
Abstract
Background
Esophageal food impaction is relatively common and increasing over time. Treatment ranges from medications to invasive endoscopic therapies. The endoscopic push technique has been advised against in favor of endoscopic retrieval for safety concerns. We sought to assess use patterns and safety of treatments for food impaction in a population-based retrospective review.
Methods
A database of recorded esophageal food impactions in Olmsted County, MN, USA, from 1975–2011 was reviewed for patient demographics, treatment, and complications.
Results
A total of 645 impactions occurred, with increasing incidence over time, peaking at 23.2 per year (2000–2004). Medications (almost exclusively glucagon) were successful in relieving impactions 34.5% of the time when trialed. Urgent endoscopy was common (74.0%), as was the need for endoscopic therapy (67.1%). Endoscopic therapy increased over time, with the endoscopic push technique becoming most common. Esophageal complications (deep mucosal injury or perforation) increased over time but remained rare (peak 11%). There was no difference in complications between push and retrieval techniques.
Conclusions
The endoscopic push technique is safe in comparison to endoscopic retrieval in esophageal food impactions. While complications surrounding impaction have increased, they remain rare. Medication trials are reasonable, as long as they do not delay endoscopy, and may prevent the need for emergent endoscopy in one-third of cases.
Keywords
Key points
Esophageal food impaction incidence has been increasing over time with the emergence of eosinophilic esophagitis. Historically, it has been recommended to avoid the esophagogastroduodenoscopy (EGD) push technique in endoscopic management of esophageal food impactions in favor of EGD retrieval given concerns about increased complication risk. Glucagon appears to be a reasonable attempted therapy and may lead to resolution of food impaction in about one-third of patients. The EGD push technique appears to be a safe and effective management approach in comparison to EGD retrieval, and overall risk of complications is rare.
Introduction
Esophageal food impaction is a relatively common acute and urgent gastroenterological issue with an annual incidence of about 13 episodes per 100,000 individuals.1,2 More recent studies suggest that it is increasing in incidence over time. 3 An underlying esophageal cause leading to food impaction is commonly found, with structural abnormalities (historically, Schatzki ring, peptic stricture) most likely, and dysmotility disorders and malignancy being less common causes.3,4 Several recent studies have documented the increasing association of eosinophilic esophagitis (EoE) with food impaction, noting that EoE is the most common cause of impaction in specific and perhaps the general population. Moreover, food impaction related to EoE is likely associated with a higher rate of complications.2,3,5,6
There are multiple treatment methods for esophageal food impaction, including ingestion of carbonated beverages, medications that affect esophageal motility (glucagon and nitrates most commonly), and endoscopic or surgical removal of the food bolus.7–12 Spontaneous resolution has been reported in up to 25% of food impaction patients. Medications have been effective in nearly 40% and endoscopy in more than 95% of patients.7–11 Historically, removal of the food impaction by retrieval and retrograde removal by mouth has been recommended because of concern that pushing the bolus into the stomach may lead to complications in the setting of luminal narrowing. However, the push technique is likely used frequently in practice, and a recent study has suggested the technique is safe and effective. 11 In light of the increasing frequency of EoE-related impactions and the possible increased rate of complications with EoE impactions, we reviewed the nonendoscopic and endoscopic management of food impaction in the fixed population of Olmsted County, MN, over a 36-year period to detect differences in method of management and occurrence of complications related to therapy.
Methods
Patient selection and study design
This study was approved by the Mayo Clinic Rochester Institutional Review Board. The Rochester Epidemiology Project (REP) was developed to create a system for documentation of care provided to patients within Olmsted County, MN, in the major medical centers within the county, Mayo Clinic, and Olmsted Medical Center. This population-based study used the REP database to include all recorded episodes of esophageal food impaction in Olmsted County, MN, in 1975–2011. These were identified via text-based search for diagnosis of esophageal foreign body impaction, foreign body in the esophagus, or foreign body in an orifice. Events were excluded if found to be nonfood items or impactions not involving the esophagus, as well as if symptoms resolved prior to emergency department presentation. Thus, food impaction was defined as the sensation of food lodged in the throat with evidence of esophageal obstruction that necessitated medical assessment and lasted long enough to seek a medical assessment. 13 All impactions in patients older than 18 years at the time of the event were included. Data extraction and review of medical charts were completed by two physician authors (C.J.L. and D.A.S.). Medical charts were reviewed for patient characteristics, treatments directed at relieving the food impaction (observation/spontaneous, medications, carbonated beverage, endoscopic retrieval, and endoscopic push technique), underlying etiology that may have led to impaction (EoE, Schatzki ring, stricture, prior esophageal surgery, prior chest radiation therapy, gastroesophageal reflux disease (GERD), achalasia, neurologic disease/stroke, diffuse esophageal narrowing, or malignancy), and complications surrounding the event (including esophageal perforation, esophageal deep mucosal disruption or “tear,” hospital admission, intubation, and aspiration pneumonia). For nonendoscopic treatment, success was defined as clear clinical resolution of the obstruction (ability to successfully swallow liquids and manage secretions) after therapeutic administration or evidence of a recently passed obstructing food bolus in the stomach on endoscopy completed during acute impaction management. Endoscopic push technique was defined as a food bolus being moved from the esophagus to the stomach with the tip of the endoscope. Diagnosis of deep esophageal mucosal disruption was made by visual evidence of a mucosal break during endoscopy. Perforation was diagnosed by postprocedural imaging (computed tomography scan showing free air or contrast esophagram displaying a leak) in the clinical context of symptoms suggesting the need for such studies. For the diagnosis of periprocedural aspiration pneumonia, those who developed symptoms along with radiologic evidence of pneumonia and/or high enough clinical suspicion to be treated with antibiotic therapy within one month of the food impaction event were included.
Statistical analysis
Statistical analysis was performed using JMP, version 13 Pro (SAS Institute Inc, Cary, NC, 1989–2007). Data were reported as means and population percentages with standard error. Comparisons between patient groups were made using Pearson chi-squared or Fisher exact tests for categorical and Mann–Whitney test for continuous variables.
Results
Study population characteristics
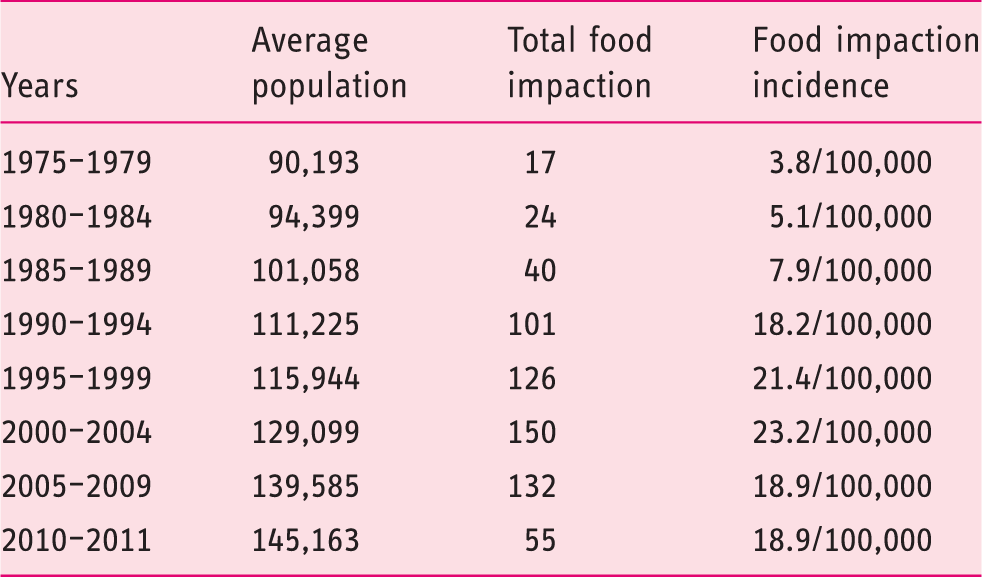
In our population, 645 esophageal food impactions were documented between 1975 and 2011. These impactions occurred in 480 patients, giving an average of 1.3 impactions per individual (range, 1–19, SD = 1.28). The population was predominantly male (61.6%) and the average age at the time of impaction was 58.4 ± 21.1 years. Average age at time of first impaction was 57.0 ± 20.8 years. This remained stable throughout the study (54.6–62.5 years). The male predominance in the study population was relatively constant over time (50.0%–72.5%). The vast majority of food impactions were with meat (84.2%). The yearly incidence of food impaction was 3.8 per 100,000 in 1975–1979, with a large increase in 1990–1994 to 18.2 per 100,000, peaking at 23.2 per 100,000 in 2000–2004, and with a slight decrease but remaining stable since that time (18.9 per 100,000 in 2005–2011) (Figure 1; Table 1).
Incidence of food impaction over time. Food impactions in the study population over time.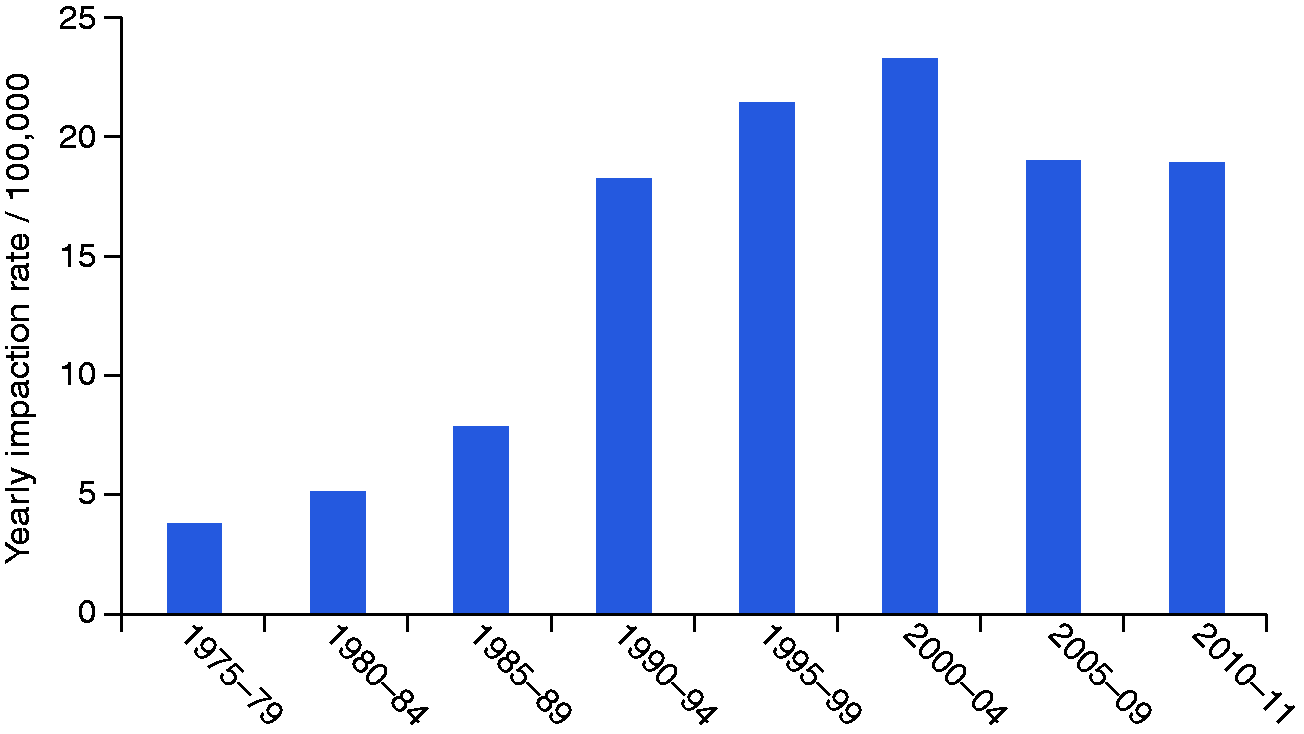
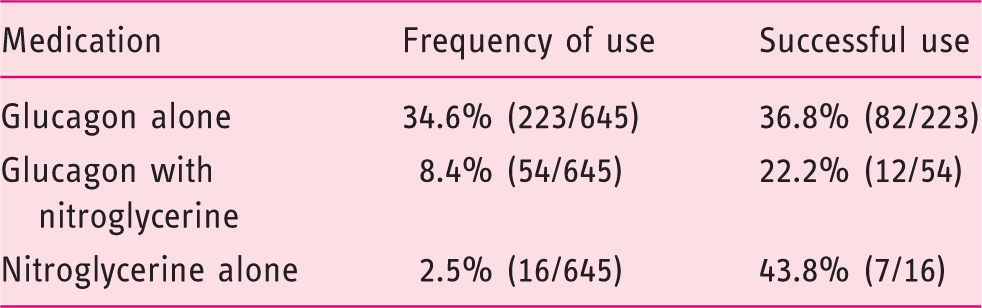
Medication use in acute food impaction management.
Underlying conditions in patients with acute food impaction.
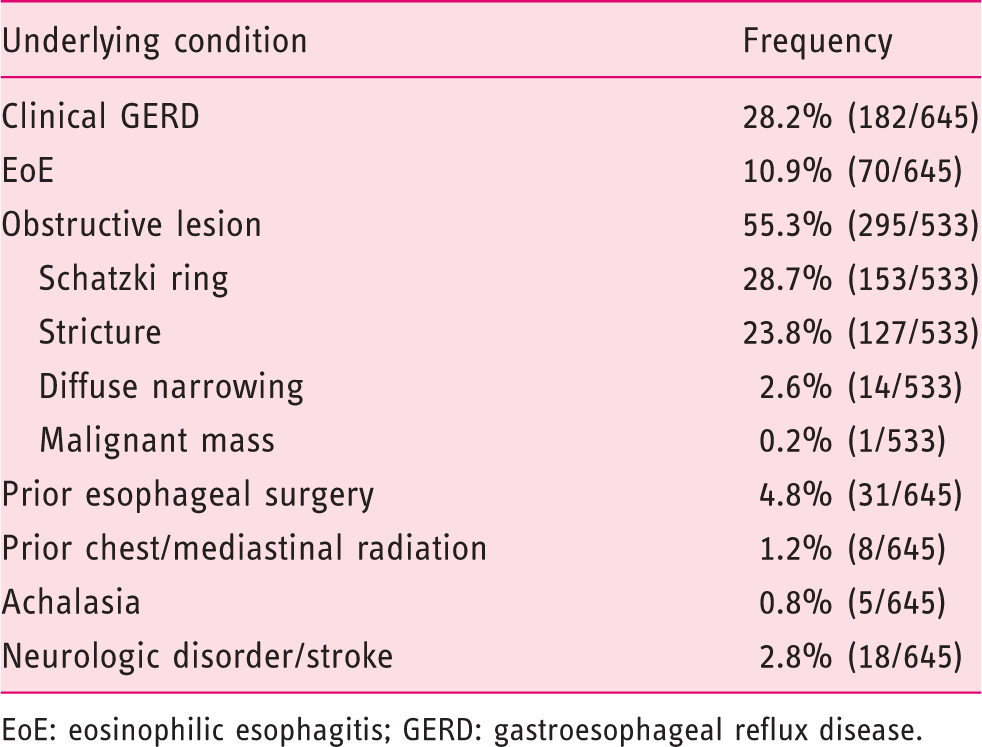
EoE: eosinophilic esophagitis; GERD: gastroesophageal reflux disease.
Histologic assessment of the esophagus via biopsy was unfortunately not performed in a significant number of patients. Biopsies were obtained surrounding 19.5% (104/533) of total food impaction events, which included an EGD for therapy/work-up and 33.3% (25/75) of food impactions that occurred after 2006 that had EGD completed.
Complications surrounding food impaction were rare, with esophageal deep mucosal disruption occurring on 37 occasions (5.7%) and only one esophageal perforation (0.2%). Hospital admission was also rare (39 episodes, 6.1%), and in only nine episodes (1.4%) did patients require intensive care unit admission. Intubation surrounding endoscopic therapy or during hospitalization after the event was also rare, with this required on only 15 occasions (2.3%), with six performed prophylactically for airway protection, eight for procedural agitation, and only one in the postprocedure setting in light of respiratory complications. Aspiration pneumonia was also rare with only six occurrences (0.9%). While all these complications were rare in this population, outside of esophageal perforation, the frequency of all complications increased over time (Figure 2).
Complications over time.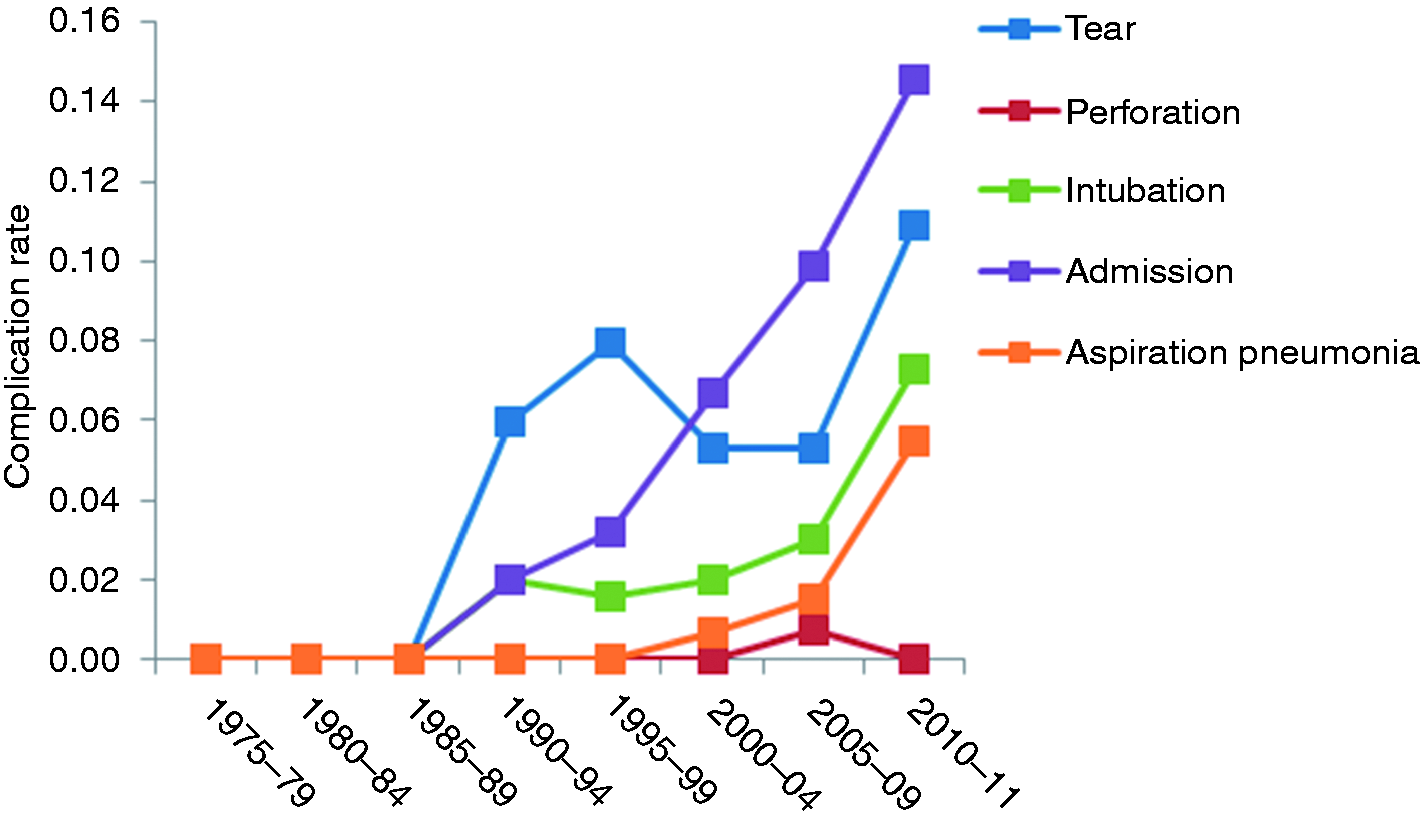
Treatment over time
The frequency at which treatments for esophageal food impaction were used between the time of emergency department presentation and resolution or endoscopy over time was not constant. Spontaneous resolution was initially common (58.8% in 1975–1979) but trended toward uncommon (11.4%–12.7% in 2005–2011). Endoscopic treatment was initially required in only 35.3% of cases in 1975–1979 but quickly trended up to 74.3% in 1990–1994 and remained common and stable since that time (60.0%–70.0% in 1995–2011). EGD retrieval has become less common, as it was initially used 35.3%–50.0% of the time in 1975–1984 but trended down to 18.2%–18.9% in 2005–2011, while the EGD push technique has become much more commonly used, going from no use in 1975–1984 to 41.8%–43.7% in 1995–2011. Successful clearance via medications has been more stable over time with some uptrend recently, going from 5.8%–12.5% use in 1975–1984 to 21.8%–24.3% in 2005–2011 (Figure 3).
Successful impaction treatment over time.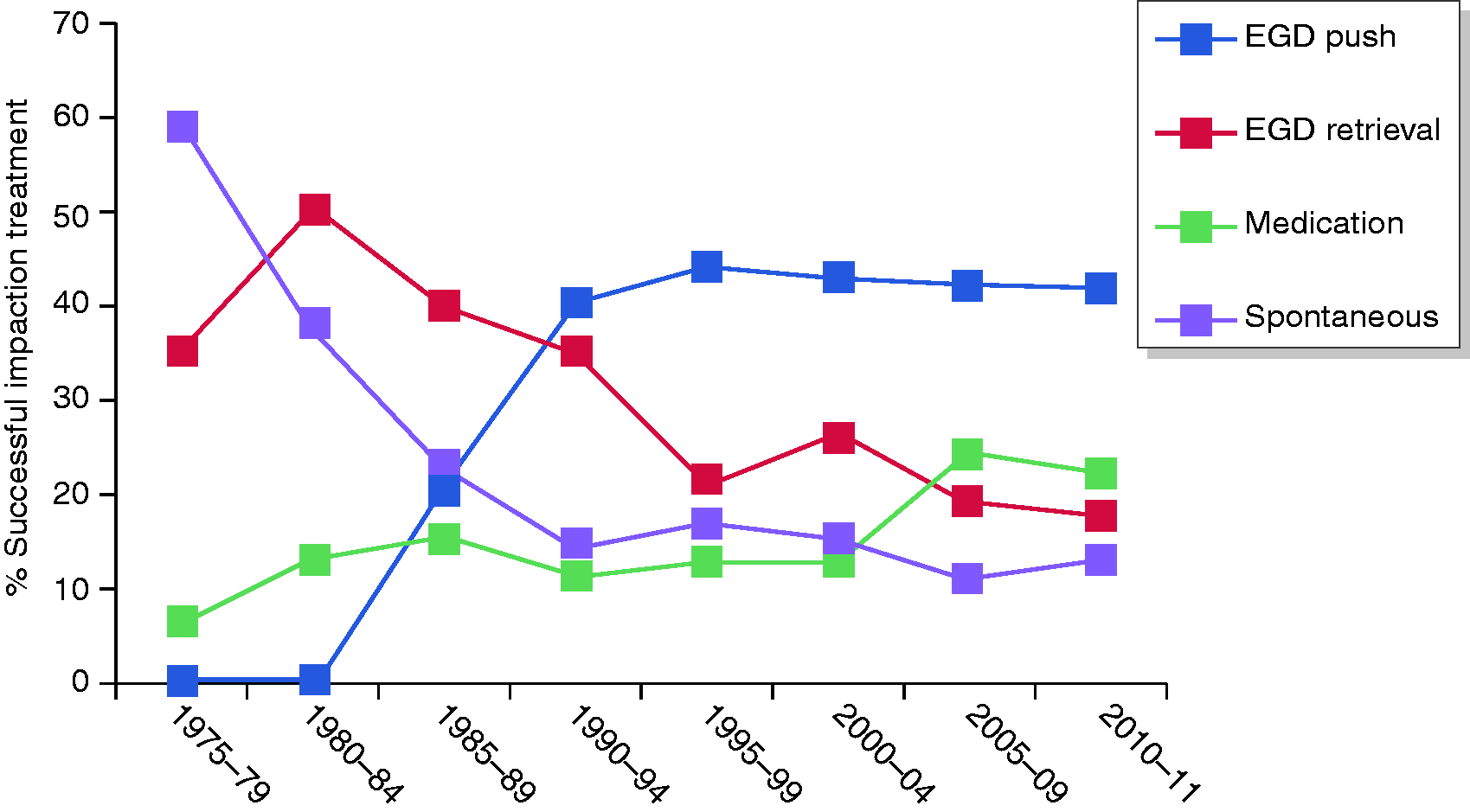
Etiology over time
The underlying esophageal pathology related to development of food impaction has changed over time. Eosinophilic esophagitis has become much more common, with no reported cases related to food impaction in 1975–1984, but seen in 21.8%–22.7% in 2005–2011. A relatively large proportion of cases were without clear underlying etiology initially (52.5%–70.6% in 1975–1989), which has become less frequent but is still relatively common (23.7%–38.2% in 1990–2011). Other underlying etiologies varied somewhat more sporadically over the time of the study (Figure 4).
Etiology of impaction over time.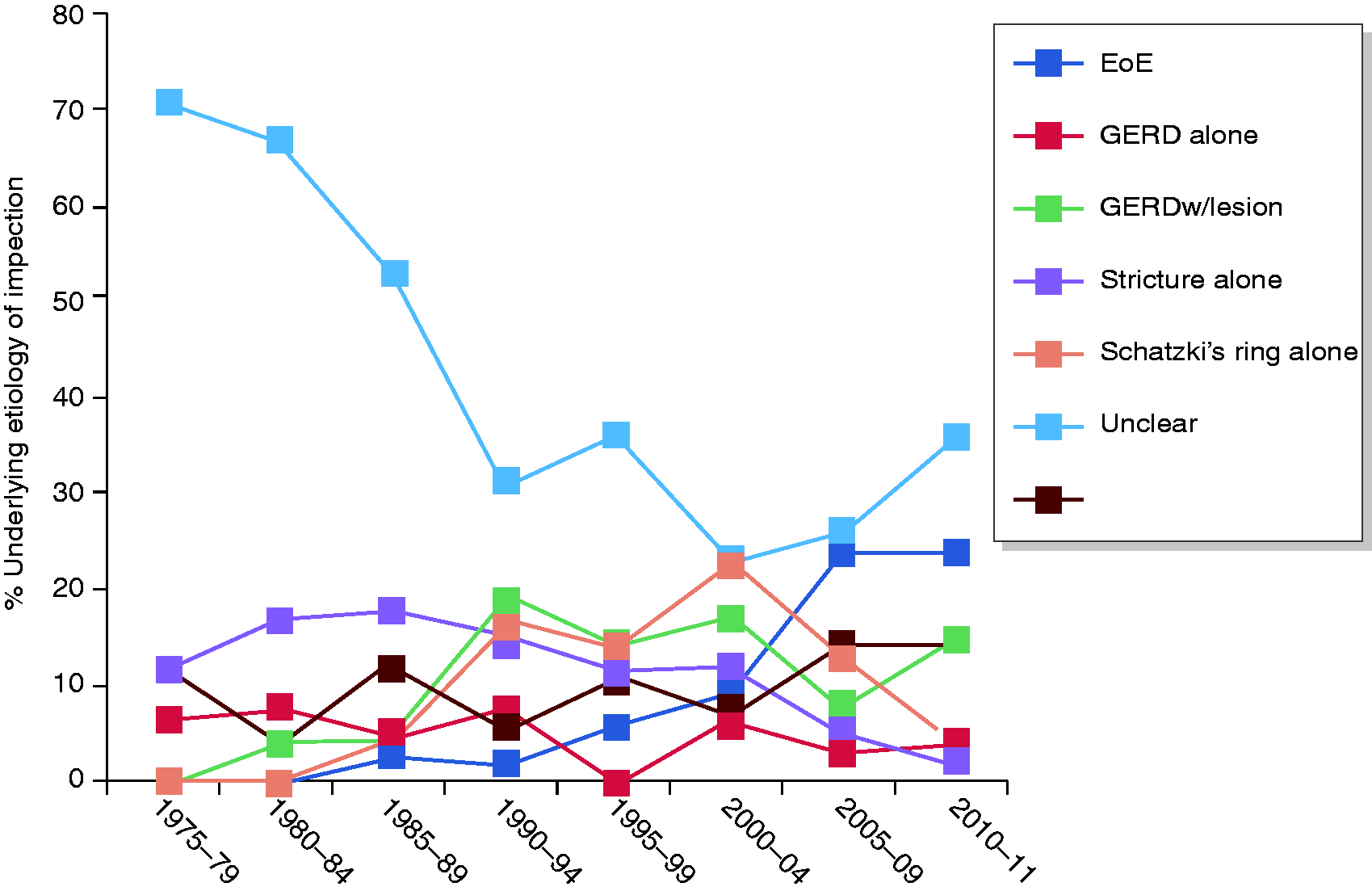
Complications by etiology
Complications by etiology over time are displayed in Figure 5. Numerically, the complication rate for EoE appears higher than for other food impaction etiologies. There were no significant differences in the frequency of hospital admission, need for intubation, or aspiration pneumonia when comparing this between groups based on underlying contributing etiology to the food impaction.
Esophageal complications by etiology over time.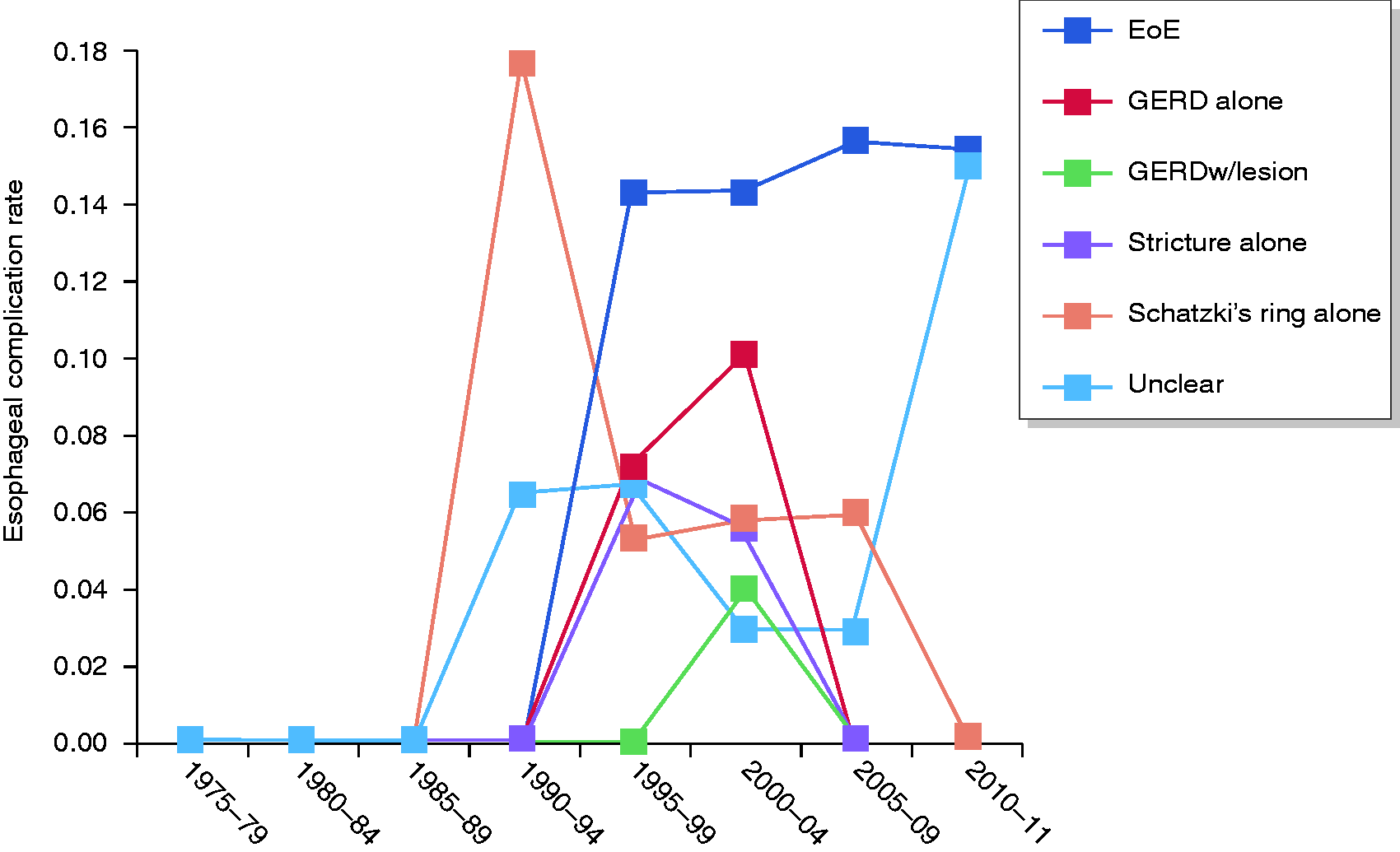
When compared with those without the diagnosis of EoE, patients with EoE did differ in that they were younger (38.2 vs 59.3 years, p < 0.0001) and were more likely to have trialed medication as a therapeutic option for their food impaction (61.2% vs 43.6%, p = 0.006). Despite the increased medication use, they were not more likely to have resolution of the impaction via this route (20.9% vs 15.1%, p = 0.2). Notably, there was a significant difference in the rate of esophageal mucosal disruption in those with EoE (14.9% vs 4.7%, p = 0.003). There were no esophageal perforations occurring in patients with EoE, with there being no significant difference when comparing this to those without EoE (0.0% vs 0.2%, p = 1.0). There were also no significant differences between the EoE group and others when looking at aspiration pneumonia (0.0% vs 1.8%, p = 0.6), periprocedural intubation (5.5% vs 3.6%, p = 0.5), or hospital admission (9.1% vs 9.7%, p = 1.0).
Complications by treatment
There was no difference found between the rate of esophageal complications when comparing endoscopic food bolus retrieval and the endoscopic push technique, with there being deep esophageal mucosal disruption in 7.0% and 9.8%, respectively (p = 0.4), and esophageal perforation in 0.0% and 0.4%, respectively (p = 0.5). The rates of admission (13.1% vs 9.6%, p = 0.4 and aspiration pneumonia (1.0% vs 1.1%, p = 1.0) were also similar when comparing the retrieval vs push techniques. Intubation was more common (9.1% vs 3.2%) in those undergoing endoscopic retrieval compared with the push technique, although when intubation was separated into preprocedural/periprocedural and postprocedural (a true complication), the intubation rate was similar (1.0% vs 0.0%). After an initial period without any esophageal complications in 1975–1989, the rate of esophageal complications with EGD retrieval has been relatively stable over time, between 4.0% and 11.4% since. Similarly, complications were initially rare with the EGD push technique, 0.0%–5.0% in 1985–1994 (it was not used in our population prior to 1985), with a recent uptrend to 10.9%–21.7% in 2005–2011 (Figure 6).
Esophageal complications by type of endoscopic therapy over time.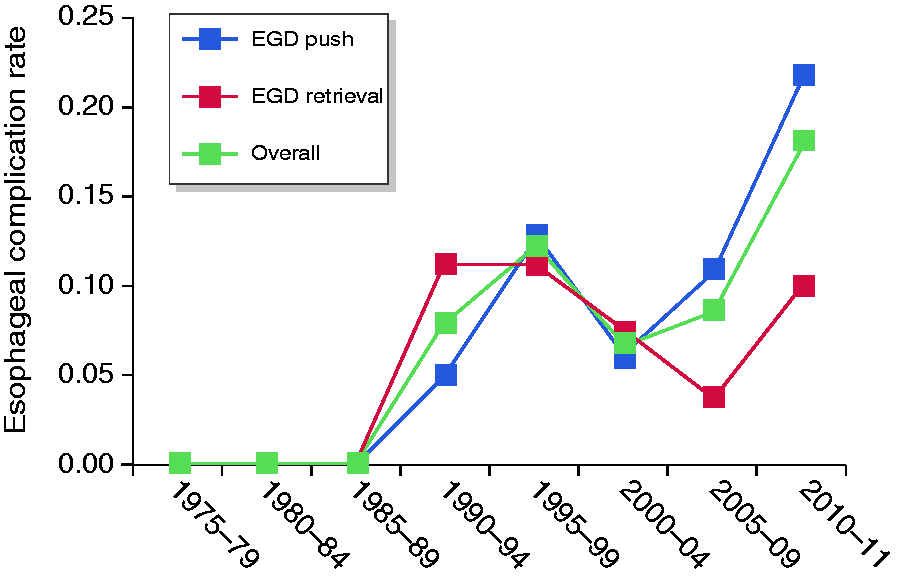
Discussion
This population-based study demonstrates confirmation of the increase in the incidence of esophageal food impaction over the course of time that has been suggested in prior studies, 3 but may also suggest a plateauing in the incidence more recently. These data have been published in detail by our group. 13 This significant rise in the incidence of food impaction comes with what has been noted in prior studies of increasing incidence of EoE.2,3,5,6
The study also gives us several insights into the evolving management of esophageal food impaction. First, glucagon therapy is effective in about one-third of patients. In a recent web-based survey of gastroenterology practice by Hiremath et al., 52% of responding gastroenterologists used smooth-muscle relaxants (glucagon) in the management of food impaction. 14 As there were no complications reported in our experience, glucagon treatment seems to be a reasonable emergency department practice as the first step in the treatment for food impaction. The use of glucagon without delaying EGD is also supported by the American Society for Gastrointestinal Endoscopy (ASGE) and European Society of Gastrointestinal Endoscopy (ESGE).4,16 Other medications were too rarely used to make significant recommendations regarding standard use.
The endoscopic push technique appears to be used more commonly than the retrieval technique and is safe and effective in relieving food bolus impaction. This is consistent with the data presented by Vicari and colleagues suggesting efficacy (97%) and safety (no adverse events) in a smaller population of patients who had the push technique performed to relieve their food impaction. 11 Seventy-four percent of our patients required endoscopic bolus removal, and the push technique became more common than retrieval in our practice around 1990. The complication rate was similar between the retrieval and push techniques. Of note, intubation was more common in the retrieval patients. While intubation itself may not necessarily be a marker for poorer outcomes, it certainly leads to increased cost and risk for hospitalization and further complications. Historically, the push technique was to be avoided because of fears of perforation, 17 but gentle pushing of the bolus has been advocated by the ASGE and ESGE recently.4, 15,16 While other endoscopic techniques, like rigid endoscopy, can be used in management of food impaction, there was no evidence of use of other types of endoscopic therapy in our population, thus making it impossible to clarify their safety or efficacy. 18
EoE has increasingly been associated with food impaction. Biopsy is necessary to make the diagnosis of EoE and is important to obtain even in those with normal-appearing mucosa as 16%–33% of EoE patients will have a normal-appearing esophageal mucosa.19,20 Unfortunately, esophageal biopsies for EoE are not being routinely performed in patients with food impaction in our population. This has been the case even after the 2007 EoE consensus statement, with the occurrence of obtaining biopsies during EGD surrounding food impaction increasing only from 19.5% to 33.3%. Albeit somewhat lower in our population, this is consistent with the recent findings of Hiremath et al., who noted a significant lack of biopsy looking for EoE in patients presenting with acute esophageal food impaction based on a survey of more than 400 practicing gastroenterologists from around the United States (14% not performing biopsy and 51% not performing biopsy with normal-appearing mucosa). 14
Interestingly, the increase in the proportion of food impactions related to EoE may be understated in our study population. Even after 2006 there were a significant number of impactions in our population that were without clear underlying etiology (30.8%), and 42.3% of these patients did not undergo EGD either emergently or within a reasonable time after the food impaction. On top of this, in those who did have EGD completed in this group, biopsies to assess for EoE were not uniformly performed. We agree with the assessment by Hiremath and colleagues that there appears to be a missed opportunity here for diagnosing underlying conditions that may be amenable to treatment to help prevent future impactions.
There are several study limitations that need to be recognized. The major limitations of our study are inherent to the retrospective nature of the study. The quality of the data for all the patients in this study is limited to the quality of the medical record. Additionally, given the relatively recent discovery of EoE, it is quite possible that findings such as rings and furrows on EGD or pathologic specimens showing eosinophils may have been ignored and not mentioned in the record in earlier time periods. 5 The population of Olmsted County, MN, is predominantly Caucasian (particularly in the earlier years in the study), and while not that dissimilar from overall demographics in the United States, information obtained from this study may not hold true for all populations, particularly those with significant differences in demographics.
Despite its limitations, this long-term population-based study offers a significant contribution to the data regarding the treatment and complications surrounding esophageal food impaction. The large study comes from a fixed population and was performed predominantly but not exclusively at a medical center with considerable expertise in esophageal disease and particularly EoE over a 36-year period.
From our population, it appears that treatment of food impaction is associated with relatively low rates of esophageal complications as well as need for hospitalization, intubation, and development of aspiration pneumonia. Moreover, we feel that these data are suggestive of safety of the EGD push technique and that the recommendation to avoid this practice may not only be overly conservative but may in fact suggest avoidance of a necessary and effective therapeutic option. Certainly, obtaining data from multiple centers to increase the diversity of patients and treating physicians would go further to validate these findings and should be the focus of future research to better clarify the safety and effectiveness of all treatments for food impaction. It is hoped this would lead to the ability to create stronger clinical guidelines on therapy and work-up in the setting of acute food impaction that may help to avoid missed opportunities for diagnosing and treating the underlying cause of these events.
Footnotes
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
This study was funded by Mayo Clinic with a grant from the Department of Gastroenterology. There was no other outside funding obtained.
Ethics approval
This study was approved by the Mayo Clinic Rochester Institutional Review Board.
Informed consent
This study was completed as part of the Rochester Epidemiology Project. This was deemed minimal risk the by the Mayo Clinic Rochester IRB and was granted waiver of consent. All patients included in the study were confirmed to have given approval to use their information in research via the Minnesota Research Authorization.