
Abstract
Background
Chronic pancreatitis (CP) in children is an inreasingly recognized disease.
Objective
The purpose of study was to analyse the safety and long-term efficacy of endoscopic treatment in children with CP.
Methods
Records of 38 patients aged <18 years, referred to the Digestive Endoscopy Unit at Catholic University, Fondazione Policlinico “A. Gemelli” IRCCS between 1991 and 2017, were reviewed. Abdominal pain, analgesia and number of episodes of acute pancreatitis in the pre- and post- endoscopic retrograde cholangiopancreatography (ERCP) period were evaluated. Need for surgery was assessed. Therapeutic intervention data and complications were interrogated.
Results
In total 158 ERCPs were performed. Median post-ERCP follow-up was 7 years. The majority of patients had CP type IV (47%) and type Ib (37%) (Cremer’s classification). Major papilla pancreatic sphincterotomy was performed in 47%, major and minor in 24% and minor in 29% of patients. Stones/plugs were removed in at least one ERCPs in 66% individuals. Eleven out of 38 patients had stricture of the pancreatic duct; these were dilated and stented in 5/11 and stented in 6/11. Five complications were recorded (3%). Severity and frequency of abdominal pain improved significantly; p < 0.001. Use of analgesia and number of episodes of acute pancreatitis decreased significantly; p < 0.001. One child required subsequent surgery.
Conclusion
Endoscopic management of symptomatic CP in children is safe and effective.
Key summary
Endoscopic therapy of CP is an effective treatment in adult cohorts. Lack of data on ERCP efficacy and safety in children with CP remains an issue. Our large European cohort supports high efficacy of endoscopic treatment in pediatric patients with CP. Rate of complication in experienced hands is very low. Endoscopic intervention minimized severity and frequency of abdominal pain and episodes of acute pancratitis significantly in our study. Minimum of children (just one in our cohort) had to undergo subsequent surgery (we looked at outcomes recorded during a long (26 years) period).
Introduction
Chronic pancreatitis (CP), a pathological fibroinflammatory condition of the pancreas which develops in individuals with genetic, environmental, and/or other risk factors, used to be diagnosed very rarely in the pediatric population; nevertheless, it has become increasingly recognized recently.1-3 Irreversible structural changes result in pain syndrome (recurrent episodes or persistent pain) and can progress to exocrine and/or endocrine pancreatic insufficiency.1,4 Gene mutations (including PRSS1, SPINK1, CFTR and CTRC mutations) and anatomical variations of the pancreatic ducts are reported to be the most typical risk factors in the pediatric population with CP.1,5,6
If medical therapy of pain related to CP fails, endoscopic and surgical strategies remain alternative therapeutical options.4,7 Endoscopic therapy of CP is an effective treatment in adult cohorts,8,9 and growing evidence of high efficacy has been documented also in the pediatric population.10-13 Due to a higher rate of complications caused by endoscopic retrograde cholangiopancreatography (ERCP) compared with any other gastrointestinal (GI) endoscopy, careful selection of patients for therapeutic ERCP and use of non-invasive tests for diagnostic purposes of pancreatic disorders are essential. 11 A lack of data on ERCP safety in children remains an issue.11,14
The purpose of this single-centre retrospective study from a prospectively collected database was to analyse safety and long-term efficacy of ERCP procedures performed on a pediatric population with CP in a tertiary referring centre.
Methods
Records on therapeutic ERCP procedures performed on consecutive patients younger than 18 years, who were referred to the Digestive Endoscopy Unit at Catholic University, Fondazione Policlinico “A. Gemelli” between October 1991 and July 2017, were reviewed.
Magnetic resonance cholangiopancreatography (MRCP) has been performed systematically before the first ERCP in children with suspicion of CP since 1998. A total of 87% (33/38) children underwent MRCP prior to the first ERCP. Based on the pancreatographic findings, type of CP was scored according to the classification of Cremer et al. 15 Therapeutic interventions included sphincterotomy ± dilatation ± plugs/stone extraction ± stenting.
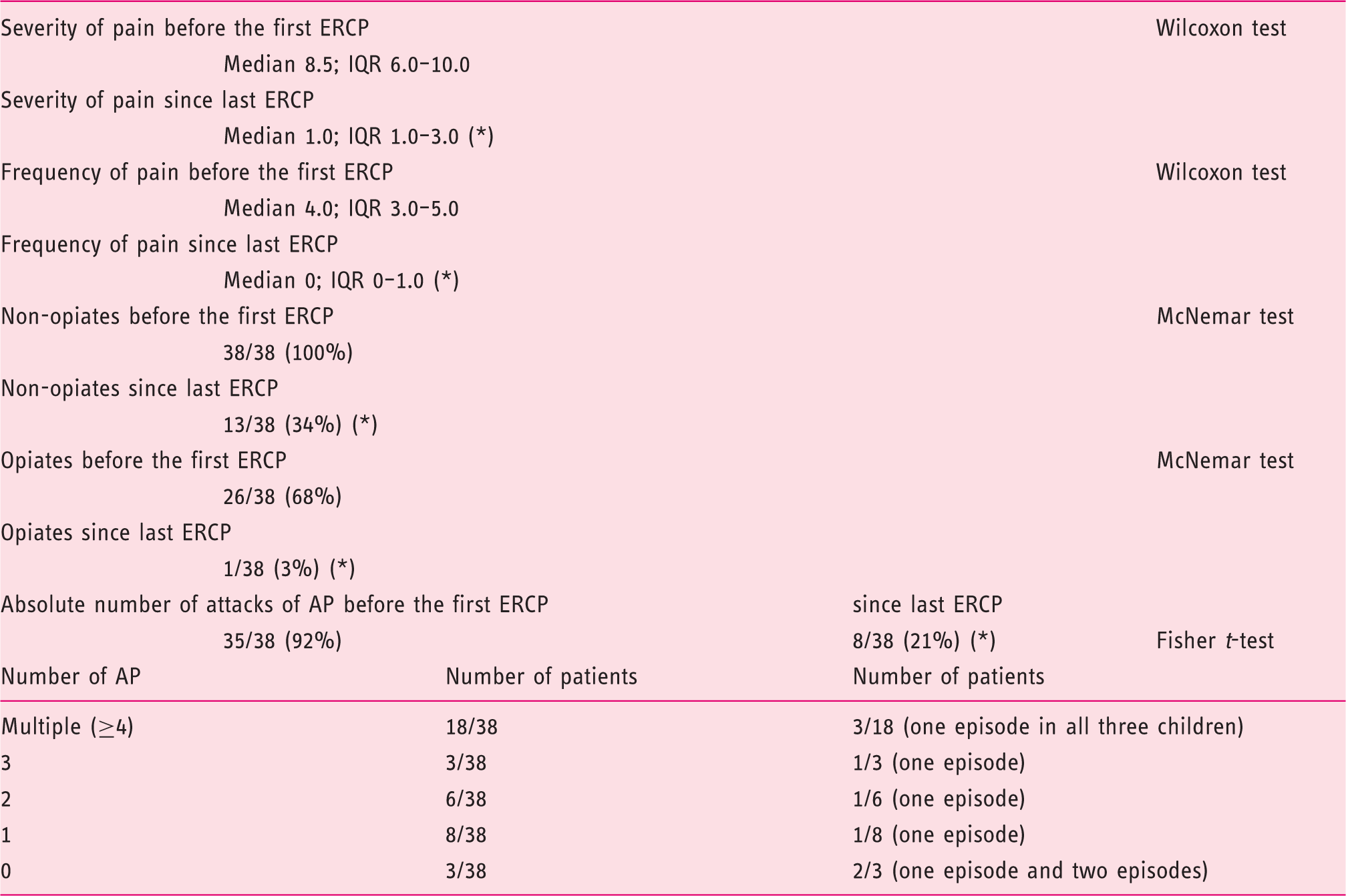
Clinical symptoms and use of analgesia prior to the first ERCP and since the last ERCP. AP: acute pancreatitis. (*): statistical significance; p < 0.001.
ERCP was performed with a standard therapeutic duodenoscope with a 4.2 mm working channel (Olympus TJF series, Tokyo, Japan) in all the cases. Endoscopic accessories commonly used for procedures in adult patients were used for ERCP in this cohort. Radiation exposure was kept to the minimum required for a safe procedure, and protection of radiosensitive organs (gonads, thyroid gland) was provided
16
(Figure 1). All procedures were carried out under general anaesthesia with endotracheal intubation by a certified anaesthesiologist.
A 3-year-old girl (weight: 16 kg) undergoing ERCP. Radiation protection apron is placed on the gonads and thyroid.
Data on therapeutic intervention, including sphincterotomy of the major and/or minor papilla, pancreatic duct stricture dilatation, sphincter dilatation, pancreatic plugs/stone extraction and pancreatic stent insertion were interrogated.
All children stayed overnight and adverse events were recorded accordingly.
Follow-up
The follow-up period was defined as the period between the date of the last ERCP at Gemelli hospital and the last follow-up contact (December 2017).
The following parameters were assessed: severity and frequency of abdominal pain (assessment as above), use of analgesics (non-opiates, opiates), number of episodes of acute pancreatitis, exocrine insufficiency (conveyed as presence of steatorrhoea and/or medication with pancreatic supplements), endocrine insufficiency (presence of diabetes mellitus), body mass index (BMI), need for surgery and current clinical status in general (good–fair–poor).
Ethical issues
All subjects and their family members were given the necessary information about the procedure and informed consent was provided from the parent of each child via a signed form.
The project was approved by the Ethical Committee of the Catholic University of Rome (May 25th 2017, protocol #0026801/17). The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.
For obtained data, all personal identification information was removed.
Statistical analysis
Data were tested statistically by means of tests of normality, descriptive statistics, Mann–Whitney test, Wilcoxon test (non-normal distribution of data), McNemar test and Fisher test (categorical data) using STATISTICA software, version 13, 2013, Tulsa, OK, USA.
Results
In total, 39 children with CP received therapeutic ERCP. One patient was lost to follow-up, therefore data from 38 individuals are provided.
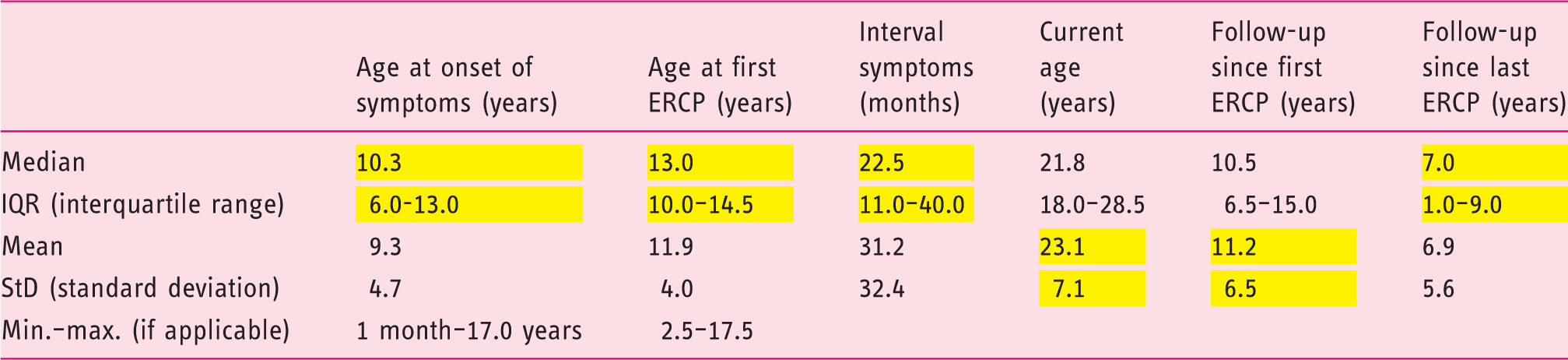
Descriptive statistics of enrolled patients. Depending on tests of normality, data provided in yellow are the correct one.
Positive family history of CP (parents and/or grandparents suffering from CP) has been confirmed in 26% individuals (10/38) with positive CFTR gene in 4/38 (11%).
A total of 87% (33/38) children underwent MRCP prior to the first ERCP with results being indicative of CP.
In the pre-ERCP period, 74% (28/38) children suffered from recurrent acute pancreatitis (with or without further episodes of abdominal pain), 13% (5/38) from a single episode of acute pancreatitis, 5% (2/38) had combination of abdominal pain and a single episode of acute pancreatitis, and 8% (3/38) had history of attacks of abdominal pain.
Anatomical variation of the pancreas was present in 16/38 (42%) children. Pancreas divisum was the most common one (Figure 2). A total of 158 ERCPs (median 3; IQR 1–5) were performed in these 38 children; 71% (27/38) individuals underwent ≥2 ERCPs. The majority of patients had CP type IV (18/38; 47%) according to Cremer’s classification
15
(Table 3).
Chronic pancreatitis in a child with pancreas divisum. Stone is visible (arrow) inside the pancreatic duct. Stone was radiotransparent and not visible on plain abdominal film. Details regarding anatomy, repeat ERCP and classification according to Cremer.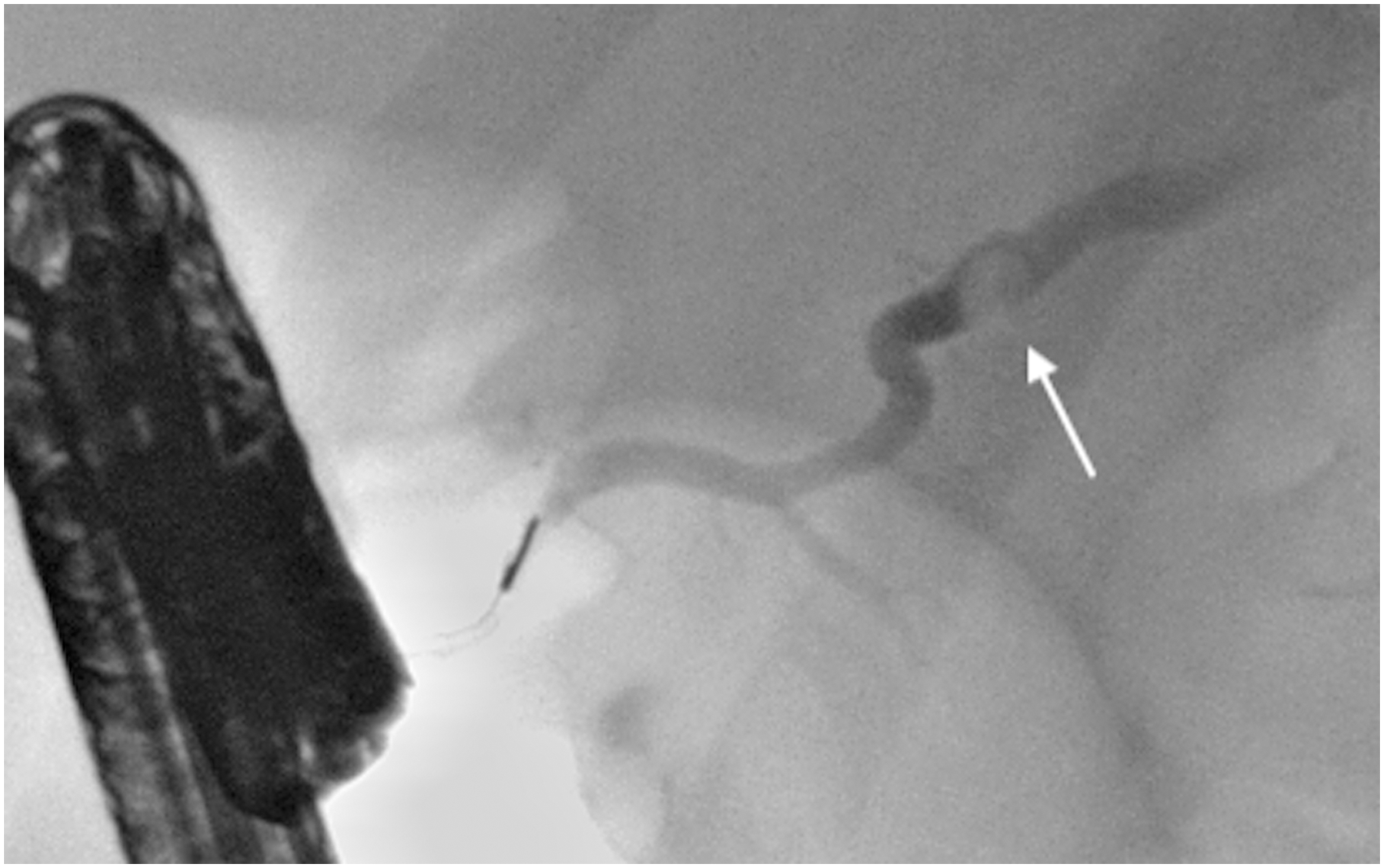
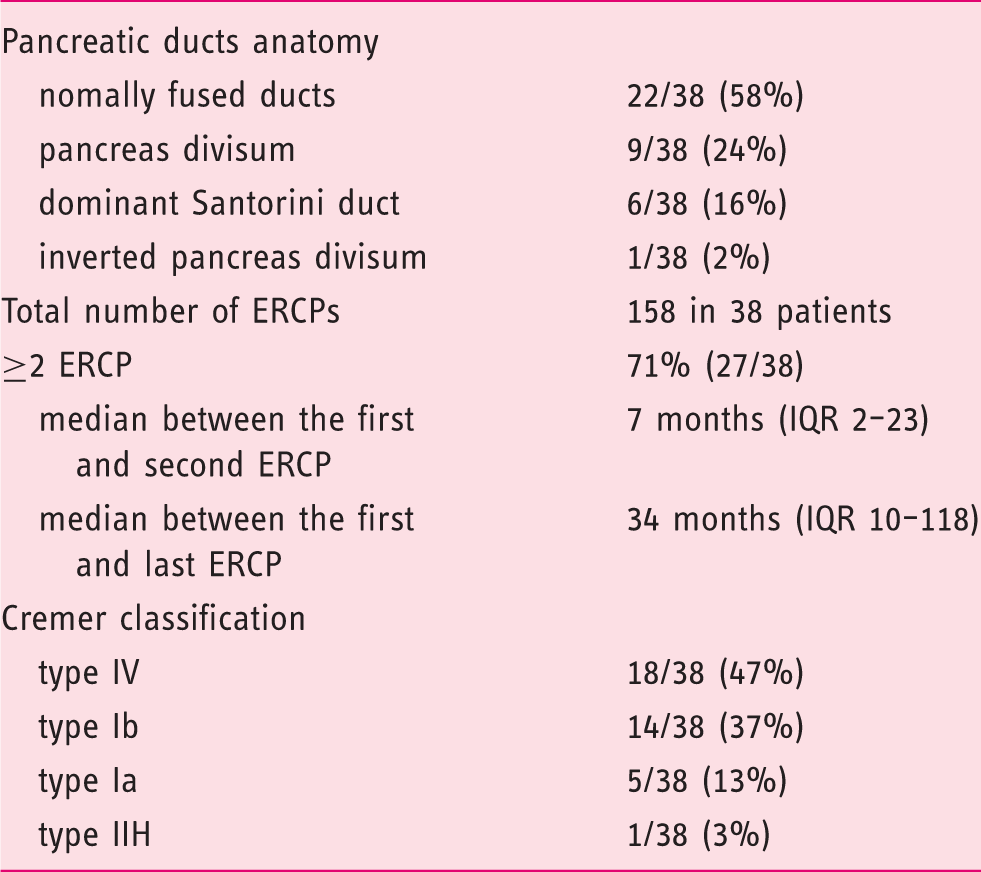
Extracorporeal shock wave lithotripsy (ESWL) was performed in three individuals (3/38; 8%). Stones and/or plugs were removed in at least one of the ERCPs in 25/38 (66%) children. Three patients who received ESWL had calcifications; the remaining 22 patients had plugs or radiotransparent stones extracted.
Summary of therapeutic ERCP interventions.
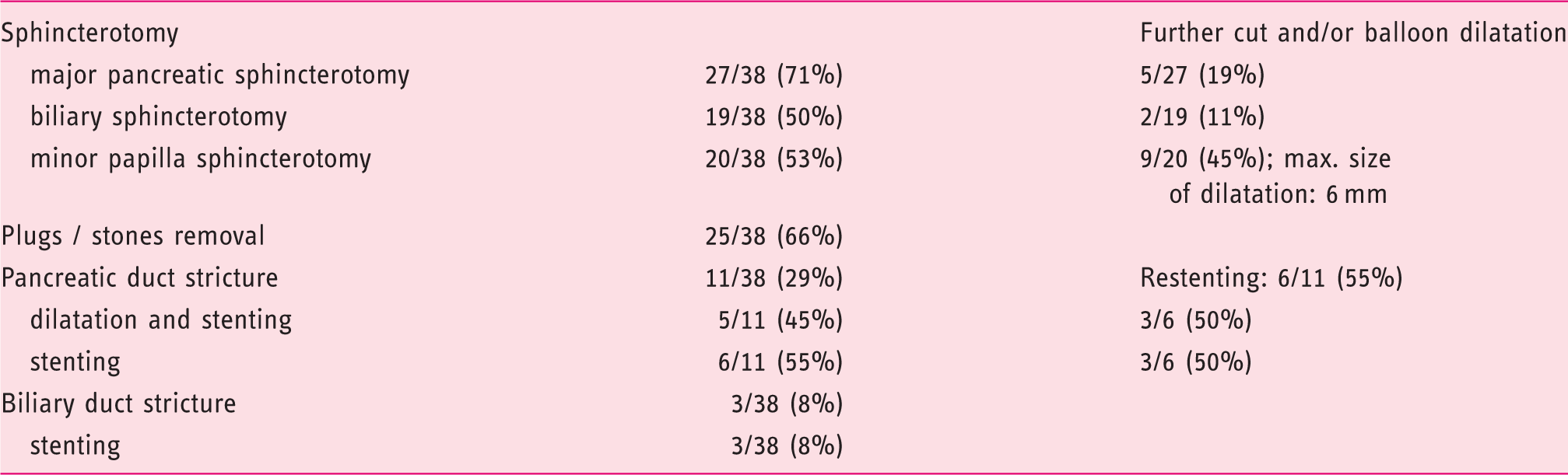
Eleven out of 38 patients (29%) had a stricture of pancreatic duct. This required dilatation with a 4–6 mm balloon and stenting in 45% (5/11) or stenting alone in 55% (6/11) (Table 4). Stents were usually inserted for 1–6 months. Cumulative duration of the stenting period which would be longer than 12 months was observed in three cases: 17 months, 45 months and 56 months. Plastic stents were always used with the exception of one patient who received a fully covered pancreatic metal stent (6 mm diameter) in the setting of a clinical trial during further retreatment when the individual was older than 18 years. If there was no stricture of the pancreatic duct or a stricture after previous papillotomy, either a prophylactic 5 french pancreatic stent or a nasopancreatic drain (for 24 h) were always inserted after a pancreatic sphincterotomy.
Biliary stricture was confirmed in three patients (8%; 3/38) and plastic biliary stenting was performed in all three cases. One more plastic biliary stent had to be introduced in the patient who had a metal pancreatic stent inserted and developed acute cholangitis.
Adverse events
Five complications were recorded (3%; 5/158): delayed post-ERCP bleeding which was successfully treated by endoscopic hemostasis and did not require blood transfusion, acute pancreatitis, acute cholangitis (requiring biliary stenting) and acute cholecystitis in two cases. All the complications resolved by endoscopic or medical therapy without long-term consequences; no procedure-related mortality occured. The median length of admission in five patients with complications was 5 days (IQR: 4–9; minimum: 3, maximum: 24 days).
Follow-up
Current age of individuals enrolled in our cohort is 23 ± 7 years. Severity and frequency of abdominal pain improved significantly since the last ERCP compared with the pre-ERCP period (p < 0.001); 66% (25/38) of children became pain free. Use of non-opioid and opioid analgesia decreased significantly since the last ERCP, and so did the number of episodes of acute pancreatitis (p < 0.001) (Table 1).
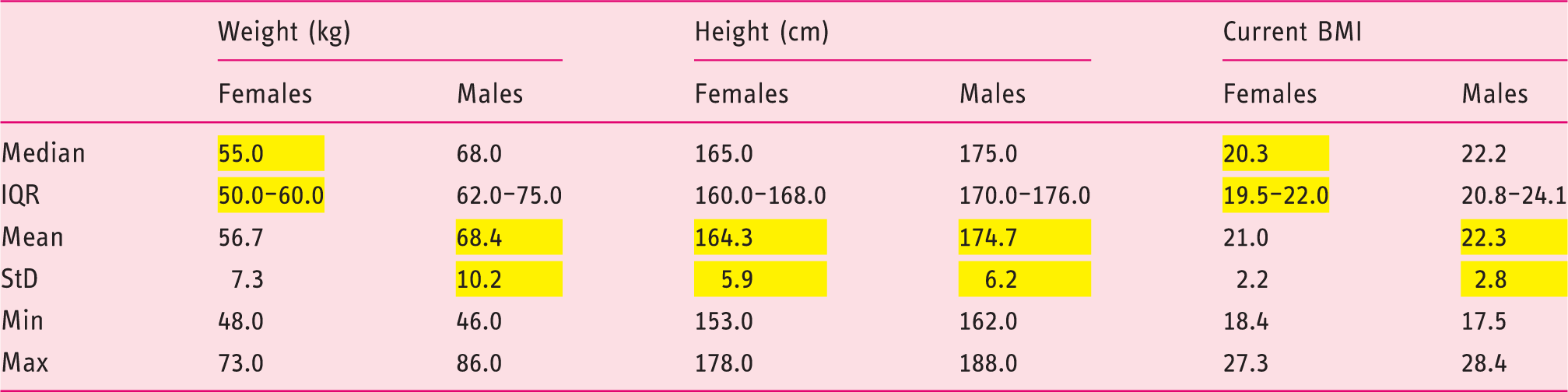
Current weight, height and BMI of female and male patients. Trend towards a statistical significance in higher BMI in males was found; p = 0.07. Depending on tests of normality, data provided in yellow are the correct one.
One patient required subsequent surgery (hepatico-jejunoanastomosis) for refractory bile duct stricture.
In total, 74% (28/38) patients classify their current clinical status as good, 26% (10/38) as fair, and no patient described their clinical status as being poor.
Discussion
CP in children, an increasingly recognized disease, can interfere with the psychophysical development of such an individual significantly.1,3,7,17 The possibility to influence abdominal pain and episodes of acute pancreatitis, associated with impaired nutrition, need for admissions and need for surgery, is an imperative in patients with CP, especially in the pediatric cohort. Our study looked at the safety and long-term efficacy of therapeutic ERCP in children and adolescents with CP.
In agreement with data published recently,10,12,18,19 our series confirmed that ERCP in a pediatric population with CP is a safe therapeutic option, having had five complications after 158 therapeutic procedures (3%).
Our study has confirmed data published by Halvorson et al. that therapeutic ERCP can be performed safely and efficaciously by adult gastroenterologists who have been trained in advanced endoscopy. 20 All individuals in our cohort were endoscoped with an adult duodenoscope, and accessories commonly used for ERCP performed in adults were used. This did not decrease technical success and did not increase complication rate. Our conclusions are in agreement with results provided by Yildrim et al. 21
Post-ERCP pancreatitis is the most common complication, yet strong data on risk factors and prophylaxis including rectal indomethacin administration and prophylactic pancreatic duct stenting have been identified in the adult population so far.22,23 In concordance with European Society of Gastrointestinal Endoscopy (ESGE) recommendations, 16 diclofenac was not used in our study as the majority of patients were younger than 14 years. Two recent studies analysed factors associated with post-ERCP pancreatitis in the pediatric population and both confirmed that pancreatogram, pancreatic sphincterotomy and pancreatic stenting were associated with higher incidence of post-ERCP pancreatitis. Further (prospective) studies on the role of prophylactic pancreatic stenting will have to take place. On the contrary, both studies have, once again, clearly documented, that CP is negatively associated with post-ERCP pancreatitis.24,25 Together with the high volume of patients treated at our teriary referring centre, this would explain why the incidence of post-ERCP pancreatitis was low in our cohort (1%, 1/158).
Regarding the patient with acute cholangitis, this occurred after a fully covered metal pancreatic duct stent had been inserted (otherwise, plastic stents were used in all other cases). We are aware of the recent study published by Jeong et al. 26 regarding their initial experience with the use of fully covered self-expandable metal stents for recurrent benign pancreatic duct strictures in children. Their case series (with median age 12 years) showed significant improvement of parameters observed and no post-ERCP complication occurred. The age of our patient was 19, therefore diminutive size of the ampullary area cannot explain the increased risk for obstruction of biliary system by the fully covered metal stent, but rather the presence of such a stent itself. Therefore, further studies on fully covered self-expandable metal stents need to be realized in a cohort of pediatric patients and adolescents with CP.
One post-ERCP cholecystitis was recognized in a child with biliary stricture which had required biliary stenting. The other child with cholecystitis had undergone biliary and pancreatic sphincterotomy of the major papilla without any further interventions, and no risk factors for cholecystitis were noted. Both patients received antibiotic treatment. A conservative approach was successful in both cases.
The only post-ERCP bleeding which required subsequent endoscopy was identified in a 13.5-year-old girl, who underwent sphincterotomy of the minor papilla.
In general, a very important prerequisite is to observe the pediatric patients after the ERCP procedure for 24 hours closely, so that a potential complication can be recognized and treated accordingly. Delayed complications after discharge could not be formally excluded in our study, but to our knowledge none were recorded.
Obstruction of the pancreatic duct was treated by appropriate sphincterotomy in all enrolled patients, by removal of plugs/stones if present and by dilatation and/or stenting of the pancreatic duct stricture if appropriate. This led to significant improvement of pain, significant decrease of episodes of acute pancreatitis and significant decrease in the need for analgesia. The first two outcomes influenced quality of life, undoubtedly. The third outcome is important not only when acute side effects are taken into account (mainly gastrointestinal toxicity of NSAID, status of consciousness during treatment with opiates), but from the long-term point of view, too (nephrotoxicity caused by NSAID medication). Similar to Oracz et al., 27 our study confirmed the efficiency of pancreatic duct stenting with plastic stents in a pediatric cohort with CP. Another important goal was also achieved: after the endoscopic interventions, BMI reached normal ranges in girls and boys.
Typically (almost 80%) children with CP suffer from multiple episodes of mild to moderate abdominal pain, and pancreatic insufficiency is rather rare.4,28,29 On the contrary, more than 50% adults with a diagnosis of non-alcoholic CP develop a painless form of the disease which is accompanied by a progressive deterioration of exocrine and endocrine pancreatic function. 30 In our cohort, after a median follow-up of 7 years, 37% patients have exocrine pancreatic insufficiency and one patient has diabetes mellitus. It would be interesting to assess the impact of an early endoscopic drainage of the pancreatic duct on endocrine and exocrine pancreatic function long term (median follow-up 10 years). The patient with diabetes mellitus requires insulin treatment. Surprisingly, more than half of patients received opiates before the first ERCP, resulting in an overtreatment aiming at a complete and durable pain relief in this pediatric population.
The main advantage of ERCP over surgical therapy in this setting is that the treatment can be repeated, is less invasive and can be performed even in those with portal hypertension. 4 Although 71% of children in our cohort had to undergo ERCP repeatedly, it did not impair their school attendance (admissions were usually short, lasting 2–3 days with prompt recovery) or free time activities including sport. Achievement of ERCP outcomes (mainly with regards to pain) can also indicate that the child would benefit from surgery as a more definitive option. 7 Data from large cohorts, which would compare primary endoscopic management with a primary surgical approach of CP in children, are not available. Iqbal et al. enrolled 37 children with CP: 12 children were managed endoscopically, five patients with surgery, and 20 children with surgery after previously failed ERCP. They found that the rate of recurrent pancreatitis was significantly higher in the ERCP alone group compared with patients managed operatively. Yet they did not confirm a difference in frequency of hospitalization required for CP, and narcotic use was not different between these two groups. 31 Our study demonstrated a significant drop in episodes of acute pancreatitis and a significant decrease in narcotic use after endoscopic interventions. Surprisingly, the study by Iqbal et al. also reported the same procedure-related morbidity in the ERCP and operative group. 31 This was due to a high incidence of post-ERCP pancreatitis (26%) in the ERCP alone group, which was not replicated in our study (1/158; 1%).
In agreement with Sacco Casamassima et al. and recently published guidelines,32,33 we recommend the proposed step-up practice: only if conservative management, including endoscopic interventions, fails, tailored surgery should follow in children with CP. Organ preservation is the goal; nevertheless, total pancreatectomy with islet autotransplant can be contemplated in carefully selected cases.33,34
The main limitation of the study is its retrospective and single-centre design.
Based on our data on long-term efficacy and safety, we would recommend endoscopic management of CP in pediatric patients before surgery is contemplated. Still, clinicians should decide carefully whether each child can benefit from the therapeutic ERCP long term, and information should be provided to the family members accordingly.
Footnotes
Declaration of conflicting interests
Guido Costamagna has received grant/research support from Olympus Japan, is a member of advisory committees or review panels for Cook, Inc., Boston Scientific Corp., and Taewoong Medical, Inc., and has been a speaker and teacher for Boston Scientific, Corp. and Given Imaging.
Ivo Boškoski had a consulting agreement for Cook, Inc.
Other authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
The project was approved by the Ethical Committee of the Catholic University of Rome (May 25th 2017, protocol #0026801/17). The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.
Informed consent
All subjects and their family members were given the necessary information about the procedure and informed consent was provided from the parent of each child via a signed form.