
Abstract
Background
Experts have hypothesized that a reduction of multitasking distractions and improved bowel cleanliness can explain why insertion water exchange enhances adenoma detection rate.
Objective
The purpose of this study was to test the role of both distractions during withdrawal and bowel cleanliness in enhancing adenoma detection rate using coded video records of colonoscopy.
Methods
The withdrawal phase of videos of 299 consecutive colonoscopies from two randomized controlled trials comparing water exchange versus air insufflation at a regional hospital in Taiwan were coded. The primary outcome was distractions; activities that preclude full attention being paid to inspection of the mucosa for polyps. A single blinded reviewer collected the data.
Results
There were significant agreements in inter-rater reliability indexes. Compared to air insufflation, water exchange had significantly fewer distractions; higher diagnostic yield (intervention time and number), adenoma detection rate, and Boston Bowel Preparation Scale score. Water exchange had a higher withdrawal technique score (predominantly adequacy of cleaning). The association between increased adenoma detection rate and water exchange was mediated by the number of distractions and withdrawal time, but not the Boston Bowel Preparation Scale score.
Conclusion
The speculation by experts that a reduction of multitasking distractions underlies the significantly higher adenoma detection rate of water exchange is supported by the current study. Increased bowel cleanliness did not contribute to the increased adenoma detection rate by use of water exchange.
Introduction
The introduction of water exchange (WE) colonoscopy has been a prime example of research focused on patient-centered care with the successful demonstration of reduced insertion pain.1–5 A non-WE core group of investigators published a report 6 confirming the efficacy of WE in reducing insertion pain.3–5 Follow-up studies of a serendipitous observation that WE improved overall adenoma detection rate (ADR) 1 revealed a reproducible significant improvement of ADR by WE worldwide,7–9 marking a defining moment in the evolution of WE colonoscopy.
In a list of the top 10 most important topics in 2017 published by the editorial board of Gastrointestinal Endoscopy, 10 colorectal cancer screening ranked at the top, and three of the five manuscripts supporting the unanimous choice pertained to WE significantly increasing the overall ADR.7–9 The interest of US colonoscopists was reflected in an invited essay on the subject in the June issue of ASGE Connection. 11 All of these recent developments attest to the growing recognition of the importance of WE. A recent network meta-analysis compiled by a group of world-renowned experts elegantly summarized the data showing that WE enhances patient-centered outcome and colonoscopist-controlled performance measure. 12 Without providing substantive evidence, but citing an earlier report, 13 these experts hypothesized that a reduction of multitasking distractions and improved bowel cleanliness underlie the observation, 12 Their speculation dramatized the fundamental importance of such an explanation for the effectiveness of WE in increasing ADR. Because of a previous report that the withdrawal colonoscopists could be adequately blinded if they were made unaware of the insertion method, 9 the experts also recommended that future randomized controlled trials (RCTs) involving WE should employ blinded-withdrawal colonoscopists without knowledge of the insertion methods, 12 Their endorsement of the exclusion of the insertion phase as a valid approach to blind the withdrawal colonoscopist was the critical foundation on which this current report rests.
In two RCTs of head-to-head comparisons of WE with other methods focused on insertion pain 4 or ADR, 8 video recordings of the procedures were prospectively collected. These videos were edited to exclude the insertion phase and coded to blind the reviewer who analyzed these video recordings. We postulated that insertion WE enhances the quality of mucosal inspection by decreasing the number of multitasking-related maneuvers that can distract an endoscopist from the principal task of searching for polyps during the withdrawal phase of colonoscopy. To increase the chance of obtaining significant differences if they were present, only AI and WE cases were selected for their relatively larger difference in overall ADR. In agreement with the expert recommendations we tested the hypothesis that reduction of multitasking distractions and improved bowel cleanliness explain why insertion WE is the best method for enhancing ADR.
Methods
Patients
A total of 299 prospectively collected video recordings of AI and WE in two RCTs (NCT01535326 and NCT01894191)4,8 were selected for analysis. The patients gave consent for the procedure to be recorded and analyzed. These studies were conducted at the Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan. Permission was obtained from the local Institutional Review Board (IRB)to review, analyze, and report de-identified findings (B10302018, 15 July 2014). Written, informed consent was obtained from each patient included in the study. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution's Human Research Committee.
In the RCTs, patients received the following bowel preparation instructions. For morning colonoscopies, split dosing was used (with 10 mg Dulcolax at noon the day before, one liter of polyethylene glycol (PEG) the night before, and one liter of PEG on the morning of colonoscopy). For afternoon colonoscopies, two liters of PEG were administered on the morning of colonoscopy (with 10 mg Dulcolax given the night before).4,8 Two experienced colonoscopists (YHH and CWT) performed all of the recorded colonoscopies. The quality of bowel preparation was assessed by the video reviewer with the Boston Bowel Preparation Scale (BBPS). 14
Assessment of video recordings
Inclusion criteria for the video recordings are shown in Figure 1. The selected video was edited to remove the insertion phase to blind the video reviewer to the insertion methods. One blinded reviewer (HWY) not involved in the performance of the colonoscopies evaluated the edited videos. To validate the scoring method, YHH and the designated reviewer (HWY) separately reviewed 13 randomly selected videos. The scores were compared, and discrepancies were discussed and resolved. The process was repeated until agreement was reached (Table 1). Formal review began when the number of the selected videos reached the calculated sample size. They were coded and randomized for assessment by the blinded reviewer.
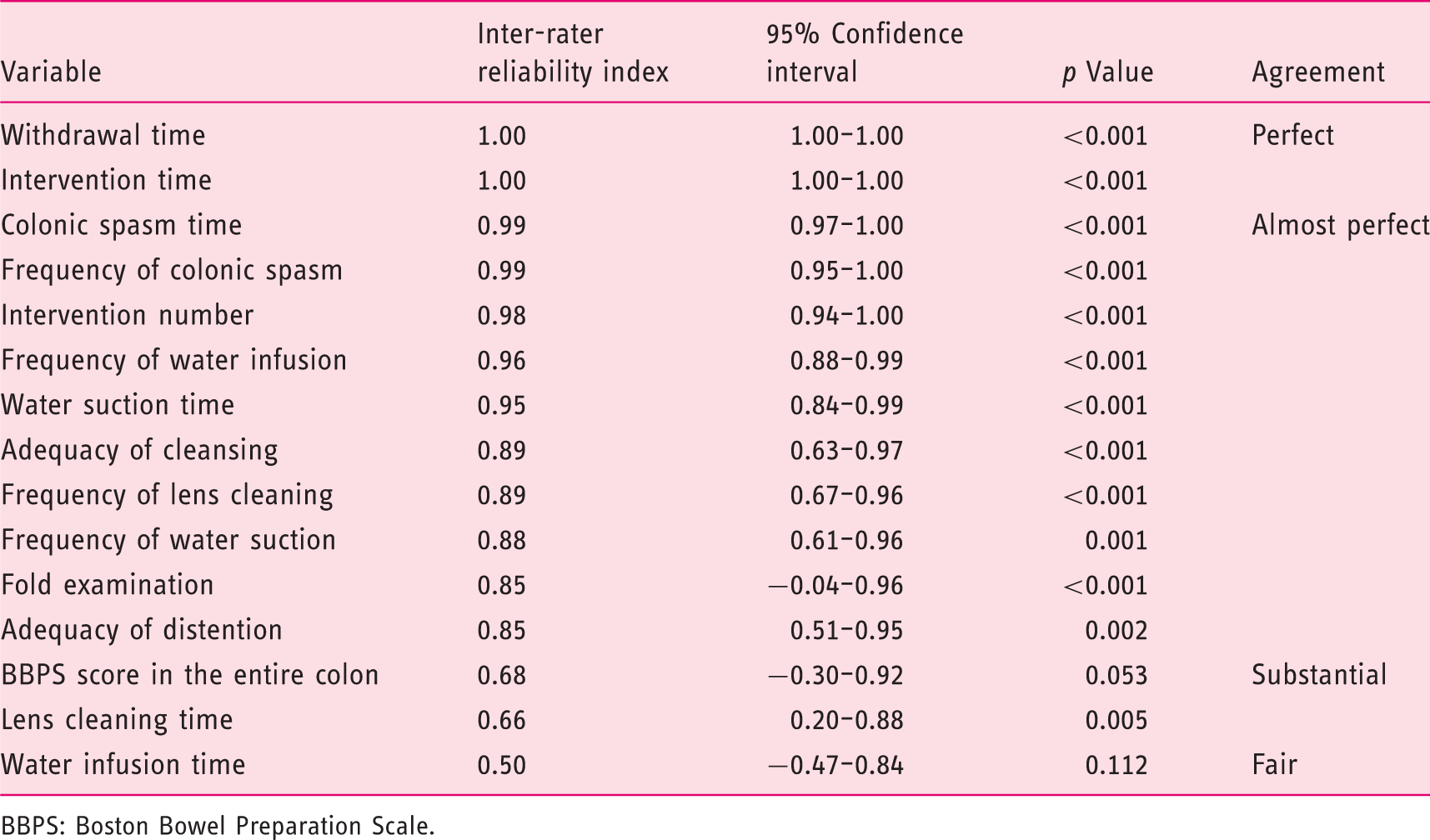
Flow diagram of selection and exclusion of video recordings. WE: water exchange. Inter-rater reliability assessed by the Shrout-Fleiss reliability index listed in decreasing order of agreement. BBPS: Boston Bowel Preparation Scale.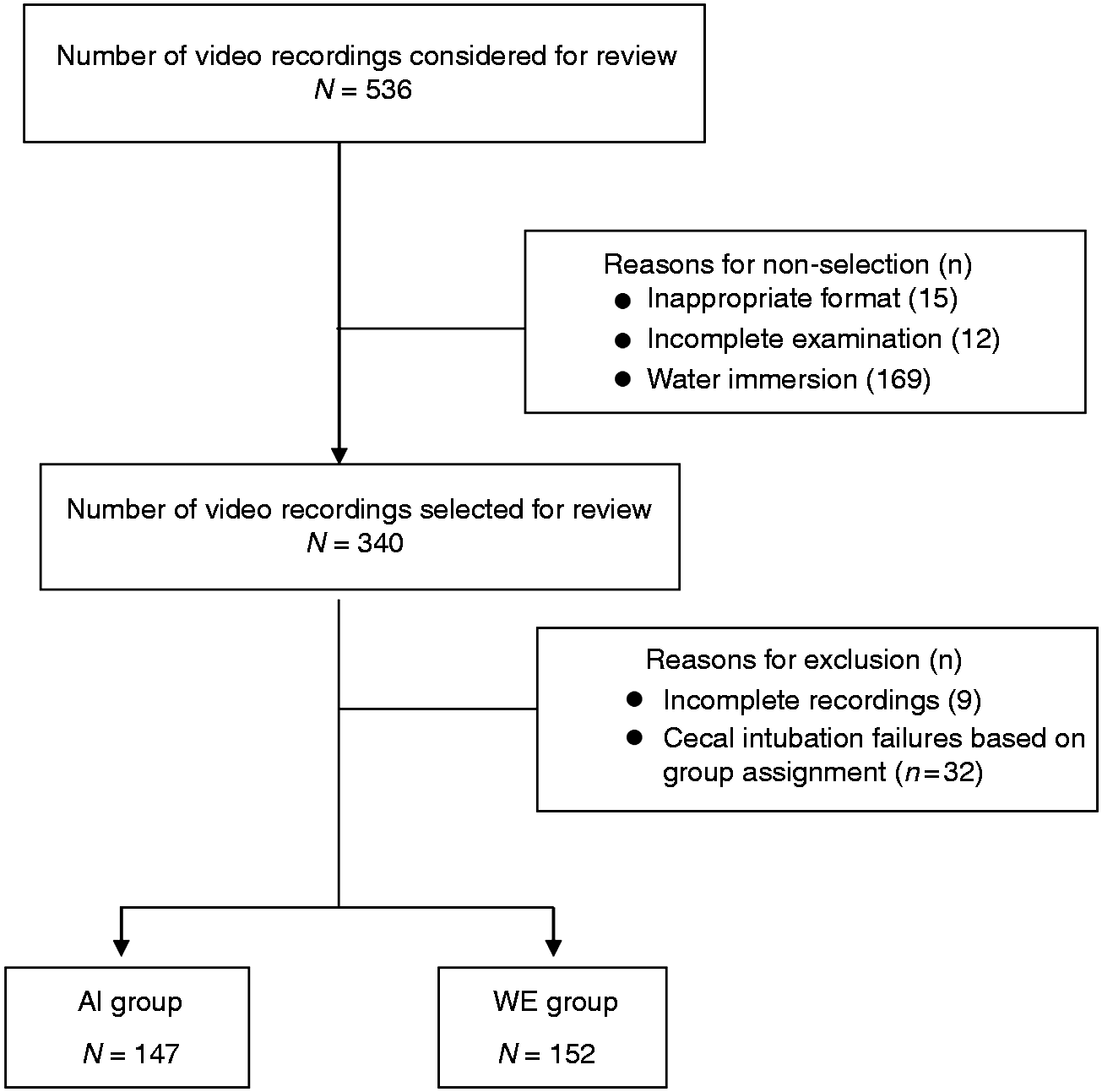
Distractions - any activities that were not directly related to inspection of the mucosa for polyps
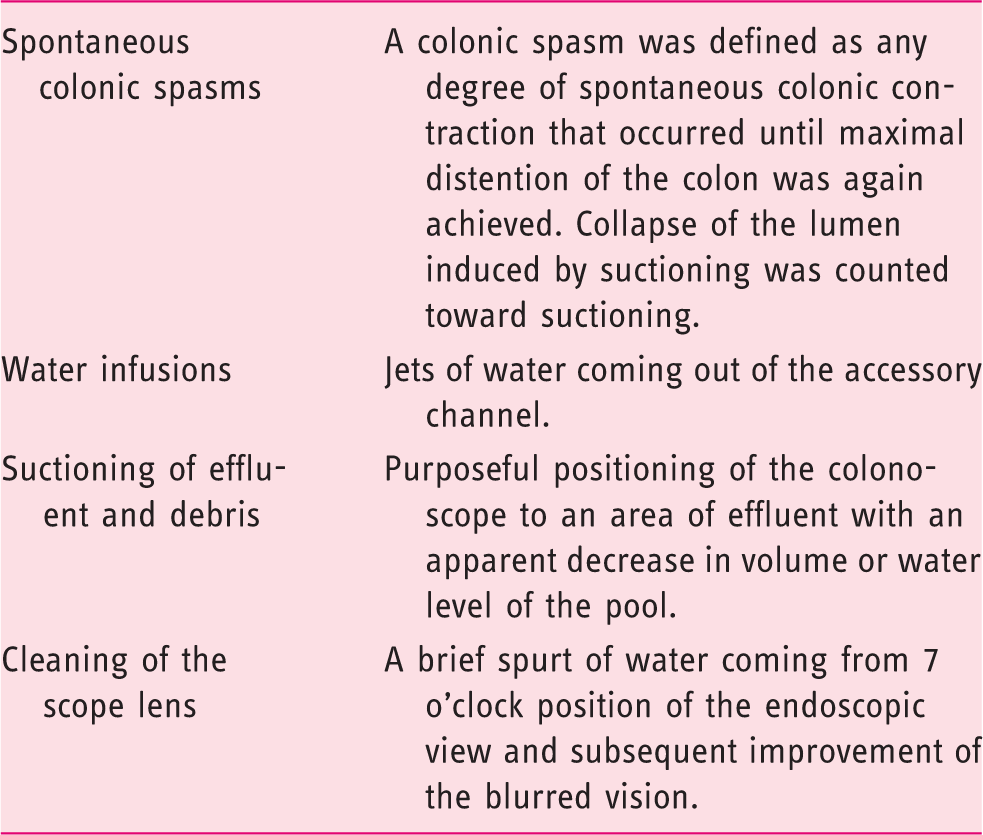
Biopsies and polypectomies were performed during the withdrawal phase. All time spent on biopsy and/or polypectomy and related maneuvers, hemostasis, or any other use of accessories passed through the biopsy channel into the field of view was counted as intervention time. An intervention began when a device first appeared in view and ended when the colonoscope was moved away from the field with all accessories removed. The mucosal inspection time was defined as withdrawal time minus total distraction (colonic spasm + water infusion + water suction + lens cleaning) and intervention time.
Statistical analysis
A pilot study showed the mean intervention number was 1.51 in the AI group and 2.11 in the WE group with a combined standard deviation of 1.82. Sample size estimation revealed 145 per group (a total of 290) were needed for significant differences to be demonstrated at the 0.05 level with a power of 0.80. Statistical analyses were performed using IBM SPSS software package, version 24.0 (IBM Corp, Armonk, New York, USA). A p value <0.05 was considered to be statistically significant. Variables were summarized as count (percentage of total), or median (minimum–maximum) and mean with standard deviation. The chi-squared test or Fisher’s exact test was used for comparison of categorical data. The Kruskal-Wallis test was used to compare the medians of continuous variables. Shrout-Fleiss intraclass correlation coefficients were used to assess inter-rater reliability index. Multiple logistic regression analysis, using likelihood-ratio-test-based backward selection method, was performed with ADR as the dependent variable, and method (WE vs AI), number of distractions, BBPS score, the duration of distraction, withdrawal technique scores, and age as independent variables. Inspection time was part of the withdrawal time which was previously described as a significantly determinant (when >6 min) of ADR. We did not include mucosal inspection time in the logistic regression analysis because it was strongly correlated with withdrawal time (Pearson correlation coefficient = 0.82, 95% confidence interval (CI) 0.78–0.86).
Multiple mediation analysis was conducted to assess mediators of the association between insertion method (WE vs AI) and ADR. Mediation analyses are employed to clarify the nature of an existing relationship between a dependent variable and independent variables by exploring the underlying process via the inclusion of mediating variables. Potential mediating variables evaluated were BBPS score, withdrawal time, withdrawal technique score, duration of distraction, and number of distractions, adjusting for age. We did not include mucosal inspection time in the mediation analysis model because it was strongly correlated with withdrawal time (Pearson correlation coefficient = 0.82, 95% CI 0.78–0.86). First, we evaluated if these variables could fulfill the definition of a mediator provided by Baron and Kenny. 17 A variable is considered a mediator (M) if it can satisfy the following three criteria: (a) x (the independent variable, i.e. the insertion method (WE vs AI)) significantly predicts y (the dependent variable; i.e. ADR in this study); (b) x significantly predicts M, and (c) M significantly predicts y controlling for x. Second, the PROCESS macro for SPSS, offered by Preacher and Hayes 18 was used to assess mediators of the association between insertion method and ADR, adjusting for age. A bootstrapping method with 5000 bootstrap resamples was used in the present study to calculate the bias-corrected 95% CI around the mediated and direct effects.
Results
Inter-rater reliabilities assessed by the Shrout-Fleiss reliability index listed in decreasing order of agreement are shown in Table 1. Parameters showing distraction: frequency and time of water suction; frequency and time of spasm; frequency of lens cleaning; withdrawal time; withdrawal technique scores: adequacy of fold examination, distention and cleansing; and parameters showing yield: number and duration of interventions had perfect or almost perfect agreement.
Characteristics of the patients included in the video analysis.
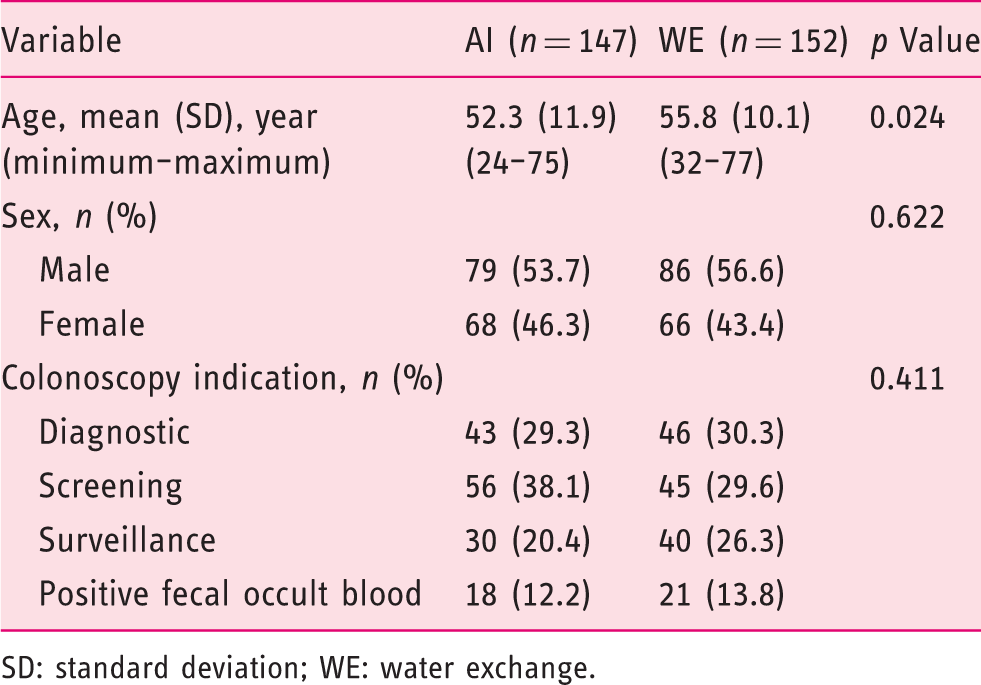
SD: standard deviation; WE: water exchange.
Bowel preparation quality scores, withdrawal technique, distractions, and diagnostic yield.
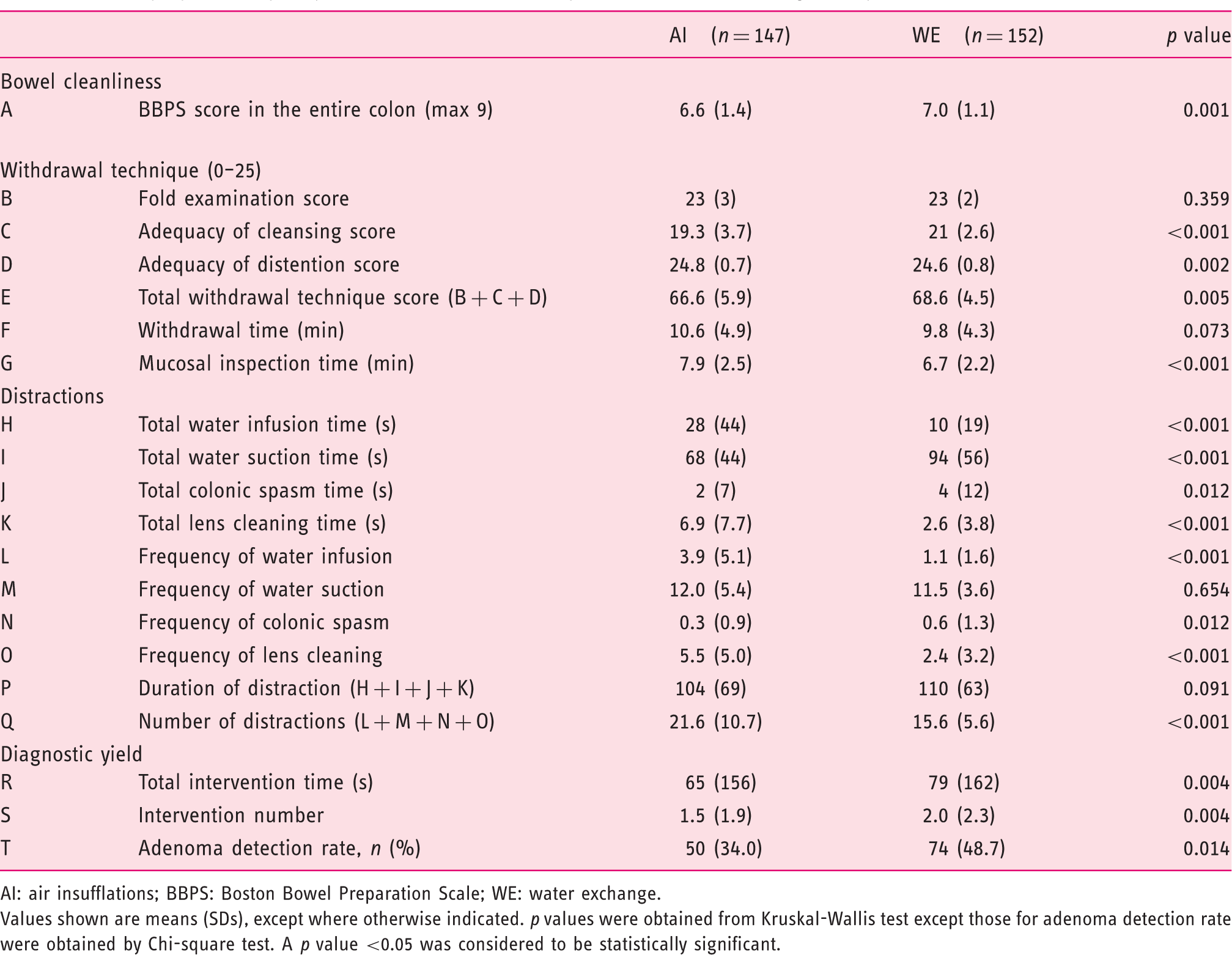
AI: air insufflations; BBPS: Boston Bowel Preparation Scale; WE: water exchange.
Values shown are means (SDs), except where otherwise indicated. p values were obtained from Kruskal-Wallis test except those for adenoma detection rate were obtained by Chi-square test. A p value <0.05 was considered to be statistically significant.
Multiple logistic regression analysis showed that the number of distractions was significantly and independently associated with ADR (odds ratio = 0.96 per distraction, 95% CI 0.92–0.99, p = 0.021), adjusting for withdrawal time and age. Figure 2 shows the results of multiple mediation analysis. The number of distractions and withdrawal time fulfilled the requirements for mediators, and were further evaluated with a multiple mediation analysis. An examination of the specific indirect effects indicated that the number of distractions and withdrawal time were mediators because their 95% CIs did not contain zero.
Multiple mediation model of the association between insertion method and adenoma detection. WE: water exchange, AI: air insufflation.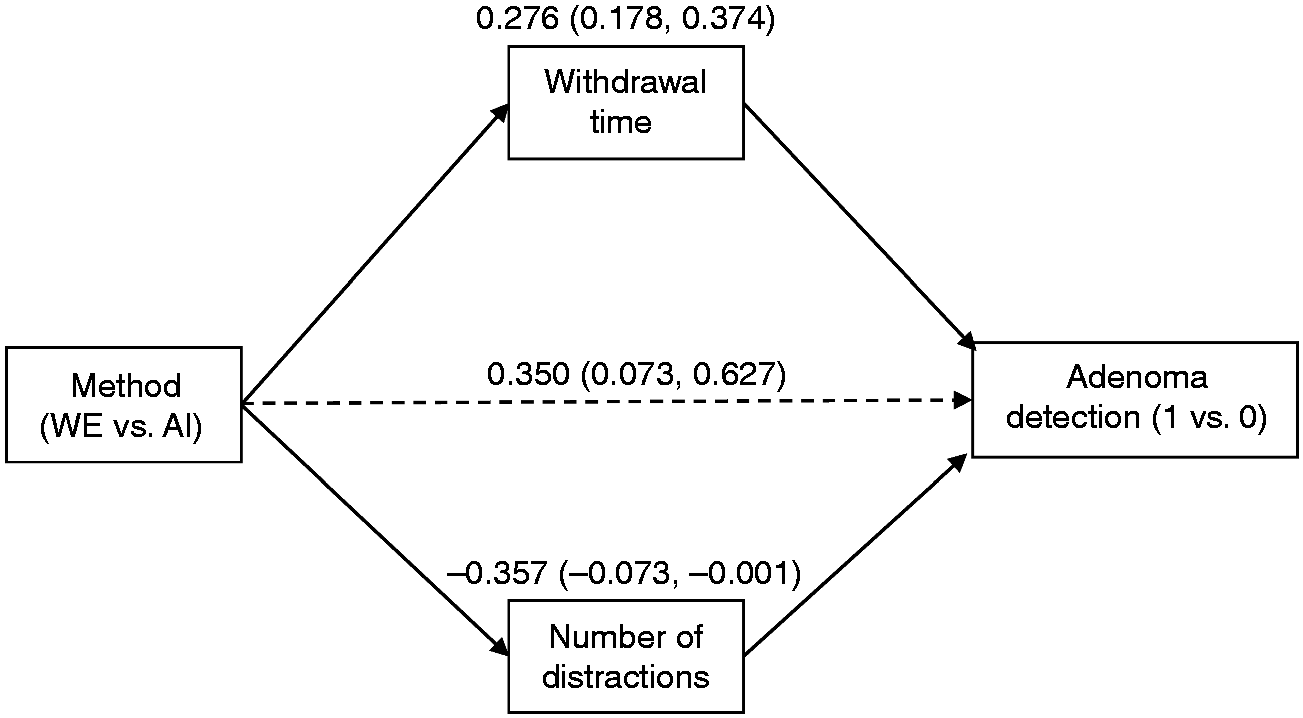
Discussion
The most important new finding in the current study is that WE had a significantly lower number of distractions during withdrawal. Confirmation of the published results of better bowel cleanliness (higher BBPS scores) and significantly higher diagnostic yield, i.e. time and number of intervention and ADR, and a significantly shorter mucosal inspection time added validity to the observations.
For almost a decade, the novelty of WE did not garner the full endorsement of editorialists and commentators. Concerns over WE included: (a) lengthy procedure time; 19 (b) insufficient evidence that WE was superior to water immersion (WI); 20 (c) the distinction between WI and WE was less important than what advocates of WE had claimed; 21 (d) a single colonoscopist's significant observations required confirmation by others; 22 (e) whether the results for WE could be demonstrated by others? 23 These concerns have been adequately addressed.6,12 A non-WE core group of investigators published a report 6 confirming the efficacy of WE in reducing insertion pain.1–5 A network meta-analysis, believed to be highest quality of evidence, reported that WE colonoscopy most effectively increased ADR. 12 An accompanying editorial commented that expert endorsement, a prerequisite to general acceptance, marked a significant milestone in the history of WE. 24
Traditional AI emphasizes expeditious arrival to the cecum. The method necessitates cleaning during withdrawal, multitasking at a time when inspection for lesions should be the most important task. Multitasking adversely affects the performance of the primary duty, often without awareness of the operator.25–27 Multitasking is not as efficient as focused work performed on a single task, and distracted subjects exhibit impairment when asked to perform even very simple tasks at the same time. 28 Although withdrawal cleansing is a long-accepted “routine” part of AI, accounting for up to 19.2% of the total withdrawal time, 29 interrupting mucosal inspection with cleansing maneuvers during withdrawal lowers the diagnostic yield compared with WE. WE compartmentalizes the two tasks, with bowel cleansing during insertion and searching for polyps during withdrawal, obviating the drawbacks of withdrawal multitasking. Thus, WE provides focused inspection evidenced by fewer distractions from the main task of searching for polyps.
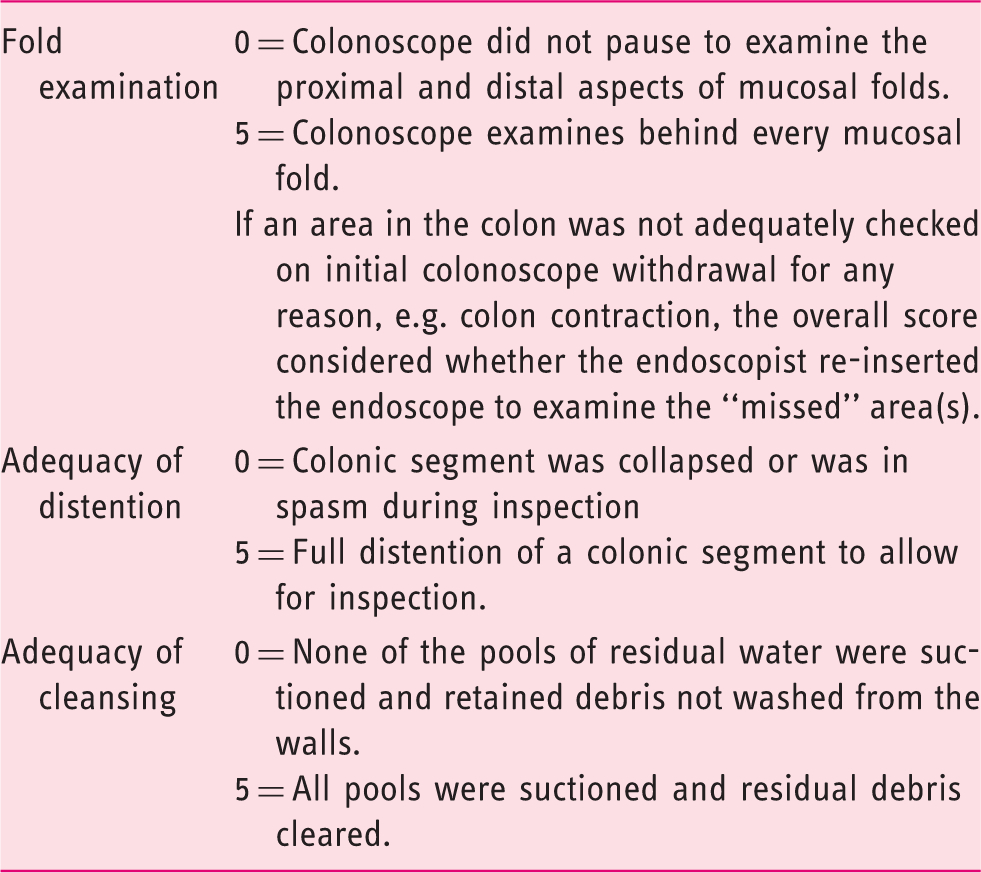
Uncontrolled observational studies have reported conflicting impacts of withdrawal time and withdrawal technique30,31 on ADR in colonoscopies performed with AI. In the current study, withdrawal time, as well as mucosal inspection time, exceeded the quality standard of six minutes in both groups. Paradoxically, WE had a shorter mucosal inspection time, but higher ADR. The withdrawal technique scores varied between the two groups despite the best efforts of the colonoscopists to perform optimal withdrawal, reflecting the possibility that the withdrawal techniques might be influenced by the insertion methods. WE had higher withdrawal technique scores, of which most came from higher adequacy of cleansing scores. Compared with AI, there were fewer pools of water or residual debris in the lumen during the withdrawal phase after WE insertion, so it was easier to clear them and to achieve a higher cleansing score. A recent European RCT reported that split-dose bowel preparation could significantly increase ADR from 40.9% to 53.0%. 32 In the current study, even though all patients were given similar instructions, suboptimal compliance with split-dose regimen due to barriers 32 might explain why use of WE could still achieve better bowel cleanliness than AI.
Distractions from mucosal inspection that occur during colonoscope withdrawal may play a role in negatively impacting the ADR outcome, 13 Our data revealed that the WE group had a significantly lower frequency of suction but significantly longer total duration of suction. Insertion suction aspiration of water by WE removed most scattered pools of water and residual stools. Some of the infused water flowed to the dependent parts of the colon, such as around the splenic flexure and descending colon, which was removed more efficiently in fewer sessions, albeit of longer duration. Lens cleaning was a component of distraction not previously ascribed such a role by Yung et al. 16 The lens blurred by dirty fluid or stools impaired inspection. During cleaning of the lens, the colonoscopist could not be examining for lesions as well.
Multiple logistic regression analysis showed that the number of distractions was significantly and independently associated with a low ADR. However, logistic regression analysis is not an appropriate statistical method to determine whether the number of distractions was a mediator in the association between insertion method and ADR. Therefore, multiple mediation analysis was conducted, and the results indicated that the number of distractions and withdrawal time were mediators in the association between insertion method and ADR. Our findings appear to support the notion that the enhanced ADR observed in WE, compared to AI, could be explained by a significant relationship between withdrawal time and number of distractions during withdrawal inspection.
Mucosal inspection time is a component of withdrawal time. Use of WE showed significantly shorter inspection time than AI, suggesting that the inspection with few distractions is more efficient. The efficiency was demonstrated in the significantly higher ADR with WE despite a shorter inspection time. The significantly shorter inspection time contributed to the shorter withdrawal time with WE, although the difference was not significant.
It is intuitive to interpret the current findings that a higher BBPS score by WE should be seen as a “promoter” or “facilitator” of a withdrawal phase with less distractions leading to a higher ADR. After insertion using WE, withdrawal has less distractions because the colon is cleaner (compared with AI), therefore, in particular, better bowel cleanliness contributes to an increase in ADR by WE. From a statistical point of view, however, withdrawal technique and BBPS scores are related (Pearson correlation coefficient = 0.75, 95% CI 0.69–0.79). BBPS was closely related to insertion method, being significantly higher with WE than with AI in several earlier reports.7–9,12 Thus BBPS score per se was not a significant independent factor in the logistic regression analysis.
Several limitations should be mentioned. Only one blinded reviewer performed the evaluations. The video reviewer did not independently verify if blinding was adequate by double-checking that correct guessing of the insertion method was <50%. The mean age of the WE group was older, possibly contributing as a confounding factor to the higher ADR. Another limitation is the assumption that mucosal inspection was taking place when no other defined distraction was present. Other potential distractions unrelated to the video images were not included in the analysis.
This study has some strengths. Overall, the scoring systems had a high inter-rater reliability, reinforcing the validity of these findings,13,16 The video recordings were edited to remove the insertion phase, to mimic the study 9 in which the withdrawal colonoscopists could be adequately blinded by their lack of knowledge of the insertion methods. The data in the current study filled the gap in our knowledge which even experts considered worth invoking as a plausible explanation of the beneficial effect of WE. 12
In summary, it had been several years since many researches wondered if the higher ADR by WE was due to less distractions, better colon cleanliness, or other factors (e.g. polyps less flattened and floating toward the lumen during insertion). 12 The current analysis suggests an important role for minimized distractions rather than improved bowel cleanliness per se accounting for the increased ADR with WE. The hypothesis that polyps are less flattened and floating toward the lumen during insertion remains to be tested in future studies.
In conclusion, the speculation by experts that reduction of multitasking distractions underlies the significantly higher ADR of WE is supported by the current study. Increased bowel cleanliness did not contribute to the increased ADR by WE.
Study highlights
What is our current knowledge?
Water exchange (WE) increases adenoma detection rate (ADR) as compared to air insufflation (AI) during colonoscopy. How WE enhances ADR is not fully understood.
What is new here?
Compared to AI, WE had significantly fewer distractions, higher ADR, and better bowel cleansing. Distractions and withdrawal times are significant mediators of the impact of WE on ADR.
Footnotes
Acknowledgements
This work was presented in part at the Digestive Disease Week, Chicago, Illinois, USA, 6–9 May 2017. The following author contributions were made: FWL and YHH defined the research theme, designed methods, interpreted the results and wrote the article. YHH and CWT performed and recorded the endoscopic examinations. YHH and HWY validated the video analysis method. HWY performed the video analysis. YHH, MK, and FWL analyzed the data. MK performed the logistic regression and multiple mediation analyses and assisted with interpretation of the results and writing of the article. All authors revised the manuscript critically for important intellectual content, and all authors read and approved the final version to be published.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Financial disclosure
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
The study was approved by the Institutional Review Board of Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation (IRB B10302018) and registered at ClinicalTrials.gov ID: NCT02978664.
Informed consent
Written informed consent was obtained from each patient included in the study.