
Abstract
Background
A subset of patients with functional defecation disorders have predominance of the puborectalis muscle (PRM) on three-dimensional high definition anorectal manometry (HDARM), known as paradoxical puborectalis syndrome (PPS). The aim of this study was to assess clinical and manometric differences between patients with and without PPS.
Methods
A total of 227 women with functional defecation disorders undergoing HDARM between December 2012 and October 2016 at a single center were included in this study. All completed the Rome III constipation module and Pelvic Floor Distress Inventory 20 (PFDI-20).
Results
Eighty-seven out of 227 women had a 3D pressure topographic profile consistent with PPS. They had higher mean PDFI-20 scores for straining and incomplete evacuation symptoms than those without PPS. In addition, they demonstrated higher mean resting anal pressure, a more negative mean anorectal pressure differential, and a greater proportion with prolonged balloon expulsion test. These findings were more pronounced in a subgroup of 58 PPS patients with a distinct pattern of both posterior and posterolateral wall indentation.
Conclusion
Among female patients with functional defecation disorders, those with PPS demonstrated clinical and manometric differences compared to those without PPS. These differences may be driven by predominant posterolateral wall indentation in a subgroup of PPS patients.
Keywords
Key summary
- Paradoxical purorectalis syndrome (PPS) is a recently described subtype of dyssynergic defecation characterized by failed relaxation of the puborectalis muscle. - In this study, patients with PPS demonstrated more severe clinical symptoms and differences in multiple manometric parameters compared to non-PPS patients with a functional defecation disorder. This may be driven by a novel subtype of PPS described in this paper. - This study suggests that three-dimensional high-definition anorectal manometry can be used to specifically assess the functioning of the puborectalis muscle.
Introduction
Dyssynergic defecation (DD) is characterized by paradoxical contraction or inadequate relaxation of pelvic floor muscles (i.e. anal sphincter and/or puborectalis muscle) during attempted defecation. 1 Anorectal manometry (ARM) includes a series of sensory and motor physiological measurements of anorectal function,2–4 and along with the balloon expulsion test (BET), has been particularly useful in diagnosing dyssynergia in patients with chronic constipation (CC).5–9 Traditional ARM provides a pressure measurement from the sum of all muscles in the anal sphincter, but does not differentiate the individual contributions of each muscle. The anal sphincter is a complex structure consisting of the overlapping internal anal sphincter, external anal sphincter, and puborectalis muscle (PRM).10,11 With three-dimensional high definition anorectal manometry (HDARM), closely spaced circumferential sensors extending across the anal canal allow for spatial reconstruction of pressures in the anorectum. This permits assessment of individual muscles in those with DD.12–15
Paradoxical puborectalis syndrome (PPS) is a specific type of dyssynergic defecation in which the puborectalis muscle either paradoxically contracts or fails to relax during attempted defecation, leading to a lack of straightening of the anorectal angle and resulting outlet obstruction. 16 Historically, it has been diagnosed by electromyography (EMG) or defecography. 16 In a recent study, Xu et al. identified a population of individuals with PPS on the basis of findings from rectal examination, defecography, EMG, and BET. The authors then demonstrated typical findings on HDARM pressure topography plots in this group of patients: specifically, a high-pressure area in the distal posterior wall of the anorectum, indicating that the diagnosis of PPS can be made primarily on the basis of HDARM. 17
Despite the wealth of information provided by HDARM, the clinical significance of specific findings on this testing modality remains under question, as prior studies have noted abnormal findings in a large proportion of healthy individuals without clinical symptoms.18,19 Given this, we compared women with PPS diagnosed by HDARM to women with a functional defecation disorder in the absence of PPS, and assessed for differences in clinical symptoms between the two groups. We also compared manometric parameters between groups, and further analyzed 3D pressure topography of patients with PPS for additional features that predicted clinical symptoms.
Methods
Participants
All women referred to Beth Israel Deaconess Medical Center for HDARM for CC from December 2012 to October 2016 were considered for study enrollment. Patients younger than 18 years were excluded, as were those with a history of fecal incontinence and major anorectal or colonic surgery. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki, as reflected in a prior approval from the institutional review board of Beth Israel Deaconess Medical Center on September 24, 2012. Written, informed consent was obtained from each patient included in the study.
ARM procedure
HDARM was performed with the patient in the left lateral decubitus position with knees and hips flexed, using the ManoScan™ HDARM probe, which is 6.4 cm in length, has an outer diameter of 10.75 mm, and contains 256 pressure sensors arranged in 16 rows (Sierra Scientific Instruments, Los Angeles, CA, USA). Assessment of anorectal pressure was performed after a five-minute resting period in the following order: at rest (20 seconds), during three simulated squeezes (20 seconds each), and during three simulated defecation attempts. Rectal sensation thresholds were then measured through progressive inflation of the intrarectal balloon with 10–20-ml increments until the patient reported first sensation, and thereafter with 20-ml increments until the patient reported desire to defecate and/or severe urgency (maximum of 250 ml reached).
All patients subsequently underwent a timed BET, performed by inserting a standard, single-use anorectal balloon expulsion catheter (Mui Scientific, Mississauga, ON, Canada) followed by inflating a nonlatex 400-ml volume balloon with 50 ml of warm water with the patient in the left lateral decubitus position. 20 The patient was then asked to sit on a commode in privacy and expel the balloon. A BET of >2 minutes was considered delayed.21,22
HDARM analysis
Analysis of manometric data was performed using ManoView analysis software (Medtronic, Minneapolis, MN, USA). Individuals with inadequate anal sphincter relaxation or inadequate propulsive forces during attempted defecation were classified as having a functional defecation disorder, in accordance with Rome IV classification. The Rome IV classification does not provide a clear cutoff value to define abnormal anal sphincter relaxation or inadequate defecatory propulsion. Reported mean values for rectal push on high definition and high resolution ARM range from 20 mmHg to 64 mmHg,19,23–26 while reported mean values for anal sphincter relaxation range between 24% and 32%.23–27 Recent review articles of high definition and high resolution ARM and DD have suggested an increase of rectal pressure of <40 mmHg 28 and a reduction in anal pressure of ≤20% as being abnormal.28,29 In this study, we used these cutoff values to define the presence of a functional defecation disorder.
HDARM pressure data were modified using interpolation to generate high-resolution pressure topography plots rendered with color-coded, spatiotemporal representations of pressure recordings in the anorectum (Clouse plots). Patients were classified as having PPS based on visual analysis of these plots for presence of the characteristic “boot-shaped” pressure cylinder and high-pressure area in the posterior rectal wall during simulated defecation previously noted to be characteristic of PPS.
17
Two authors with five (M.Z.) and two (W.H.) years of practice in reading anorectal manometry visually examined the HDARM color patterns to identify the PRM, and a third author (A.L.) with more than 20 years' such experience was consulted if the first two disagreed. Within the PPS group, there were two subgroups of patients with (a) predominant posterolateral wall indentation, or (b) isolated posterior wall indentation (Figure 1). We labelled these PPS posterolateral (PPS-PL) and PPS isolated posterior (PPS-IP), respectively.
(a) Paradoxical purorectalis syndrome-(PPS) posterolateral, (b) PPS-isolated posterior, and (c) non-PPS dyssynergic defecation.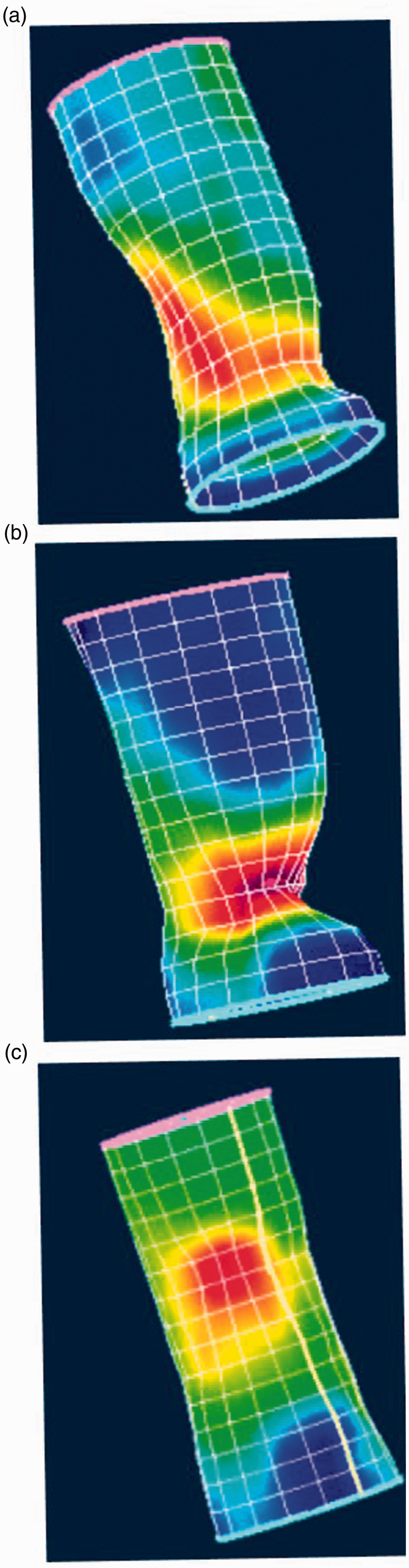
Symptom assessments
All patients completed the Pelvic Floor Distress Inventory 20 (PFDI-20) questionnaire and the Rome III Constipation Module prior to undergoing HDARM. The PFDI-20 is a validated measure of symptom severity and symptom-related distress in all forms of pelvic floor disorders. 30 It has a total of 20 questions, each of which is rated on a five-point Likert scale. 31 We assessed the severity of straining, digital maneuvers, incomplete evacuation, and pain with defecation using questions from the PFDI-20 questionnaire.
Statistical analysis
Continuous variables were summarized using means and standard deviations (SDs). We compared baseline characteristics and HDARM results of patients based on 3D topographical pattern. For discrete outcomes, univariate comparisons were made using the Fisher exact test or chi-squared test and continuous outcomes were compared using t test for pairwise comparisons, or analysis of variance (ANOVA) for comparison of more than two groups. When ANOVA testing was significant, we tested group differences using a two-sample t test with Bonferroni correction. We used multivariable logistic regression to estimate the association between demographics, HDARM topographical pattern, irritable bowel syndrome (IBS) status, HDARM parameters, and the proportion of delayed balloon expulsion.
Results
Study sample
Of 462 consecutive women with constipation referred for HDARM, 227 met the criteria for a functional defecation disorder. The mean age was 46.8 years (SD = 15.6). A total of 43.8% met Rome III criteria for IBS. Among these patients, the mean PFDI score for straining was 2.94 (range 0–4, SD = 1.44), and mean PDFI score for incomplete evacuation was 3.12 (range 0–4, SD = 1.18).
PPS
Based on HDARM topographical evaluation, PPS was identified in 87 patients (mean age = 40.8 ± 15.2) with a functional defecation disorder. The remaining 140 patients did not demonstrate predominant PRM contraction (non-PPS; mean age = 50.3 ± 15.6). Of the 87 patients identified as having PPS, 76 had a mean anal sphincter relaxation of ≤ 20%, and 44 had a BET greater than two minutes. Thirty-nine out of the 87 had both decreased anal sphincter relaxation and prolonged BET, while five out of the 87 had neither.
Clinical characteristics
Clinical and Anorectal Manometry Parameters: PPS vs non-PPS patients.
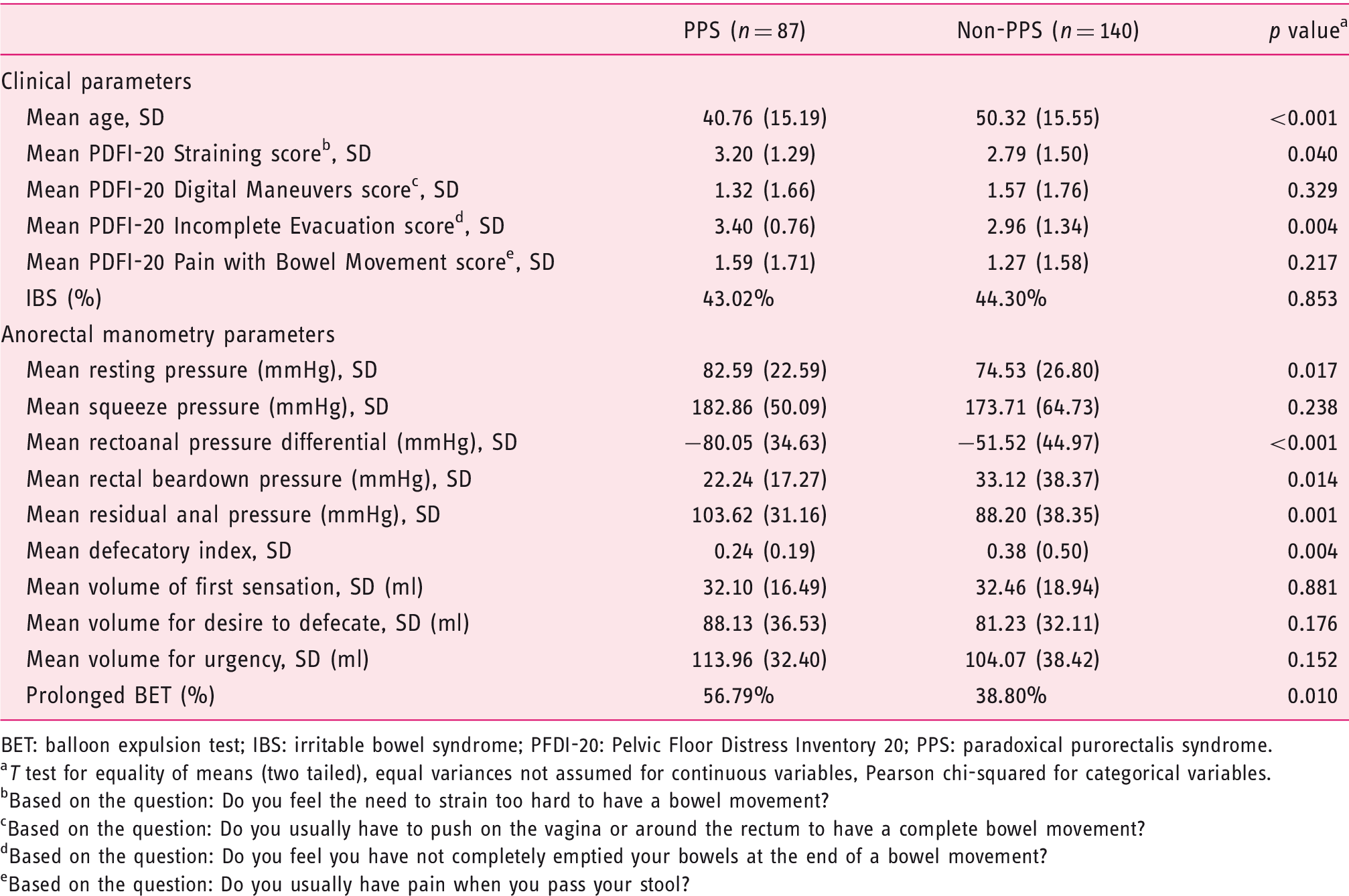
BET: balloon expulsion test; IBS: irritable bowel syndrome; PFDI-20: Pelvic Floor Distress Inventory 20; PPS: paradoxical purorectalis syndrome.
T test for equality of means (two tailed), equal variances not assumed for continuous variables, Pearson chi-squared for categorical variables.
Based on the question: Do you feel the need to strain too hard to have a bowel movement?
Based on the question: Do you usually have to push on the vagina or around the rectum to have a complete bowel movement?
Based on the question: Do you feel you have not completely emptied your bowels at the end of a bowel movement?
Based on the question: Do you usually have pain when you pass your stool?
Anorectal Pressure Parameters and BET
Mean resting anal pressure was significantly higher in the PPS group compared to the non-PPS group (82.6 mmHg vs 74.5 mmHg, p = 0.017) (Table 1). During simulated push, the mean rectoanal pressure was significantly more negative in PPS patients than in non-PPS patients (–80.1 mmHg vs –51.5 mmHg, p < 0.001). PPS patients also had lower mean rectal beardown pressure (22.2 mmHg vs 33.1 mmHg, p = 0.014) and mean defecatory index (0.24 vs 0.38, p = 0.004), along with higher mean residual anal pressure (103.6 mmHg vs 88.2 mmHg, p = 0.001) during simulated push. No significant difference was present between the groups in other anorectal manometry parameters (Table 1).
A significantly higher proportion of PPS patients had a prolonged BET (i.e. > 2 minutes) compared to non-PPS patients (56.8% vs 38.8%, p = 0.010). After multivariable adjustment for age and resting pressure, PPS remained an independent predictor of prolonged BET on multivariable analysis (odds ratio (OR) 1.91, 95% confidence interval (CI) 1.05–3.46).
PPS subtypes
Clinical and Anorectal Manometry Parameters: PPS subtypes and non-PPS.
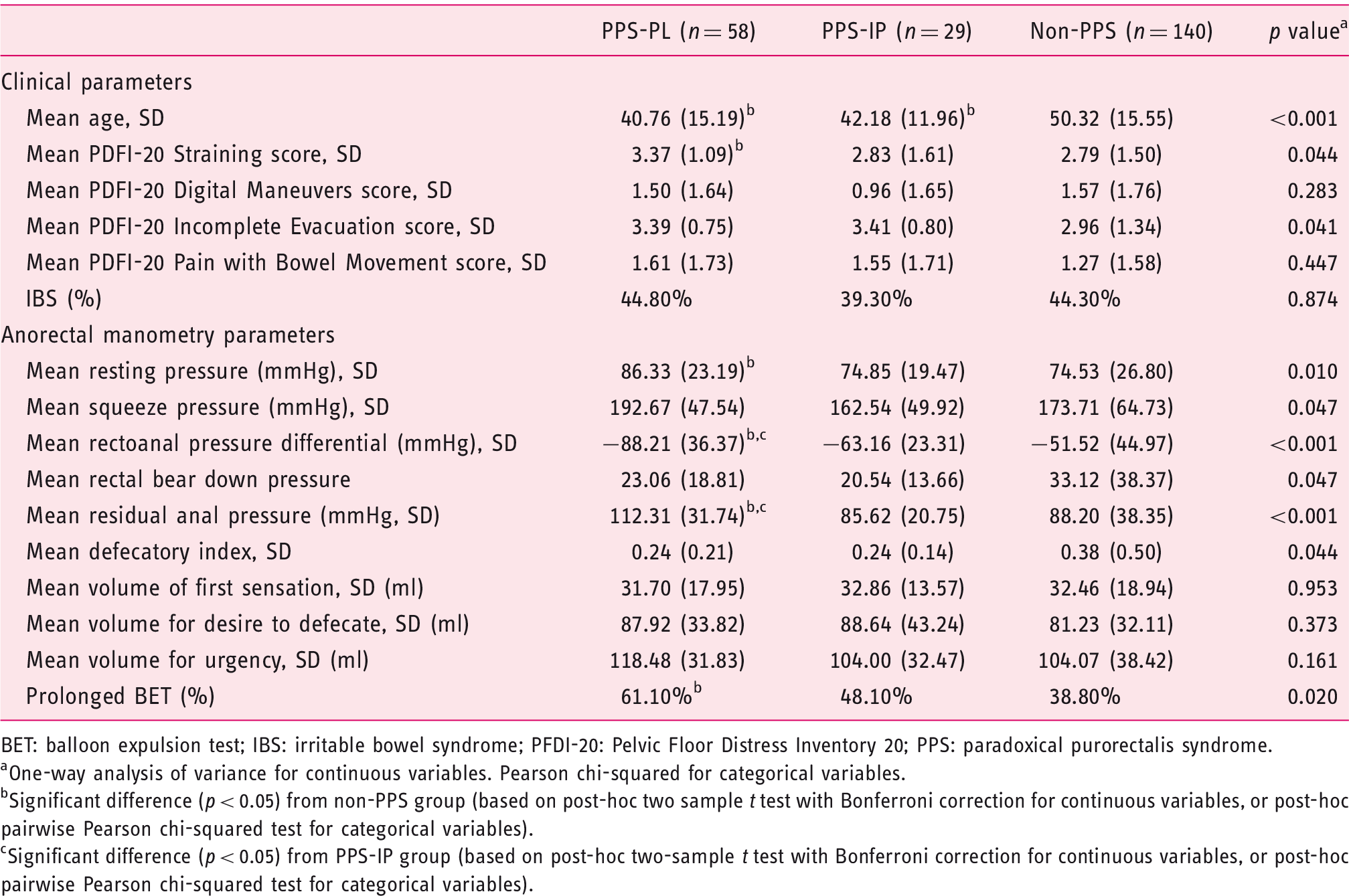
BET: balloon expulsion test; IBS: irritable bowel syndrome; PFDI-20: Pelvic Floor Distress Inventory 20; PPS: paradoxical purorectalis syndrome.
One-way analysis of variance for continuous variables. Pearson chi-squared for categorical variables.
Significant difference (p < 0.05) from non-PPS group (based on post-hoc two sample t test with Bonferroni correction for continuous variables, or post-hoc pairwise Pearson chi-squared test for categorical variables).
Significant difference (p < 0.05) from PPS-IP group (based on post-hoc two-sample t test with Bonferroni correction for continuous variables, or post-hoc pairwise Pearson chi-squared test for categorical variables).
PPS subtypes: clinical parameters
ANOVA revealed significant differences between groups in straining score and incomplete evacuation score on the PFDI questionnaire (see Table 2). On post hoc pairwise comparison, the PPS-PL group had a significantly higher PFDI straining score compared to the non-PPS group (p = 0.041). While ANOVA testing demonstrated significant differences between the groups in incomplete evacuation PFDI score, pairwise post hoc testing did not demonstrate any differences between individual groups.
PPS subtypes: anorectal pressure parameters and BET
ANOVA revealed significant differences between groups in mean resting anal sphincter pressure, mean rectoanal pressure differential, and mean residual anal pressure (see Table 2). The PPS-PL group had higher mean resting anal sphincter pressure than the non-PPS group (p = 0.009). The PPS-PL group demonstrated a significantly more negative mean rectoanal pressure difference than both the PPS-IP group (p = 0.024) and the non-PPS group (p < 0.001). The PPS-PL group also demonstrated a higher mean residual anal pressure than both the PPS-IP group (p = 0.003) and the non-PPS group (p < 0.001). ANOVA testing demonstrated significant differences between groups in mean squeeze anal sphincter pressure, rectal beardown pressure, and defecatory index, but pairwise post hoc testing did not demonstrate any difference between specific individual groups.
Chi-squared testing demonstrated a significant difference between groups in percentage of patients with prolonged BET. Based on post hoc pairwise testing, the PPS-PL group had a significantly higher proportion of patients with prolonged BET compared to the non-PPS group (p = 0.005). PPS-PL was also the only independent predictor of prolonged BET on multivariable analysis after controlling for age and resting pressure (OR 2.03, 95% CI 1.08–3.83, p = 0.028). PPS-IP was not a predictor of prolonged BET (OR 1.36, 95% CI 0.62–3.09, p = 0.456).
Discussion
In this study, we used spatial 3D pressure topographic analysis from HDARM of individual female patients with functional defecatory disorders to distinguish those with PPS. Recently, Xu et al. 17 showed that PPS could be readily diagnosed based on HDARM pressure topography. 17 We demonstrated significant differences in both clinical and manometric parameters between PPS and non-PPS. We also identified a subgroup of PPS patients with predominant PL wall indentation on HDARM pressure topographic analysis.
A major advantage of HDARM compared with conventional manometry is that it allows for more detailed understanding of defecatory physiology and the specific function of individual muscles involved in defecation. 32 However, the specific application of the additional information provided by HDARM remains a topic of ongoing research. Recent studies, for example, have investigated the role of HDARM in the evaluation of anal sphincter defects.33,34 To our knowledge, the study by Xu et al. to identify PPS was the first to differentiate DD patients based on the individual function of the muscles involved in the defecatory process.
In their study of 79 patients with PPS (41 of whom were female) compared to 71 healthy adults (37 of whom were female), Xu et al. 17 noted an increased maximum resting anal pressure, mean resting anal pressure, residual anal pressure, high-pressure zone length, and a more negative rectoanal pressure differential in patients with PPS. In accordance with the findings from their study, we also demonstrated increased mean resting anal pressure and a more negative rectoanal pressure differential in patients with PPS. Building on these findings, we demonstrated that the presence of PPS was associated with differences in self-reported clinical outcomes. Given that completely normal findings on anorectal manometry were previously reported in only 13% of healthy volunteers, 18 we believe that identifying specific abnormal findings on this modality that correlate with clinical symptoms represents an important advance in understanding. All individuals classified as having PPS in this study had complained of constipation, and the vast majority (82/87) had abnormal anal sphincter relaxation, abnormal balloon expulsion time, or both. We believe that this further supports the clinical relevance of this manometric finding. More broadly, it points to the utility of assessing the function of specific muscles on anorectal manometry, and suggests there may be a role for pelvic floor physical therapy targeted toward normalizing the function of the puborectalis muscle in individuals found to have PPS on HDARM.
We noted that the presence of PPS with PL wall indentation was a predictor for prolonged BET, while the presence of PPS without PL wall indentation was not. Only the PPS-PL group demonstrated a higher straining score than the non-PPS group. Similarly, only the PPS-PL group demonstrated higher mean anal sphincter resting pressure, more negative mean rectoanal pressure differential, higher mean residual anal pressure, and higher incidence of prolonged BET compared to the non-PPS group. The PPS group without PL indentation did not demonstrate a significant difference compared to the non-PPS group on any of these variables.
Together, these results suggest that PL wall indentation represents a distinct subtype of PPS, and that this particular subtype appears to be the main driver of the clinically important differences between constipation patients with and without PPS that were noted both in this study and the study by Xu et al. 17 It is possible that patients with PL wall indentation have more global puborectalis dysfunction, while those with IP wall indentation may have a more focal dysfunction, or may have manometric findings that are in part due to the internal and external anal sphincters, rather than the puborectalis.
Strengths of this study include a large sample of constipation patients with and without PPS, with concomitant survey data collected at the time of HDARM. To our knowledge, this is the largest study of HDARM parameters in patients with PPS, and the first to assess clinical parameters in individuals with and without PPS. The main weakness is that the presence of PPS was identified on the basis of visual examination of 3D pressure topography (rather than by magnetic resonance (MR) defecography or EMG), and thus could have been prone to interobserver variability. Translating qualitative visualization of puborectalis muscle function into a quantitative analysis that can be replicated by multiple observers represents a challenge. In the future, this may involve analysis of pressures recorded by specific sensors on the HDARM probe in the posterior rectum, and noting the ratio between these pressures and overall residual anal pressure during a simulated push. This method would require prospective validation in future studies.
Additionally, we performed HDARM with a rigid high-resolution probe (which does not conform to the anorectal angle) in the left lateral decubitus position, which is not a normal position for defecation. 19 We also asked participants to perform simulated beardown with a noninflated rectal balloon, which has been shown to result in increased likelihood of a DD pattern in healthy controls. 19 A future area of exploration would be to correlate findings on HDARM with findings on imaging studies like X-ray or MR defecography to provide additional corroborating data on the functioning of individual pelvic floor muscles, as well as with findings on colonic transit studies. In our study, there were only 19 patients with a diagnosis of PPS who underwent X-ray or MR defecography within one year of HDARM. Eight of these patients underwent MR defecography, and seven were noted to have abnormal studies, with findings consistent with DD, abnormal relaxation of the puborectalis muscle, or both. However, the small number of individuals who underwent these studies precluded us from making broad inferences regarding correlation between HDARM and findings on dynamic imaging during defecation.
In conclusion, this study builds on the findings of Xu et al. by confirming that there are significant differences in manometric parameters between constipation patients with and without PPS. This study also reports the novel finding that PPS patients demonstrated more significant clinical symptoms. A subgroup of PPS patients with predominant PL wall indentation may be primarily responsible for these differences. Future studies are needed to assess whether PPS patients (including those with and without PL wall indentation) respond differently to biofeedback therapy compared to non-PPS patients (both in terms of findings on repeat manometry, as well as evolution of reported clinical symptoms).
Footnotes
Declaration of conflicting interests
None declared.
Funding
Research reported in this publication was supported by the National Institutes of Health under award numbers R01AT00857303 and T32DK007760.
Ethics approval
This study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki, as reflected in a prior approval from the institutional review board of Beth Israel Deaconess Medical Center on September 24, 2012.
Informed consent
Written, informed consent was obtained from each patient included in this study.