
Abstract
Background
Variable prevalence rates between 2.4 and 35% have been reported for chronic constipation across different countries worldwide, with a low 5% for Germany.
Objectives and methods
We conducted a computer-assisted telephone interview among 15,002 representative individuals in Germany, asking about health-related problems, including constipation. Those who acknowledged the presence of constipation symptoms during the preceding 12 months were questioned concerning constipation features and sociographic variables.
Results
Of 15,002 individuals interviewed, 2,239 (14.9%) acknowledged having experienced constipation during the last 12 months, 864 (5.8%) reported constipation during the last 4 weeks, and 380 (2.5%) had current constipation symptoms; 4.4% had taken medication because of their constipation, and 2.6% had consulted a doctor for constipation. In comparison to non-constipated volunteers, those constipated had a lower health quality of life and poorer health, and lower income and social status.
Conclusion
Up to 15% of the general (German) population report symptoms of constipation depending on the definition. This matches pooled constipation rates across 18 countries (14%).
Background
The prevalence of chronic constipation has been reported to range between 5% and 15% of the general population, depending on the size and type of assessment, the definition of constipation, and variables such as nationality, culture, and the healthcare system.1–3 Prevalence of constipation has been reported to be 5% in Germany. 4 This is substantially lower than in other European countries and worldwide, 5 even when assessed with a similar instrument and for the same purpose. 4 Pooled prevalence across 41 studies was reported to be 14%. 5 However, many of these studies lack the control for representativeness of the sample, and were either conducted in clinical populations or for assessment of many and other gastrointestinal symptoms as well, and may therefore underestimate the constipation prevalence. 6
Despite differences in total prevalence, a number of statistical descriptors have repeatedly been reported across different studies. Constipation appears to be more frequent in women than in men, 7 to increase with age, 8 and to be associated with lower income and social status. 9 This has been attributed to altered hormonal changes, 10 age-related bowel dysfunction, and nutritional habits, 11 respectively, alone or in combination. Other factors that may contribute to constipation prevalence are pregnancy, 12 poor hygiene conditions, 13 and high workload and time pressure for those employed, 14 but these data are far less conclusive. Constipation as a secondary symptom is well established for a number of neurological (e.g. stroke, Parkinson’s disease, spinal cord injury), systemic (diabetes, hypothyroidism, scleroderma), and other disorders, but also secondary to intestinal or non-intestinal surgery,15–17 and may as well occur secondary to a variety of medications used for treatment of chronic clinical conditions, e.g. calcium antagonists for high blood pressure, 18 opioids for chronic pain, 19 and tricyclic antidepressants for major depression. 20
Quality-of-life (QoL) has been reported to be low in chronic constipation when assessed with both constipation-specific QoL instruments,21,22 as well as with generic QoL tests in comparison to other chronic conditions.23–25
Methods
The aim of the GECCO study was to (1) determine the prevalence of chronic constipation among adults in Germany by a telephone survey and (2) to obtain information on their quality of life and further medical parameters. We here report the data from a 10-minute telephone interview conducted to identify patients and non-patients that experience constipation symptoms. For research efficiency reasons, the study was conducted in German only, i.e. it was restricted to adults with sufficient German language skills. Moreover, only people living in private households (as opposed to institutions, military barracks, prisons, monasteries, etc.) with landline connection were included in the telephone survey, thereby excluding people with cell phone availability only.
Random last digit
We planned a random last digit (RLD) approach to conduct a 10-min telephone interview (computer-assisted telephone interview) with individuals who acknowledged the presence of constipation symptoms during the preceding 12 months.
RLD is based on a methodology utilizing a general telephone registry of all available (landline) phone numbers. However, in West Germany 10–20% of households with landline connection are not listed in these registries; 26 in East Germany the percentage is even higher (15–25%). Moreover, single-person households and younger people are underrepresented in telephone registries. 27 To account for such systematic biases, and to include also non-registered phone numbers, a “block number approach,” in which the last two digits are replaced by random digits, is the basis of almost all RLD studies in Germany.27,28
The RLD procedure selected phone numbers belonging to households. The next selection step was identifying the target person in this household (an adult ≥18 years). If two or more adults lived in the household, the target person was randomly selected, using the “last-birthday” method. 29 Two avoid a bias resulting from differences in accessibility, target persons who were not available upon a first dialing were contacted multiple times at different weekdays and hours.
Data acquisition
The data acquisition process was conducted in two steps: a test of the instruments and logistics with a sample size of 1,000 people approached by RLD, and a second step with the sample size of 15,000 people based on the prevalence and response rates of step 1 as well as estimates of needed numbers of constipated individuals to be approached in step 2. Step 1 was conducted during early spring 2012, step 2 in the subsequent summer months (May and June, 2012).
The protocol of the study methodology had been reviewed by the Ethics Committee of the Tübingen University Medical School, and the study was conducted in accordance with approved standards for epidemiological research. 30
To avoid potential biases during the construction of the questionnaire battery, during data acquisition and interpretation, specific care was taken to separate study sponsoring from study conductance. For this, a contract between the University of Tübingen Clinics (UKT, Tübingen, Germany) and Movetis-Shire Inc. (Beerse, Belgium) ruled the finances of the project and the aim of the study, while a separate contract between UKT and infas (Institut für Sozialforschung, Bonn, Germany) rules the responsibility of UKT for content of the interview and questionnaire, and data interpretation, while infas conducted both tasks on behalf of UKT. While Shire-Movetis was consulted during the construction phase, the sole responsibility for it was with UKT.
Step 1: Pilot study – instrument testing and screening
Based on available survey data on constipation in Germany, 4 we estimated that interviewing 1,000 adults would provide us with 50 individuals experiencing constipation, of which 80% (n = 40) would accept to be interviewed. This was regarded as sufficient to eliminate errors and misunderstandings in the interview guidelines, and to calculate the sample size for step 2. To reach 1,000 target individuals by RLD, an approximately threefold number of dialings within the target group had to be performed.
Step 2: Main study – population survey
Based on prevalence response rates during step 1 with 1,005 people interviewed, we decided to approach 15,000 adult individuals aged 18 or older during step 2. Similar responses as in step 1 rates assumed, this would allow interviewing 2,612 (95% CI: 2,260–2,964) individuals with constipation. To interview 15,000 individuals, approximately 45,000 telephone calls within the target group were to be conducted, based on previous experience of infas.
As the RLD numbers are generated using a random procedure, most of them do not exist as telephone numbers. Another considerable percentage of RLD numbers does not belong to private households or it is unknown whether they belong to the target group. Thus, to call 45,000 target group households, approximately 230,000 random numbers were to be generated.
The telephone interview
All interviews were conducted by experienced call-center staff of the infas Institute (Bonn, Germany). Each interview lasted approximated 10 minutes. To avoid a bias in the willingness to participate, the interview was not initiated with the focus on constipation but with the more general statement that this was a study on behalf of the University of Tübingen Medical Clinic interested in “health and health-related issues in the general population”. No financial incentive was offered for participation.
The interview started with a series of questions related to general health and life satisfaction, health activities, nutritional habits, and health-related problems (pain, circulation, urination, gynecological problems, digestion, and constipation). Only if the latter (constipation) was confirmed, further questioning asked for its type, its duration and first occurrence, and whether the person had consulted a physician about it, or had taken medication for constipation. The interview concluded with sociographic data (education and training, professional status, family income). Final questions referred to the willingness to participate in a future follow-up questionnaire study.
Weighting
All data were weighted to maintain representativeness of the sample respondents. First, a design weight was calculated to compensate for the target persons’ different probability of selection. This step is necessary as people in single-person households and in households available through multiple (ISDN) lines have a higher probability of selection than people in multi-person households or in households with one landline only. Second, a redressment was performed to adapt the distribution of specific socioeconomic variables collected in the survey (age, gender, age/gender, household size, educational level) to the distribution of these variables known from official population statistics on an aggregate basis. Moreover, to control for any seasonal effects when collecting data on health status, the distribution of “health problems during the past four weeks” was controlled using average values from both pilot study and main study.
Statistics
Prevalence rates for constipation were computed based on variable constipation definitions: presence of constipation symptoms during the preceding 12 months, presence of constipation during the last 4 weeks, acute constipation, consultation of a physician for constipation, and medication intake for constipation. Data are reported as mean ± SD. The significance level was set to 0.05 for all tests, when constipated were compared to non-constipated participants with parametric and non-parametric tests. No correction for multiple testing was applied as all statistical comparisons between the constipated and non-constipated were performed only once, and variables were regarded as independent of each other.
Results
Acceptance and response rates
Sample generation in the screening phase (step 1) and the sampling phase (step 2) (see text for details)
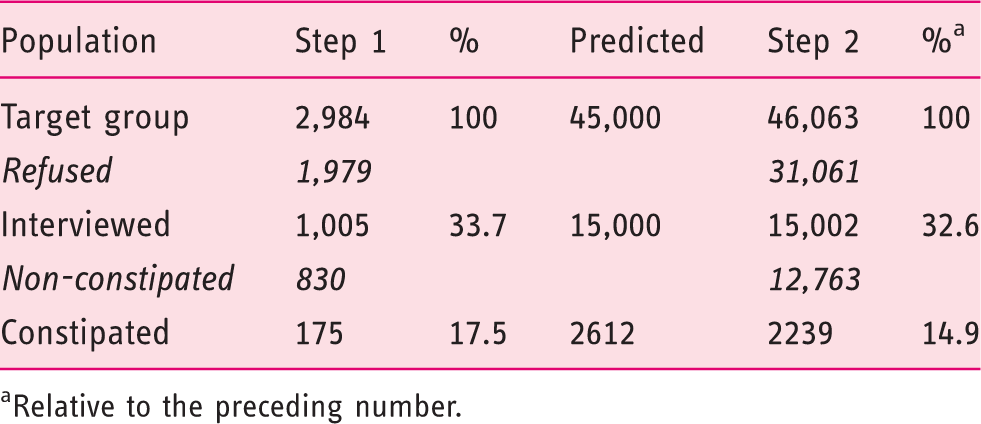
Relative to the preceding number.
The differences in response between step 1 (pilot study) and step 2 (main study) were thought to represent (among others) differences, for example, in seasonal variation of constipation and other health issues. These were used to calculate the weighting factor for the questionnaire sample (see above).
Prevalence of constipation in the general population
Based on the definition of constipation as used in the interviews, prevalence rates were 14.9% (been constipated in the last 12 months), 5.8% (constipation during the last 4 weeks), and 2.6% (currently constipated); 2.6% had ever consulted a doctor for constipation, 4.4% had taken medication because of their constipation. More men than women had consulted a doctor for constipation (22 versus 19% of all, p < .001), but more women than men had taken medication because of it (29 versus 32%, p < .001).
The 12-months prevalence varied according to age and gender, with women reported more constipation than men at a ratio of 2.3:1 (Figure 1). Taken together, participants with constipation of any kind were 49.6 ± 18.0 years. On average, constipation was present for 2.68 ± 1.99 years, and 80% reported having constipation for more than 6 months.
Prevalence (%) of constipation in the GECCO sample in men and women across different age groups. The 2:1 ratio diminishes with increasing age.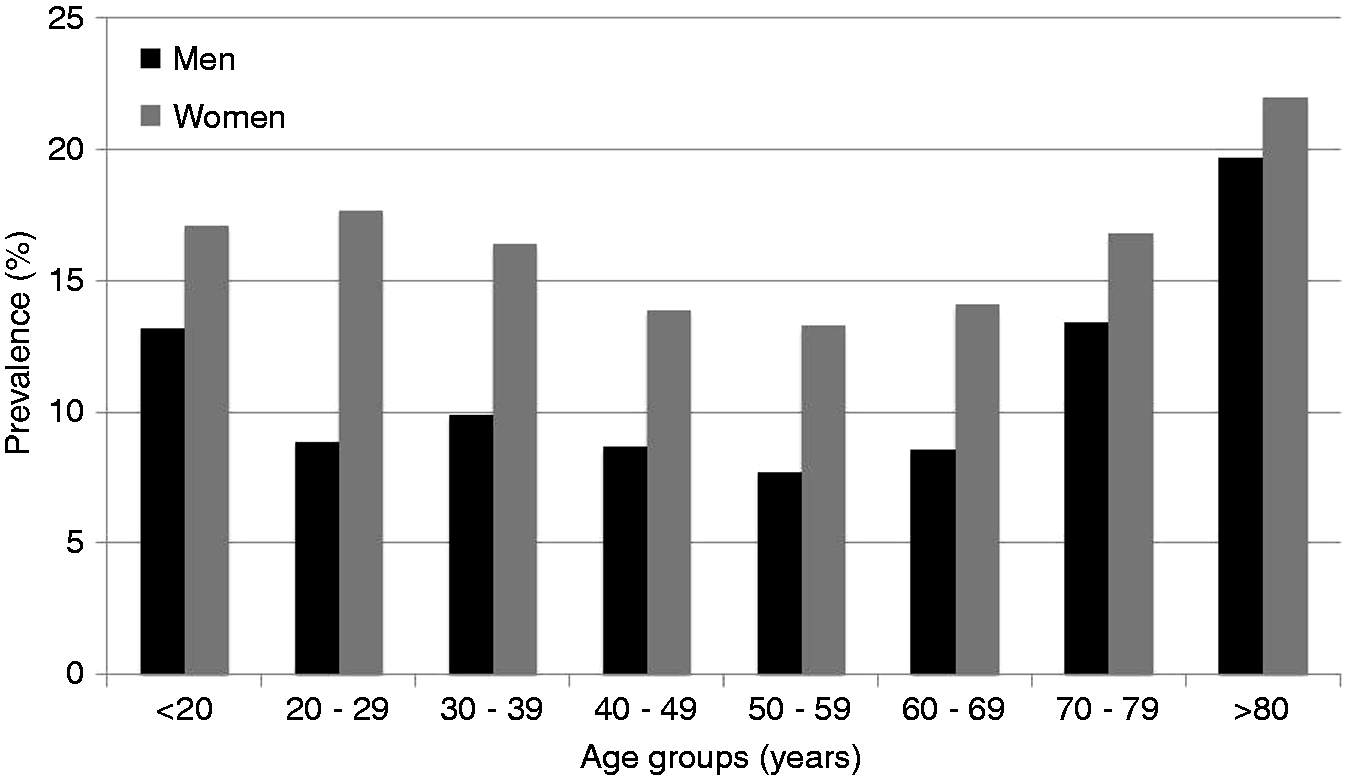
Constipation characteristics among participants in the survey (n = 2239)
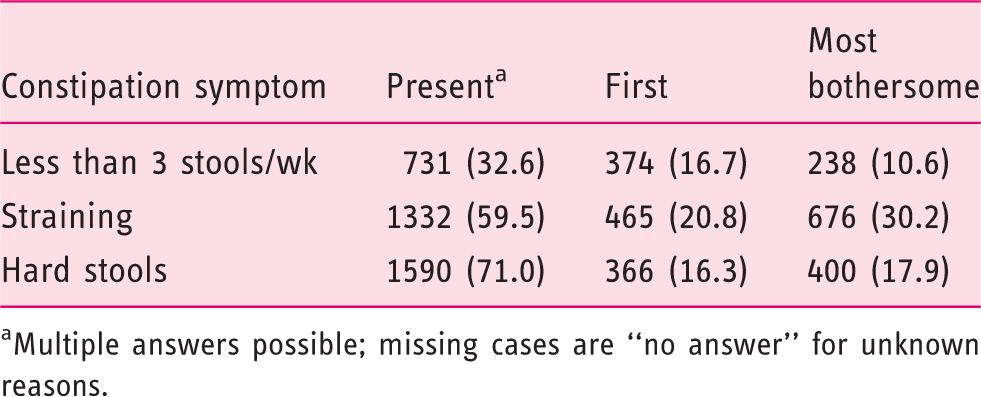
Multiple answers possible; missing cases are “no answer” for unknown reasons.
Of all 1849 respondents that provided answers, the majority experience two of the three symptoms (n = 837, 45%), 499 (30%) report all three, and among those that reported only one of the three (n = 543), hard stool was the most important single symptom (n = 310, 17%). If straining is present, it appears to be an early symptom and the most bothersome, as compared to the others.
Constipated versus non-constipated
When all constipated (n = 2,239) were compared to all non-constipated (n = 12,763) in the sample, a number of characteristics were found. The constipated were of similar age than the non-constipated (49.3 ± 17.9 vs. 50.6 ± 20.1, n.s.) but included a higher proportion of women (64.2% vs. 49.2%, p < .001); in consequence, they had lower height (169 ± 9.6 vs. 172 ± 9.5 cm, p < .001) and weight (74.8 ± 17.7 vs. 76.9 ± 16.2 kg, p < .001) but an equal body mass index (BMI) (26.0 ± 5.2 vs. 25.8 ± 4.8, n.s.).
Absolute and relative (%) health problems and life satisfaction in constipated and non-constipated
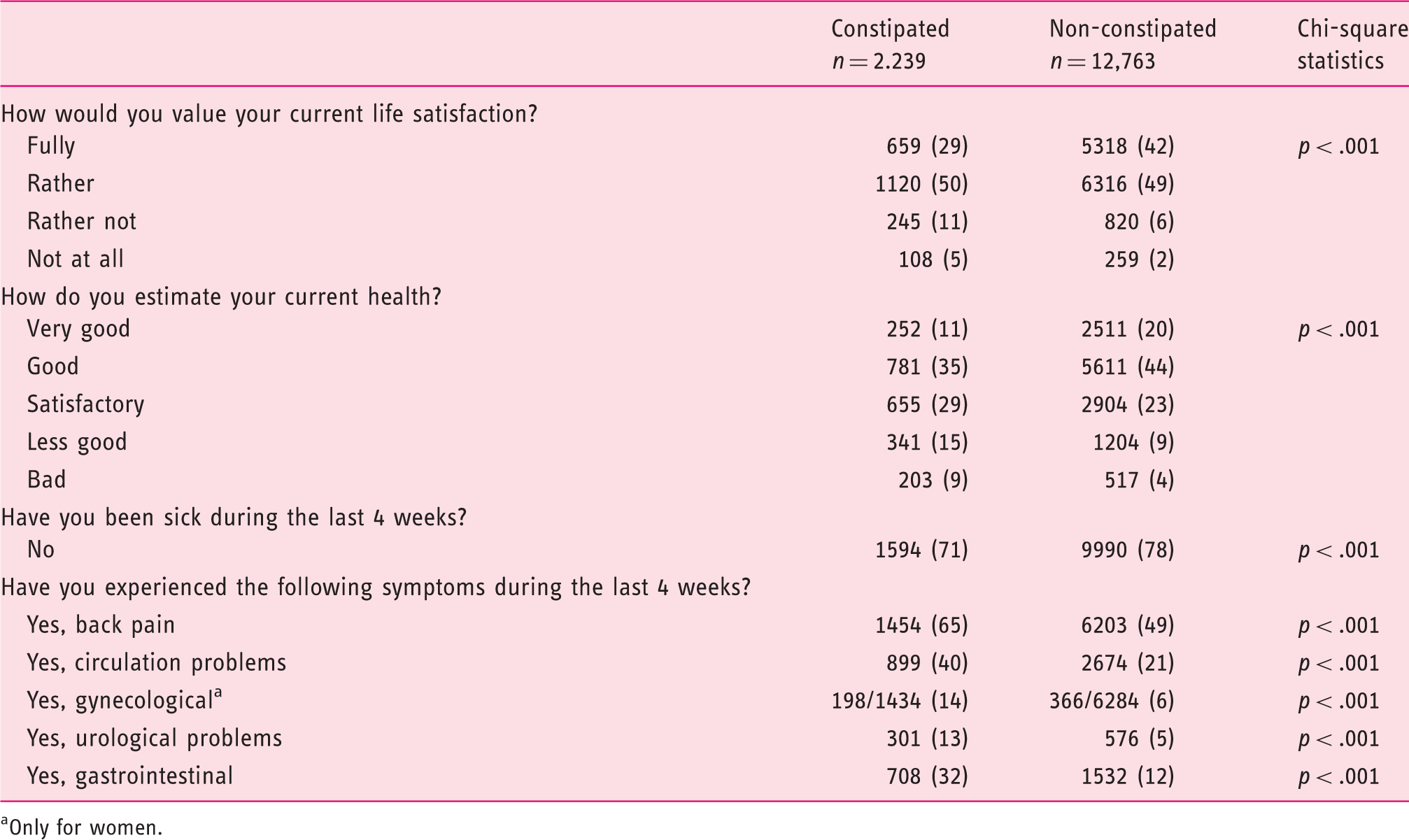
Only for women.
Absolute and relative (%) sociographics; missing cases are “no answer” for unknown reasons
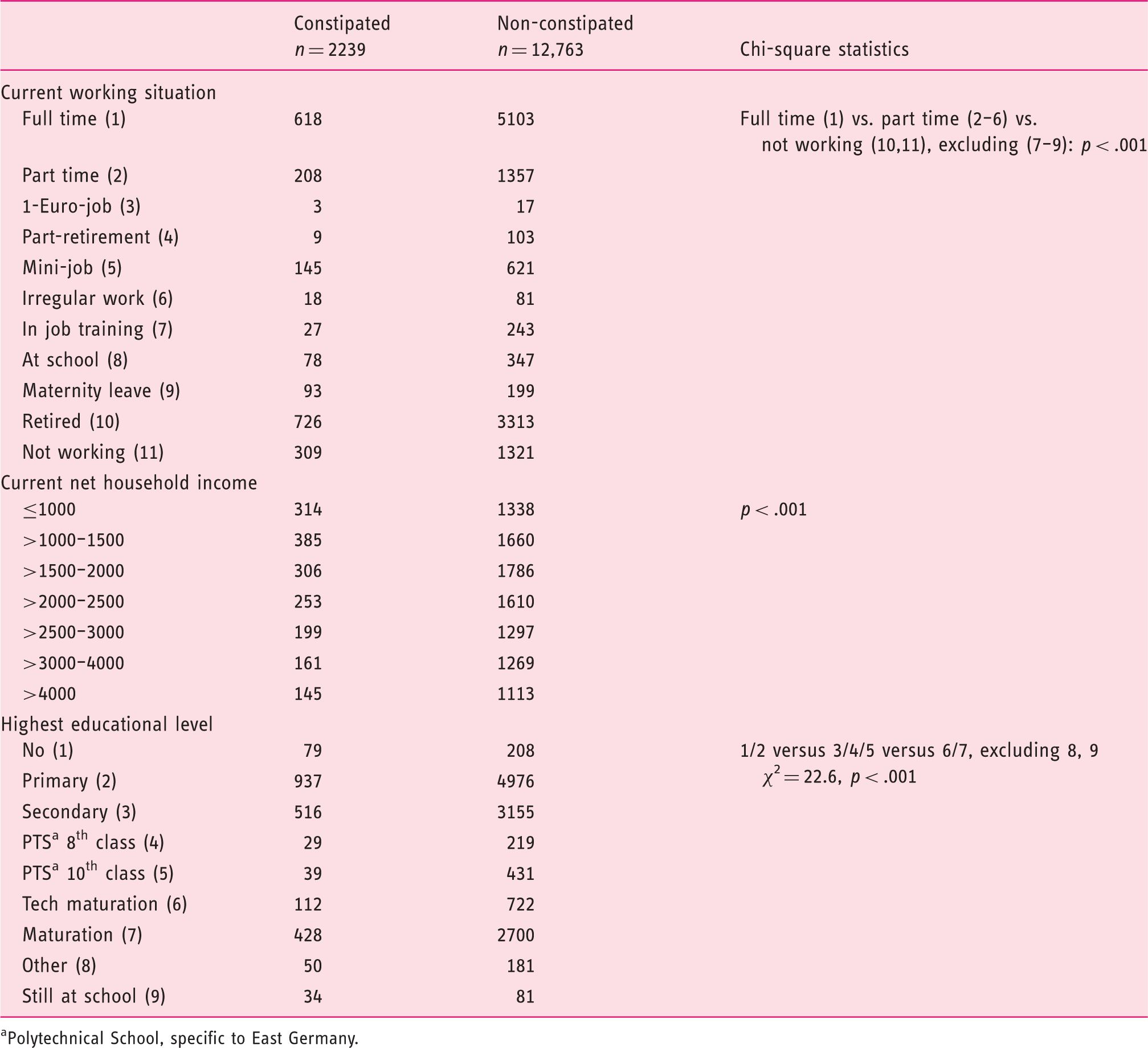
Polytechnical School, specific to East Germany.
Discussion
Our population survey, representative for Germany, generated a number of surprising as well as confirming results.
The prevalence of constipation in the general population (in Germany) is higher (14.9%) than previously reported (5%), 4 and similar to data for other European and non-European countries;1–5 it is almost equal to the pooled prevalence of 14% across 18 countries in 41 studies. 5 It varies, however, with the definition of type and severity of the condition. This may to a large degree explain the variability (between 2 to 30%) that can be found in epidemiological reports, depending also on the type of assessment. It has been noted, for instance, that electronic health record data report lower prevalence rates for a number of symptoms including constipation than do population health surveys, 31 and reports from internet-based self-selection surveys may overestimate rates in comparison to representative population samples. 32 However, different assessment modalities have their advantages and pitfalls and, therefore, a certain degree of “noise” in the data may be acceptable in light of the achievable depth of the data.
The prevalence of constipation increased with age, was more frequent in women, and the constipated had overall lower health status and life and health satisfaction. This is in full agreement with many previous reports,7,8 underlining the quality of our survey. While the higher prevalence of constipation in women is well known across all nations, the reason for this female predominance is not. The unequal distribution of men and women among the constipated may be due to female sex hormones and their change during the menstrual cycle, 33 a slower colonic transit, 34 and differences in dietary habits and transit-promoting foods. 35 The sex distribution is even more skewed among patients attending medical care, 36 owing to differences in consulting behavior and healthcare seeking. 37 However, some of these factors have been challenged. Promoting more probiotic intake to counteract obesity (and maybe other diseases) has been shown to be effective in women but not in men, 38 shedding light on a potential novel factor that has yet to be evaluated, the role of the gut microbiota in constipation. 39
Less well established is also the association of constipation with lower income and social status. This has been noted before;5,9 it is usually attributed to poorer nutritional and other health behaviors in lower social classes, but such an effect has never been strongly confirmed. For example, the National Health and Nutrition Examination Survey, 11 including >10,000 men and non-pregnant women, could not confirm a predictive role of fiber intake on constipation, while low liquid consumption was associated with higher constipation rates. Since overall the constipated were marginally older than the non-constipated in our survey, differences in social status may as well be a consequence of lower family income after retirement. The higher degree of retirement in the constipated despite similar age than non-constipated could also point towards other co-morbid conditions that may or may not be directly related to the constipation, e.g. neurological or systemic disorders,40,41 or adverse events of medications taken for these conditions.
QoL is lower in patients and subjects with chronic constipation, which has been shown in many respective studies around the world.23,24 This is usually done with the help of generic QoL scales such as the SF12, 42 but constipation-specific QoL scales have also been developed. 22 Most of these are, however, not suitable for oral questioning during a telephone survey, and due to time restraints we limited our questioning to the assessment of an overall life satisfaction and health on global visual analog scales. This showed the constipated to be less satisfied with their health and their life than the non-constipated. It will need to be shown in subsequent analyses whether such simple questioning has the same exploratory value than more detailed QoL scales.
We were unable to verify any matching of the constipated volunteers with approved or proposed diagnostic criteria, such as the Rome criteria for functional constipation (FC) or constipation-predominant irritable bowel syndrome (IBS-C), 43 during this short (10 min) telephone interview; we will attempt this with the questionnaire data. Other authors have looked for differences between patients with FC matching or not matching Rome criteria and IBS-C according to the Rome criteria. Rey et al. could not see differences in QoL (SF12) between painful and non-painful constipation and IBS-C (21), but found patients with painful (n = 30) or painless constipation (n = 209) not matching IBS-C criteria (n = 49) to be moderately younger, and more frequently consulters in comparison to IBS-C, while Zhao et al., 44 comparing IBS-C (n = 183) to FC (n = 948), showed IBS-C only to have a lesser need to strain, but more incomplete evacuations after defection. Only the mental health subscale of the SF-36 was significantly lowered in IBS-C. Some differences were found with respect to upper GI symptoms not assessed in our survey. Koloski et al. compared 206 patients meeting Rome criteria for FC to 106 patients with IBS-C and found only a few differences between both groups: 45 a higher age at constipation onset for FC, less likelihood to exercise, and, similar to Zhao et al., 44 higher mental health compared to IBS-C. Finally, Heidelbaugh et al. identified and compared 552 patients with chronic idiopathic constipation with or without abdominal pain and 326 IBS-C patients and found both IBS-C and constipation with pain significantly more bothering than constipation without pain. 46
A few limitations need to be acknowledged, beyond those that were already mentioned above. For one, a low response rate of 30% towards unsolicited phone calls and interview requests may surprise, but is typical for marketing approaches. In contrast, once people have agreed to enter the interview, the compliance rate was rather high throughout the interview. To avoid focusing the telephone interviewees on GI symptoms in general and constipation especially and thereby promoting a self-selection bias, we only asked for GI symptoms in general and hidden among a number of other bodily complaints, and only if these were acknowledged, narrowed the focus somewhat down on constipation. Therefore, a more detailed questioning on the kind of symptoms (e.g. for matching Rome criteria) and their effects on daily life (using validated quality-of-life tests) was postponed and planned for a subsequent questionnaire study. The same holds true for concurrent co-morbid conditions, current medication intake, and the relation of constipation to nutritional habits.
Overall, however, we feel that our survey served the purpose it was implemented for: it corrected the prevalence numbers for Germany, and demonstrated a high prevalence of constipation symptoms in the general population, with more women than men affected, but this difference diminishes with age. To further summarize, our results also show that constipation is frequently associated with other health gastrointestinal as well as extra-intestinal problems, an overall lower quality of life, and lower social status, as measured by income and formal education.
Footnotes
Acknowledgements
We would like to thank Alain Joseph (Shire, Eysins, Switzerland) and Paul Hodgkins (Shire Development LLC, Wayne, PA, USA) for their help during development of the questionnaire.
PE had the idea for the study, and PE and JSK designed the interview and questionnaire. JL, MS, and TK contributed to interview and questionnaire design, supervised the data collection performed “in-house” at infas, conducted quality-control measures of the data, and provided the raw data (tabled, as SPSS file) to PE and JSK who evaluated the data and wrote the manuscript.
Funding
This work was supported by a grant from Shire-Movetis NV, Belgium.
Conflict of interest
JL, MS, and TK are employees of infas Institute, Bonn, Germany and conducted the study based on a contract with the University Hospital Tübingen.