
Abstract
Background
Inability to advance to an oral diet, or oral feeding intolerance, is a common complication in patients with acute pancreatitis associated with worse clinical outcomes. The factors related to oral feeding intolerance are not well studied.
Objective
We aimed to determine the incidence and risk factors of oral feeding intolerance in acute pancreatitis.
Methods
Patients were prospectively enrolled in the Acute Pancreatitis Patient Registry to Examine Novel Therapies in Clinical Experience (APPRENTICE), an international acute pancreatitis registry, between 2015 and 2018. Oral feeding intolerance was defined as worsening abdominal pain and/or vomiting after resumption of oral diet. The timing of the initial feeding attempt was stratified based on the day of hospitalization. Multivariable logistic regression was performed to assess for independent risk factors/predictors of oral feeding intolerance.
Results
Of 1233 acute pancreatitis patients included in the study, 160 (13%) experienced oral feeding intolerance. The incidence of oral feeding intolerance was similar irrespective of the timing of the initial feeding attempt relative to hospital admission day (P = 0.41). Patients with oral feeding intolerance were more likely to be younger (45 vs. 50 years of age), men (61% vs. 49%) and active alcohol users (44% vs. 36%). They also had higher blood urea nitrogen (20 vs. 15 mg/dL; P<0.001) and hematocrit levels (41.7% vs. 40.5%; P = 0.017) on admission; were more likely to have a non-biliary acute pancreatitis etiology (69% vs. 51%), systemic inflammatory response syndrome of 2 or greater on admission (49% vs. 35%) and at 48 hours (50% vs. 26%;), develop pancreatic necrosis (29% vs. 13%), moderate to severe acute pancreatitis (41% vs. 24%) and have a longer hospital stay (10 vs. 6 days; all P<0.04). The adjusted analysis showed that systemic inflammatory response syndrome of 2 or greater at 48 hours (odds ratio 3.10; 95% confidence interval 1.83–5.25) and a non-biliary acute pancreatitis etiology (odds ratio 1.65; 95% confidence interval 1.01–2.69) were independent risk factors for oral feeding intolerance.
Conclusion
Oral feeding intolerance occurs in 13% of acute pancreatitis patients and is independently associated with systemic inflammatory response syndrome at 48 hours and a non-biliary etiology.
Keywords
Key summary
Current knowledge on this subject
Oral feeding intolerance is a relatively common complication of acute pancreatitis; Oral feeding intolerance results in longer hospitalization and frequent readmissions.
What is new in this study
The incidence of oral feeding intolerance is similar irrespective of the timing of the initial feeding attempt; Oral feeding intolerance is independently associated with systemic inflammatory response syndrome at 48 hours and non-biliary etiology.
Introduction
Oral feeding intolerance (OFI) is a well-known complication of acute pancreatitis (AP). 1 This condition is characterized by recurrent gastrointestinal symptoms on resuming an oral diet, such as abdominal pain, nausea and vomiting, often seen in association with biochemical abnormalities and increased opioid requirements during hospitalization. 1 It is estimated that approximately one in five patients with AP are diagnosed with OFI.1–3 AP patients with OFI achieved lower scores in five out of six quality of life domains, 4 and have a higher risk of readmission following hospital discharge. 5
There is no standardized approach to oral refeeding in AP and it varies based on the treating physician’s preference on timing, route and type of nutrition. 6 In mild AP, evidence-based and societal guidelines support early oral refeeding. 7 In contrast, patients with predicted moderately severe or severe AP may require the initiation of early enteral nutritional support rather than oral diet.6,8
A few studies in AP have assessed the potential predictors of OFI, but none of these has been adopted into clinical practice.1–3,5,8–14 As such, a ‘one size fits all’ approach as it relates to oral refeeding in AP is likely to result in suboptimal clinical outcomes. A novel approach to address this problem could evaluate and incorporate unique patient and disease-related risk factors for OFI to guide the nutrition management plan in AP. Patients determined to be at high risk of OFI may require early enteral nutrition as the initial approach. On the other hand, patients at low risk of OFI could start oral feeds early in the hospital course, aiming for early discharge and reducing the length of hospitalization.
The aim of our study was to determine clinically meaningful risk factors and predictors of OFI utilizing an international, prospective cohort of AP patients.
Methods
Study design
The Acute Pancreatitis Patient Registry to Examine Novel Therapies in Clinical Experience (APPRENTICE) is an international, multicenter collaboration including 22 centers around the world.15,16 This consortium includes eight centers in the United States, five in Latin America, six in Europe and three in India. Patients were prospectively enrolled between November 2015 and January 2018. The study protocol was approved by the institutional review board or ethics committee at each participating study site (PRO15040389/approval date: 07/14/2015). Each participating site submitted a data-use agreement form to the coordinating center. The study protocol conforms to the ethical guidelines of the World Medical Association Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.
The inclusion/exclusion criteria were universally implemented throughout all sites. Subjects were at least 18 years old, willing to participate and enrolled within 7 days from onset of pain. Patients with chronic pancreatitis or pancreatic cancer were excluded. Written, informed consent was obtained from all subjects. Standardized questionnaires were used to obtain information on demographics, etiology of AP, coexisting comorbidities, laboratory values and clinical outcomes of enrolled subjects. For transferred patients, early data were collected from the referral hospital. All data were entered by the enrolling site in a centralized research electronic data capture (REDCap) database. The data were de-identified and monitored by the University of Pittsburgh, which functioned as the coordinating center.
Study variables/definitions
The AP cohort was categorized in groups based on the nutrition route. The oral group included all patients who were initially fed orally. Patients in the oral group were further characterized as either tolerant or intolerant. OFI was defined as worsening abdominal pain and/or vomiting after resumption of any type of oral diet. Patients who consumed their initial meal with minimal abdominal pain and/or nausea that was not enough to discourage them from eating were classified as tolerant. Subjects who did not tolerate the oral feeding attempt, were unable to consume a significant portion of their meal due to the recurrence of symptoms, required increased doses of analgesic and antiemetic medications, or developed emesis were termed intolerant. Patients who were initially fed through the enteral route or parenteral route were classified in the non-oral group.
Active alcohol use was defined as the consumption of alcohol over the past 6 months and smoking as active tobacco use in the past 6 months. Patients who fulfilled at least two out of the four systemic inflammatory response syndrome (SIRS) criteria were characterized as SIRS positive. The revised Atlanta classification (RAC) was used to define severity, dividing patients into three groups: mild, moderately severe and severe. 17 The lipase ratio was defined as the recorded lipase level divided by the upper limit of normal for a given institution. Length of stay was defined as the total hospital stay, including days of hospitalization in both the initial and the referral hospital for transferred patients. The timing of the initial feeding attempt was determined relative to the initial admission date.
Statistical analysis
Categorical variables were described using percentages, and continuous variables were described using the median and interquartile range (IQR). Pearson’s chi-square and Wilcoxon’s rank-sum tests were used to compare categorical and continuous variables across groups, respectively. Univariate analysis was performed to examine the association between clinical variables and OFI. Covariates included age, gender, comorbidities, active alcohol and tobacco use, transfer status, previous history of AP, etiology of AP, admission blood urea nitrogen (BUN) and hematocrit levels, positive SIRS status on admission, and at 48 hours of hospitalization and the development of pancreatic necrosis.
A multivariable logistic regression model was subsequently constructed to determine whether any of the variables found to be significant in univariate analyses (P value < 0.05) were independently associated with OFI. We set out to develop a model to predict OFI including the following variables: age, gender, alcohol and smoking use, transfer status, recurrent attacks, non-biliary etiology, admission BUN, hematocrit, and admission and 48-hour SIRS. Cross-validation was performed by splitting the dataset into 10 equally sized training sets. Logistic regression analysis was performed in nine of them to estimate the probability of having OFI as a function of predictors. Subsequently, the predicted probability of OFI was calculated in the omitted training set. This was repeated until all 10 training sets had predicted probabilities calculated. The above process was then iterated 200 times by randomly splitting the patient cohort. A receiver operating characteristic curve was developed including the predictive probabilities of all the 200 models.
Finally, patients with an initial oral feeding attempt and patients who were directly introduced to enteral or total parenteral nutrition (TPN) were compared with respect to demographics, laboratory values and clinical outcomes. All statistical analysis was conducted using STATA 15.1. A P value of less than 0.05 was considered statistically significant.
Results
Overall, 1544 patients were enrolled, of which 105 were excluded from the study due to incomplete data related to OFI (Figure 1). Out of the included 1439 patients, 1233 (85.6%) were categorized in the oral group and 206 patients (14.3%) had a non-oral initial feeding attempt. More specifically, in the non-oral group the feeding route initially attempted was enteral for 119 patients (nasogastric or percutaneous endoscopic gastrostomy for 25 patients, nasojejunal or percutaneous endoscopic jejunostomy for 94) and TPN for 87 patients.
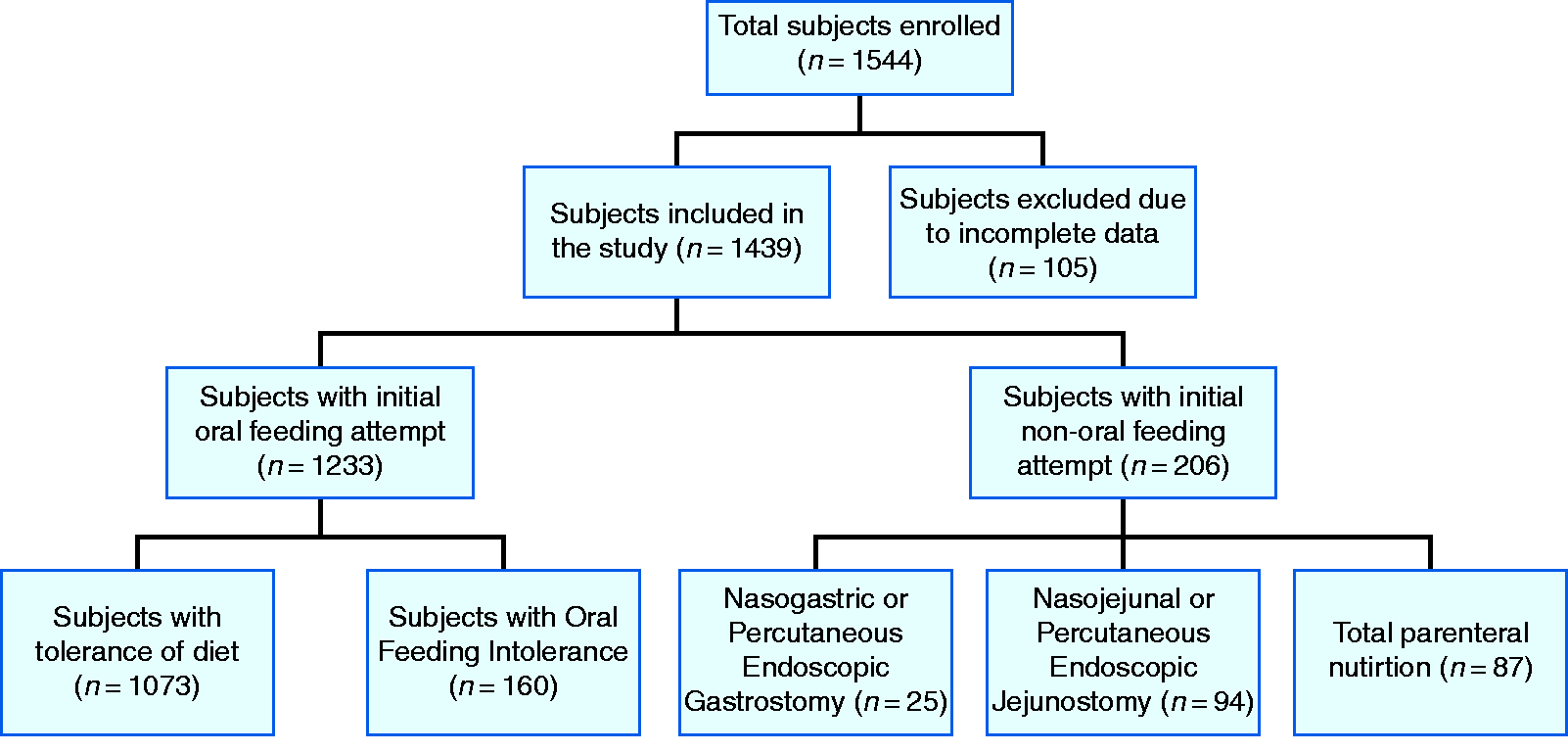
Flow chart of the subjects through the study.
Out of the 1233 patients in the oral group, 1073 (87%) were tolerant and 160 (13%) met the criteria for OFI. Patients who developed OFI were younger (45 vs. 50 years; P = 0.018), predominantly men (61% vs. 49%; P = 0.004), active drinkers (44% vs. 36%; P = 0.034) and smokers (29% vs. 21%; P = 0.022) (Table 1). Patients intolerant of oral feeding were more likely to be transferred from an outside hospital (38% vs. 29%; P = 0.02), and had a lower lipase ratio on admission (9.4 vs. 14.7; P = 0.019). A non-biliary etiology was found to be more common in the intolerant group (69% vs. 51%; P < 0.001). The intolerant patients also had higher BUN (20 vs. 15 mg/dL; P < 0.001) and hematocrit levels on admission (41.7% vs. 40.5%; P = 0.017). They were more likely to be SIRS positive on admission (49% vs. 35%; P < 0.001) and at 48 hours (50% vs. 26%; P < 0.001), develop pancreatic necrosis (29% vs. 13%; P < 0.001) and moderate to severe AP (41% vs. 24%; P < 0.01). They also had more frequent intensive care unit (ICU) admission (20% vs. 6%; P < 0.001), longer hospital stay (10 vs. 6 days; P < 0.001) and higher mortality (3% vs. 0.2%; P < 0.001).
Demographic characteristics and clinical outcomes of patients according to tolerance of oral diet.
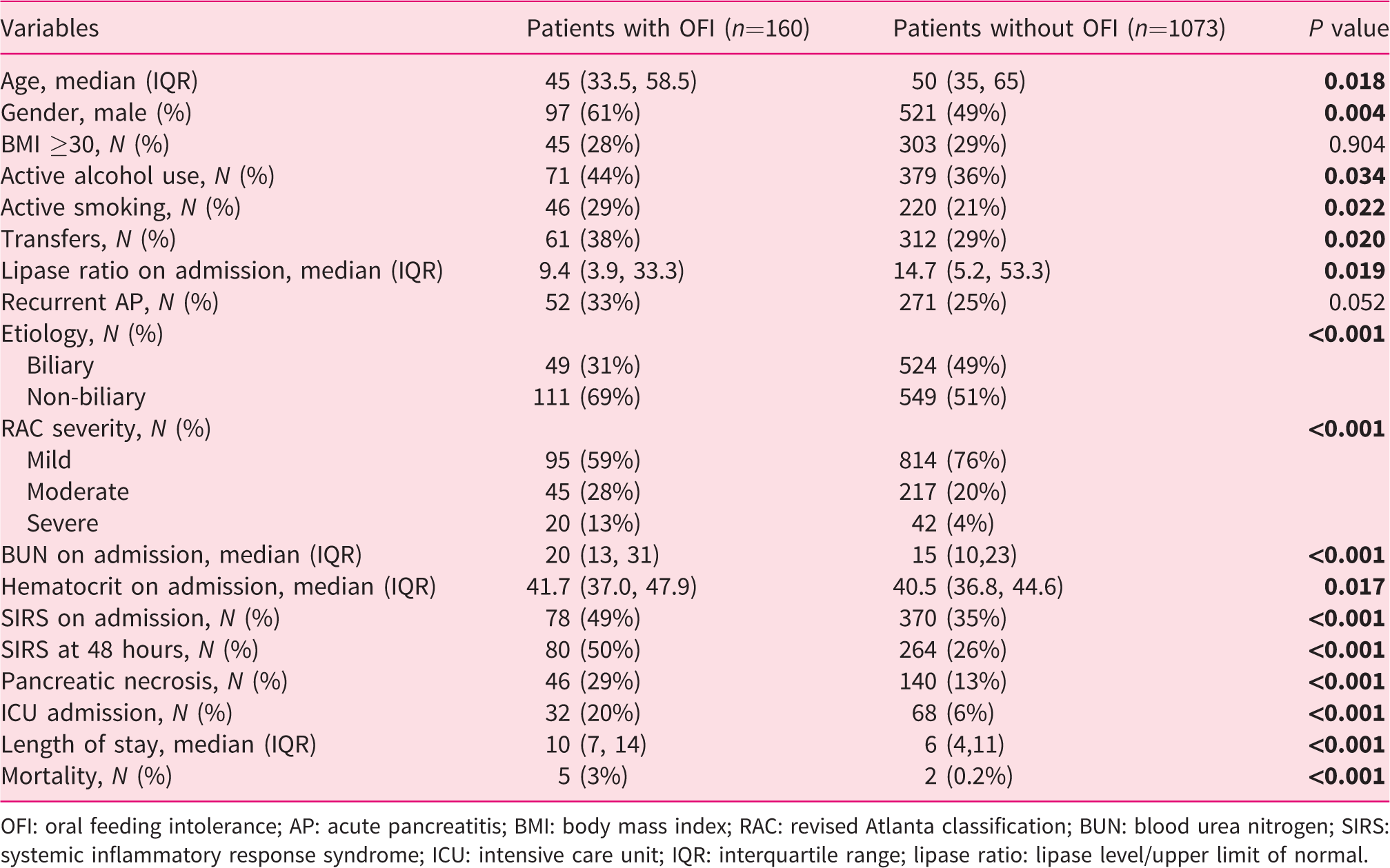
OFI: oral feeding intolerance; AP: acute pancreatitis; BMI: body mass index; RAC: revised Atlanta classification; BUN: blood urea nitrogen; SIRS: systemic inflammatory response syndrome; ICU: intensive care unit; IQR: interquartile range; lipase ratio: lipase level/upper limit of normal.
With respect to the timing of the initial feeding attempt, 291 (23.6%) patients started an oral diet on the day of admission (day 1) or day 2, 342 (27.7%) patients on day 3, 232 (18.8%) patients on day 4, 158 (12.8%) patients on day , and 206 (16.7%) patients on day 6 or later. Data were missing for the exact timing of the initial feeding attempt for four (0.03%) patients (Table 2). The rate of OFI was similar regardless of the day of the initial feeding attempt (P = 0.41). The timing of feeding was different between continents, being earliest in North America (2 days, IQR 1–3), followed by Europe (2 days, IQR 2–4), Central/Latin America (3 days, IQR 2–4) and India (3 days, IQR 2–4) (P < 0.001).
Timing of first feeding in the oral feeding group.
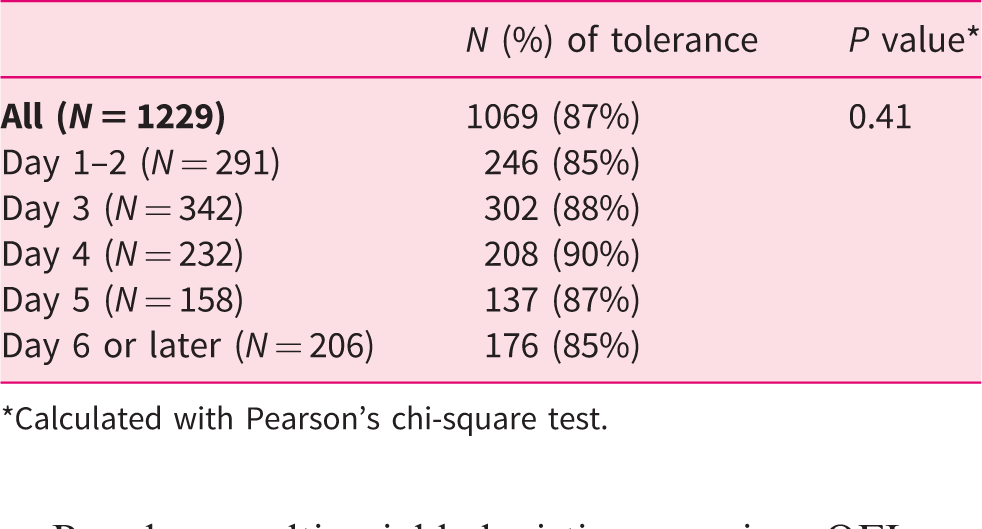
*Calculated with Pearson’s chi-square test.
Based on multivariable logistic regression, OFI was found to be independently associated with non-biliary etiologies (odds ratio (OR) 1.65, 95% confidence interval (CI) 1.01–2.7; P = 0.046) and SIRS at 48 hours (OR 3.1, 95% CI 1.8–5.2; P < 0.01) (Table 3).
Multivariable logistic regression analysis to determine factors independently associated with oral feeding intolerance.
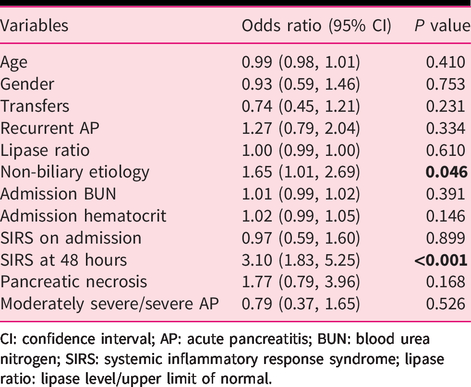
CI: confidence interval; AP: acute pancreatitis; BUN: blood urea nitrogen; SIRS: systemic inflammatory response syndrome; lipase ratio: lipase level/upper limit of normal.
The predictive model including probabilities of all 200 randomly split training set runs revealed an area under the curve (AUC) of 0.663 (95% CI 0.61–0.71) (Figure 2).
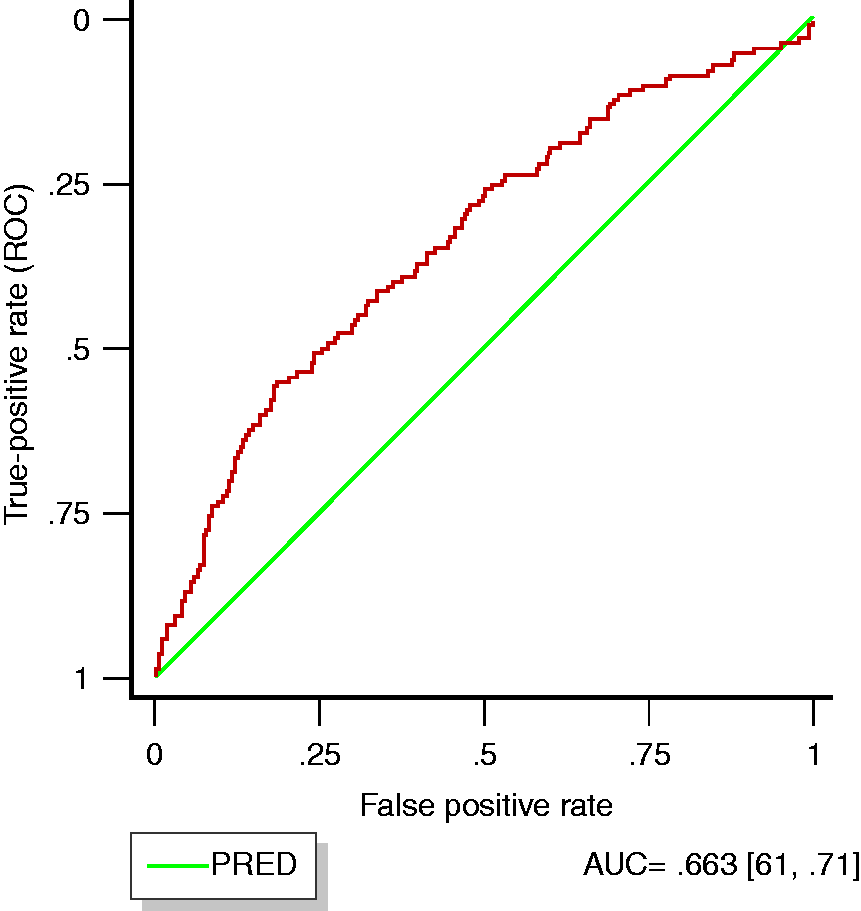
Receiver operating characteristic curve for model predicting oral feeding intolerance in patients with acute pancreatitis.
Finally, we performed a comparative analysis with respect to the initial feeding route (Table 4). The group having an initial non-oral (enteral or parenteral) route was younger (47 vs. 49 years; P = 0.045) predominantly men (67% vs. 50%; P < 0.001), with more frequent alcohol (47% vs. 37%; P = 0.006) and smoking use (30% vs. 22%; P = 0.008) compared to patients who were fed orally at the beginning. The non-oral group was more likely to be transferred from an outside hospital (62% vs. 30%; P < 0.001), had increased BUN (24 vs. 15.1 mg/dL; P < 0.001) and hematocrit levels (42.6% vs. 40.6%; P < 0.001) on admission. Patients fed initially through either the enteral or parenteral routes were more likely to have moderate/severe AP (81% vs. 26%; P < 0.001), more frequently had SIRS-positive status on admission (69% vs. 36%; P < 0.001) and at 48 hours (79% vs. 29%; P < 0.001). They required ICU care more often (70% vs. 8%; P < 0.001), had a longer hospital stay (16 vs. 7 days; P < 0.001) and an increased mortality rate (12% vs. 0.6%; P < 0.001).
Comparison between subjects with initial oral versus non-oral feeding attempt.
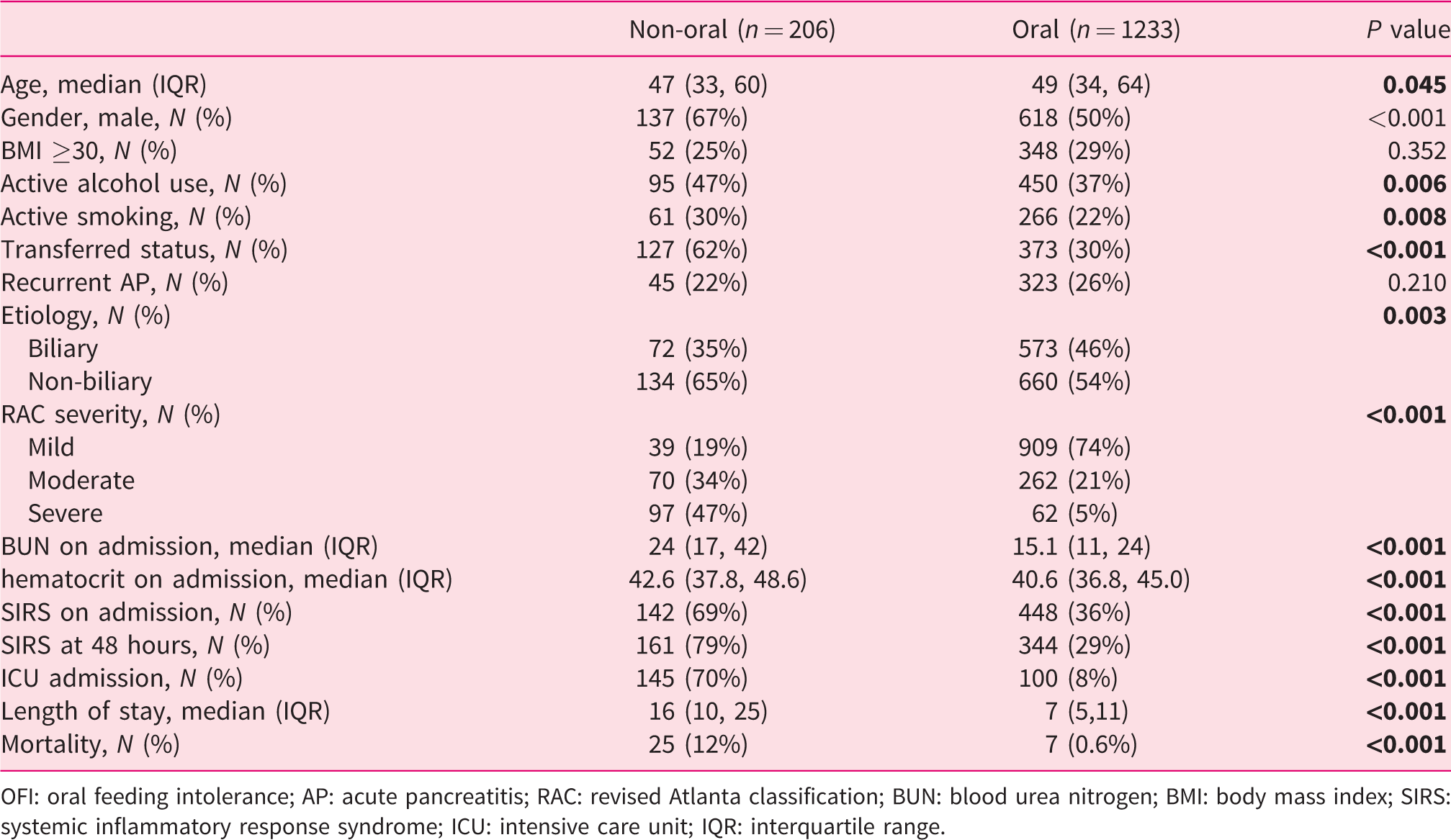
OFI: oral feeding intolerance; AP: acute pancreatitis; RAC: revised Atlanta classification; BUN: blood urea nitrogen; BMI: body mass index; SIRS: systemic inflammatory response syndrome; ICU: intensive care unit; IQR: interquartile range.
Discussion
To our knowledge, this is the largest, international, prospective, cohort study to assess the incidence, clinical predictors and outcomes of OFI in patients with AP. We found that OFI developed in 13% of our cohort. Younger, male patients, and those with active smoking and alcohol use were more likely to develop OFI. Hemoconcentration and elevated BUN at admission are potential predictors of OFI. Non-biliary etiology and SIRS at 48 hours after admission were independent risk factors for OFI. The timing of the initiation of an oral diet does not appear to be associated with the development of OFI. OFI was associated with worse clinical outcomes including longer hospital length of stay.
The incidence of OFI was 13% in our study, with the previously reported rates varying between 8% and 25%.1–3,11 Bevan et al. reported an overall incidence of OFI at 16% in a meta-analysis including centers from multiple continents. 18 Our data are therefore comparable to contemporary literature on this subject. Overall, it appears that the rates of OFI in AP have not improved over the years. This could be due to poor recognition of high-risk patients for OFI and a lack of personalized refeeding protocols in patients with AP.
The optimal timing to start refeeding remains a challenge in the management of AP patients. In our analysis no significant difference was noted with respect to the incidence of OFI based on the day of the initial oral refeeding attempt. The day of initiation of an oral diet was based on the treating physician’s judgement, according to the subject’s symptomatology and clinical course. The continental difference in the timing of oral feeding initiation in our cohort can be partially explained by variations in the severity of AP among different geographical areas, as it was reported from a previous study of our consortium. 16 Typically, AP patients are initially kept NPO (nil per os), and diet is resumed with clinical improvement. It has been suggested that feeding stimulates the release of cholecystokinin, which causes the secretion of proteolytic enzymes that lead to autodigestion and as a result further damage of the pancreas. 19 Several randomized controlled trials have sought to determine the optimal timing of initiating an oral diet with mixed results.8–10,12–14 Recent data suggest that early oral refeeding in mild AP has no difference in terms of OFI clinical outcomes or incidence compared to delayed feeding.10,12,14 Based on these data, it appears that OFI depends on unique patient and disease-related factors and is not entirely a function of the timing of refeeding. Early oral refeeding in patients at low risk of OFI may enable early discharge and reduce the economic impact of AP.
Patients with certain baseline clinical characteristics, including younger age and male gender, were more likely to develop OFI. Other factors associated with OFI include active alcohol use and smoking, probably due to their association with the severity of AP. Multiple studies have reported an association of alcohol consumption with a more severe clinical course of AP.20,21 Alcohol use has also been associated with a higher need for ICU care, infectious complications and mortality.22,23 Even though smoking is a well-known risk factor for chronic pancreatitis, 24 it has been difficult to examine its association with OFI in AP, because tobacco use is closely related to alcohol consumption, 24 and it has been challenging to control for confounding secondary to alcohol use. 25
Biliary etiology was found to be associated with a reduced rate of OFI in our study. Non-biliary causes included alcohol, hypertriglyceridemia and idiopathic causes. Both alcoholic and hypertriglyceridemia-induced causes are associated with a more complicated course of AP compared to other etiologies.26,27 Our findings suggest adopting a cautious approach with oral refeeding in patients with alcoholic, hypertriglyceridemia and idiopathic etiology.
Laboratory parameters such as BUN and hematocrit on admission were elevated in the OFI group. These markers are also associated with disease severity.28–32 Elevated BUN is associated with increased mortality,31,32 while hemoconcentration can predict pancreatic necrosis and organ failure.28,29 These conventional laboratory markers provide information about the intravascular volume status of patients, and changes in their values can reflect patient’s response to fluid resuscitation.
Pancreatic necrosis was also noted to be associated with OFI in the univariate analysis. Patients with elevated BUN and hematocrit on admission,29,30 as well as significant alcohol use20,21 are at risk of pancreatic necrosis. After controlling for these confounding factors in multivariable analysis, a trend was noted showing an independent correlation of pancreatic necrosis with OFI, which did not reach statistical significance (P = 0.06).
In terms of clinical outcomes, we found that patients with OFI had a more severe clinical course, with longer hospital stay and requirement for ICU management. These patients frequently have SIRS on admission and at 48 hours. The latter was identified as an independent risk factor for OFI in the multivariable regression analysis. Singh et al. showed that positive SIRS on admission is associated with a severe clinical course. 33 Other studies proposed that SIRS at 48 hours is associated with organ dysfunction and increased mortality.34,35 Our findings suggest that SIRS has the potential to be used in clinical practice to risk stratify patients for OFI.
We found an association of OFI with longer length of stay, which was consistent with previous reports.1,3,4,18 Early recognition, prevention and appropriate management of OFI will likely improve patients’ symptomatology during hospitalization and reduce the economic burden associated with AP. 4 It has been reported that AP patients who are discharged with gastrointestinal symptoms, or without having tolerated solid diet during their stay, are at high risk of early readmission. 5 The tolerance of a solid oral diet could be used to guide physicians in the discharge planning of AP patients.
In order to examine the predictability of OFI, we constructed a statistical model composed of key clinical variables. The results of our model suggest that a clinician has a 66% probability of correctly predicting OFI using the above variables. However, an AUC of 0.663 is only of low to modest predictive accuracy and is unlikely to be adapted in clinical practice.
Finally, patients who received enteral/parenteral nutrition had a similar risk profile as patients who developed OFI. Factors associated with non-oral nutrition included young age, men, active smoking and alcohol, non-biliary etiology, moderate/severe AP based on RAC, elevated BUN/hemoconcentration at admission, SIRS at admission and 48 hours. A more proactive approach at the initiation of enteral nutrition is likely to be warranted after stabilization of hemodynamics and fluid resuscitation in patients with a predicted moderate or severe course of AP.
This study had several limitations. Given that this is an observational study, no causal association can be established with regard to potential risk factors of OFI. Also, most of the participating centers of the study are academic tertiary centers. Therefore, the results might not be generalizable. The strengths of this study derive from the fact that this is the first international study to examine clinical predictors of OFI. A diverse population of AP patients was prospectively enrolled and carefully phenotyped from multiple leading pancreatic centers around the globe. The questionnaires were standardized, and data were monitored and analyzed centrally at the coordinating site.
In conclusion, our study confirmed that OFI is relatively common and is associated with worse clinical outcomes in AP. Young age, male gender, alcohol use, smoking, elevated BUN and hemoconcentration are potential predictors of OFI. The non-biliary etiology of AP and SIRS at 48 hours may serve as important prognostic factors in stratifying patients at risk of OFI. Detecting patients with these clinical features should rationalize a more cautious approach by the treating physicians with their refeeding strategy. Additional research in the form of randomized clinical trials is needed to determine the optimal timing and consistency of suggested diets in patients with AP stratified by clinical risks and laboratory predictors of OFI.
Footnotes
Declaration of conflicting interests
The author(s) declare that there is no conflict of interest.
Ethics approval
The study protocol was approved by the Institutional Review Board (IRB) or Ethics Committee at each participating study site (PRO15040389/Approval date: 07/14/2015).
Funding
No funding was required for this study.
Informed consent
Written, informed consent was obtained from all subjects.