
Abstract
Introduction
Endoscopic submucosal dissection (ESD) is the gold-standard treatment for superficial lesions of the digestive tract. No medico-economic study has been conducted in Europe.
Material and methods
A monocentric study was conducted including all patients undergoing ESD between January 2015 and December 2017. The global cost of hospital stays was measured by microcosting, and revenue was based on the diagnosis-related group (DRG) system. The primary objective was to assess the cost/revenue balance. A medico-economic comparison with surgery was performed as a secondary outcome.
Results
A total of 193 patients were prospectively included. The cost per procedure was €3463.79, subtracted from a €2726.84 revenue, with a deficit of −€736.96 per stay. Presence of comorbidities/complications increasing DRG value was the only predictive factor for a positive budgetary balance in a multivariate analysis (odds ratio 49.21, 95% confidence interval 11.3–214.25, p < 0.0001). In comparison with surgery, ESD was associated with shorter length of stay (11 vs 2 days; p < 0.0001) and lower morbidity (28% vs 14%; p = 0.061), lower cost (€8960 vs €1770; p < 0.0001).
Conclusion
The ESD cost/revenue balance is negative in 80% of cases. Given the benefits of ESD in terms of patient morbidity and financial savings compared with surgery, the implementation of a specific ESD reimbursement is warranted.
Keywords
Key summary
Established knowledge on this subject
Endoscopic submucosal dissection (ESD) is the gold-standard treatment for superficial lesions of the digestive tract. No medico-economic study assessing the cost of this procedure for hospitals and reimbursement systems exists.
What are the significant and/or new findings of this study?
ESDs generate additional financial costs to hospitals. ESD medical devices account for the majority of the increased expenditure. ESDs ensure medical benefits to patients and lower cost compared with surgery.
Introduction
Endoscopic submucosal dissection (ESD) is the gold-standard treatment for superficial lesions of the digestive tract. 1 It allows resection of large lesions in a single piece, permitting complete histological analysis to examine the risk of lymph node metastasis. When the criteria for anatomopathological curability are met, this technique has the same treatment efficacy as surgical resection.
Despite growing scientific data on the efficacy and safety of this technique for patients with superficial lesions of the digestive tract, it is not widely performed in Western and European countries because of its high technical proficiency requirement, its steep learning curve and the absence of a medico-economic study assessing the cost of this procedure for hospitals and reimbursement systems.
No medico-economic study has emerged on the topic of ESD in Europe to date. Thus, the aim of this medico-economic study was to evaluate the cost/revenue balance of ESD with a cost analysis, as well as to compare ESD with surgery for similar lesions from medical and economic standpoints.
Materials and methods
Inclusion criteria and patient selection
We conducted a retrospective analysis of prospective collected data of all patients who underwent ESD at the Limoges University Hospital for superficial neoplasms from January 2015 through December 2017. This study was conducted after approval by the Regional Scientific Ethical Committee of Limoges University Hospital Center, January 20, 2018 (protocol number: 242-2018-08). French legislation on studies of anonymized retrospective data does not require informed consent.
Exclusion criteria
We excluded ESD procedures for submucosal lesions and neuroendocrine tumor.
Main objective
The primary aim of this study was to assess the cost/revenue balance for ESD with a cost analysis.
Secondary objectives
The secondary aims were as follows: (1) to assess the cost of sterile medical devices in the overall cost of ESD, (2) to analyze the predictive factors of a positive cost/revenue balance and (3) to compare ESD and surgery for colonic superficial neoplasms.
Primary endpoint
The primary endpoint of this study was to assess the cost/revenue balance for each ESD patient. The balance calculation is shown in Figure 1.
Budgetary balance calculation for endoscopic submucosal dissection (ESD).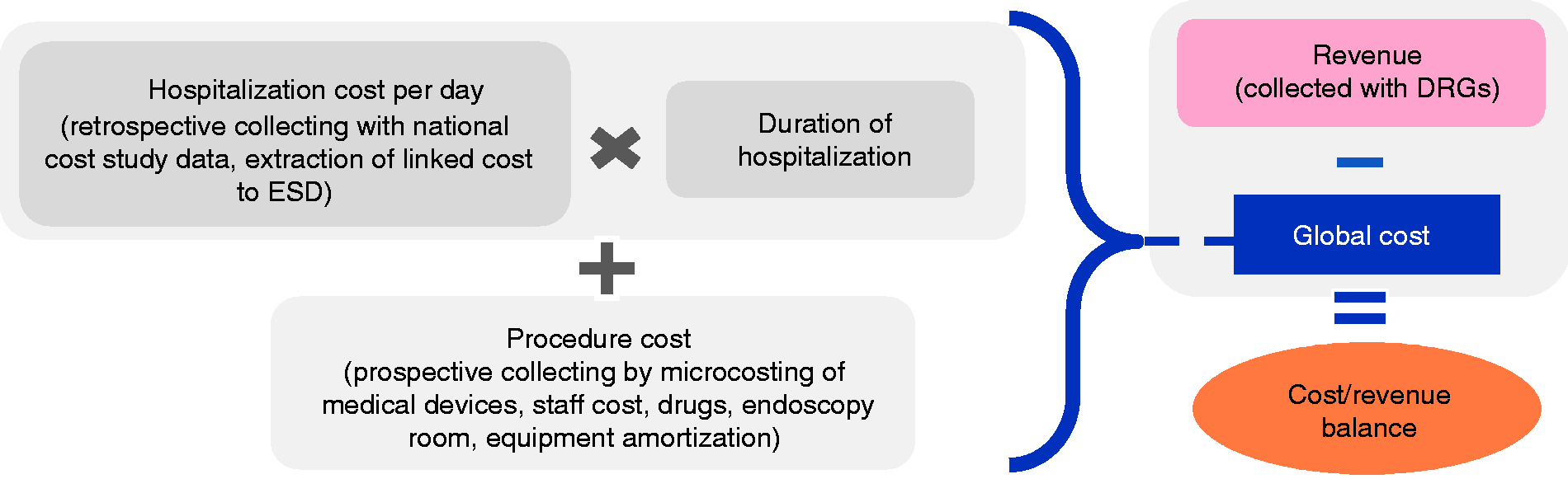
Hospital revenue collection
The diagnosis-related group (DRG)-based system for funding of patient hospital stays is used in France. As part of this system, a procedure can be funded in two ways. A specific procedure, such as surgery, can be classified according to specific variables and a specific revenue can be determined; if the procedure cannot be classified, the revenue depends on the main diagnosis. For ESD, which has no specific code, endoscopic mucosal resection (EMR) coding is used and funding depends on the anatomopathology and location of the lesion. Funding can be increased by presence of comorbidities/complications increasing DRG value (e.g. cirrhosis, diabetes, hemorrhage, heart failure).
Calculating the cost of a hospital stay for ESD
Our center is part of a national study (Etude Nationale des Coûts) assessing hospitalization costs for patients based on the DRG system. The costs associated with ESD were not taken into account in this study, as they are based on EMR coding and are thus underestimated. These costs include the following:
– Activities of the gastroenterology unit (medical staff, nurses, accommodation and maintenance) – Medical logistics (pharmacy, sterilization and biomedical engineering) – Drugs – Organization, logistics and management – Biology – Anatomopathology
Calculating the cost of ESD
Procedure costs were collected prospectively using microcosting. All spending was taken into account, from patient admission to the endoscopy unit to discharge. Procedure time was also registered prospectively. The cost of ESD included the following direct and indirect costs:
Direct costs
– Medical and paramedical staff activities during the procedure – Medical devices used during the entire procedure including endoscopy and anesthesia – Drugs used during the procedure
Indirect costs
– Amortization of endoscopy equipment – Endoscopy room, covering all charges related to the consumption of general or logistic supplies and accommodations
Secondary aims
The impact of the main characteristics of the hospital stay (surface > 1100 mm2, presence of cancer, presence of complications/comorbidities increasing DRG value) was first estimated using a univariate model, followed by a multivariate model. Next, the costs generated by medical devices were estimated and compared to the total cost of the procedure. Lastly, the clinical and medico-economic data from patients undergoing ESD were compared with those undergoing surgery for colonic superficial neoplasms (adenoma or adenocarcinoma T1a or T1b) in the same center from 2009 to 2017. All consecutive patients who were surgically treated during this period for superficial colonic lesion were retrospectively included thanks to an anatomopathological database. We stop the inclusion at January 2009 because before this period no expert physician was trained in our center for large, wild-field, piecemeal EMR or ESD and a lot of superficial colonic lesions were directly treated by surgical resection. Exclusion criteria were colectomy for another indication than superficial lesion, emergency colectomy or colectomy associated with another resection.
Statistical analysis
Quantitative data are expressed using the median and interquartile range, and qualitative data are expressed as numbers and percentages. Univariate comparisons were performed using Fisher test for qualitative variables and the Wilcoxon rank test for quantitative variables. Logistic regression was used for multivariate analyses and included data that were significant or close to significant in the univariate analysis. P values <0.05 were considered to indicate statistical significance. Data were analyzed using the open-source software R (version 3.0.2; 2013-09-25) and LATEX on platform i386-w64-mingw32.
Results
Clinical results
Clinical results for endoscopic submucosal dissection (means).
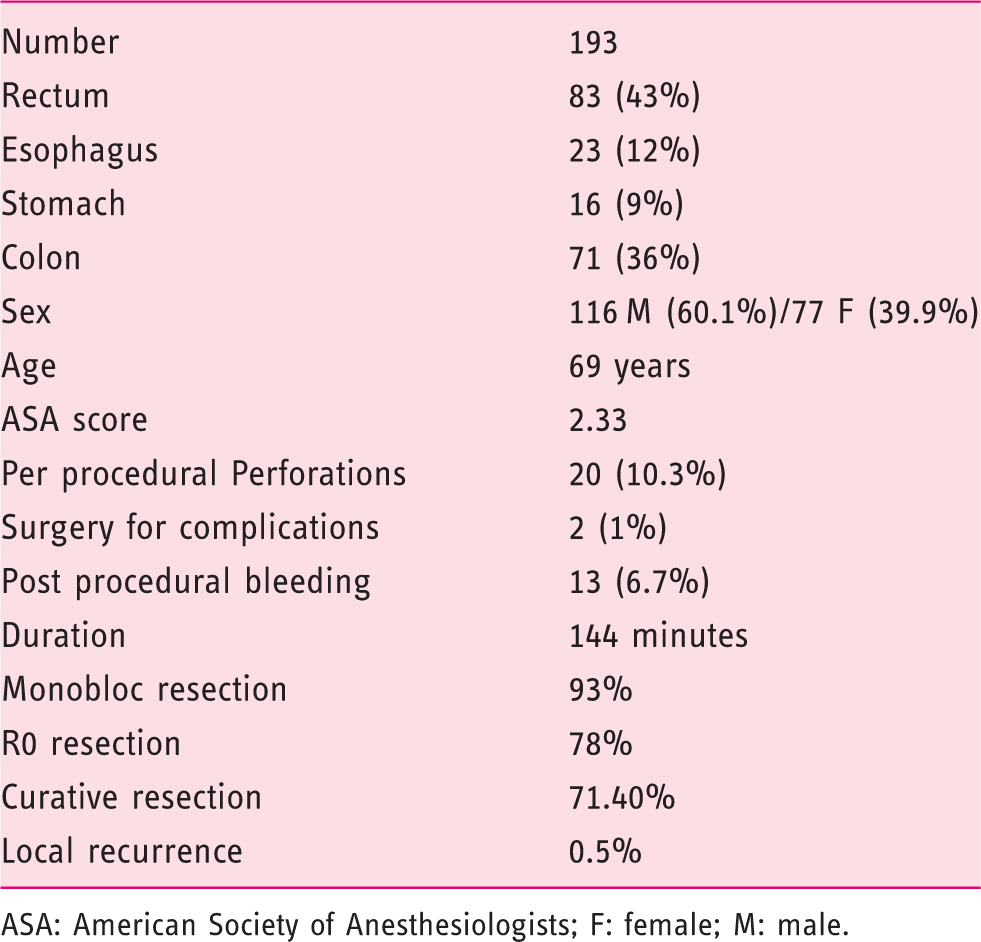
ASA: American Society of Anesthesiologists; F: female; M: male.
The average diameter of the lesions was 52.96 ± 18.3 mm. Two (1%) secondary postdissection perforations after large colonic ESD of the ascending colon with peritonitis required emergency surgical management.
Main objective: cost/revenue balance for ESD
Revenue from hospital stays
Of the 193 ESDs performed, 18 different DRGs were used depending on the location of the tumor, the final pathology and comorbidities or complications present. At Limoges University Hospital, the mucosectomy code was used depending on the location of the tumor. The mean revenue from these DRGs was €2726.84 per stay.
Cost from hospital stays
The cost of a hospital stay, excluding the cost of the ESD procedure, was retrospectively determined to be €1858.84. This cost includes the average cost of the day of hospitalization for ESD (€463.18), the average cost of anatomopathology (€191.86) and the average cost of drugs used outside of the procedure (€3.74).
Procedure cost
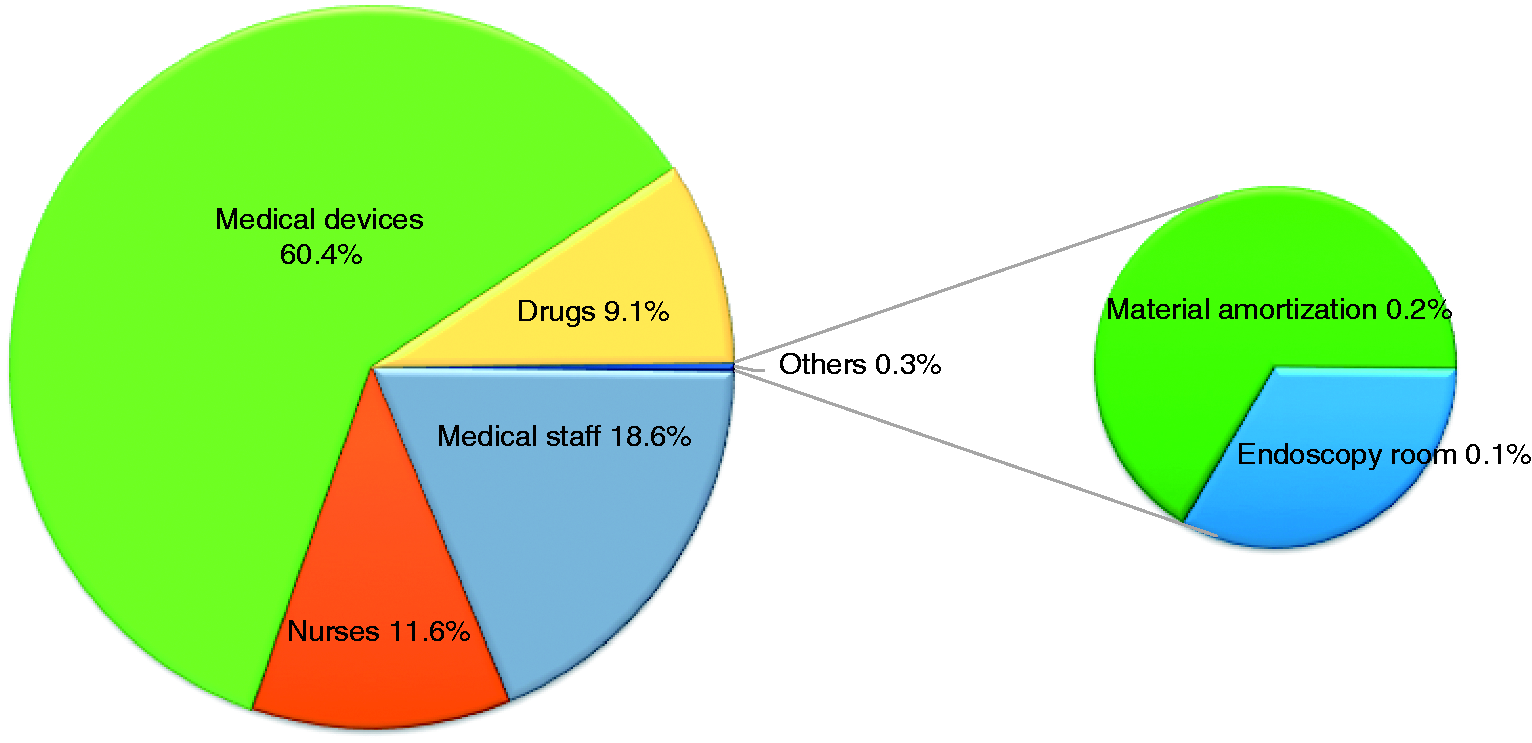
The procedure cost was prospectively determined to be €1604.96 ± 627 (Figure 2) and includes the following:'
– Medical and paramedical staff cost: €484.25 ± 275.13 per procedure – Medical devices cost: €970.78 ± 413.70 per procedure – Cost of drugs used during the procedure: €144.62 ± 26.02 per procedure – Interventional endoscopy room material cost: €3.45 per procedure – Cost related to endoscopy room: €1.85 ± €0.97 per procedure Part of expenditure item in the global cost of ESD.
Total cost
From the various costs mentioned above and given the average length of stay of 3.6 days, the average cost per stay was €3463.79 ± 1720.96.
Cost/revenue balance for the hospital
The hospitalization of 193 patients for ESD resulted in a total additional cost of €142,232.56 for the hospital, with an average cost/revenue balance of −€736.96 ± 1719 per stay. Figure 3 shows the average financial balance per stay according to anatomopathology and location of the lesion. In total, 157 (81.4%) stays had a financial deficit and 36 (18.6%) stays had financial balances in favor of the hospital.
Budgetary balance according to diagnosis-related group.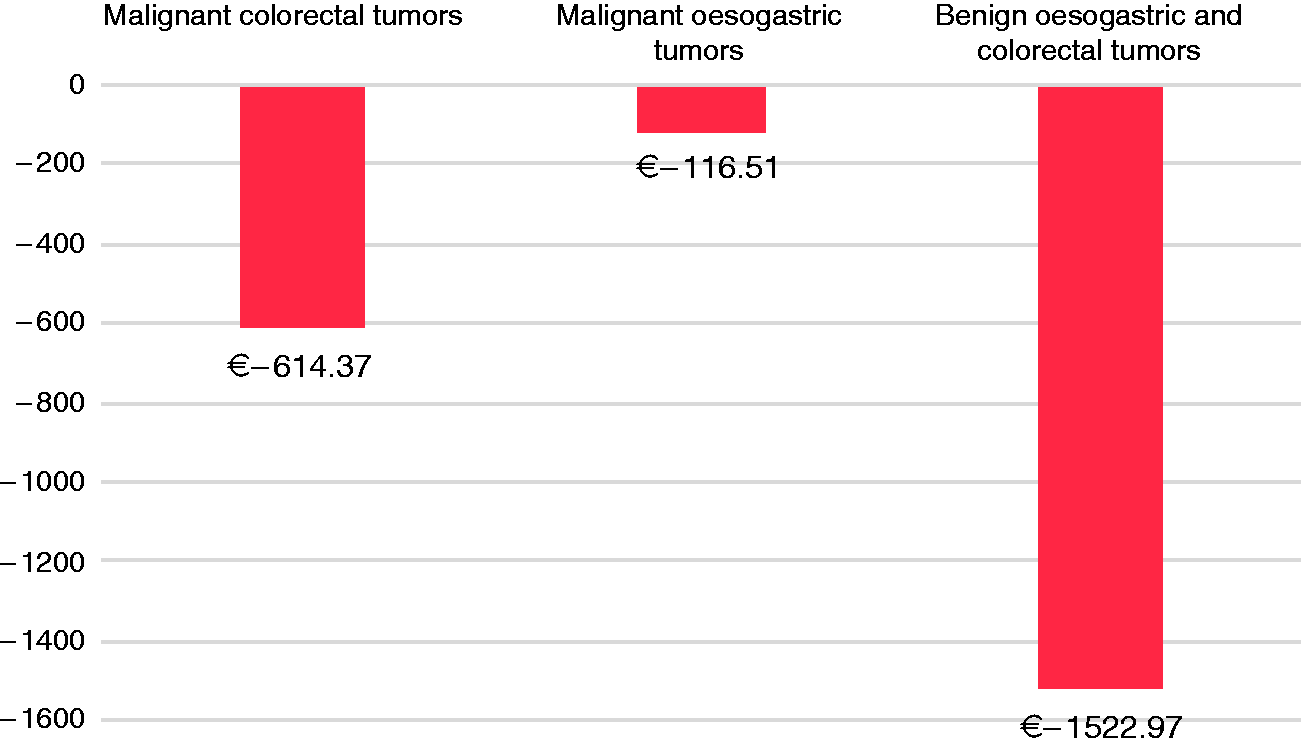
Secondary aims
Medical devices cost
Predictive factors for positive budgetary balance in univariate and multivariate analysis.
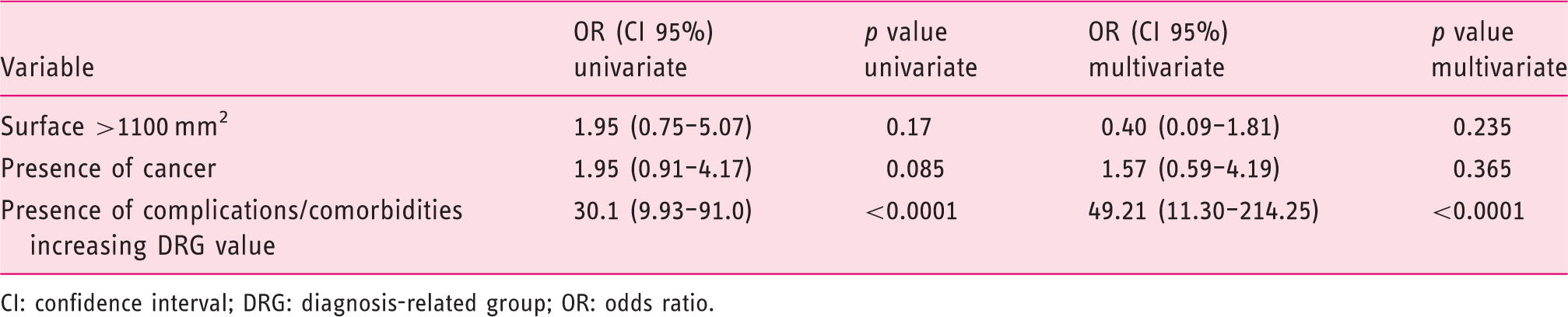
CI: confidence interval; DRG: diagnosis-related group; OR: odds ratio.
Factors influencing the cost/revenue balance (Table 2)
In univariate analysis, presence of comorbidities/complications increasing DRG value as well as the presence of cancer positively influenced the cost/revenue balance. In multivariate analysis, only presence of comorbidities/complications increasing DRG value remained significantly associated with a benefit balance (odds ratio 49.21, 95% confidence interval 11.30–214.25; p < 0.0001).
Comparison with surgery
Clinical and medico-economic comparison with surgery for colonic lesions.
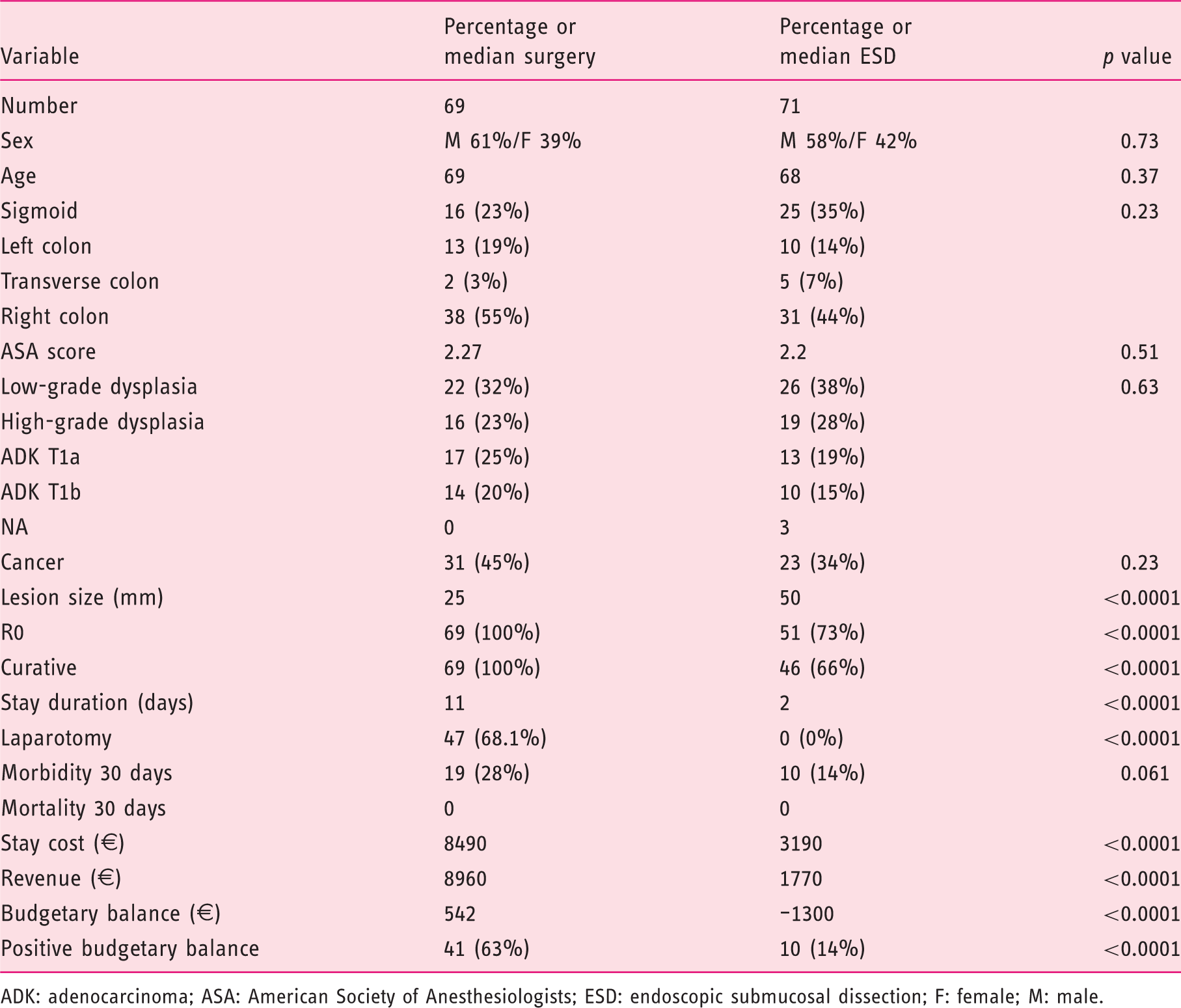
ADK: adenocarcinoma; ASA: American Society of Anesthesiologists; ESD: endoscopic submucosal dissection; F: female; M: male.
DRG values for colorectal ESD and EMR in European countries (without comorbidities/complications).
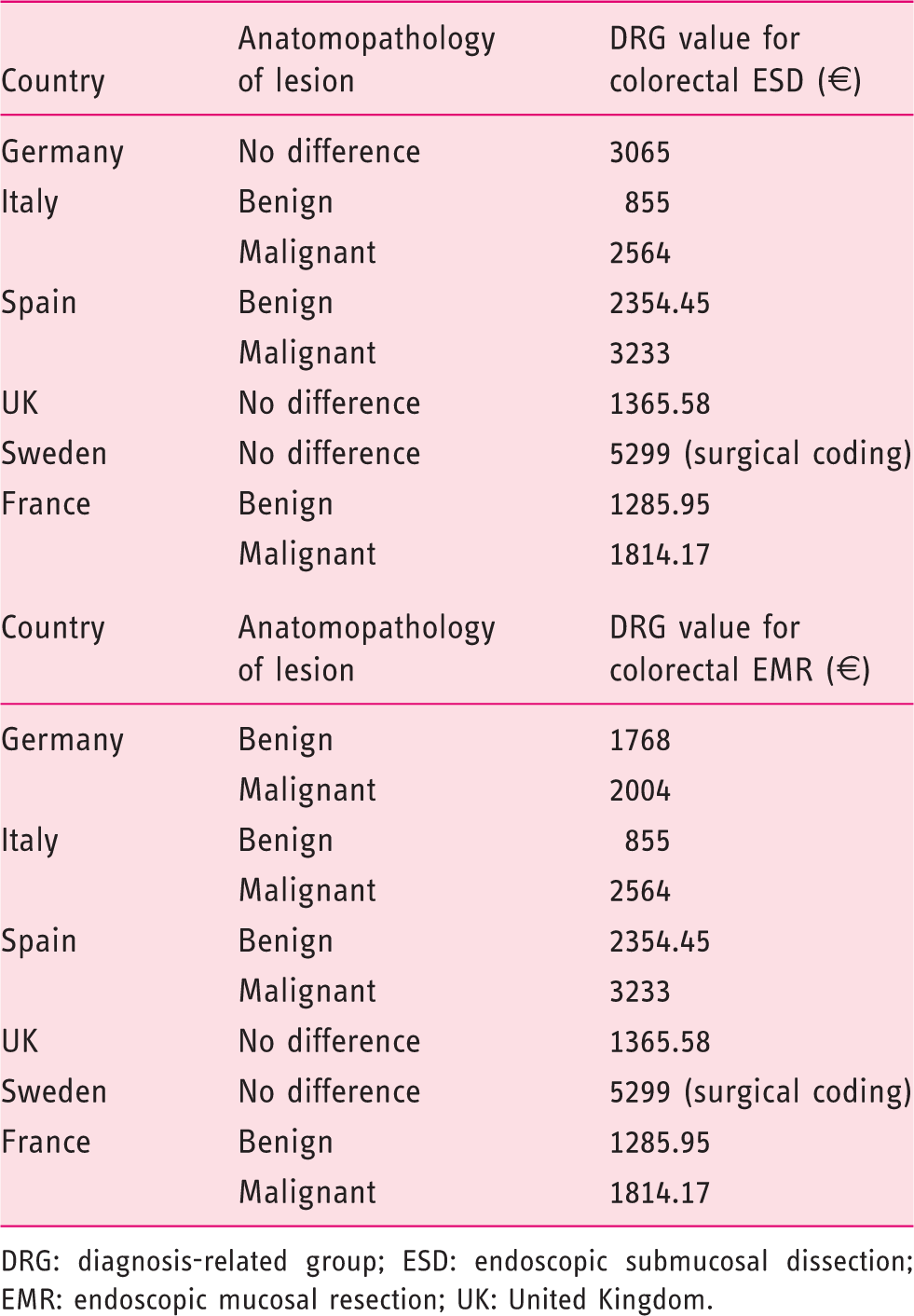
DRG: diagnosis-related group; ESD: endoscopic submucosal dissection; EMR: endoscopic mucosal resection; UK: United Kingdom.
Discussion
Our study is the first European medico-economic study to assess the cost of ESD at the hospital and national health insurance levels.
The total financial losses for our establishment and per stay were estimated to be €142,232.56 and €736.96, respectively. These economic results suggest the current reimbursement system for ESD procedures does not fully cover total hospital expenditures. Reimbursement for the same procedure may double depending on the location of the tumor and the anatomic pathological results.
Our results suggest that medical devices are the main source of expenditure. A potential solution to cover these expenses would be to allocate a specific fixed amount to medical devices, as in Belgium, where €700 is granted for medical devices. This value is close to the amount that was calculated in this study (€970).
The second largest expense is the cost of medical and nonmedical staff, which varies mainly according to procedure length. Apart from unpredictable factors, such as technical difficulties including exposure, mucosal fibrosis and difficulty handling the endoscope, the size of the lesion is the main factor that determines the length of the procedure. This could also be taken into account as a factor modifying the reimbursement.
The average cost of the procedure itself (€1604.96) represents 46% of the total cost of the stay. This cost is not covered by the DRG for benign lesions, for which, despite excellent oncological results reported in our series, the hospital incurs a large deficit, except in cases in which complications occur.
No medico-economic study has been performed in Europe. From a clinical standpoint, the results of our study are comparable to data from the scientific literature in terms of R0 resection, monobloc resection, and recurrence rate.2,3 Our monocentric series of nearly 200 cases is one of the largest series of ESD in the Western world, and these data reinforce the reliability and extrapolation of our results in Europe, especially as the cost of medical devices used varies little from one European country to another. DRG values used in ESD and EMR for colorectal lesions without comorbidities in other leading European countries are summarized in Table 4. All these countries have the same DRG values for ESD and EMR except in Germany, where specific coding for ESD are used. These DRG values are not linked to the endoscopic resection procedure (EMR or ESD) but are linked only to the pathological analysis of the resected specimen. Sweden is the only country whose DRG value (€5299) is big enough to cover the global cost of ESD (€3463.79) as calculated in the survey. Even if hospitalization costs may vary from one country to another, the cost of the procedure tends to be similar. As for benign lesions, the estimated procedure cost (€1604.96) is not fully reimbursed by DRGs in the United Kingdom, France, Spain or Italy. Our results might help to better reassess all these DRGs according to real cost data and thus contribute to making this important procedure more widely performed for the best care of patients.
The comparison of ESD with the retrospective surgical cohort for treatment of colonic lesions is essential. The results are indisputable in terms of safety, length of stay and cost to the health system without a loss of oncological benefit. In the case of complete excision failure or predictive anatomopathological criteria of lymph node invasion, second-look surgery is neither more complicated nor less effective. 4 An American study has produced results similar to ours, with close to 50% reduction of costs for ESD compared with surgery without a loss of oncological efficacy. 5
This economic advantage has already been demonstrated for colonic EMR vs surgical colectomy through several cost-effectiveness studies.6–8 Although many studies continue to show that more than 30% of large polyps are operated on,9–12 our results reinforce the idea that there is no scientific or economic reason to perform surgery in patients with superficial colorectal lesions. We deliberately excluded endoscopic or surgical treatment of rectal lesions from this secondary analysis because our center does not perform transanal endoscopic microsurgery (TEM). However, a multicenter study is currently comparing TEM and rectal ESD in France, with the main objective of comparing cost-effectiveness ratios (NCT02885142). These results are counterbalanced by the deficit met by health structures. Indeed, although the benefits for patients seem obvious compared to surgery, and the cost for the reimbursement system is lower, the health structure loses money when a patient is treated with ESD but earns money when the same patient receives surgical treatment. This economic problem is a major limiting factor for the development of ESD in Western countries.
Questions remain unanswered concerning the medico-economic comparison of ESD and EMR for large superficial lesions of the colorectum. No direct comparative study exists; however, a recent study has attempted to compare the three following strategies from medical and economic viewpoints: piecemeal EMR for all lesions, ESD for all lesions, and selective ESD for lesions suspicious for malignancy. 13 The selective strategy appeared to be the most cost effective. The end results were balanced out, however, by the average size of the lesions included (25 mm), the high reimbursement rate of the dissection act in Australia ($4500) and the low level of sensitivity for the prediction of high-risk lesions (30%). 14
These results highlight the importance of randomized controlled trials with medico-economic objectives on this subject to decide whether the Japanese point of view (ESD for all) or the more Western attitude (ESD for risky lesions) should be adopted.
Despite the exhaustive nature of microcosting, our study is not without limitations. First, this study was monocentric and reflects the results of a French expert center where two operators performed all procedures. Next, colonic dissection was introduced in our center in January 2016, which may have resulted in an increased cost due to the learning curve. Although the learning curve may have increased costs, the results of our comparison with the surgical cohort remain indisputable. Lastly, the costs associated with anatomopathology were largely underevaluated (costs for polyp analysis), as it was not possible to perform microcosting of these data.
In conclusion, our study demonstrated that ESD procedures generate additional financial costs to hospitals. ESD-specific medical devices accounted for the majority of the increased expenditure. Cost of ESD is not covered by DRGs in most European countries. This procedure should be recommended, however, because of the medical benefit to patients and lower cost compared with surgery. The creation of sampling systems that take into account all costs involved is essential to promote the necessary expansion of ESD for the benefit of patients.
Supplemental Material
Supplemental material for What is the cost of endoscopic submucosal dissection (ESD)? A medico-economic study
Supplemental material for What is the cost of endoscopic submucosal dissection (ESD)? A medico-economic study by Martin Dahan, Emmanuelle Pauliat, Sandra Liva-Yonnet, Sonia Brischoux, Romain Legros, Arnaud Tailleur, Paul Carrier, Aurélie Charissoux, Virginie Valgueblasse, Véronique Loustaud-Ratti, Abdelkader Taibi, Sylvaine Durand-Fontanier, Denis Valleix, Denis Sautereau, Sébastien Kerever and Jérémie Jacques in United European Gastroenterology Journal
Footnotes
Acknowledgment
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This study was conducted after approval by the Regional Scientific Ethical Committee of Limoges University Hospital Center, January 20, 2018 (protocol number: 242-2018-08).
Informed consent
French legislation on studies of anonymized retrospective data does not require informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.