
Abstract
Background
A low adenoma detection rate (ADR) increases risks of interval cancers (ICs). Proximal colon flat polyps, e.g. serrated lesions (SLs), are difficult to find. Missed proximal colon flat lesions likely contribute to IC.
Aims
We compared chromoendoscopy with water exchange (CWE), water exchange (WE) and air insufflation (AI) in detecting adenomas in screening colonoscopy.
Methods
After split-dose preparation, 480 veterans were randomized to AI, WE and CWE.
Results
Primary outcome of proximal ADR (55.6% vs 53.4% vs 52.2%, respectively) were similar in all groups. Adenoma per colonoscopy (APC) and adenoma per positive colonoscopy (APPC) were comparable. Detection rate of proximal colon SLs was significantly higher for CWE and WE than AI (26.3%, 23.6% and 11.3%, respectively, p = 0.002). Limitations: single operator; SLs only surrogate markers of but not IC.
Conclusions
When an endoscopist achieves high-quality AI examinations with overall ADR twice (61.6%) the recommended standard (30%), use of WE and CWE does not produce further improvement in proximal or overall ADR. Comparable APC and APPC confirm equivalent withdrawal inspection techniques. WE alone is sufficient to significantly improve detection of proximal SLs. The impact of increased detection of proximal SLs by WE on prevention of IC deserves to be studied. This study is registered at ClinicalTrial.gov (NCT#01607255).
Key summary
Summarize the established knowledge on this subject.
Missed lesions contribute to interval colon cancer, especially in the proximal colon. Water exchange colonoscopy (WE) improves the overall and proximal adenoma detection rate (ADR). Proximal sessile serrated lesions may contribute to interval cancers through a different accelerated pathway. What are the significant and/or new findings of this study?
For colonoscopists with a high ADR using air colonoscopy, the use of WE did not further improve the overall or proximal ADR. WE colonoscopy significantly improved the detection rate of sessile serrated lesions in the proximal colon.
Introduction
Traditional colonoscopy with air insufflation (AI) can fail to detect significant colorectal neoplasia, including some cancers, and it is less effective at reducing mortality from proximal colon cancers. 1 Missed lesions may account for the majority of interval cancers (ICs) in patients of colonoscopists with a low adenoma detection rate (ADR). 2 ADR is defined as the proportion of patients with at least one adenoma of any size. Low ADR increases the risk of ICs, which tend to cluster in the proximal colon. A 1% increase in overall ADR is associated with a 3% reduction in risk of IC. Aside from adenomatous polyps, other premalignant lesions important to identify include serrated lesions (SLs),3,4 which tend to cluster in the proximal colon. Proximal colon hyperplastic polyps (HPs), with a different pathology compared with distal HPs, are more closely related to sessile serrated adenoma/polyps (SSAs/Ps).3,4 Collectively proximal serrated lesions (SLs: SSA/Ps/traditional serrated adenomas and proximal colon HPs) are linked to proximal colon cancers through a pathway different from the conventional adenoma-carcinoma sequence. Thus, methods that can reduce IC must be able to at least enhance detection of lesions in the proximal colon. 5 The predominantly flat, proximal SLs may be more difficult to identify by endoscopy with AI. As missed lesions they may also contribute to ICs.
Water exchange (WE) has been shown to increase ADR compared with AI. In a retrospective analysis, 6 meta-analysis 7 and randomized controlled trials (RCTs),8–10 WE consistently increased overall ADR. WE can improve bowel cleanliness with salvage cleansing during scope insertion, thus resulting in less distraction from activities linked to cleaning (irrigation and suction) on scope withdrawal as compared with AI.11,12 This improves the detection of even diminutive lesions, especially in the proximal colon, where bowel cleanliness is likely to be suboptimal. 6
Prior studies of chromoendoscopy (0.2% indigo carmine) using a dye spray method suggested an improved overall ADR13,14 but dye spray can be tedious. We reported a controlled study comparing the effect of combined chromoendoscopy (0.008% indigo carmine) with water exchange (CWE) vs WE alone and showed that there was a significant increase in overall ADR and proximal ADR by CWE.15,16 Combining chromoendoscopy with WE addresses some of the potential drawbacks of performing dye spray chromoendoscopy with traditional AI.
In this study we performed a three-arm, prospective RCT comparing the use of CWE vs WE vs AI in screening colonoscopy with the primary outcome of proximal colon ADR. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution's human research committee. This study was funded by the Veterans Administration (VA), approved by the ethical review board VA Institutional Review Board on January 10, 2012, and registered with ClinicalTrial.gov (#NCT01607255) May 20, 2012, VA Northern California, Health Care System, IRB.
Method
From May 2013 to July 2017, 480 veterans were prospectively randomized (Figure 1). Inclusion criteria were patients between age 50 and 75 years with no prior history of colonoscopy within 10 years. Indications included healthy (American Society of Anesthesiologists (ASA) I–II) asymptomatic individuals referred for outpatient colorectal cancer (CRC) screening, those with a positive family history of colon cancer, and a few patients (n = 6, CWE 1, WE 4 and AI 1) with a positive fecal immunochemical test performed for CRC screening. Exclusion criteria included refusal to give consent, failure to keep colonoscopy appointment, history of colonoscopy or colonic polyp within the previous 10 years, significant comorbidity (ASA III or IV), prior colon surgery or inflammatory bowel disease.
Consolidated Standards of Reporting Trials flowchart.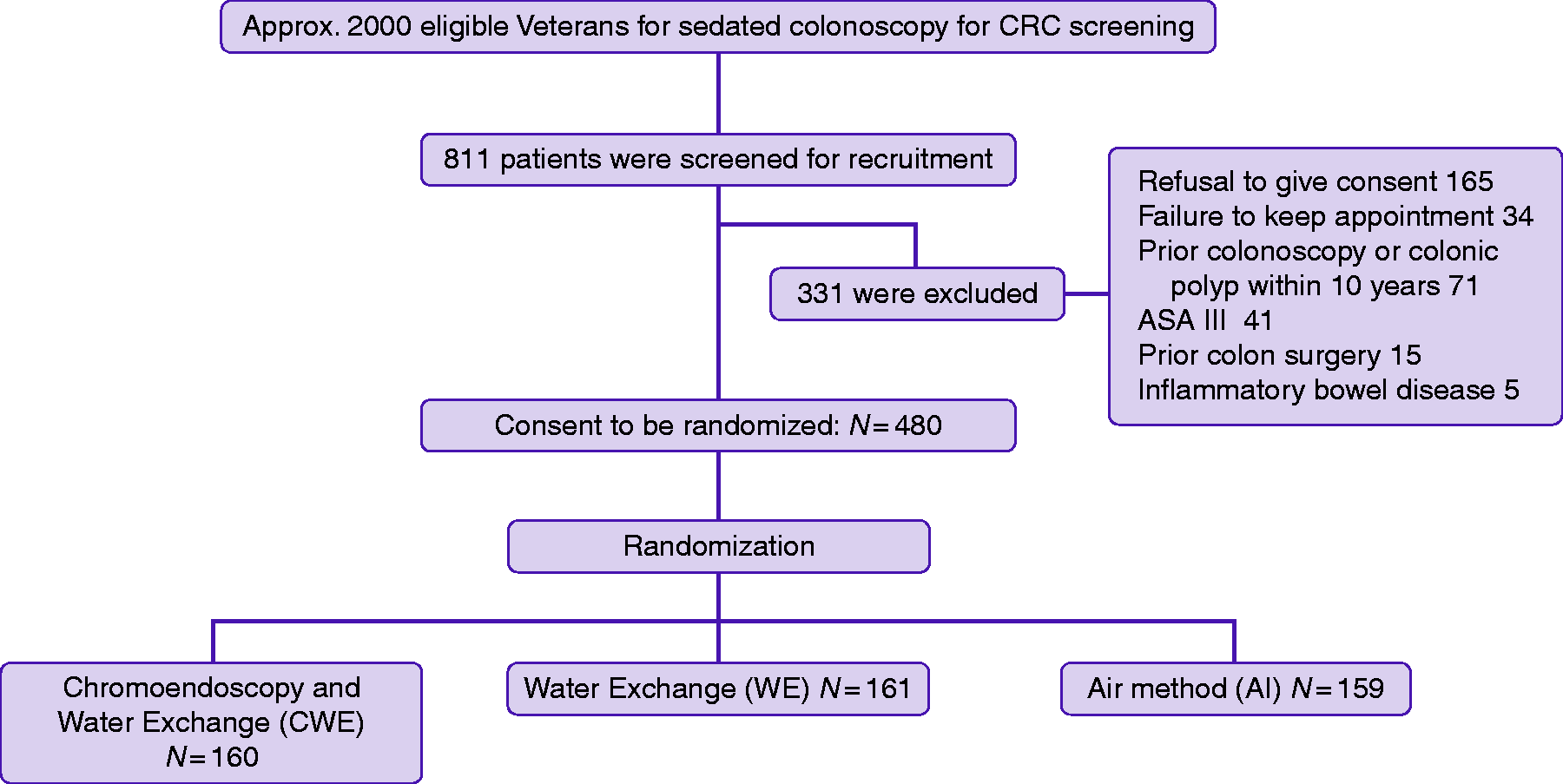
Bowel preparation in the proximal colon is often suboptimal, especially among veterans with diabetes and those on narcotic pain medications. At regular weekly open-access classes, patients were educated on bowel preparation before colonoscopy. All patients received four liters of polyethylene glycol 3350 and electrolytes oral solution as a split-dose bowel preparation. In the education class, patients were informed of the available research study and those who agreed to participate were contacted by the study coordinator to determine suitability for enrollment. Information on the study and informed consent were mailed to the patient.
The day of colonoscopy, patients were given the opportunity to ask questions before they were asked to provide consent for the colonoscopy and research study. Written, informed consent was obtained from each patient included in the study. Blood was taken before and after the colonoscopy to monitor serum electrolytes (Na+ and K+).
The patient was placed in the left lateral position for the colonoscopy. A towel covered their eyes to maintain blinding. All patients received intravenous (IV) moderate sedation with an initial combination of 25 μg fentanyl and 1 mg midazolam with incremental doses up to 75 μg fentanyl and 3 mg midazolam and a single dose of 25–50 mg of diphenhydramine. The randomization sequence was generated by computer and the assignment of intervention was stored in a sealed opaque envelope that was opened just before scope insertion to avoid bias.
Bowel prep score under water (UWBPS) and under air (UABPS) examination a .
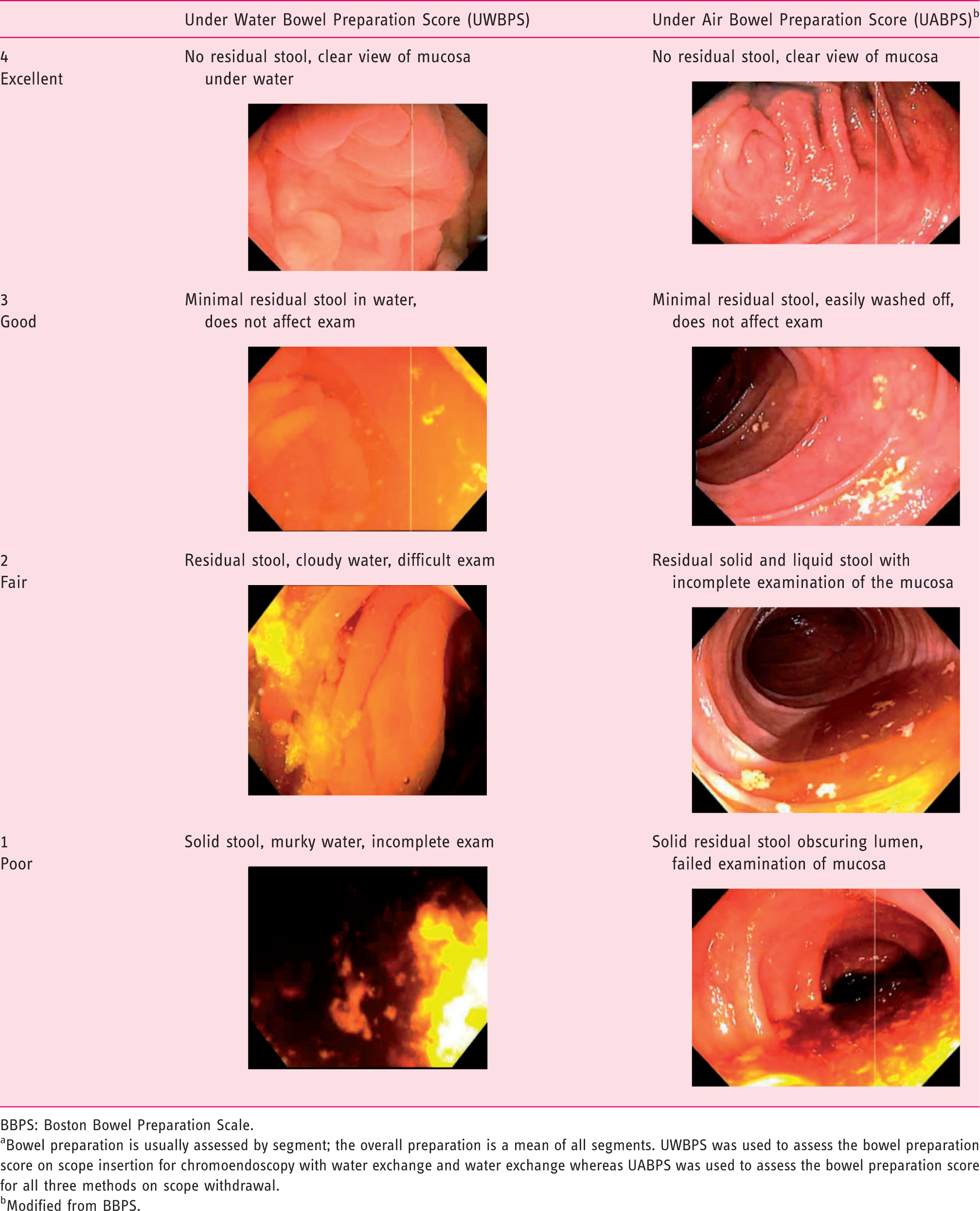
BBPS: Boston Bowel Preparation Scale.
Bowel preparation is usually assessed by segment; the overall preparation is a mean of all segments. UWBPS was used to assess the bowel preparation score on scope insertion for chromoendoscopy with water exchange and water exchange whereas UABPS was used to assess the bowel preparation score for all three methods on scope withdrawal.
Modified from BBPS.
Colonoscopy methods
AI was performed with minimal air on scope insertion and regular scope shortening. Abdominal compression was applied by the technician at the request of the endoscopist. Water was used for irrigation when residual stool was encountered, and residual water was removed with suction on scope withdrawal.
WE was performed with the air button turned off. Water was infused and suctioned (exchange) to facilitate scope insertion until the cecum was reached by identifying the appendix opening under water, seeing the ileocecal valve and touching the cecal floor. The residual water was removed with suction and air was used on scope withdrawal to facilitate examination. 15 Removal of the infused water and residual debris was implemented predominantly during insertion.
CWE used a dilute indigo carmine (0.008%) solution instead of plain water. The method of scope insertion and withdrawal was the same as for WE.16,17
Polyps were removed using biopsy forceps (<5 mm), cold snare (5–8 mm) or hot snare (>8 mm). All resected lesions were placed is separate specimen jars for histopathologic assessment.
Statistics
Based on our pilot data 16 to show a difference of 19% between the study (CWE) and control group (WE), power calculation indicated that 160 patients would be required in each group. At the recommendation of grant reviewers, an AI group was added as a conventional control arm, therefore a total of 480 patients were recruited for the study. Chi-squared test, unpaired t-test, Wilcoxon rank sum test, Fisher exact test, Kruskal-Wallis test and analysis of variance were used for data analysis. A p value of < 0.05 was considered significant.
Results
Patient demographics.
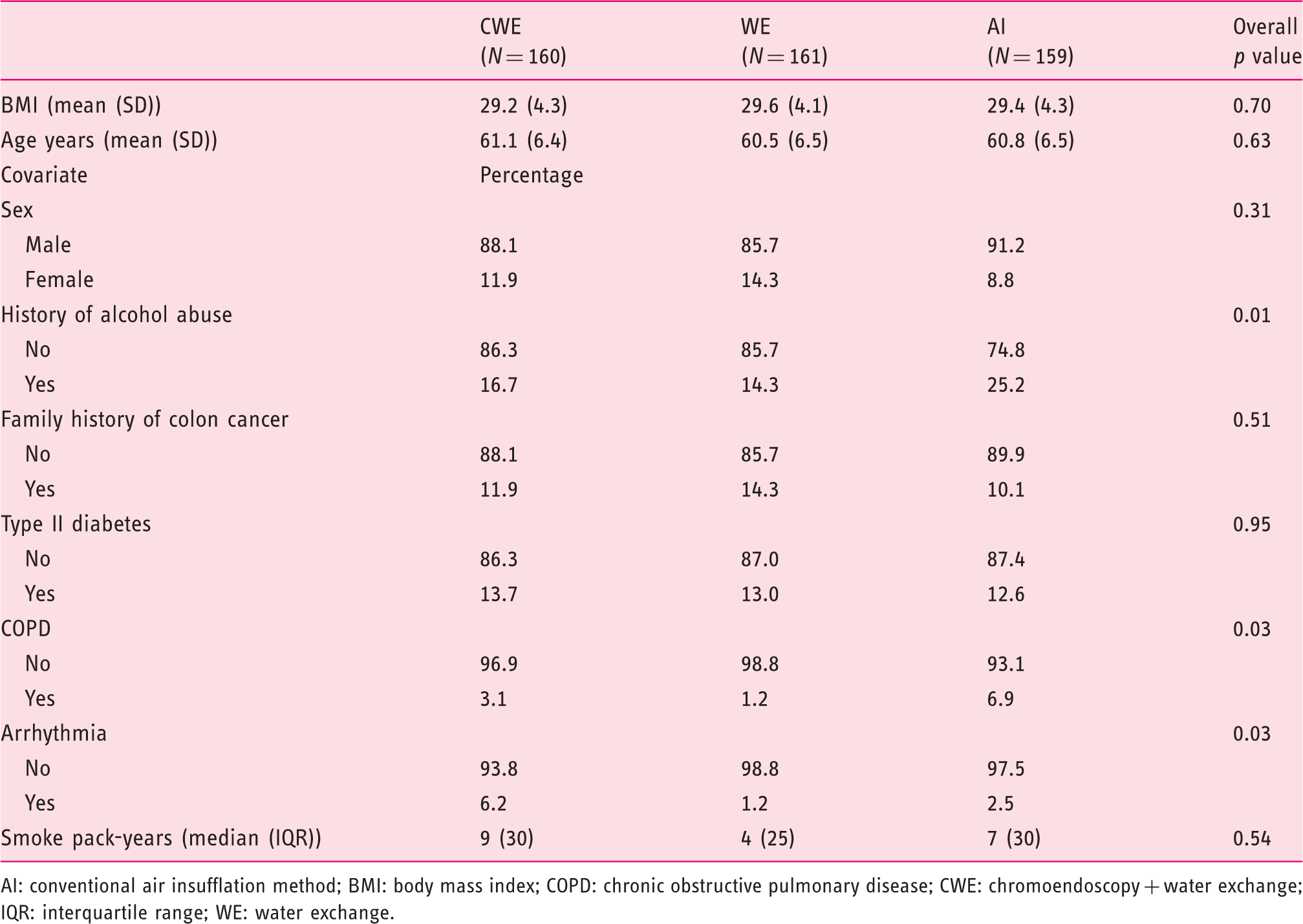
AI: conventional air insufflation method; BMI: body mass index; COPD: chronic obstructive pulmonary disease; CWE: chromoendoscopy + water exchange; IQR: interquartile range; WE: water exchange.
Procedure characteristics.
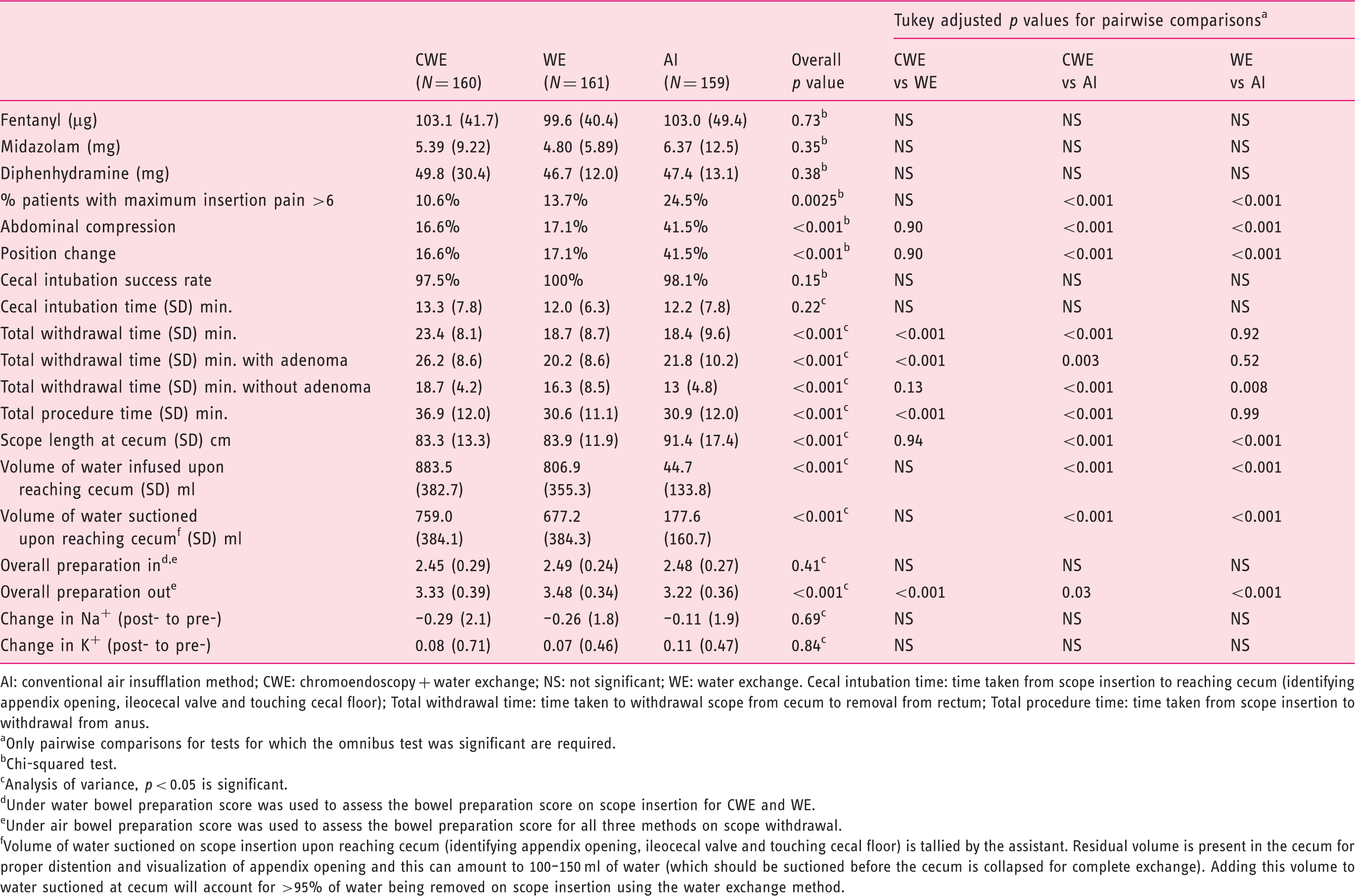
AI: conventional air insufflation method; CWE: chromoendoscopy + water exchange; NS: not significant; WE: water exchange. Cecal intubation time: time taken from scope insertion to reaching cecum (identifying appendix opening, ileocecal valve and touching cecal floor); Total withdrawal time: time taken to withdrawal scope from cecum to removal from rectum; Total procedure time: time taken from scope insertion to withdrawal from anus.
Only pairwise comparisons for tests for which the omnibus test was significant are required.
Chi-squared test.
Analysis of variance, p < 0.05 is significant.
Under water bowel preparation score was used to assess the bowel preparation score on scope insertion for CWE and WE.
Under air bowel preparation score was used to assess the bowel preparation score for all three methods on scope withdrawal.
Volume of water suctioned on scope insertion upon reaching cecum (identifying appendix opening, ileocecal valve and touching cecal floor) is tallied by the assistant. Residual volume is present in the cecum for proper distention and visualization of appendix opening and this can amount to 100–150 ml of water (which should be suctioned before the cecum is collapsed for complete exchange). Adding this volume to water suctioned at cecum will account for >95% of water being removed on scope insertion using the water exchange method.
Outcome measures.
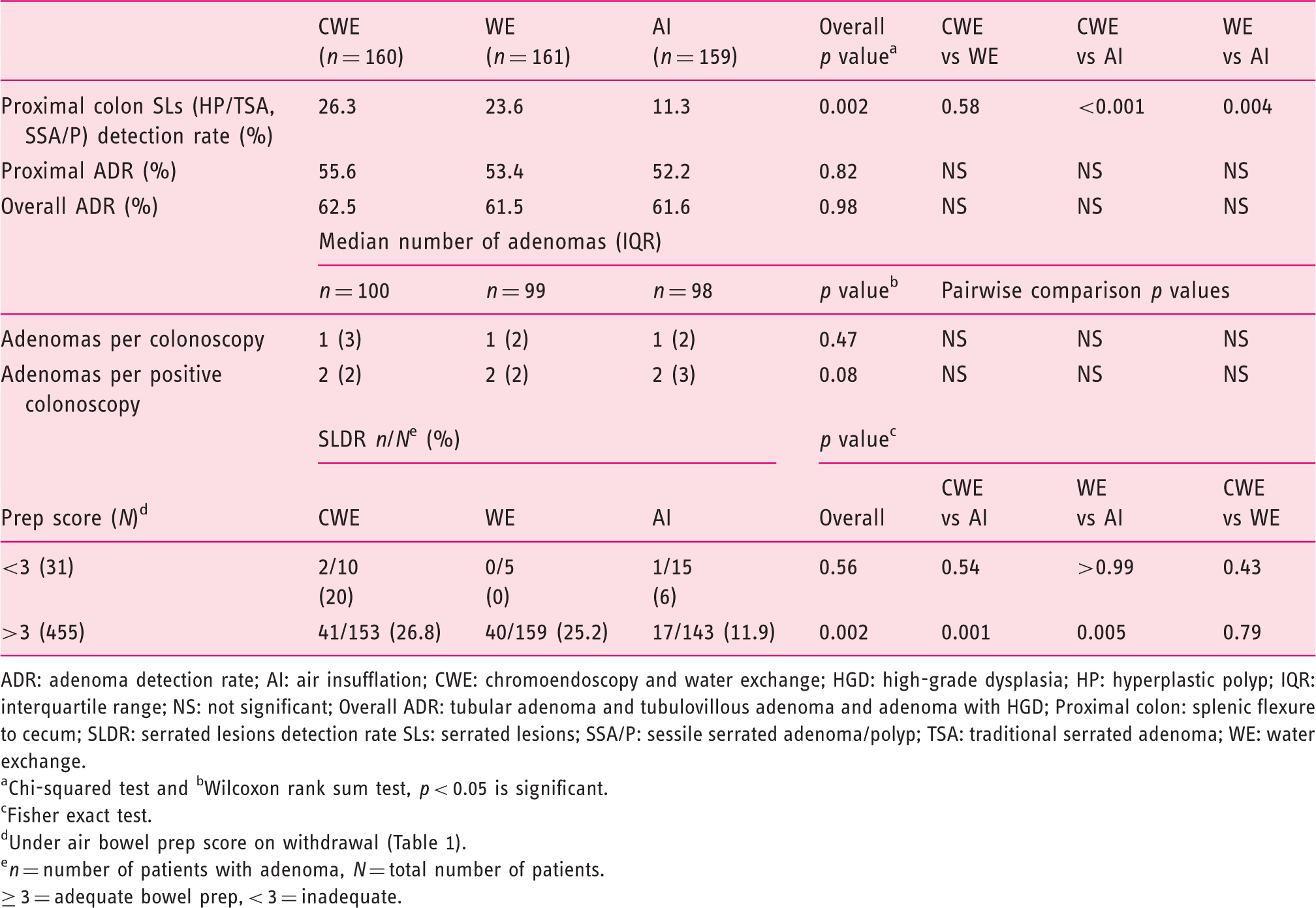
ADR: adenoma detection rate; AI: air insufflation; CWE: chromoendoscopy and water exchange; HGD: high-grade dysplasia; HP: hyperplastic polyp; IQR: interquartile range; NS: not significant; Overall ADR: tubular adenoma and tubulovillous adenoma and adenoma with HGD; Proximal colon: splenic flexure to cecum; SLDR: serrated lesions detection rate SLs: serrated lesions; SSA/P: sessile serrated adenoma/polyp; TSA: traditional serrated adenoma; WE: water exchange.
Chi-squared test and bWilcoxon rank sum test, p < 0.05 is significant.
Fisher exact test.
Under air bowel prep score on withdrawal (Table 1).
n = number of patients with adenoma, N = total number of patients.
≥ 3 = adequate bowel prep, < 3 = inadequate.
The proximal colon serrated lesions detection rate (SLDR) were significantly higher for CWE and WE than AI (26.3%, 23.6% and 11.3%, respectively, p = 0.002), and there was a significant correlation between proximal colon SL detection rate and proximal withdrawal bowel preparation score.
Complications.
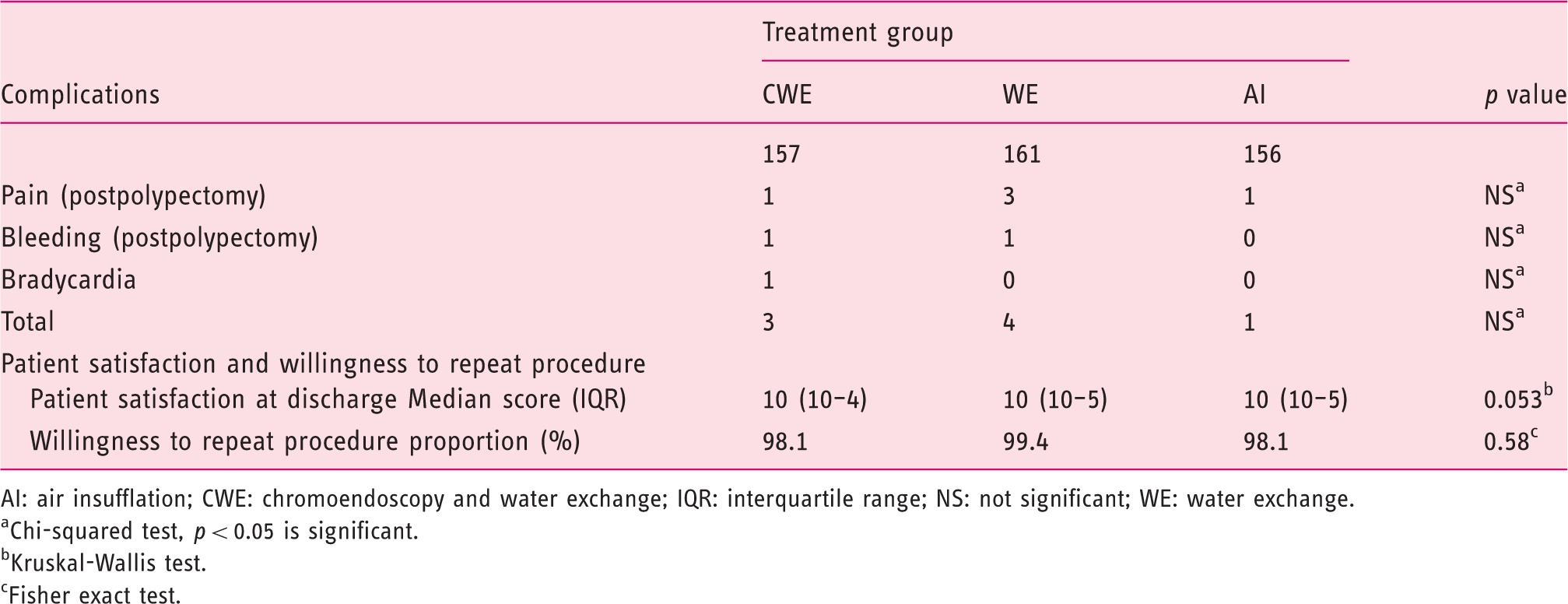
AI: air insufflation; CWE: chromoendoscopy and water exchange; IQR: interquartile range; NS: not significant; WE: water exchange.
Chi-squared test, p < 0.05 is significant.
Kruskal-Wallis test.
Fisher exact test.
Discussion
Investigator's overall adenoma detection rate in prior reported studies.
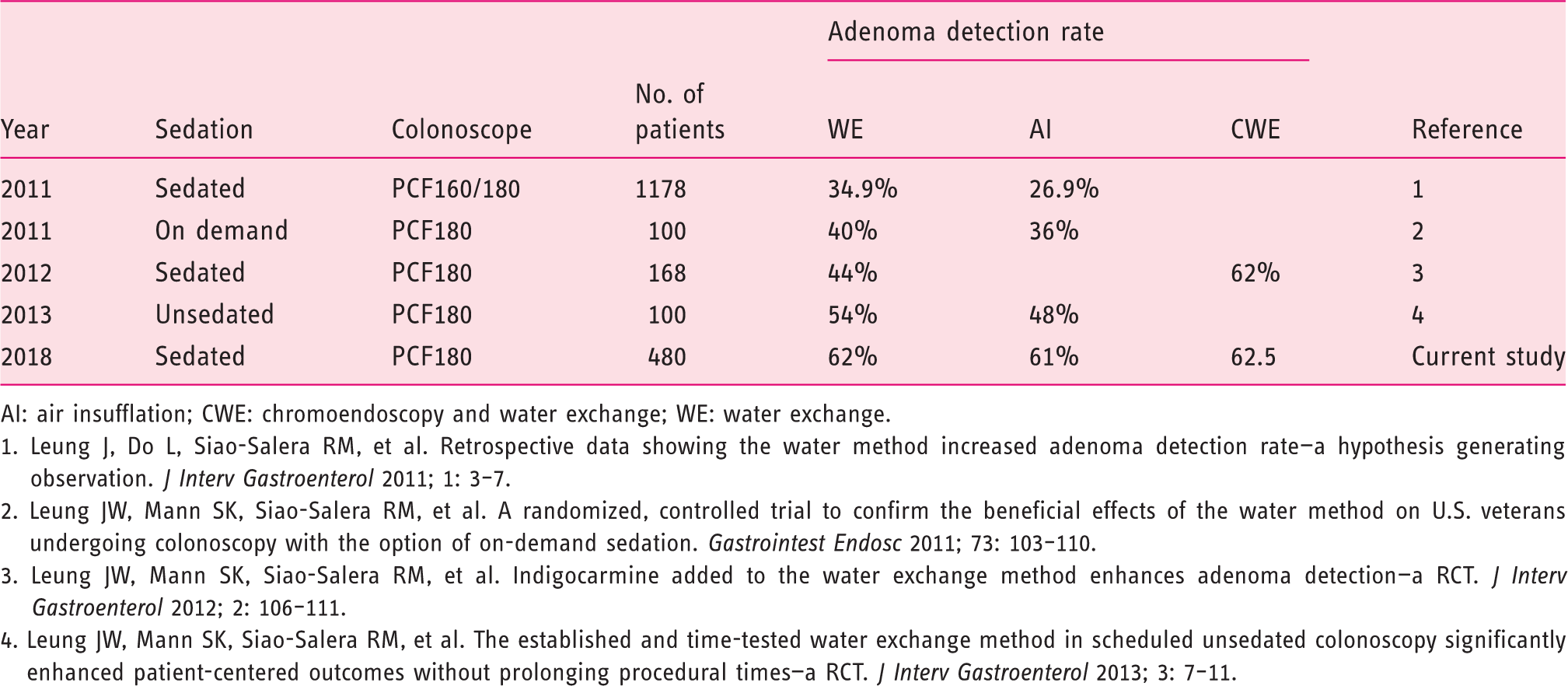
AI: air insufflation; CWE: chromoendoscopy and water exchange; WE: water exchange.
1. Leung J, Do L, Siao-Salera RM, et al. Retrospective data showing the water method increased adenoma detection rate—a hypothesis generating observation. J Interv Gastroenterol 2011; 1: 3–7. 2. Leung JW, Mann SK, Siao-Salera RM, et al. A randomized, controlled trial to confirm the beneficial effects of the water method on U.S. veterans undergoing colonoscopy with the option of on-demand sedation. Gastrointest Endosc 2011; 73: 103–110. 3. Leung JW, Mann SK, Siao-Salera RM, et al. Indigocarmine added to the water exchange method enhances adenoma detection—a RCT. J Interv Gastroenterol 2012; 2: 106–111. 4. Leung JW, Mann SK, Siao-Salera RM, et al. The established and time-tested water exchange method in scheduled unsedated colonoscopy significantly enhanced patient-centered outcomes without prolonging procedural times—a RCT. J Interv Gastroenterol 2013; 3: 7–11.
Important advances in the quality of colon cancer screening in 2017 included the following: A prospective Polish study confirmed previous retrospective findings that increased ADR was associated with a reduced risk of IC and death. 20 In an Italian multicenter, endoscopist-blinded RCT, split-dose bowel preparation significantly increased overall ADR (53.0% vs 40.9%). 21 Three RCTs evaluated the impact of WE on overall ADR measured as the primary outcome, and all three studies showed WE significantly increased overall ADR compared with AI.8–10 Despite the use of split-dose bowel prep, all three RCTs also showed a significant improvement in bowel cleanliness by WE compared with AI.
The overall ADR in the AI group in the current report is high, twice the recommended quality standard of 30% for men. The data suggested a ceiling effect; when the colonoscopist has achieved a high overall ADR with AI, the use of WE and CWE would not confer further improvement. WE has the benefits of reducing pain and need for assistance (abdominal compression and patient positioning) during the colonoscopy, suggesting that mastering the WE technique could achieve maximal quality improvement in ADR. The experience gained could also improve the ADR even with AI.
Previously, all CRCs were considered to arise from adenomas by the traditional adenoma-carcinoma sequence. Recently, several research studies have showed this pathway accounted for only about 60% of CRCs.4,22,23 Three or more distinct molecular pathways were thought to be related to CRC24,25 and up to 35% of CRCs developed from SLs 26 —a more rapid pathway27,28 and overrepresented in the IC subgroup. The detection of SLs at baseline screening was associated with an increased risk of interval neoplasia on surveillance colonoscopy. 29 A more recent report suggested that proximal HPs and SSPs irrespective of size were associated with an increase in synchronous advanced neoplasia in the colon. 30 However, detection of SLs remains a challenge for colonoscopists. These lesions are typically flat with indistinct borders and are located in the proximal colon where the bowel preparation quality may be poor; the surface is usually pale and may be obscured/concealed by stool debris or the mucous cap.4,31,32 As a result, SLs could be easily overlooked and incompletely resected, contributing to the development of IC. Adequate detection of SLs with complete removal is crucial to the prevention of serrated pathway-related CRC. Thus, the detection rate of proximal serrated polyps is emerging as one important quality indicator. The detection rate of SLs is variable among different endoscopists, ranging from 1% to 22%.33,34 Anderson et al. believe a benchmark of 11% should be appropriate. 35 In the current study, the effectiveness of CWE and WE is well demonstrated by the significantly higher detection rate of the even more subtle proximal colon SLs by CWE (26.3%) and WE (23.6%) over AI (11.3%). By enhancing the outline of underlying lesions, chromoendoscopy does improve the detection of smaller SLs, especially in the proximal colon. The lack of a significant difference in the detection rate of SL between CWE and WE conceivably could be a type II error due to small sample size.
In the current study we found that bowel preparation quality was not significantly different among the three groups during scope insertion but only on withdrawal, with WE and CWE having a better bowel preparation. We speculate that WE and CWE can increase the detection rate of SLs partly by optimizing the examination during scope withdrawal. The lack of statistically significant difference between CWE and WE suggests that WE alone is sufficient to improve the detection of proximal SLs. WE and CWE required suction removal of residual feces to improve visualization and to navigate the lumen during scope insertion resulting in fewer distractions from cleaning (irrigation and suction) on scope withdrawal, 36 and the more focused inspection could explain the higher yield of SLs when compared with AI. There was an added benefit of a “straighter” scope with less looping to achieve cecum intubation using WE. 37 Less looping and angulations compared with AI could improve scope tip control and enhance detection of flat lesions.
This RCT has several limitations. There was one single operator, with only veterans, primarily male, patients, and SLs were only surrogate markers of but not ICs. The bowel prep score under water has not been validated, especially when put head to head with that under air. This study has some strengths. It demonstrates that very high overall ADR can be achieved even with AI after adoption of WE, and WE can enhance the detection of more subtle lesions in the proximal colon.
Indigo carmine provides surface contrast that helps highlight even slight mucosal irregularities raising the suspicion of pathology and resulting in more biopsies and resection of normal tissue. Chromoendoscopy with indigo carmine remains a tedious process, even when combined with WE colonoscopy. Residual stool changes the effluent color green, which requires more exchange to allow examination with the blue highlight. This could partially explain the longer withdrawal times, even in exams without adenomas for CWE compared with WE and AI. Although CWE enhances detection of mucosal pathologies (including SLDR) compared with AI, similar detection rates were obtained with WE, and CWE did not offer significant additional benefits. We advocate the continued use of WE for colonoscopy in future studies.
In conclusion, compared with AI, both WE and CWE improved detection of proximal colon SLs significantly, even though the quality outcomes of high overall and proximal colon ADR of AI were not further surpassed. For colonoscopists with a low ADR, learning the WE method could potentially improve ADR even if AI is used after practice with WE. By virtue of increasing the detection of SLs in the proximal colon, the potential of WE in preventing proximal colon ICs deserves to be studied.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This work was supported by a VA Merit Review Grant. We received research support (via loan of colonoscope) from Olympus America. We acknowledge the support from Research Service of VANCHCS (J.W.L.) and VAGLAHS (F.W.L.). This project also was supported by the National Center for Advancing Translational Sciences, National Institutes of Health (NIH), through grant number UL1 TR001860. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Ethics approval
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution's human research committee.
Informed consent
Written, informed consent was obtained from each patient included in the study.