
Abstract
Purpose
The rise in oesophageal adenocarcinoma incidence in women with age is delayed compared with men until the post-menopausal period. A matched cohort study was therefore undertaken of post-menopausal women on hormone replacement therapy (HRT) to examine the association between HRT, oesophageal cancer and the potentially associated conditions, reflux oesophagitis and Barrett’s oesophagus.
Methods
Women aged over 50 years within the UK General Practice Research Database with a history of HRT exposure were matched by age and general practice with controls without HRT exposure (1:1). Matched Cox-regression analysis was performed to estimate adjusted hazard ratios.
Results
51,851 HRT users and controls were studied. Prolonged HRT use for 5–10 years (hazard ratio 0.25 (95% CI 0.07–0.95)) and time-dependent covariates for increasing duration of HRT use (0.06 (0.01–0.43)) were associated with a reduced oesophageal cancer risk. HRT use was associated with reflux oesophagitis (1.27 (1.12–1.43)), but when analysis was confined to women with codes for both reflux oesophagitis and endoscopy there was no association (1.1 (0.81–1.44)), suggesting increased reporting of reflux symptoms among HRT users rather than an association with endoscopic reflux oesophagitis.
Conclusion
Long-term post-menopausal HRT may be associated with a reduced risk of oesophageal cancer.
Keywords
Introduction
The male predominance for oesophageal squamous cell carcinoma can be explained by differences in risk factors such as alcohol and tobacco consumption. However, the more marked male predominance for oesophageal adenocarcinoma remains unexplained by established risk factors such as reflux symptoms and obesity. 1 A recent study of patients with oesophageal adenocarcinoma found that uniquely among cancers, the age-specific incidence was delayed by 17 years in women compared with men, and one possible explanation is a potential protective effect of sex hormones in menstruating women. 2
Studies on post-menopausal women have shown that systemic and topical oestrogen therapy are associated with accelerated cutaneous wound healing compared with age-matched controls.3,4 The same phenomenon may plausibly occur in oesophageal injury, raising the possibility that oestrogen may limit the severity of oesophageal injury in response to gastro-oesophageal reflux. Severe oesophageal reflux injury has been proposed be a pre-requisite for the development of Barrett’s oesophagus, which in turn is thought to be a pre-requisite for the development of oesophageal adenocarcinoma.5,6
A previous nested case-control study within the UK General Practice Research Database (GPRD) examined the influence of hormone replacement therapy (HRT) among women with oesophageal adenocarcinoma and found no association between oesophageal adenocarcinoma and HRT use, but found a strong inverse association between HRT and gastric cancer. 7 The authors of the study were unable to examine the use of HRT for prolonged periods or the influence of HRT on the potentially related conditions of Barrett’s oesophagus and reflux oesophagitis. Furthermore, there is recent evidence to suggest an inverse association between oesophageal cancer and HRT use. 8 We have therefore re-examined the influence of HRT on oesophageal cancer, Barrett’s oesophagus and reflux oesophagitis in a matched cohort of post-menopausal women.
Materials and methods
General Practice Research Database
The UK GPRD has been described in detail, and validation studies have demonstrated the high quality of data recorded in the GPRD.9–11 We obtained access to the GPRD under the Medical Research Council licence which restricts datasets to around 100,000 subjects or just over. Ethics approval for the study was obtained under the provisions of the ISAC (Independent Scientific Advisory Committee) approval process for GPRD (protocol number 09-005RA).
Sample size estimation
The incidence of oesophageal adenocarcinoma in women over the age of 50 years is 14 per 100,000 per year (personal communication from West Midlands Cancer Intelligence Unit, Birmingham, UK), corresponding to seven cases per year in a sample of 50,000 subjects and 35 cases in 5 years. Assuming that HRT is at most associated with a reduction of oesophageal cancer by 50%, a sample size of 50,000 women exposed to HRT and followed for at least 5 years would provide 80% power at the 5% significance level to detect this association.
Study design
A matched cohort study using data from the GPRD between 1 January 1987 and 31 October 2008 was conducted. In total, 51,851 women between 50 and 80 years of age with a prescription code for HRT at least twice per year for a minimum of 1 year and the same number of women without a record of having been prescribed HRT, matched by age within 5 years, general practitioner (GP) practice and duration on the GPRD, were identified. Women were excluded if they had a disease code for Barrett’s oesophagus or oesophageal cancer before or 6 months after the first date of HRT prescription and from the reflux oesophagitis analysis if they had a code for reflux oesophagitis prior to starting HRT. Women with less than 1 year of follow-up or those developing oesophageal cancer within 12 months of registration at the general practice were also excluded.
The cohort was followed longitudinally in the database until development of oesophageal cancer, death or exit from the database. Dates of diagnosis of reflux oesophagitis, Barrett’s oesophagus and oesophageal cancer were extracted to analyse the temporal sequence of events. Data on use of lower oesophageal sphincter relaxing drugs and co-morbid conditions were additionally analysed.
HRT exposure
All forms of HRT were considered during the analysis, including oral, transdermal preparations and oestrogen implants. ‘Current’ users were defined as women who were on HRT during their time on the database, as opposed to ‘ever’ users, who had been exposed to HRT at some point in the database. A similar exposure window in each matched women in the unexposed (control) group was defined. HRT use was further stratified by duration of exposure (in years) to exposure windows of 0–2 years, 2–5 years and 5–10 years of HRT use.
Oesophageal cancer histology
Histology of each oesophageal cancer was sought by examining anonymized free text attached to each subject in the GPRD by searching for the following terms: oesophageal adenocarcinoma, oesophageal squamous cell carcinoma or squamous cell cancer, oesophageal cancer, oesophagectomy, chemotherapy, radiotherapy and neo-adjuvant. Oesophageal cancer was then divided into three groups: adenocarcinoma, squamous cell carcinoma and indeterminate (when histology was not available).
Statistical analysis
Skewed data were initially log transformed for analysis. Categorical data were compared between groups using the Chi-square test. Matched Cox-regression analysis was used to examine the relationship between HRT use and the risk of reflux oesophagitis, Barrett’s oesophagus and oesophageal cancer and hazard ratios with 95% confidence intervals (CI) were calculated. Time-dependent covariates were additionally used to examine the effect of length of HRT use on the risk of reflux oesophagitis, Barrett’s oesophagus and oesophageal cancer.
Results
Study cohort
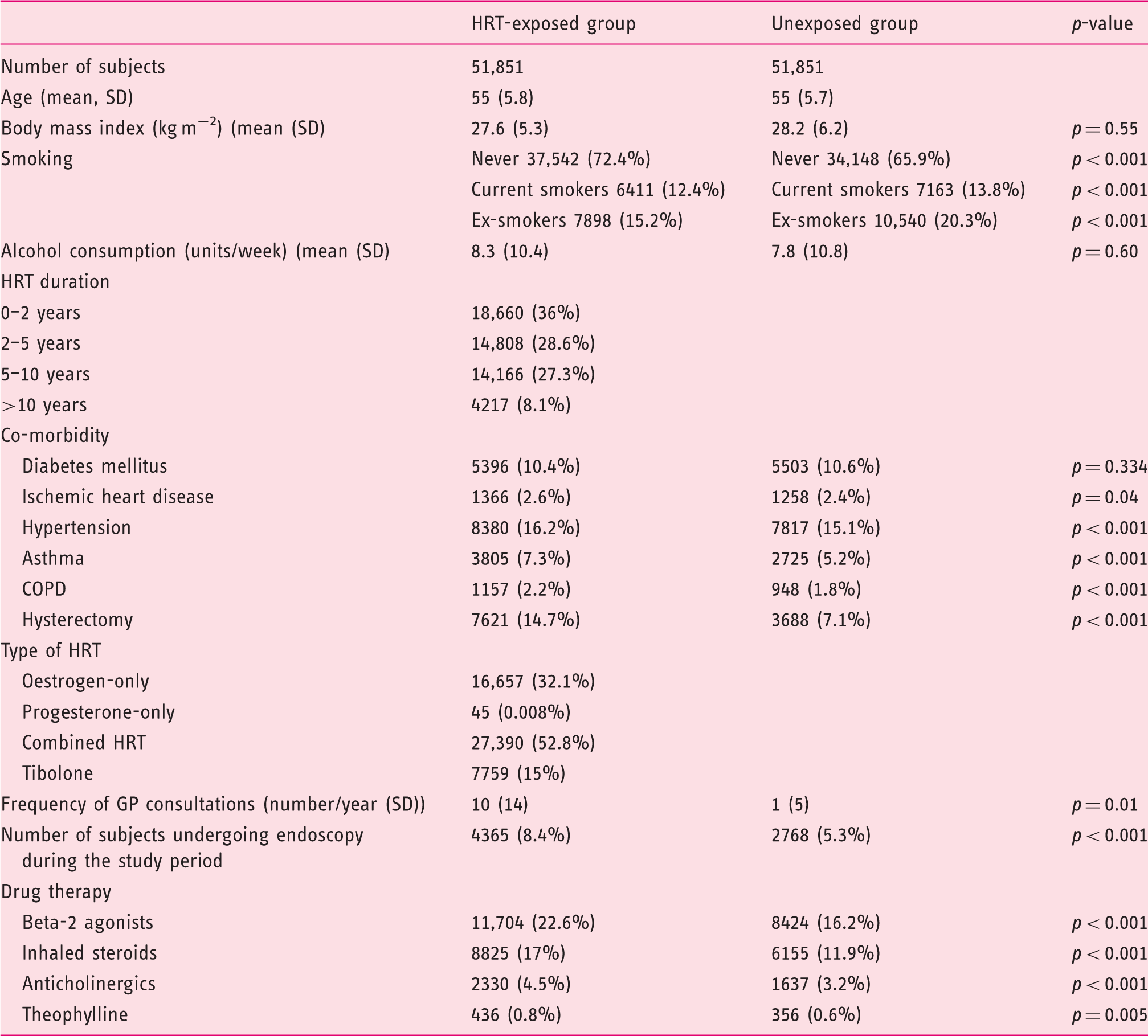
The demographic characteristics of the study cohort
Oesophageal cancer
Univariable analysis of risk factors associated with oesophageal cancer, Barrett’s oesophagus and reflux oesophagitis in the study cohort

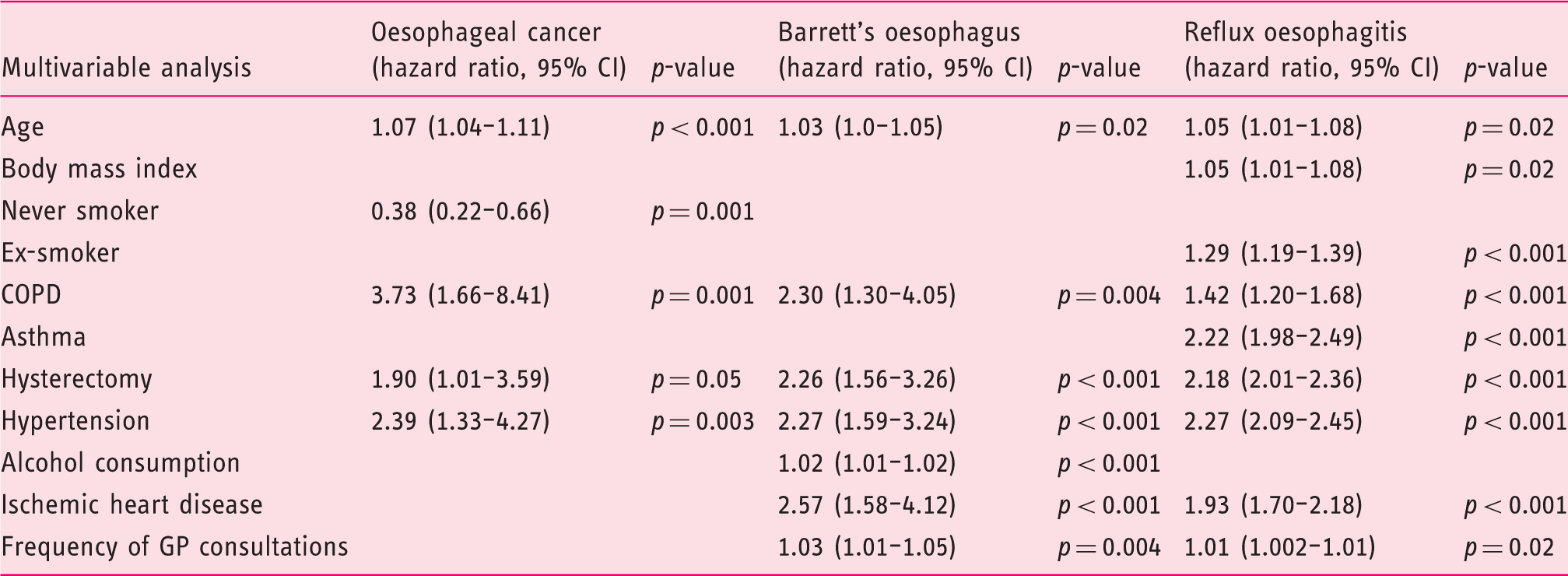
Multivariable analysis of risk factors associated with oesophageal cancer, Barrett’s oesophagus and reflux oesophagitis in the study cohort
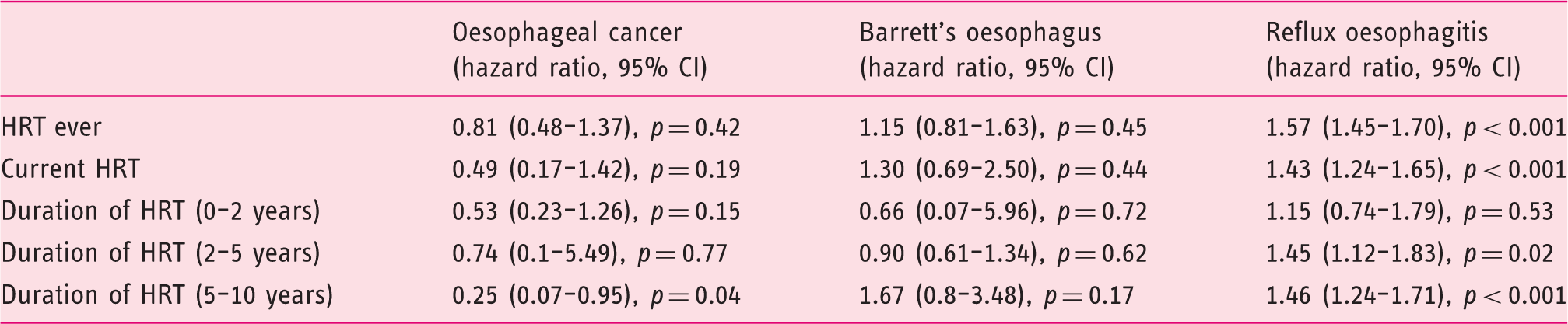
Hazard ratios for oesophageal cancer, Barrett’s oesophagus and reflux oesophagitis in women exposed to HRT relative to matched controls by duration of HRT exposure
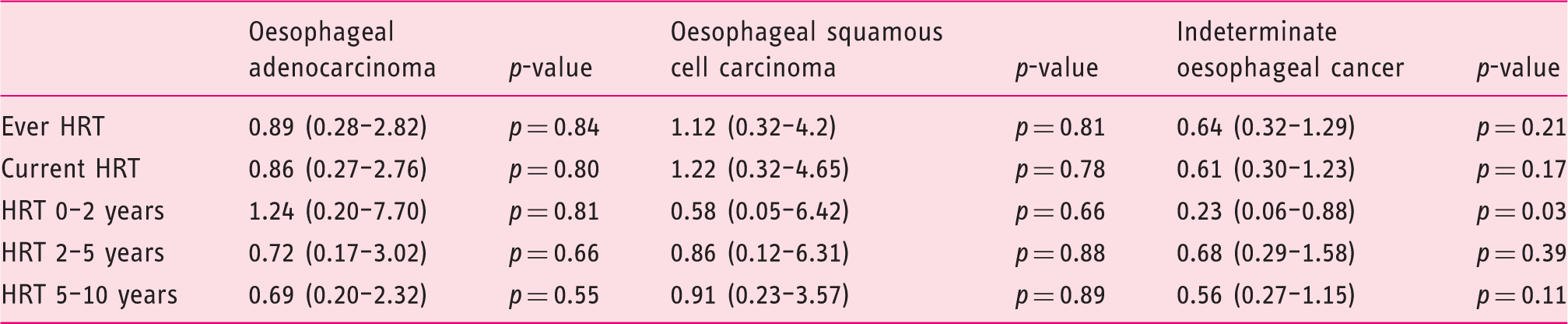
Hazard ratios for oesophageal cancer histological subtypes for in women exposed to HRT relative to matched controls
Barrett’s oesophagus
There were 78 cases of Barrett’s oesophagus in the HRT-exposed group compared with 76 in the unexposed group. Univariable analysis identified that age, alcohol consumption, COPD, asthma, diabetes mellitus, hypertension, ischemic heart disease, hysterectomy, frequency of endoscopy and GP consultations and beta-2 agonist therapy were associated with Barrett’s oesophagus (Table 2). Multivariable analysis revealed that age, alcohol consumption, COPD, hypertension, ischemic heart disease, hysterectomy and frequency of GP consultations were associated with Barrett’s oesophagus (Table 4). These variables were adjusted for in subsequent analyses.
‘Ever’ HRT exposure (1.15 (0.81–1.63), p = 0.45)) and current HRT (1.30 (0.69–2.50), p = 0.44)) were not associated with Barrett’s oesophagus (Table 4). Increasing duration of HRT was also not associated with Barrett’s oesophagus. Duration of HRT use was examined further by using time-dependent covariates and there was no association between length of HRT use and risk of Barrett’s oesophagus (0.94 (0.58–1.55), p = 0.82). Analysis by subtype of HRT did not reveal an association with Barrett’s oesophagus (data not shown).
Reflux oesophagitis
There were 2221 women with codes for reflux oesophagitis in the HRT-exposed group compared with 1467 in the unexposed group. Univariable analysis identified that age, body mass index (BMI), smoking (current and ex-smoking positively associated and never smoking negatively associated), COPD, asthma, diabetes mellitus, hypertension, ischemic heart disease, hysterectomy, frequency of endoscopy and GP consultations, beta-2 agonist and inhaled steroid therapy were associated with reflux oesophagitis (Table 2). Multivariable analysis identified age, BMI, ex-smoking status, COPD, asthma, hypertension, ischemic heart disease, hysterectomy and frequency of GP consultations were associated with reflux oesophagitis (Table 3). These variables were controlled for in subsequent analyses.
Both ‘ever’ HRT use (1.57 (1.45–1.70), p < 0.001) and current HRT use (1.43 (1.24–1.65), p < 0.001) were associated with reflux oesophagitis (Table 4). Analysis by subtype of HRT suggested that ‘ever' but not current use of Tibolone was associated with reflux oesophagitis (1.22(1.06–1.41, p = 0.01) but no association was found with oestrogen, progesterone or combined HRT use and reflux oesophagitis (data not shown). However, exclusion of women who were on proton pump inhibitor (PPI) therapy prior to their initial HRT prescription weakened the association of HRT with reflux oesophagitis (1.27 (1.12–1.43), p < 0.001). Furthermore, time-dependent covariates revealed no association between duration of HRT use and reflux oesophagitis (1.05 (0.97–1.14), p = 0.23). Finally, we examined whether the association between HRT use and reflux oesophagitis might relate to women being coded in primary care with reflux oesophagitis based on acid reflux symptoms rather than an endoscopic diagnosis. Selecting women coded for both reflux oesophagitis and endoscopy and who were not on PPI therapy prior to their HRT prescription revealed no association between HRT use and reflux oesophagitis on multivariable analysis (1.1 (0.81–1.44)). This suggests an association between HRT use and reflux symptoms rather than endoscopic reflux oesophagitis.
Discussion
A lag of 17 years has been reported among women developing oesophageal adenocarcinoma compared with men, and this seems to coincide with the onset of the menopause in women. 2 We recently reported an acceleration in the incidence of endoscopic reflux oesophagitis in women after the age of 50, with the incidence of reflux oesophagitis in women finally catching up with that in men by age 80. 12 We hypothesized that a lack of systemic oestrogen in post-menopausal women may be responsible for this phenomenon by providing some protection from reflux induced damage prior to the menopause.
Oestrogen has been shown to have anti-inflammatory properties with modulation of immune cell activity including changes in cytokine production, cell activation and proliferation and wound healing.13–22 Oestrogen replacement in the form of HRT in post-menopausal women may therefore potentially confer a protective effect against oesophageal cancer by lessening the extent of oesophageal injury due to acid reflux and therefore reducing the risk of Barrett’s oesophagus and oesophageal adenocarcinoma.
In the present study, ‘ever’ use of HRT was not associated with oesophageal cancer, as reported in a previous study of HRT and oesophageal cancer. 7 However, examining prolonged HRT use in the present study revealed that HRT use for 5–10 years was associated with a lower risk of oesophageal cancer. Time-dependent covariates were used separately to determine the effect of length of HRT use on the risk of oesophageal cancer, and again using HRT for longer was associated with a lower risk of oesophageal cancer. The results of the present study are consistent with a recently published nested case-control study within the GPRD examining the effect of HRT use in women over 50 years of age on the risk of oesophageal, gastric and colorectal cancers. 8 The authors reported a negative association between oesophageal cancer and ever use of HRT (0.68 (95%CI 0.53–0.88)). Furthermore, a meta-analysis of four other studies gave a summary relative risk of 0.68 (0.55–0.84) for oesophageal cancer in HRT-exposed women. 8
Our hypothesis would suggest that prolonged HRT use would be associated with a larger reduction in the incidence of oesophageal adenocarcinoma than oesophageal squamous cell carcinoma. Unfortunately, histological subtype data was only available on 41% of oesophageal cancers. Consequently, the number of cases was too small to identify significant associations with different oesophageal cancer histological subtypes. However, a meta-analysis of the influence of HRT on oesophageal squamous cell carcinoma, oesophageal adenocarcinoma and oesophageal cancer described above reported similar reduced risks in studies of oesophageal adenocarcinoma and oesophageal squamous cell carcinoma with no significant heterogeneity. 8 This suggests that HRT may potentially also mitigate against the inflammatory injuries (e.g. smoking and alcohol) that contribute to the aetiology of oesophageal squamous cell carcinoma, as well as gastro-oesophageal reflux injury in oesophageal adenocarcinoma.
HRT use was modestly associated with codes for reflux oesophagitis. An association between HRT use and acid reflux symptoms has been described in a prospective cohort study among women enrolled in the Nurses Health Study, with a similar modest increased risk in ever and current HRT users.23,24 Oestrogen-only, combined HRT and selective oestrogen receptor modulators (SERM) such as Raloxifene were all associated with acid reflux symptoms despite adjusting for BMI. 24 A similar association between post-menopausal HRT use and acid reflux symptoms has been reported in population-based studies. 25 This group also found an association between post-menopausal HRT use and endoscopic oesophagitis with increasing BMI. 26 Oestrogen increases nitric oxide synthesis in smooth muscle leading to smooth muscle relaxation in animal models and in humans, and may consequently reduce lower oesophageal sphincter pressure, which in turn may potentially exacerbate gastro-oesophageal reflux.27–30 There is, however, a strong possibility of residual confounding in the association between HRT and reflux oesophagitis. Reflux oesophagitis was associated with the frequency of GP consultations and a number of co-morbidities (e.g. hypertension and ischemic heart disease) with no clear aetiological link with reflux oesophagitis. Although these associations were adjusted for, it remains possible that reflux oesophagitis is more likely to be diagnosed in women taking HRT, as such women are more likely to report symptoms and request investigation or treatment of symptoms, rather than HRT contributing to the development of oesophagitis. Excluding women who had taken a PPI prior to HRT, suggesting a history of reflux symptoms, significantly weakened the strength of the association. Examining the effect of duration of HRT exposure using time-dependent covariates on risk of reflux oesophagitis revealed no association between the duration of HRT use and reflux oesophagitis, casting some doubt on a causal association between HRT and reflux oesophagitis. Finally, examination of a cohort of women who had reflux oesophagitis diagnosed following an endoscopy revealed no association between HRT use and reflux oesophagitis, suggesting that HRT use is associated with increased reporting of reflux symptoms, which is then coded as reflux oesophagitis in primary care.
The strengths of the present study include the cohort design that allowed construction of a temporal sequence of events in relation to HRT use and thereby the examination of the effects of prolonged HRT use, and the accuracy of recording of HRT prescription data within the GPRD. However, the study has a number of potential limitations. Data on important etiological factors for oesophageal adenocarcinoma were not available. Longstanding, frequent acid reflux symptoms are associated with oesophageal adenocarcinoma. 31 Although it was possible to control partly for the influence of pre-existing acid reflux in the association of HRT with reflux oesophagitis by adjusting for PPI therapy prior to starting HRT, it was not possible to accurately assess the influence of pre-existing acid reflux in the association of HRT with oesophageal cancer. Secondly, Helicobacter pylori is negatively associated with the development of oesophageal adenocarcinoma, but data on H. pylori status is not available within the GPRD. 32 Information on oesophageal cancer, Barrett’s oesophagus and reflux oesophagitis and potential confounding factors were collected prospectively in the GPRD, reducing the possibility of reporting bias. The results for Barrett’s oesophagus in the study population need to be interpreted cautiously. The prevalence of Barrett’s oesophagus in the study is very low and similar to the prevalence of oesophageal cancer, suggesting under-reporting of Barrett’s oesophagus by endoscopists or GPs from endoscopy reports. Finally, although we found an inverse association between prolonged HRT use and risk of oesophageal cancer, the overall number of cancers was small, which is reflected in the wide confidence intervals, and necessarily affects the strength of our conclusions.
HRT use has been shown to reduce the incidence of colorectal cancer by 20–30% in randomized trials and observational data.8,33–35 However, HRT use is associated with an increased risk of thromboembolic events, and there is also an increased risk of breast, endometrial and ovarian cancers. 33 HRT use has therefore declined significantly in the last decade. The role of oestrogen as an anti-inflammatory agent remains intriguing, and further study of the potential role of hormonal factors in the pathogenesis of oesophageal adenocarcinoma is merited to better understand the pronounced gender differences in this condition.
In conclusion, prolonged post-menopausal HRT use appears to be associated with a reduced risk of oesophageal cancer.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
Acknowledgements
The GPRD dataset for this study was obtained under a collaborative research licence funded by the Medical Research Council. We wish to thank Mrs. Tarita Murray-Thomas and Mr. Gerald McCann at GPRD for their assistance and advice and the Sandwell Postgraduate Trustees (Sandwell General Hospital, West Bromwich) for sponsoring this study.