
Abstract
Background
Oesophagoscopy with biopsy is considered the gold standard for diagnosing and monitoring eosinophilic oesophagitis (EoE). Therefore is important to discover less-invasive diagnostic methods.
Methods
Cytology specimens were obtained in patients with active EoE (AEoE) (≥15 eos/hpf) and EoE in remission (EoER) (<15 eos/hpf). The samples were assessed by two independent pathologists and were compared with biopsy samples. EoE cytology specimens were compared with specimens obtained from patients with GERD.
Results
Specimens of 36 patients (69.4% male, mean age 30.88 years) were included. AEoE (17, 47.2%), EoER (11, 30.5%) and GERD (22.2%). eos/hpf in cytology (AEoE 9.23 vs. EoER 1.54 vs. GERD 2, p = 0.01). Linear correlation between eos/hpf average biopsy and cytology eos/hpf: r = 0.57, p < 0.001. For diagnosis of EoE ≥3 eos/hpf in cytology obtained a sensitivity of 70%, specificity 81%, PPV 86% and NPV 60% (AUC = 0.81, p = 0.01). For detection of AEoE, ≥3 eos/hpf in LBC obtained a sensitivity of 70%, specificity 82%, PPV 81% and NPV 66% (AUC = 0.87, p = 0.001).
Conclusions
LBC in oesophageal aspirate seems to be effective for the diagnosis and monitoring activity in EoE. These results support the usefulness of non-invasive methods for the diagnosis and monitoring of EoE.
Introduction
Eosinophilic oesophagitis (EoE) is a chronic immune-mediated disease characterised by symptoms of oesophageal dysfunction (dysphagia and food impaction),1,2 which is produced by a Th2-mediated allergic reaction 3 mainly against food antigens. 4 From the histological point of view, an eosinophilic inflammatory reaction occurs predominantly in the upper layers of the oesophageal epithelium. 5
The current consensus guidelines recommend oesophagoscopy with biopsy (at least five samples) as a technique for the diagnosis and monitoring of the disease.1,2,6 Given that the inflammatory infiltrate in the EoE is distributed in a patchy pattern 7 and additionally, the size of a biopsy represents only a minute part of the oesophagus of around 0.002%, 5 biopsies of proximal and distal oesophagus may underestimate the inflammatory activity of the disease. That is why the increase in sensitivity in the diagnosis of EoE runs parallel to the number of biopsies taken, 8 which are not exempt from complications.9,10
Histological remission can be achieved by pharmacological or dietary therapies,2,11 but the latter approach (especially the Six Food Exclusion Diet (SFED)), entails making multiple endoscopies.12,13 This fact represents an increase in risks for patients and costs to the health care system. That is why in recent years non-invasive strategies have been studied that are aimed at monitoring the disease, avoiding performing endoscopy with biopsy. For this purpose, serological parameters of eosinophil activity were analysed which demonstrated the limited usefulness of these for monitoring disease. 14 One approach that has recently been shown effective as a semi-invasive method is the determination of eosinophil granule proteins in oesophageal intraluminal secretions obtained using a device designed for the study of Helicobacter pylori and intestinal bacterial flora (oesophageal string test). 15 However, this strategy, although attractive, has several drawbacks such as laborious sample processing, which brings difficulty to carry out the analysis in non-tertiary centres and discomfort for the patient who, after swallowing the string-capsule, must keep it overnight for subsequent extraction. One possible strategy is diagnostic cytology of the oesophagus using the Cytosponge, which has proven to be useful in the monitoring of Barrett’s oesophagus, 16 being a cost-effective screening approach for oesophageal cancer. 17 And also, its applicability in the diagnosis and management of EoE has been successfully tested in a small series of patients. 18
The main objective of the study was to analyse the usefulness of liquid-based cytology (LBC) samples obtained in oesophageal aspirates for diagnosis and monitoring of inflammatory activity in EoE. A secondary objective proposed is to study the differences and similarities between the LBC of the oesophagus in EoE and gastroesophageal reflux disease (GERD).
Methods
Population and study design
This was a prospective pilot study conducted at Hospital General Universitario Ciudad Real from April to December 2013. Consecutive naïve and under dietary treatment adult EoE patients were recruited. A diagnosis of EoE was given in accordance to current guidelines (symptoms of oesophageal dysfunction, oesophageal eosinophilia ≥15 eosinophils per high-power field (eos/hpf) and unresponsiveness to proton pump inhibitor (PPI) therapy.1,6 Patients with ≥15 eos/hpf and <15 eos/hpf were classified as active EoE (AEoE) and EoE in remission (EoER). In the same period a subset of adult patients with symptoms typical of GERD endoscopic lesions who were withdrawn from the treatment with PPI at least two weeks before endoscopy is included. No healthy control group was included as absence of eosinophils in the unchanged oesophagus cytology had been previously demonstrated. 19
All patients included in the study underwent oesophagoscopy with biopsy and at the same time collection of oesophageal aspirate.
Endoscopic assessment
All endoscopic procedures were performed under conscious sedation with propofol controlled by the anaesthetist. An adult gastroscope was used with a 9.2 mm gauge and working channel of 2.8 mm (Olympus GIF-Q165, Germany). Four biopsies were taken from the proximal third and another four from the distal third using a clamp Radial Jaw 4™ (Boston Scientific, Costa Rica). The endoscopic findings of EoE patients were assessed according to the EoE Endoscopic Reference Score (EREFS) system 20 and classified by phenotypes: inflammatory (furrows, oedema, exudates) (IP), stenotic (pseudorings, stenosis) (SP), mixed (IP + SP) (MP).
Oesophageal aspirate technique
For extracting LBC a bronchioalveolar lavage device was used (Mocstrap, Covidiem™, Spain) adapted to the gastroscope suction system (Figure 1). Before performing the biopsies, an oesophageal aspirate was performed: First, the endoscopist placed the tip of the endoscope 20 cm from the dental arch and then 50 cc of saline was instilled toward to the esophageal wall. A few seconds later the liquid contained inside the oesophageal lumen was aspirated, and collected in a flask with 20 cc capacity.
Oesophageal aspiration device (Mocstrap, Covidiem™) adapted to the extraction system of a 9.2 mm gauge gastroscope (GIF-Q165, Olympus, Germany).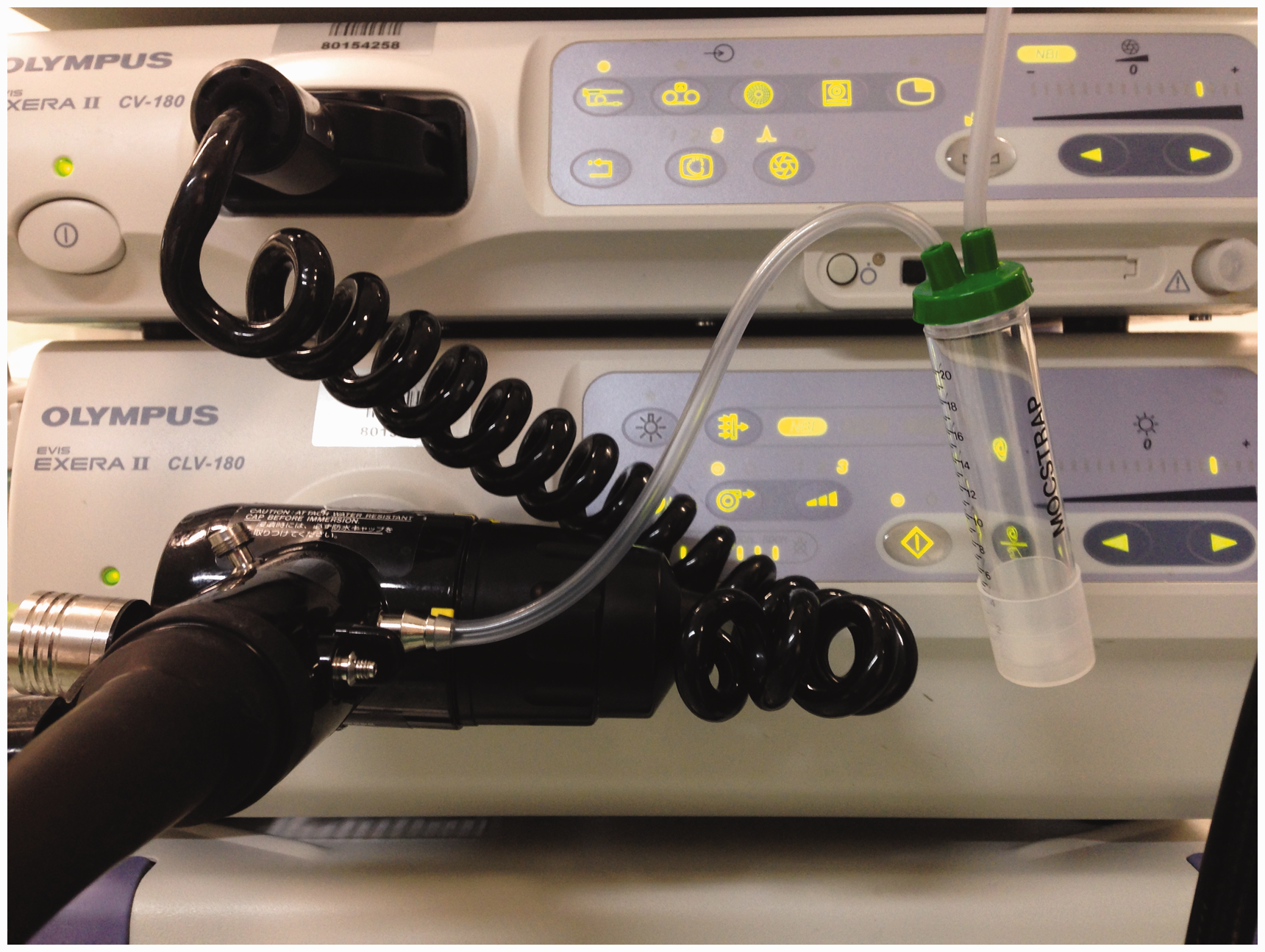
Histological and cytological assessment
Cytology specimens were collected in 20 cc CytoLyt (Hologic Inc, Bedford, MA, USA), at room temperature, and were processed by the ThinPrep technique in less than 24 hours. 21 After concentration by centrifugation, the specimen was added to a PreservCyt (Hologic Inc, Bedford, MA, USA) solution vial and run on a ThinPrep Processor 5000© using sequence 2 (FLU/FNA).
Two liquid cytology slides were obtained from each specimen. The slides were fixed, the first one being stained with May-Grünwald/Giemsa protocol and the second one with Papanicolaou stain.
Cellular material was quantified by scanning each preparation using a Leica Aperio Scanscope XT digital slide scanner, and Leica Aperio ImageScope v12.0.0.5039 as digital slide viewer.
Differential cell counts: The differential inflammatory cell count was performed on May-Grünwald/Giemsa slides selecting a 1 mm2 area in ImageScope by the random field counting technique. 22 At least 200 cells were counted in each specimen, including lymphocytes, neutrophils, eosinophils and macrophages.
Haematoxylin and eosin (H&E) histology slides were obtained from oesophageal biopsies following conventional procedures. Two pathologists reviewed each slide independently (MGR and LGL).
Statistical analysis
The PASW18 statistical package (SPSS, Chicago, IL, US) was used. Data for continuous variables were expressed as mean ± SD and we used the analysis of variance (ANOVA) test and Student’s t-test for hypothesis testing of data from the overall sample. We used the chi-square test for categorical variables. To study the correlation between LBC and histology specimens, the Spearman rho test was used. Receiver operating characteristic (ROC) curves were used to calculate the sensitivity and specificity of oesophageal LBC for diagnosis and monitoring of EoE activity.
Ethics
All patients were included in the study after signing the informed consent. The study was evaluated and approved by the Independent Ethics Committee (IEC) of the Hospital General Universitario, Ciudad Real.
Results
Baseline characteristics
Baseline characteristics of patients included in the study
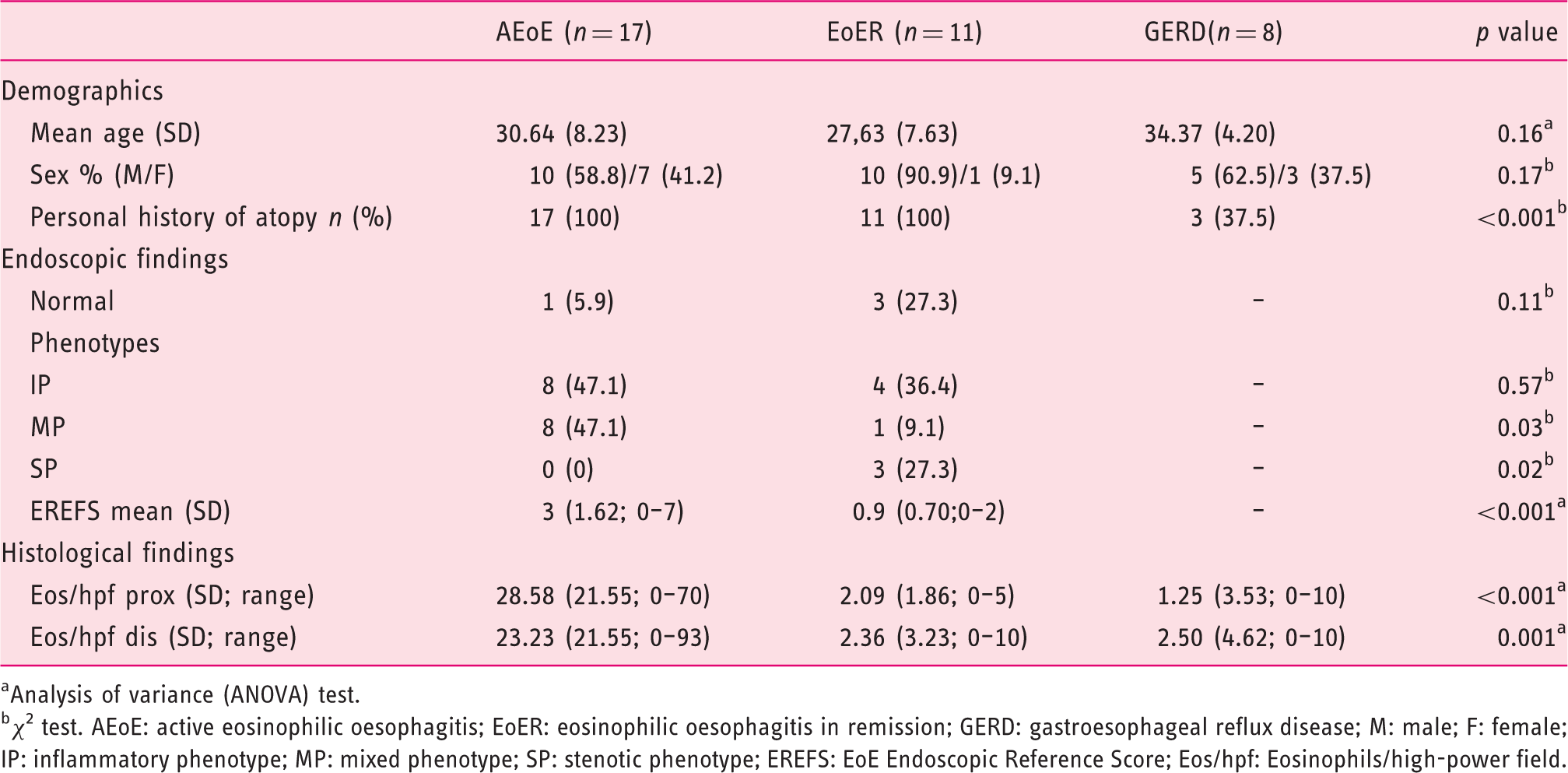
Analysis of variance (ANOVA) test.
χ 2 test. AEoE: active eosinophilic oesophagitis; EoER: eosinophilic oesophagitis in remission; GERD: gastroesophageal reflux disease; M: male; F: female; IP: inflammatory phenotype; MP: mixed phenotype; SP: stenotic phenotype; EREFS: EoE Endoscopic Reference Score; Eos/hpf: Eosinophils/high-power field.
Oesophageal aspirate for obtaining cytology
In two patients with EoE (5.2%), a fault was detected in the oesophageal aspiration technique, yielding an insufficient sample for cytological analysis. No complications were detected during the procedure.
Cell count in oesophageal cytology
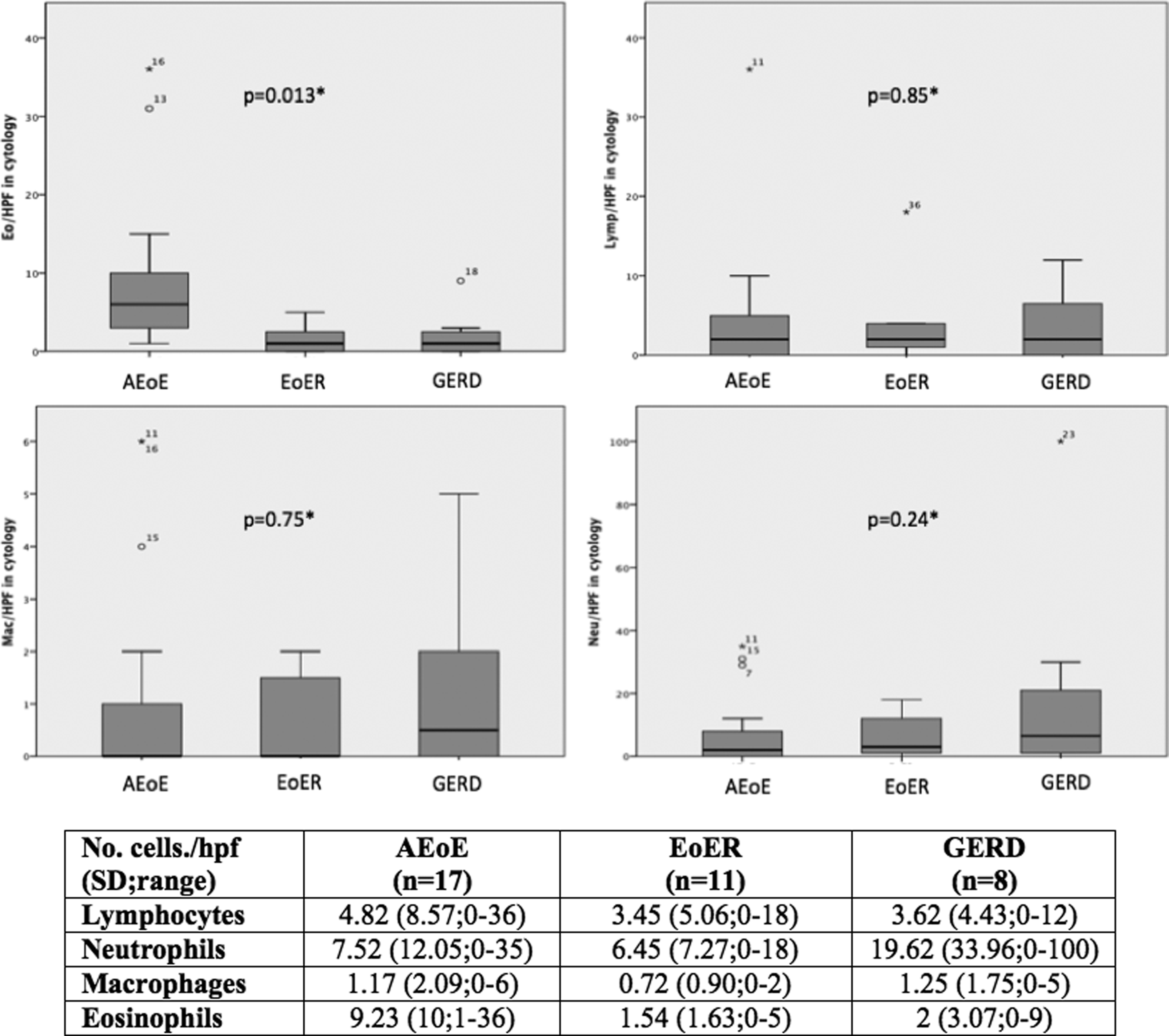
Adequate cellularity was observed in the samples corresponding mostly to oesophageal epithelium cells (Figure 2). No gastric epithelium was obtained in any of the samples. In the specimens of patients with AEoE, a significantly higher number of eos/hpf were found than in EoER and GERD. However, no differences in other inflammatory cells were found, irrespective of disease activity. It was noteworthy that in LBC specimens of patients with GERD a predominance of neutrophils was observed with respect to other populations analysed, but although this was the case, no significant differences were detected with respect to what was found in specimens from patients with EoE (Figure 3).
Cytology sample of an eosinophilic oesophagitis (EoE) patient. Cluster epithelial cells (black arrow) surrounded by more than 30 eosinophils (red arrow) with other cell subsets (yellow arrow) (lymphocytes and polymorphonuclear neutrophils) (20 ×). Inflammatory cells count in oesophageal cytology. *Analysis of variance (ANOVA) test.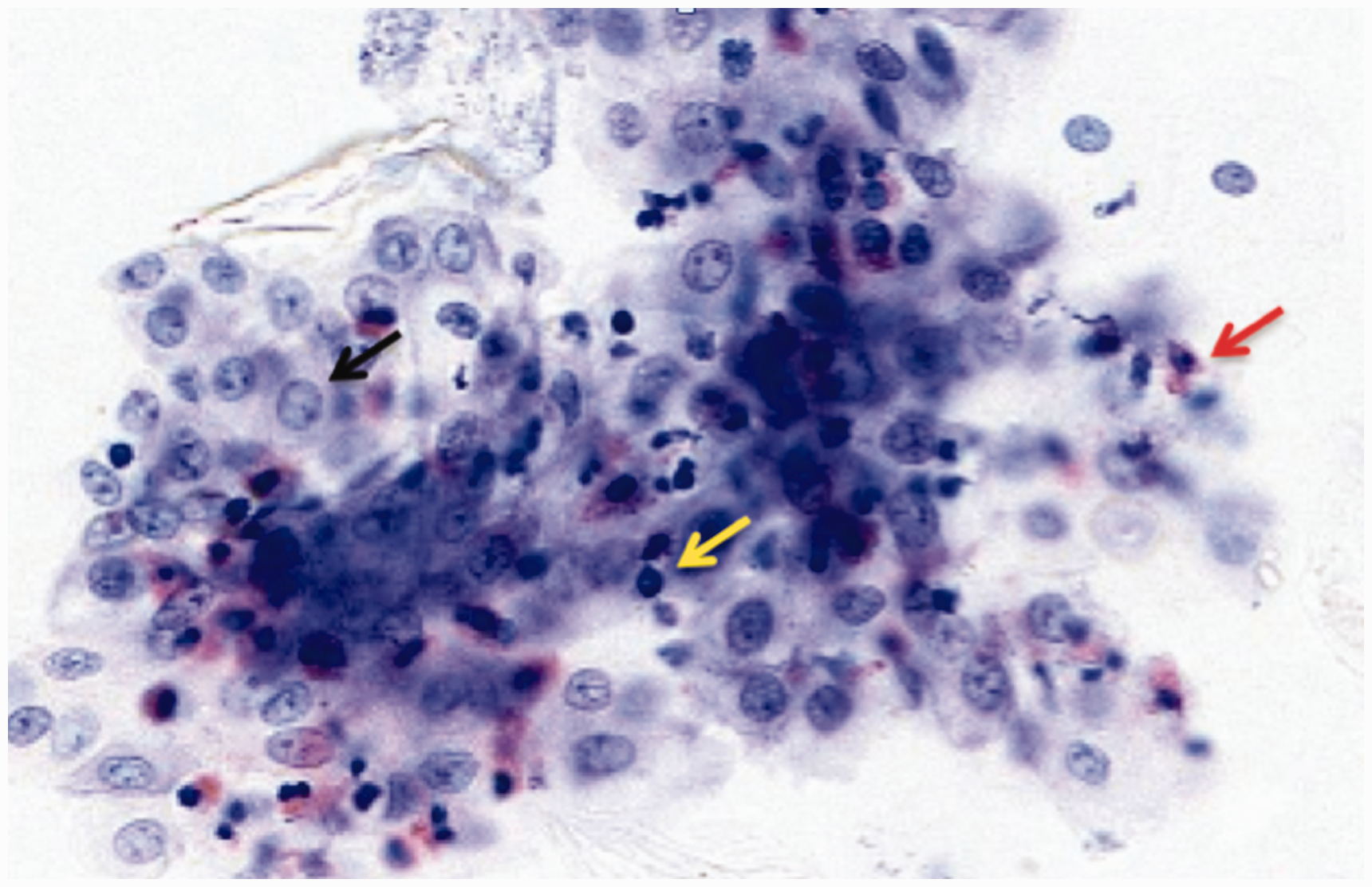
Correlation between cytology and endoscopy
A higher eosinophil count was observed in LBC of patients with IP, with respect to normal endoscopy patients (7.41 vs. 0.75, p = 0.03) and SP, despite the latter not reaching statistical significance (7.41 vs. 1.33, p = 0.06). With regards to MP, the count was similar to that observed in patients with IP. However, a strong positive correlation between eosinophil count in the LBC and the score obtained in the EREFS system was observed (Spearman rho = 0.631; p < 0.001).
Accuracy of the oesophageal cytology in the diagnosis and monitoring of EoE
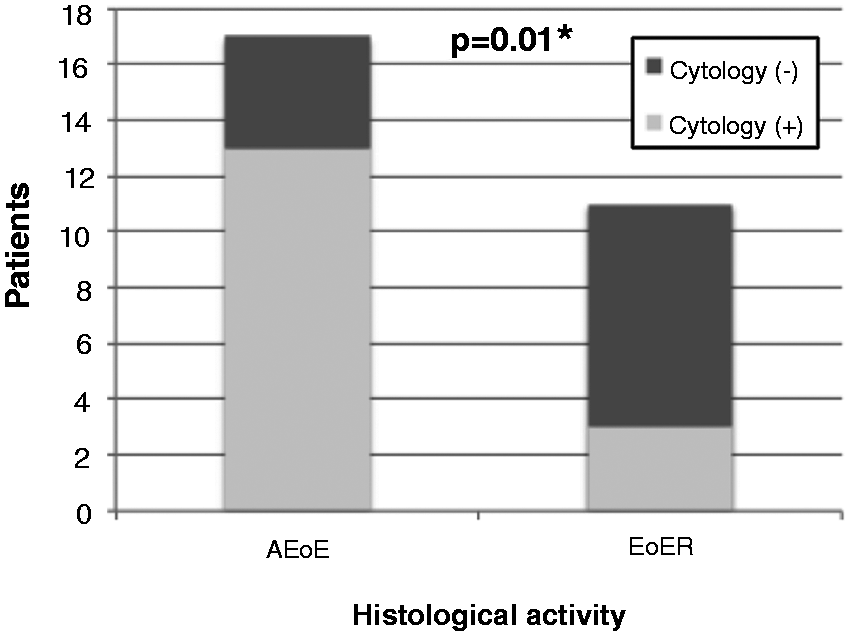
A good correlation was observed between the average number of eosinophils detected in biopsies and that detected in the LBC samples (Spearman rho 0.57, p < 0.001); however, in other cell populations studied no significant correlation was observed. Taking as a reference for the diagnosis of EoE ≥ 15 eos/hpf,1,6 and calculating ROC curves, it was seen that a number ≥3 eos/hpf on oesophageal LBC yielded for the diagnosis of EoE a sensitivity of 70%, specificity of 81%, with a positive predictive value (PPV) of 86% and a negative predictive value (NPV) of 60%. For detection of active EoE, ≥3 eos/hpf in oesophageal LBC obtained a sensitivity of 70%, specificity of 82%, with a PPV of 81% and a NPV of 66% (Figures 4 and 5).
ROC curves of the different cell populations in the oesophageal LBC. Comparison between histology and cytology findings.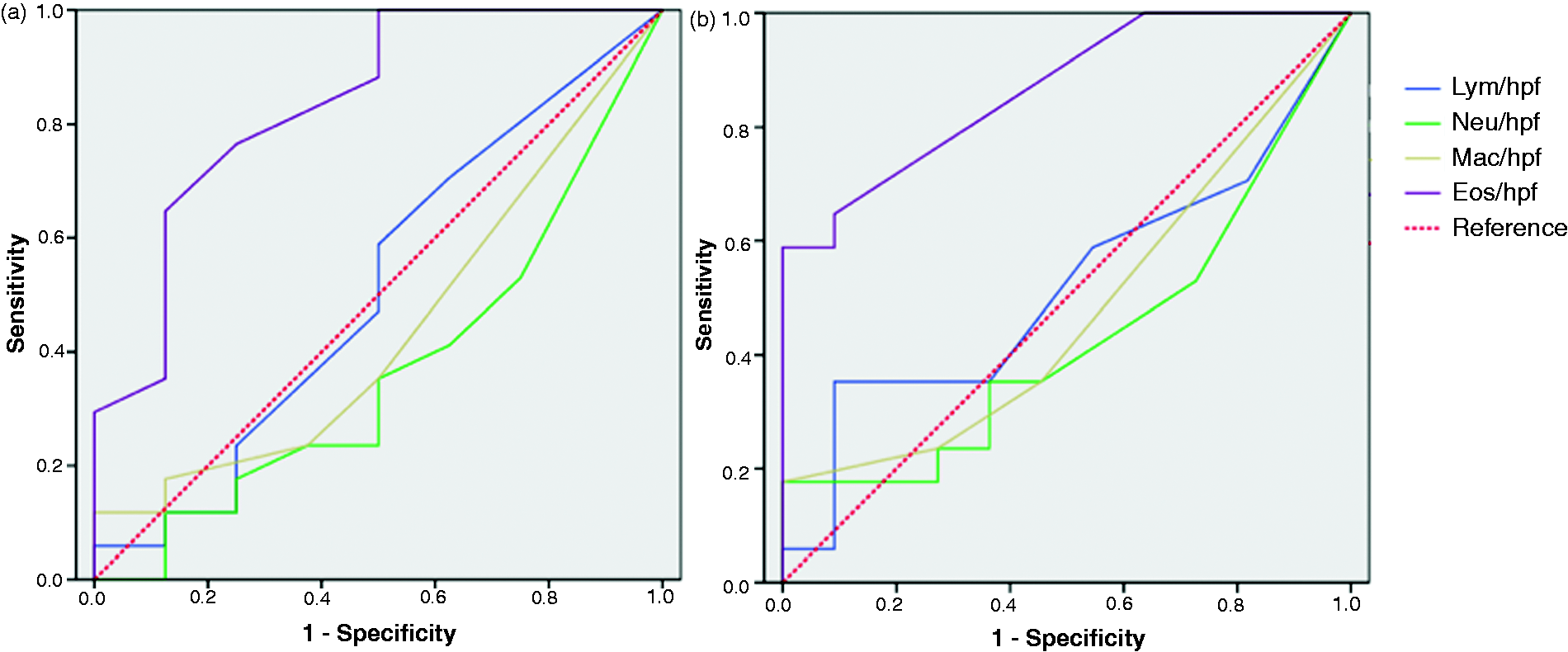
Discussion
The present study examines the usefulness of oesophageal LBC in the diagnosis and monitoring of EoE activity. The results show how the degree of inflammatory activity of the oesophageal tissue is parallel to that found in the LBC, which corroborates the results obtained previously with Cytosponge 18 and by detection of eosinophil granule proteins in oesophageal intraluminal fluid. 15
In spite of the necessity of the endoscopic procedure to obtain LBC, it has two advantages over histology: Firstly, LBC avoids the risk tears caused by biopsy sampling, and secondly, it allows for faster processing and analysis of samples, which is pretty interesting in dietary therapies during food reintroduction protocols. Although the Cytosponge is able to get oesophageal cytology without endoscopy, but it can be difficult to apply in patients with oesophageal strictures; this fact is solved by obtaining LBC.
There was a striking discrepancy in the cutoff of the eosinophil count found in the LBC (≥3 eos/hpf) compared to that found in the biopsy (≥15 eos/hpf)1,6 to determine disease activity. This reflects the reduced ability of LBC to detect eosinophils, which probably are located in superficial layers of the epithelium, which on the other hand is the predominant area affected in the EoE but not the only one.5,23 In this regard, the Cytosponge has more capacity to obtain samples with a higher volume of tissue, so its cutoff to determine disease activity is the same as biopsy samples. 18 Interestingly, the sensitivity figures obtained (70% for diagnosis and determination of activity) and NPV (60% for diagnosis and 66% for determination of activity) demonstrate the limited utility of the LBC (obtained by oesophageal aspiration) as a tool for monitoring disease. This should be improved by optimising the sampling technique, even though in our study LBC specimens were classified as suitable for diagnosis in 95% of cases. On the other hand, it is known that microscopic disease manifestations are reflected in the endoscopic findings, having a count of eos/hpf significantly higher in patients with whitish exudates. 24 Moreover, the resolution of inflammatory activity is accompanied by a resolution of the endoscopic findings. 25 This explains the positive correlation between eosinophil count in the LBC and EREFS score. While it is true, as demonstrated in a recent study, as occurs with biopsy, no significant differences were detected between the different phenotypes in terms of endoscopic eosinophil count in the LBC. 26
The analysis of the rest of the inflammatory cells shows how the inflammatory profile of EoE differs widely from that found in patients with GERD, where there is a predominance of polymorphonuclear neutrophils, which is consistent with that previously described for erosive GERD.23,27 The role of lymphocytes as coordinators of the immune response in EoE is a fact proven both in vivo 28 as well as in animal models. 29 However, the small variation found in the lymphocyte count between AEoE and GERD is notable, which can be translated into the coordinating role of the immune response of this cell line in GERD. This is also suggested in a study which shows how the lymphocytic infiltrate is the first event that happens in the inflammatory response caused by reflux. 30
The study has several limitations. The LBC sampling technique (oesophageal aspirate) is a method that seeks to simulate the technique of bronchioalveolar lavage but is not validated for obtaining oesophageal LBC, which can have a decisive impact on the results of diagnostic yield obtained with the LBC. Furthermore, the processing of samples and assessment of eosinophil count is an experimental method whose inter- and intra-observer variability has not been analysed and therefore may be subject to improvements. Another recognised limitation is the small number of patients recruited for the study; for more solid conclusions to be drawn, this technique should be tested on a larger sample and in different centres.
In conclusion, oesophageal LBC seems to be a useful tool in the diagnosis and monitoring of EoE, although these results can certainly be improved substantially by optimising the techniques for obtaining LBC specimens. It is an option in patients who suffer oesophageal strictures that hamper the passage of the endoscope for biopsy sampling.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.