27 ). We did not use these tools in our study as we wished to ‘map’ GI symptoms and therefore used the GSRS as a disease-nonspecific tool. Given our observation that CF patients report both upper- and lower-GI symptoms (although lower-GI symptoms predominate in our cohort), it would be reasonable to use or develop tools to evaluate both. However, the PAGI-SYM, PAC-SYM and their related QOL tools are 20, 12, 28 and 30 items, respectively, so may be challenging to administer in routine practice. Prospective studies are clearly warranted to validate a responsive tool (or toolset) in CF.
The prevalence both of depression and anxiety in our cohort is significantly higher than would be expected in the general population (around 5%), 28 and patients reporting GI symptoms had higher indices of psychological distress. This is entirely expected from the modern understanding of chronic GI disorders as complex neuroimmune conditions.29,30 Using a biopsychosocial model of disease not only acknowledges the ‘brain-gut axis’ as a fundamental part of the syndrome,30,31 but also introduces a number of highly effective therapies which are ‘gut focussed’ rather than generic.31,32 Therapeutic strategies that take advantage of this interaction are likely to be of use in CF, and there may be an additional advantage in engaging experienced GI physicians to promote clinical collaboration to benefit patients with CF.
Although the mechanisms underlying lower GI symptoms in CF are not clearly understood, there is intriguing evidence that guanylyl cyclase (GC), known to be involved in patients with idiopathic constipation, 33 is also implicated in CF. 34 Furthermore linaclotide, licensed for idiopathic constipation, 33 targets GC, improves transit time in animal models and may, therefore, also treat constipation in patients with CF. A greater understanding of GI symptoms, their pathophysiological origins, and how to reliably assess and monitor them is vital to assessing the efficacy of such interventions.
Further work is necessary to determine which questionnaires (including those taking into account QOL) can be employed to monitor changes when patients are treated, or even to target or ‘personalise’ specific therapies as is possible in other GI disorders. The tools used in this study have already been validated in other conditions associated with chronic GI symptoms, so are expected to be applicable. Given their obvious frequency and impact, clinical trials of existing and novel therapies for CF could focus on GI symptoms using these questionnaires, for the first time demonstrating the value of CF therapy in other organs.
Footnotes
Conflict of interest
None declared
Ethics approval
Clinicians in the Cystic Fibrosis team explained the IMPARTS screening process to patients and that data might be used for research purposes. In this way, specific consent to complete questionnaires was not required, as they were introduced as part of a routine clinical care pathway, but IMPARTS has UK national research ethics committee approval to use pseudonymised data for research purposes (IMPARTS Research Database REC reference: 18/SC/0039, with original approval granted 4 June 2013 and renewed for a further five years on 5 June 2018). All research applications arising from use of the database are assessed and approved by a patient-led research oversight committee, in line with ethical requirements. Patients were also given an information sheet and informed that completion was voluntary. As such, this research conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
Funding
None declared
Informed consent
Specific informed consent was not required for this project, but the platform used to administer questionnaires (IMPARTS) has UK national research ethics committee approval (ref 18/SC/0039).