
Abstract
Background
Nutritional status is an important prognostic factor in patients with cystic fibrosis (CF) prior to lung transplantation.
Objective
To investigate the impact of nutritional status on pulmonary function in CF transplant recipients.
Methods
Adult double lung transplanted CF patients were consecutively included. The predictive value of nutritional status on lung function – measured by spirometry – was longitudinally assessed by body composition serially evaluated by a three-compartment model bioelectrical impedance analysis (BIA) in comparison to body mass index (BMI).
Results
Overall, 147 spirometries and 147 BIAs were performed in 58 patients (59% female, median age: 30.1 years, median BMI: 19.6 kg/m2). Malnourished patients (BMI < 18.5 kg/m2; 27.6%) had a significantly reduced lung function compared to normal/overweight patients (forced expiratory volume in 1 second in percent (FEV1%pred), 57% vs 77%; p = 0.024). BMI, as well as the BIA parameters phase angle, total body water, fat free mass, body cell mass (BCM) and extracellular mass (ECM)/BCM ratio, were univariate predictors of FEV1%pred. When included in a linear mixed model, ECM/BCM ratio remained the only significant predictor of lung function (p = 0.012).
Conclusion
Nutritional status assessed by BIA predicted lung function in CF transplant recipients. Serial BIA measurements to monitor patients’ nutritional status might help to improve or maintain lung function.
Keywords
Key summary
Nutritional status is a key prognostic factor of lung function and survival in patients with cystic fibrosis (CF) prior to lung transplantation, but data are limited on its impact on lung function after transplantation. This study used serial measurements of body composition by a three-compartment model bioelectrical impedance analysis (BIA) in comparison to body mass index in order to analyse its impact on pulmonary function in adult CF transplant recipients. Extracellular mass/body cell mass ratio as measured by BIA accurately predicted lung function over time in CF transplant recipients. Serial BIA measurements to survey patients’ nutritional status might aid the improvement or preservation of lung function after transplantation.
Introduction
Cystic fibrosis (CF) is the third most common indication for lung transplantation (LT), accounting for 16.8% of all LT worldwide. 1 Whereas CF is mostly recognized for its pulmonary morbidity, multiple clinical features of the disease manifest as gastrointestinal and nutritional alterations. Exocrine pancreatic insufficiency (PI), 2 CF-related diabetes (CFRD) 3 and frequent intestinal dysbiosis, as well as intestinal inflammation, may contribute to malnutrition and deficiency of fat-soluble vitamins such as vitamin D. 4 Numerous studies have examined the association between nutritional status and lung function in CF patients prior to LT, and malnutrition has been identified as a key factor for worse prognosis. 5 Vitamin D deficiency has been associated with impaired lung function in non-transplanted CF patients,6,7 and might be associated with an increased risk of rejection and infections after LT. 8 Subsequently, nutritional support has been shown to defer impairment of pulmonary function and improve survival in LT candidates.9–12 However, data on the impact of nutritional status on lung function in LT recipients are limited.
The most frequently used method for the assessment of nutritional status is the calculation of the body mass index (BMI; kg/m2). Yet, reliability may be affected by the presence of oedema and poor association with fat free body mass (FFM). 13 Further methods, such as skin fold thickness, dual-energy X-ray absorptiometry (DXA) and bioelectrical impedance analysis (BIA) were investigated in collectives of non-transplanted CF patients: measurement of skin fold thickness is commonly used for assessment of fat mass (FM), 14 but neglects muscle mass, an important factor for pulmonary function. 15 BIA enables the estimation of several body compartments, namely FM, FFM, body cell mass (BCM) and total body water (TBW). 16 In contrast to other body composition assessment methods like DXA, BIA does not expose subjects to ionizing radiation. 17 Recently, Charatsi et al. evaluated BIA in comparison to DXA in a cross-sectional study of 54 paediatric CF patients and reported a very good accordance of both techniques, thus demonstrating that BIA can be reliably used in CF patients. 18 Additionally, patients with reduced FFM values showed worse pulmonary function, a finding that merits further attention.
The aim of this study was to evaluate the impact of nutritional status as assessed by serial BIA measurements in comparison to BMI on lung function over time in adult CF transplant recipients.
Patients and methods
All patients with confirmed diagnosis of CF according to standard criteria aged ≥ 18 years, who had undergone bilateral LT due to CF-associated lung disease and attending our CF outpatient service between January 2012 and July 2015, were consecutively included in this study.
Nutritional status was evaluated by BMI (weight (kg)/height (m2)) and body composition, as measured by three-compartment model BIA. In addition, routine laboratory values including 25-hydroxy (OH) vitamin D were measured, and the presence of CFRD, new onset diabetes after transplantation (NODAT), osteoporosis/osteopenia and exocrine PI was assessed according to standard diagnostic criteria.
Subjects were grouped in four BMI categories as suggested by the World Health Organization WHO: 19 malnutrition (<18.5 kg/m2), adequate weight (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2) or obese (≥30 kg/m2).
Body composition was assessed by single-frequency BIA (Biacorpus RX 4000®; MEDI CAL Health Care GmbH, Karlsruhe, Germany) according to European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines. 16 BIA was performed after bladder emptying, unclothed and in a fasted state. Using alternating current with a frequency of 50 kHz, the resistive resistance (measure for body water), the capacitive resistance (measure for muscle mass) and the phase angle (PA; measure for BCM) can be measured with high precision. Via this three-compartment model of BIA, we were able to evaluate FM, extracellular mass (ECM) and BCM (muscle and organ cell mass), as well as FFM, PA, TBW and the ECM/BCM ratio.
Pulmonary function was evaluated by spirometry. For statistical analysis, VCmax (maximum vital capacity in liters), VCmax%predicted (%pred; in percent), FEV1 (forced expiratory volume in one second in L), FEV1%pred (predicted FEV1), FEV1/VCmax ratio (in percent), FEV1/VCmax%pred, MEF50 (maximal expiratory flow on 50% of forced vital capacity in L/sec), MEF50%pred (predicted MEF50), TLC (total lung capacity in litres) and TLC%pred (predicted TLC) were included. Furthermore, a detailed medical history was obtained, including history or development of bronchiolitis obliterans syndrome (BOS). BOS grading was performed according to Estenne et al. 20
BMI calculation, BIA measurements, spirometries and laboratory testing were serially performed at each outpatient visit at up to five time points (time points 1–5 = T1–T5). Patients with active infections as assessed by C-reactive protein and chart review were not included in the study.
The study was performed in accordance with the guidelines of the Declaration of Helsinki (1964, including current revisions) and Good Clinical Practice Guidelines. The study protocol was approved by the Ethics Committee of the Medical University of Vienna (protocol number 1818/2013, date of approval: 4 March 2014). Written informed consent was obtained from each patient included in the study after March 2014, while written informed consent was waived for patients included before.
Statistical considerations
To identify predictors of pulmonary function, we used a linear mixed model that enabled us to account for repeated measurements within patients. The dependent variable was FEV1%pred. The model included time since LT, BMI and the BIA parameters PA, TBW, FFM, ECM, BCM, FM and ECM/BCM as fixed effects, and the patients as random effect. Spearman’s correlation coefficient was calculated to describe statistical associations between lung function parameters and laboratory parameters. Changes in BMI, BIA and lung function parameters over time (T1–T5) were analysed by descriptive statistics. Continuous parameters were compared using the Mann–Whitney U-test. Categorial variables were compared using a χ 2 test or Fisher’s exact test, where appropriate. A p-value of < 0.05 was considered statistically significant. Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 24.0 and R 3.3.1.
Results
In total, 147 test time points (T1: n = 58, T2: n = 38, T3: n = 29, T4: n = 14 and T5: n = 8), comprising BMI calculation, BIA measurement, spirometry (supplementary table 1) and laboratory testing were analysed in 58 consecutive patients (58.6% (n = 34/58) female, median age 30.1 years). The median observation period per patient was 10.3 months (interquartile range (IQR): 0.3; 18.4). The median time range between each test time point was 3.8 months (IQR: 3.1; 5.4). All patients included in the study had been double lung transplanted within a median time period of 2.3 years (IQR: 0.6; 7.6).
Patient characteristics at first presentation.
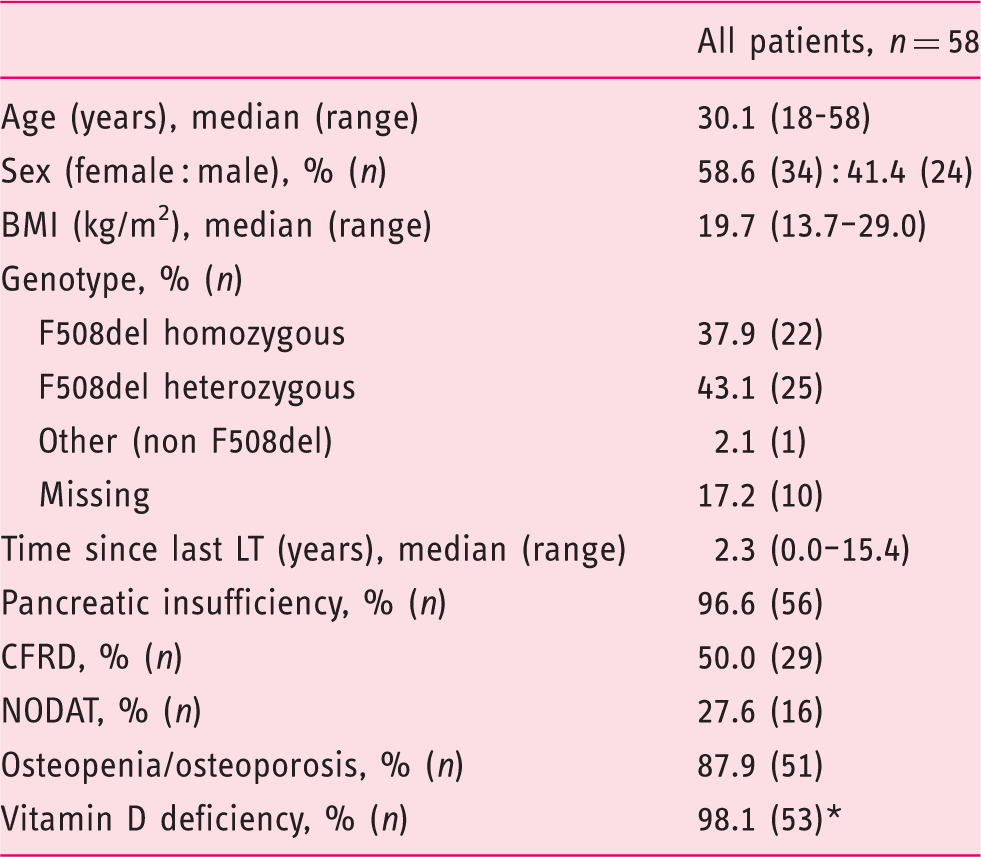
Asterisk indicates data available for 54 of 58 patients; normal range: 75–250 nmol/L.
BMI: body mass index; LT: lung transplantation; CFRD: cystic fibrosis related diabetes; NODAT: new onset diabetes after transplantation.
Laboratory values at first presentation.
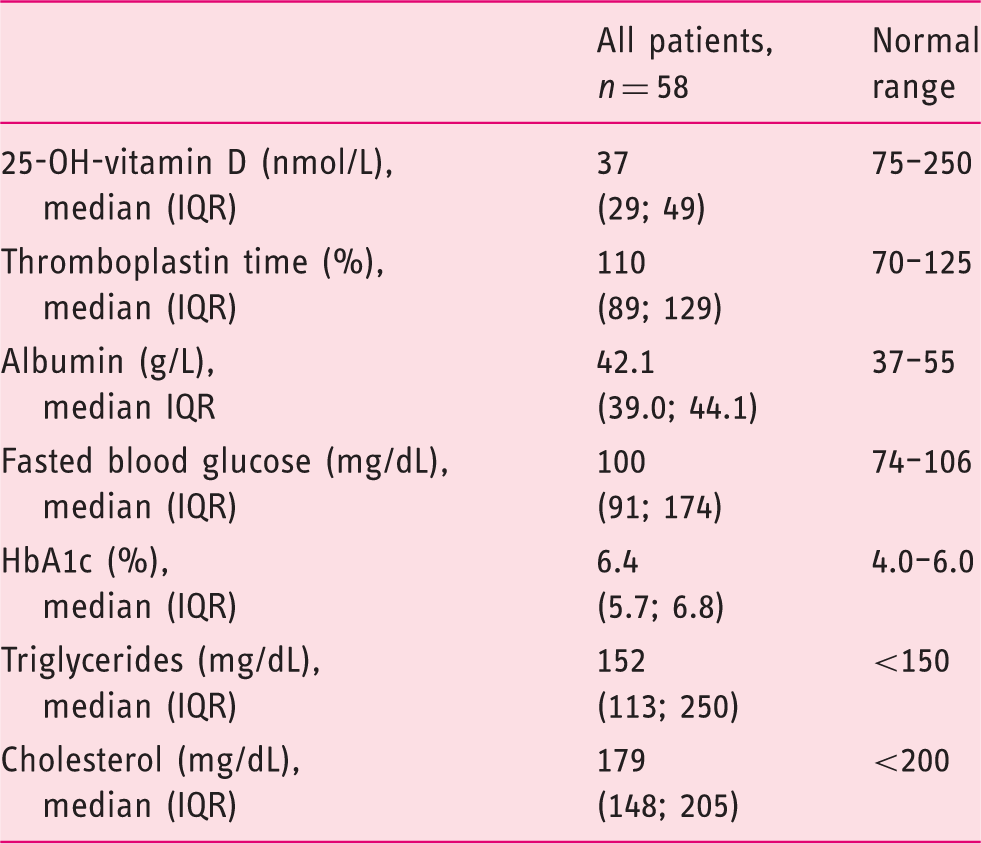
IQR: interquartile range.
Besides, four patients had received re-double LT prior to study inclusion, whereas none had to be re-transplanted within the study period. Overall, 32.8% (n = 19/58) of patients were diagnosed with BOS before or during the study period (n = 3: BOS 0-p, n = 5: BOS 1, n = 4: BOS 2 and n = 7: BOS 3). Three of them therefore underwent extracorporal photopheresis. Four out of 58 patients (6.9%) died within the observation period due to sepsis (data not shown).
The impact of BMI on lung function
Changes in median predicted forced expiratory volume in 1 second in malnourished (body mass index < 18.5) vs normal/overweight (body mass index ≥ 18.5) patients over time (time points T1–T5).
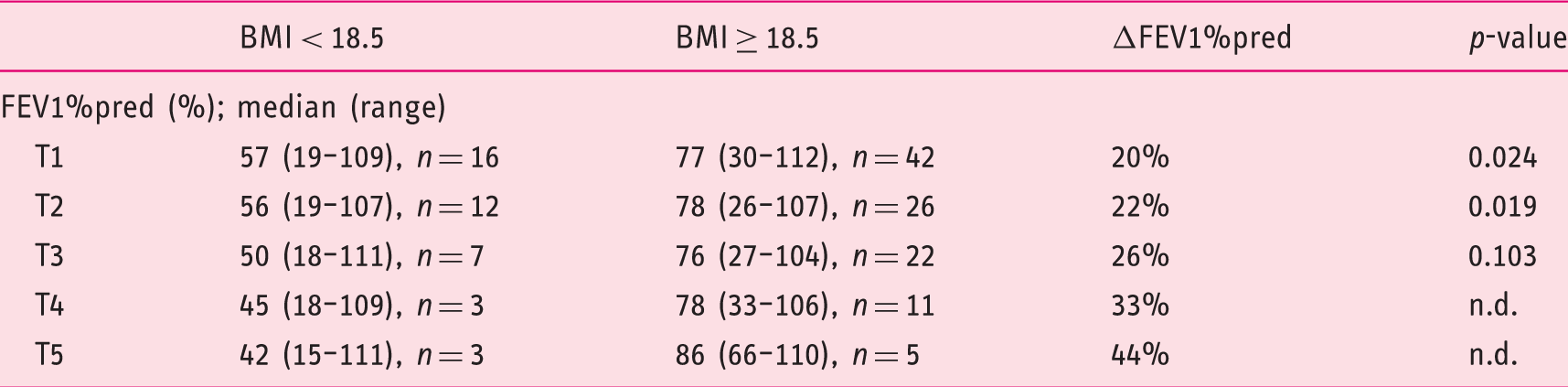
The median observation period per patient was 10.3 months (interquartile range: 0.3; 18.4).
FEV1%pred: predicted forced expiratory volume in 1 second; BMI: body mass index; T: time point; n.d.: not done due to low patient numbers per group.
BIA is superior to BMI in prediction of lung function
Univariate and multivariate analysis of prediction of FEV1%pred by time since lung transplantation, BMI and BIA parameters.
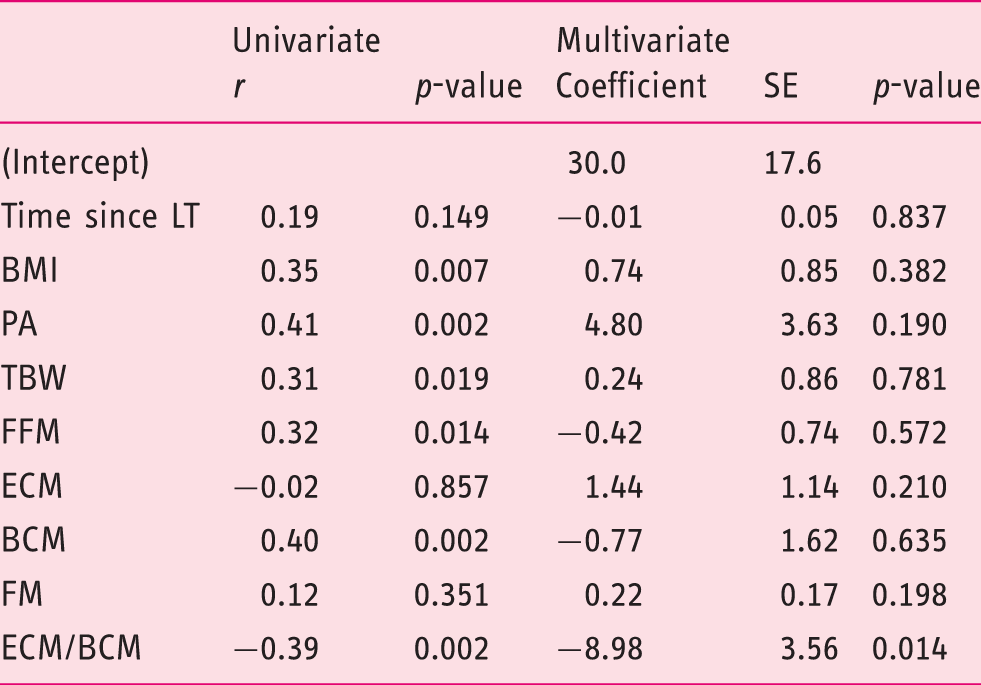
After multivariate analysis by a linear mixed model only ECM/BCM remained a significant predictor of predicted forced expiratory volume in 1 second.
r: Spearman’s correlation coefficient; SE: standard error; LT: lung transplantation; BMI: body mass index; PA: phase angle; TBW: total body water; FFM: fat free mass; ECM: extracellular mass; BCM: body cell mass; FM: fat mass.
Changes in median extracellular mass/body cell mass in malnourished (body mass index < 18.5) vs normal/overweight patients (body mass index ≥ 18.5) over time (time points T1–T5).
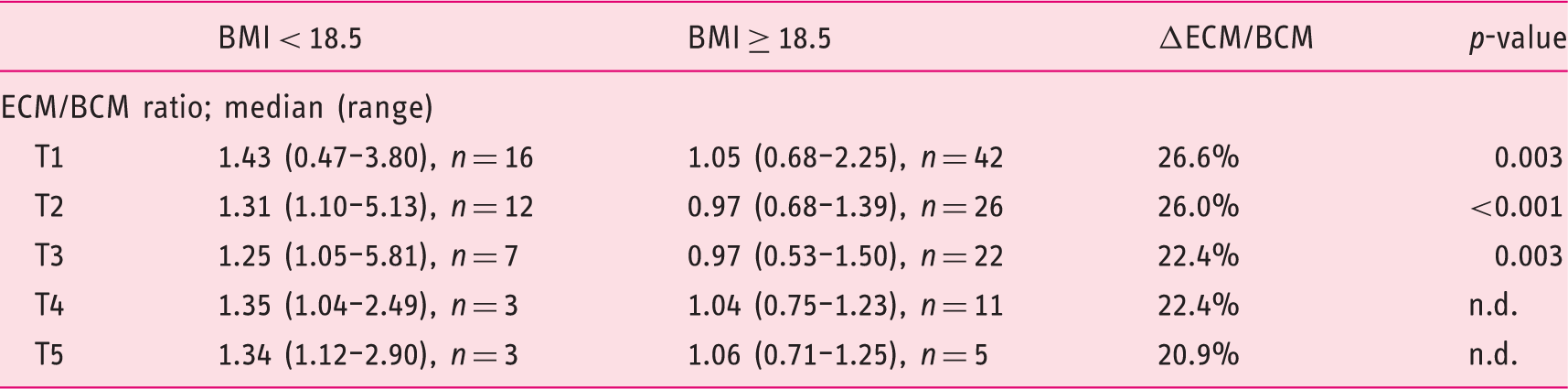
The median observation period per patient was 10.3 months (interquartile range: 0.3; 18.4). Normal range of extracellular mass/body cell mass: < 1.0.
BMI: body mass index; ECM: extracellular mass; BCM: body cell mass; n.d.: not done due to low patient numbers per group.
25-OH-vitamin D levels are associated with lung function after lung transplantation
25-OH-vitamin D values were available in 93.1% (n = 54/58) of patients at T1. Despite continuous vitamin supplementation in the majority of patients (median vitamin D supplementation dosage of 800 IU; range: 100–4000), vitamin D deficiency was found in 98.1% (n = 53/54). The median vitamin D level was 37.2 nmol/L (range: 10.0–91.1). 25-OH-vitamin D levels were significantly correlated with VCmax (r = 0.335, p = 0.017) and TLC (r = 0.310, p = 0.028), but not with FEV1%pred. No significant difference was observed between patients with or without BOS with regard to 25-OH-vitamin D levels (data not shown).
Discussion
The present study showed that more than one-quarter of our adult CF double lung transplanted patient cohort was malnourished (BMI < 18.5 kg/m2). In comparison to normal/overweight patients, malnourished patients had significantly impaired pulmonary function and FEV1%pred decreased over time, whereas the FEV1%pred remained stable in the normal/overweight patients during the observation period. BMI, as well as the BIA parameters PA, TBW, FFM, BCM and ECM/BCM, were univariate predictors of lung function. However, in multivariate analysis, ECM/BCM ratio measured by a three-compartment model (BIA) remained the only significant factor for the prediction of lung function. Vitamin D deficiency was highly prevalent, and 25-OH-vitamin D levels correlated with VCmax and TLC, but not FEV1%pred after LT.
Since malnutrition has been identified as a risk factor for impaired outcome in CF patients, 21 some effort has been made to reliably assess nutritional status beyond the use of BMI. An observational, cross-sectional study of 40 adults with CF showed that body composition measured by DXA and BIA displayed a relationship between FFM loss and diaphragm muscle mass, and thus lung function. 22 Furthermore, BIA and DXA measurements were highly correlated in a study by Ziai et al., 23 with BIA slightly underestimating FM and overestimating FFM. The authors concluded that, assuming that BIA error is constant over time, these differences might not have a significant impact when serial BIAs are performed. Ultimately, in a recent study, Charatsi et al. evaluated BIA in comparison to DXA in 54 paediatric CF patients. The authors reported a very good accordance of both techniques and demonstrated that patients with reduced FFM, consisting of the body’s water, bone, organs and muscle content, showed worse pulmonary function. 18
In our study using serial BIAs, the parameter ECM/BCM ratio was the most accurate predictor of pulmonary function and superior to FFM. BCM consists of the whole-body cell mass, such as metabolically active organs and particularly muscles, whereas ECM includes the connective tissues such as collagen, elastin, skin, chords and bones, as well as interstitial water. In healthy individuals, the BCM is always higher than the ECM, so that the ratio is < 1. 24 Therefore, a rising ECM/BCM ratio is an early warning sign of a worsening nutritional status. It has been formerly found to be a useful predictor of malnutrition in cancer patients. 25
The number of malnourished patients in our study cohort was comparable to those reported elsewhere. 5 One of the possible factors contributing to malnutrition in post-LT CF patients is inadequately treated or underdiagnosed endocrine and/or exocrine PI. Of note, 96.6% of our patients were pancreatic insufficient. Furthermore, about 80% of our post-transplant CF patients were diabetics (CFRD or NODAT), a proportion that is much higher than previously described in pre-transplant CF patients. 26 This underlines the importance of sufficient pancreas enzyme replacement treatment (PERT), as well as thorough diabetes screening not only prior to, but also after, LT.
In view of the fact that 98.1% of our patients were vitamin D deficient, regular measurements of vitamin D levels and adequate substitution are mandatory and, besides PERT, already an important cornerstone in CF care. 27 25-OH-vitamin D levels showed a significant statistical association with absolute values of lung function in our patient cohort of lung transplanted adult CF patients, but no difference concerning the prevalence of BOS. This finding is in line with a recently published a single-center, double blind, randomized, placebo-controlled, prevention trial of once-monthly oral vitamin D vs placebo that failed to demonstrate a significant beneficial effect of vitamin D on chronic lung allograft dysfunction. 28 In the third National Health and Nutrition Examination Survey, 29 a strong relationship between serum concentrations of 25-OH-vitamin D, FEV1 (L), and FVC (L) was described, but this study did not examine CF patients. Vitamin D has also been associated with the strength of muscles. 30 In view of these findings, it is interesting that a recent Cochrane analysis 31 of vitamin D supplementation in CF found no evidence of clinical benefit or harm in the limited number of small-sized published studies. Future studies should address whether vitamin D supplementation in post-LT CF patients might have an impact on lung function preservation and post-transplant survival.
Our study findings are limited by the retrospective study design, and changes in pulmonary function during the longitudinal follow-up have to be interpreted with caution. Subclinical infections not assessed by laboratory parameters could have been missed and could have altered lung function assessment. Validation of our results in larger prospective patient collectives is desirable.
Finally, BIA represents a non-invasive, safe, fast, mobile and easy-to-use procedure to evaluate body composition. Thus, it may be used in everyday clinical practice and bears the advantage of repeatability at every patient follow-up. When used repeatedly, as in our study, it might be an additional tool for patient motivation in adhering to dietary recommendations and physical training plans. In conclusion, malnutrition, diabetes and vitamin D deficiency, all of which are factors that might contribute to reduced immunity, are highly prevalent in post-transplant CF patients. Body composition as assessed by BIA was superior to BMI in prediction of lung function in this study, which is to the best of our knowledge the first study to systematically assess serial BIA measurements in post-LT adult CF patients. Continuous care by a multidisciplinary and specialized team of dietitians and gastroenterologists trained in CF care might help to improve the nutritional status, and thereby preserve the lung function of, CF patients after LT.
Supplemental Material
Supplementary Figure -Supplemental material for Impact of nutritional status on pulmonary function after lung transplantation for cystic fibrosis
Supplemental material, Supplementary Figure for Impact of nutritional status on pulmonary function after lung transplantation for cystic fibrosis by Katharina Staufer, Emina Halilbasic, Peter Hillebrand, Solveig Harm, Stefan Schwarz, Peter Jaksch, Danijel Kivaranovic, Walter Klepetko, Michael Trauner and Lili Kazemi-Shirazi in United European Gastroenterology Journal
Supplemental Material
Supplementary Tables -Supplemental material for Impact of nutritional status on pulmonary function after lung transplantation for cystic fibrosis
Supplemental material, Supplementary Tables for Impact of nutritional status on pulmonary function after lung transplantation for cystic fibrosis by Katharina Staufer, Emina Halilbasic, Peter Hillebrand, Solveig Harm, Stefan Schwarz, Peter Jaksch, Danijel Kivaranovic, Walter Klepetko, Michael Trauner and Lili Kazemi-Shirazi in United European Gastroenterology Journal
Footnotes
Acknowledgements
We would like to thank Erich Horak and Martina Fischl from our dietician’s team for their expert criticism and support in the performance of BIA analysis.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethics approval
The study protocol was approved by the Ethics Committee of the Medical University of Vienna (protocol number 1818/2013, date of approval: 4 March 2014).
Informed consent
Written informed consent was obtained from each patient included in the study after March 2014, while written informed consent was waived for patients included before.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.