
Abstract
Background
Screening by means of biennial fecal occult blood test has provided a reduction in overall colorectal cancer mortality. Notwithstanding, we should not underestimate the harms that it can produce.
Aim
The aim of this article is to identify the independent risk factors of complications after a screening colonoscopy.
Methods
A six-year, nested case-control study was conducted. Mortality/complications within 30 days after colonoscopy were registered and its predictors identified through logistic regression.
Results
After 39,254 colonoscopies, the complication rate was 1.0%. Independent predictors were sex (OR 1.68 for men; CI 95% 1.18–2.39), ASA physical status classification system (OR 1.73 for ASA II–III; CI 95% 1.53–3.69), history of abdominal surgery (OR 2.37; CI 95% 1.72–4.08), diverticulosis (OR 2.89; CI 95% 1.94–4.30), inadequate cleansing (OR 29.35; CI 95% 6.52–132.17), detection of advanced neoplasia (AN) (OR 4.92; CI 95% 3.29–7.36), detection of stage I adenocarcinoma (OR 9.44; CI 95% 4.46–20.0), polyps in right colon OR 2.27 CI 95% 1.38–3.74) and complex polypectomy (OR 2.00; CI 95% 1.25–3.20). The logistic model explained 82% of the complications (CI 95% 0.798–0.854, p < 0.001).
Conclusions
Colonoscopy, with or without removal of a lesion, is an invasive procedure with a non-deniable risk of major complications. Factors like inadequate cleansing or detection of AN are determinants. Therefore, it is vital to know which aspects predict their appearance to implement countermeasures.
Keywords
Key summary
Summarize the established knowledge on this subject:
Screening colonoscopy with polypectomy has shown to be a diagnostic and therapeutic procedure that reduces the incidence and mortality of colorectal cancer (CRC) and it is considered the gold standard in colorectal cancer detection. Although endoscopic techniques have improved over the years, they are not exempt from damage and adverse events, and different publications have shown diverse complication rates, ranging from 0.04% to 8%. Different independent factors have been identified to be related to these complications and could lead to the implementation of countermeasures. The issue is how to prioritize them by their importance. What are the significant and/or new findings of this study?
As far as we know, this is one of the few published studies that tries to identify risk factors related to the occurrence of adverse events when performing a colonoscopy in a population-based screening program with a fecal immunochemical test. This study reflects the risk associated with colonoscopies within the framework of a well-established, high participation rate and real-world practice CRC population-based screening program. The outcomes observed provide insights as to how to minimize adverse events rates, prioritize countermeasures to be established and increase the efficiency of existing programs while ensuring that the goals of reducing CRC-related morbi-mortality are reached.
Introduction
Once lesion suspicion is determined, colonoscopy is the final common denominator of all colorectal cancer (CRC) screening strategies and today is the gold standard for the detection of CRC and premalignant lesions. According to the results of a population-based case-control study, about 75%–80% of CRC cases could be prevented by colonoscopy, with a stronger effect on distal than on proximal CRCs. 1 However, this estimate was not corrected for self-selection bias.
Since well-designed and implemented screening programs demonstrate effectiveness, CRC is one of the most preventable cancers. Several studies have shown that CRC screening programs in average-risk individuals reduce the incidence and mortality.2–8 In contrast with other screening programs, such us lung, prostate or breast cancer, CRC screening focuses not only on early-stage cancer detection, but also on detecting and removing precancerous lesions (adenomas). 9 Moreover, CRC screening programs have been shown to be a highly cost-effective health care strategy.10,11
However, we must not underestimate the occurrence of adverse effects such as colonoscopy complications. In fact, a population-based screening program should not be implemented when the risks of the diagnostic and management tests required to run the program are not assumable from the ethical point of view, in order to ensure high-quality care. Overall pooled colonoscopy complication prevalence in a recent published meta-analysis for post-colonoscopy perforation, bleeding and mortality is 0.5/1000 (95% confidence interval (CI) 0.4–0.7), 2.6/1000 (CI 95% 1.7–3.7) and 2.9/100,000 (CI 95% 1.1–5.5) colonoscopies. 12
Different risk factors have been reported to be related to colonoscopy complications. The main factors are related to the size, location and shape of the polyp.13–20 Other reported risk factors include cardiovascular or chronic renal disease, 19 age,16,18 anticoagulant treatment, 19 poorer bowel preparation 19 and body mass index. 14 Cutting mode of the electrosurgical current and the inadvertent cutting of a polyp before current application have also been proved to be independent risk factors for immediate post-polypectomy bleeding. 19 The risks of serious adverse events following colonoscopy performed as part of screening are low, but there are also related risk factors, such as age and polypectomy. 20
Based on the recommendations of the European guidelines of 2010 8 and the Spanish Strategy against Cancer validated in 2009, 21 population-based screening for CRC was approved by the Basque Autonomous Government and implemented in 2009. One of the challenges of CRC screening programs and, therefore, that implemented in the Basque Country, is efficiency; hence, the reduction of incidence and morbi-mortality is the main scope, but embracing the minimum if any and acceptable adverse events. For this purpose, it is critical not only to identify and analyze screening colonoscopy complications, but also to try to implement strategies to reduce them. That is the reason why the aim of this study is to identify the independent risk factors of complications after a colonoscopy in the Basque CRC Screening Program. At the same time, this analysis could guide other similar programs when considering the risks in order to act on and minimize them.
Patients/Material and methods
Design and setting
We conducted a nested case-control study in the Basque Colorectal Cancer Screening Program (BCCSP). The screening is based on the detection of occult blood in feces using a biennial quantitative immunochemical test (FIT), targeting women and men between 50 and 69 years of age (approximately 977,819 invitations) and a colonoscopy under sedation for FIT-positive cases.
The colonoscopies were performed in publicly funded hospitals by qualified and trained specialists. All colonoscopies are reviewed and codified within 10 days to assess possible complications. Every three months, all cases are linked to the register of hospital discharges in order to identify all cases that have had an episode of admission within 30 days after colonoscopy.
Study participants
We included participants in the program with a positive FIT and who had had a colonoscopy performed. It was considered a case when a complication was identified as defined in the European guide on CRC screening: 8 hospitalization within 30 days for serious hemorrhage involving transfusion, or for perforation, vagal syndrome or peritonitis-like syndrome and death attributed to complications of a screening colonoscopy.
Cases were randomly selected from colonoscopies performed by the same endoscopy unit over the same week, matching each with the identified complication (Figure 1).
Selection of cases and controls for the study, 2009–2014.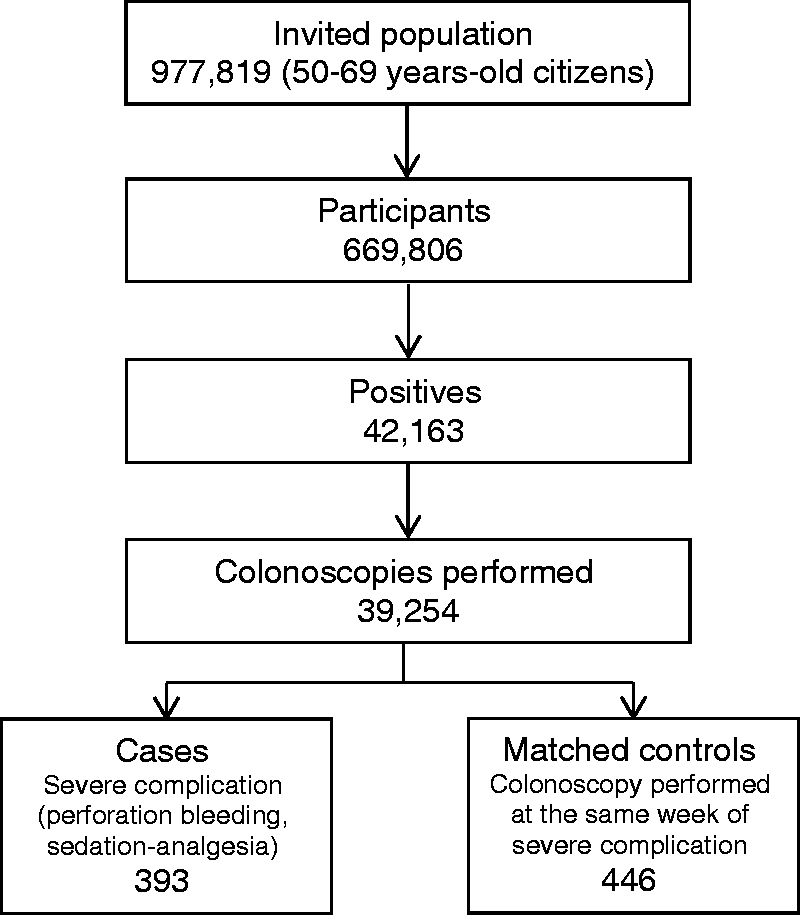
Potential independent factors
As potential independent factors, we collected the following data: age, sex, weight and height, comorbidities, deprivation index, American Society of Anesthesiologists physical status classification system (ASA), anticoagulant/antiplatelet treatments, previous abdominal surgery, diverticulosis, bowel cleansing, cecal intubation, polypectomy, lesions detected in the colonoscopy and the location/size/morphology. Size of the polyp was recorded in millimeters as informed in the histopathologic report; in those cases in which this was not documented the size estimated by the colonoscopist was recorded. To determine the number of polyps, we took the number of polyps resected. Location was categorized as rectum, distal colon (sigmoid, descending colon and splenic flexure), proximal colon (transverse, hepatic flexure and ascending colon) and cecum. Complex colon polypectomy was considered as defined by Gallegos-Orozco and Gurudu 22 as polypectomy of sessile/pedunculated polyps more than 2 cm and difficult to treat endoscopically. Adequate bowel preparation was assessed with the Boston Bowel Preparation Scale (score >6) as recommended by the European Society of Gastrointestinal Endoscopy (ESGE). 23 Adenomas ≥10 mm, adenoma with a villous component (i.e. tubulovillous/villous adenoma) or adenomas with severe/high-grade dysplasia were classified as advanced adenomas (AA). 8 Advanced neoplasia (AN) was defined as CRC plus AA.
Statistical analysis
Data are expressed as mean ± standard deviations or median and interquartile range (IQR) for quantitative variables and qualitative variables by frequency tables and percentages. For comparison between two groups Fisher’s exact test or χ 2 was used. To compare quantitative variables and categorical variables with two categories t-test or the non-parametric Mann-–Whitney U test was used. Logistic regression analysis was performed with complications as the outcome variable (dichotomous variable). Significance was set at the 5% level. The analysis was performed by IBM SPSS 23.0 and SAS 9.4.
Results
Adverse events registered.
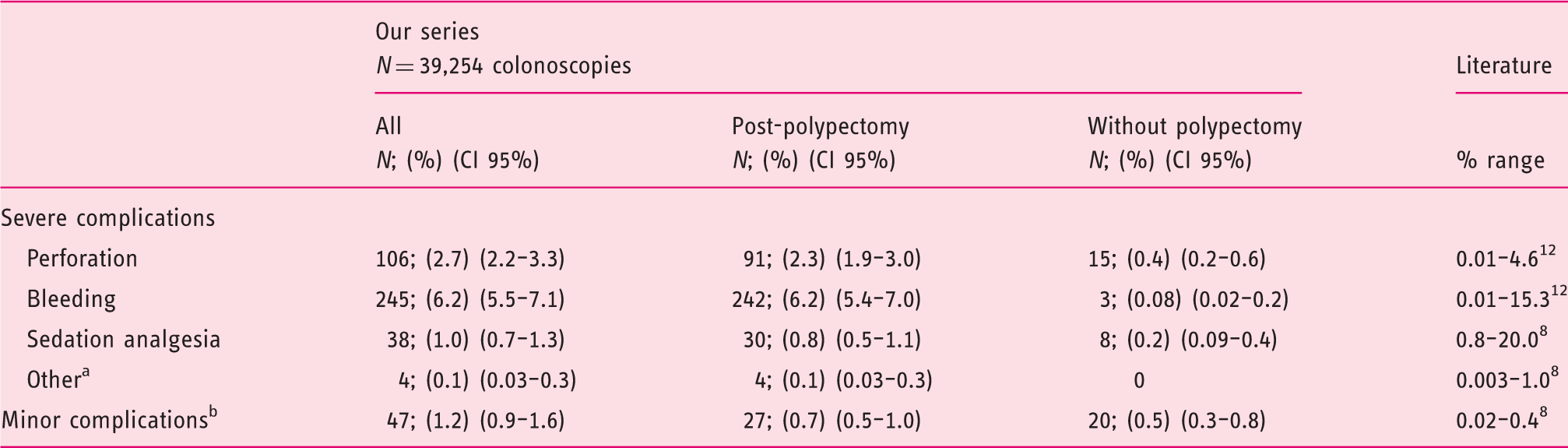
Post-polypectomy syndrome, diverticulitis and peritonitis-like syndrome.
Complications that improve spontaneously without hospitalization or emergency treatment, which can lead to interruption of the colonoscopy, such as abdominal pain, abdominal discomfort, agitation, nausea/vomiting, desaturation or heart rhythm disorder.
CI: confidence interval.
Characteristics of patients with and without adverse events (AE).
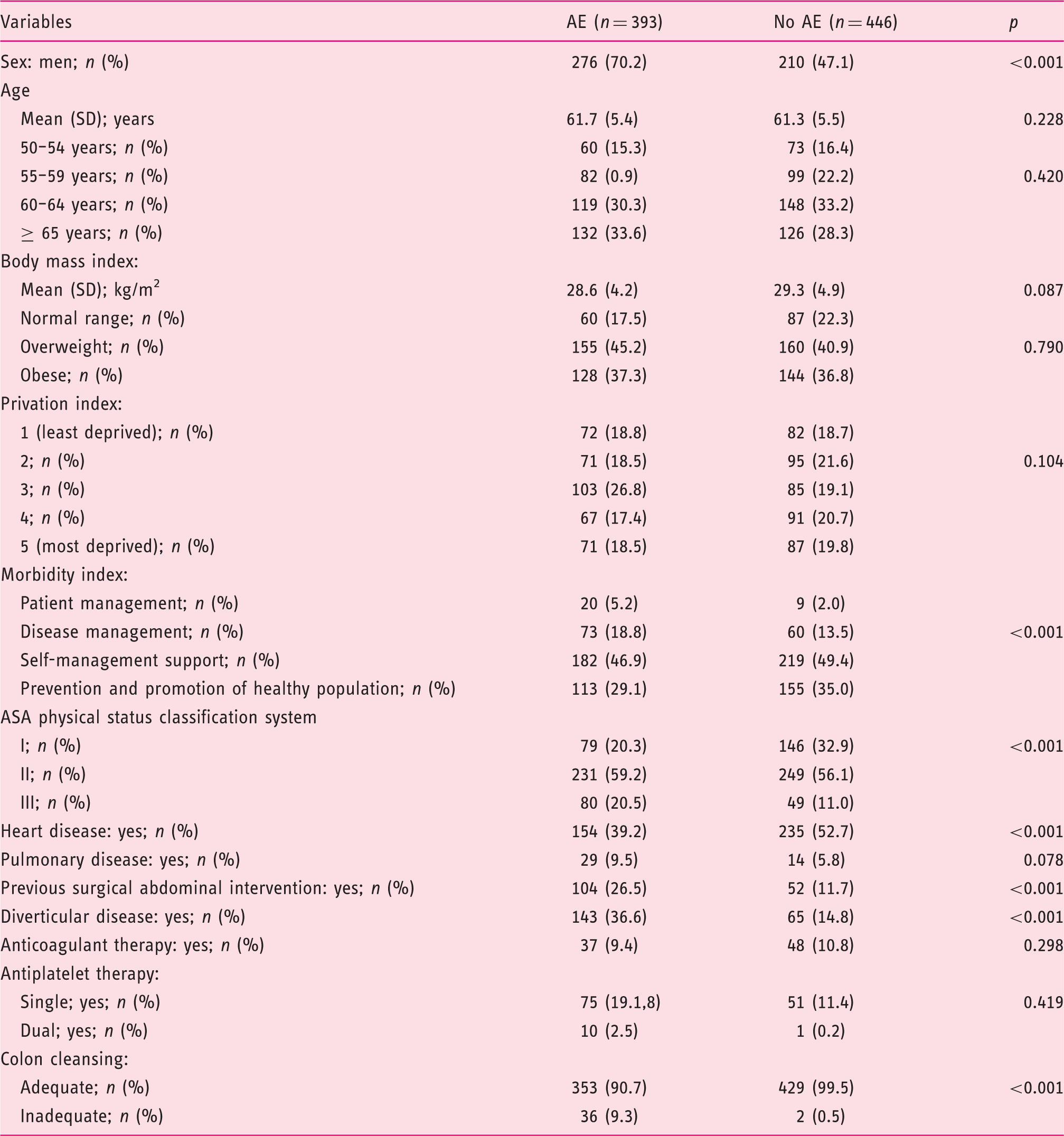
ASA: American Society of Anesthesiologists.
Characteristics of colonoscopies with and without adverse events (AE).
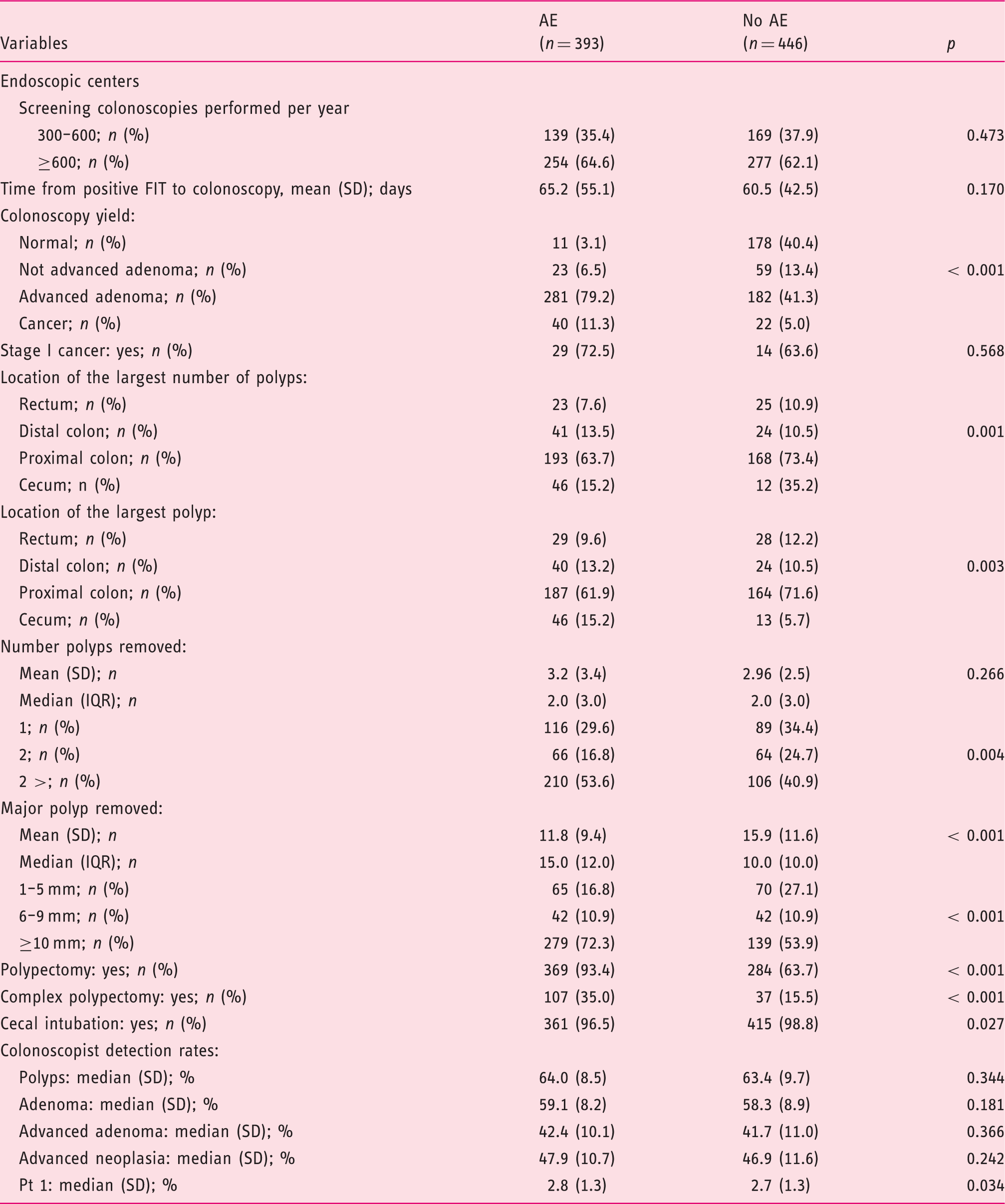
FIT: fecal immunochemical test; IQR: interquartile range.
Univariate analysis of risk factors of colonoscopy complication.
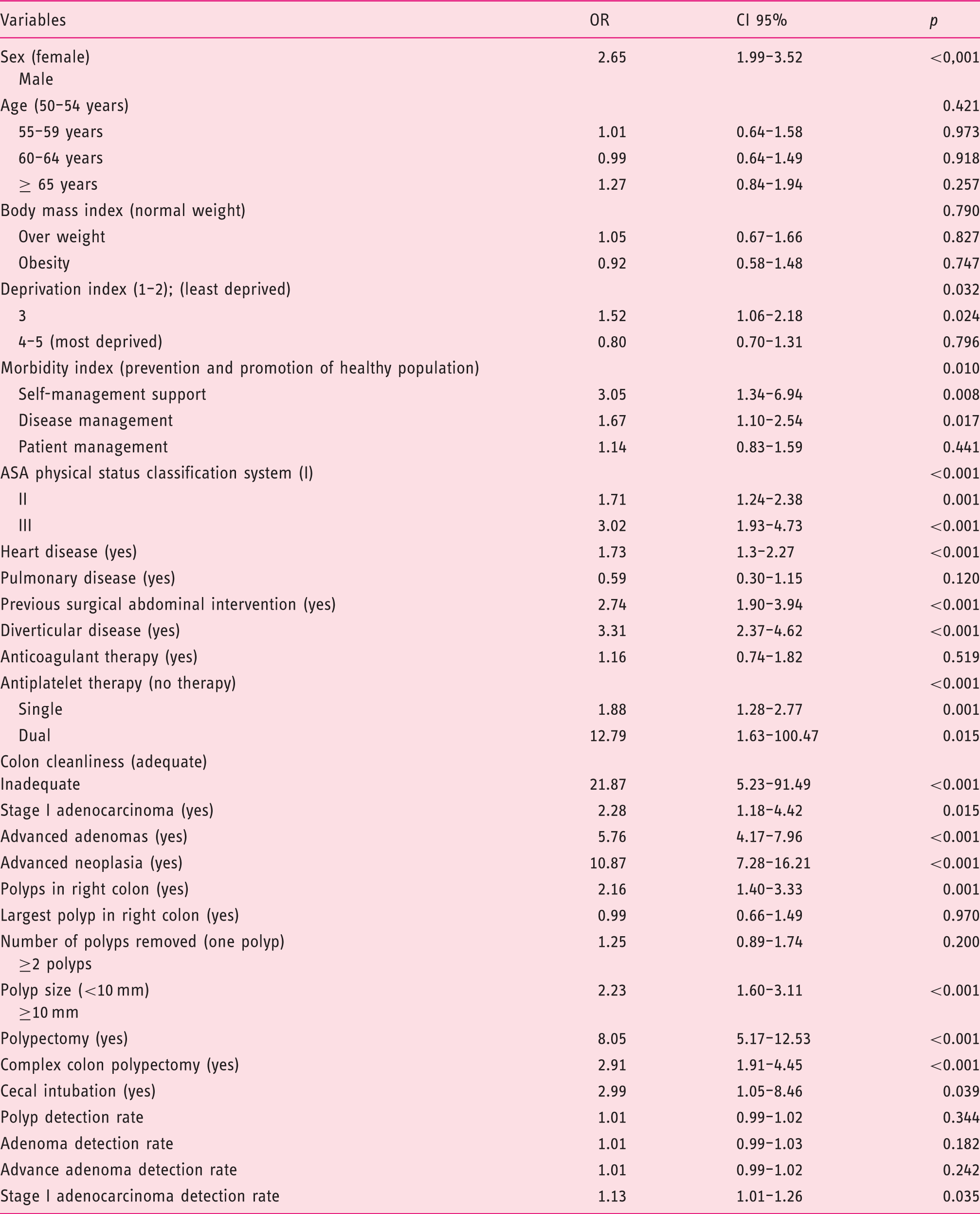
ASA: American Society of Anesthesiologists; OR: odds ratio; CI: confidence interval.
Multivariate analysis of risk factors of colonoscopy complication.
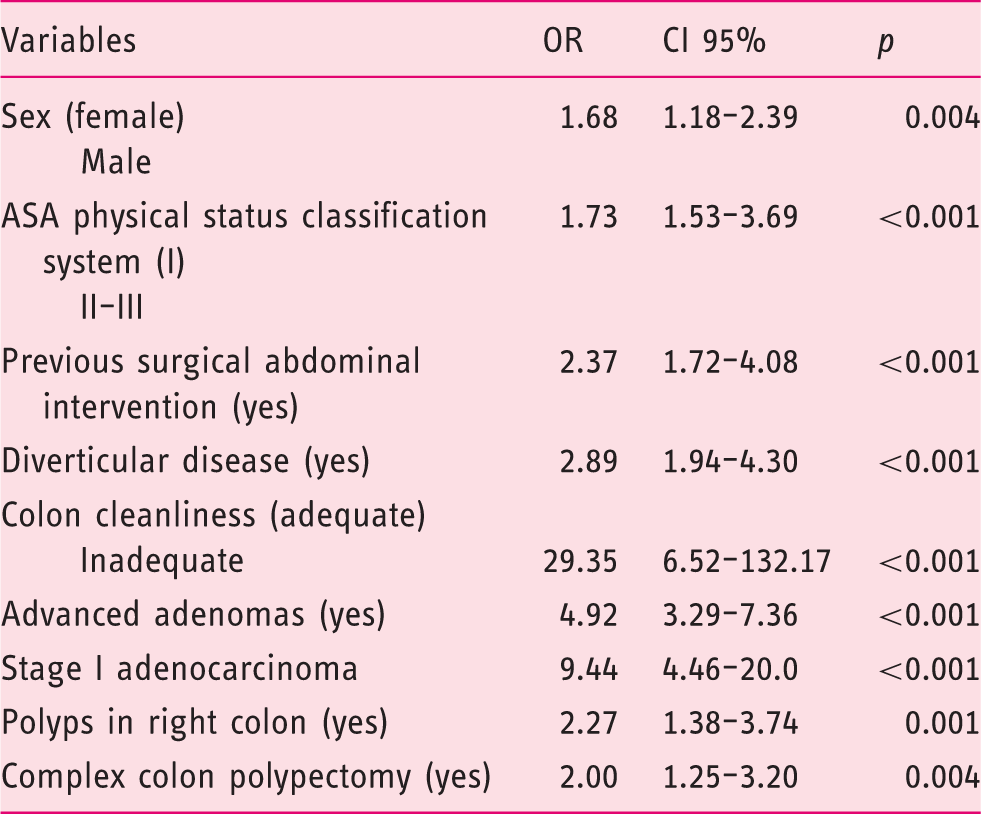
ASA: American Society of Anesthesiologists; OR: odds ratio; CI: confidence interval.
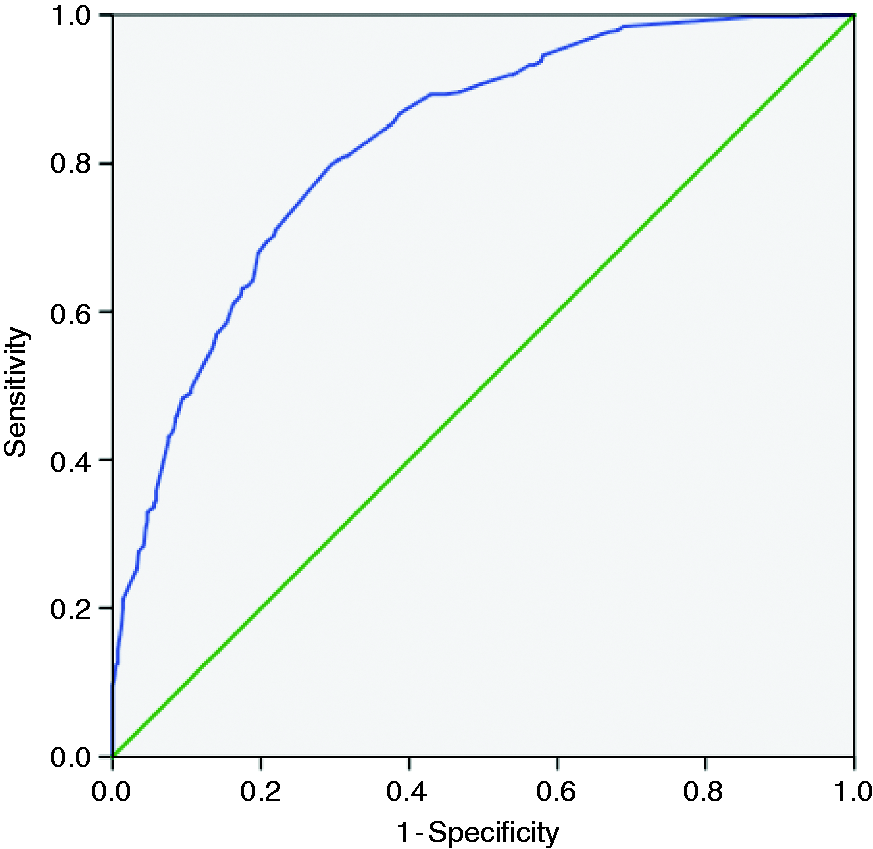
Receiver operating characteristic curve for the logistic model.
Admitted patients had a median hospital stay of 5.0 days (IQR = 3–7 days). In post-colonoscopy bleedings in 47.6% a therapeutic colonoscopy was performed and in 1.2% surgery. Of the bleedings, 21.1% required transfusion. A total of 59.1% of post-colonoscopy perforations were managed with conservative treatment. No deaths were reported.
Discussion
Screening colonoscopy with polypectomy has been shown to be a diagnostic and therapeutic procedure capable of reducing the incidence and mortality of CRC.2–8 However, although endoscopic techniques have greatly improved, they are not exempt from damage, and different publications show diverse complication rates, ranging from 0.04% to 8%.14–21 In our study we have observed that our outcomes are close to the highest rates published to date. Nevertheless, it should be emphasized that most of the published studies are retrospective, which underestimates the complication rates 17 because of the lack of records with proven quality, which could influence the completeness of the data. In the BCCSP, all colonoscopy data are collected prospectively and routinely within 10 days of their completion. In addition, all hospital discharges are linked with the program database, ensuring record quality as recommended by the European CRC guidelines. 8 The effectiveness of the screening colonoscopy depends not only on its compliance, which in our program is above the desirable level (>90%) recommended by the European guide, 8 reaching 92.7%, but also in the quality of its performance and record keeping. It is therefore of paramount importance this registry, as well as the quality of the data collected within it, be able to carry out analysis and identify independent factors related to complications, to be able to implement measures that improve the efficiency of the program.
One risk factor described extensively in the literature is the location of polyps, demonstrating how polypectomy in the proximal colon is an independent risk factor.14–21,24,25 The Munich Polypectomy Study (MUPS) study reported that proximal location of polyps had a substantial risk of major complications (odds ratio (OR) 2.40, CI 95% 1.34–4.28). 16 After performing the multivariate analysis, we estimated an OR of 2.27 (CI 95% 1.38–3.74) for severe complication after polypectomy in the proximal colon. However, other authors such as Rutter et al. 24 were able to analyze the risk that each segment of the colon had, estimating an OR of 13.5 (CI 95% 3.9–46.4) for bleeding requiring transfusion after cecal snare polypectomy and an OR of 12.2 (CI 95% 1.2–119.5) for perforation after cecal non-pedunculated polypectomy. In the referred study, 7.7% of the procedures were performed in the cecum, and in our study these were 15.2% of the total polypectomies (almost double), so we could assume a higher risk for major complications while performing polypectomies in the cecal location (univariate analysis, OR 2.98, CI 95% 1.57–5.67). A reasonable explanation for this may be the biological structure of the cecum; this is the finest and distensible part of the colon with saccular pouches between the linear tenia coli. Insufflation during colonoscopy to distend the wall leaves the cecum more susceptible to damage.14,24
The risk of severe complications also increases with polyp size. Our study showed that a complex colon polypectomy had an estimated OR of 2.00 (CI 95% 1.25–3.20) for the risk of severe complication. In the definition of complex colon polypectomy, one of the main characteristics is to have a polyp bigger than 20 mm. Our study supports several studies that had estimated the polyp size in relation to severe complications.14–21,24–26 In the MUPS study 16 the main risk factor for major adverse events reported was polyp size, with an OR of 31.01 (CI 95% 7.53–128.1). Buddingh et al. 13 reported that the risk increased by 13% (CI 95% 5–20) per millimeter, similar to the 9% per millimeter found by Sawhney et al. 27 In this context, Dobrowolski et al. 28 reported that polyp size greater than 17 mm, pedunculated polyps with a stalk diameter >5 mm, sessile polyps, and malignant lesions of the colorectal region are at high risk of hemorrhage after endoscopic excision. Gimeno-García et al. 17 also stablished a cutoff point of 14 mm polyp size as the most important predictor of post-polypectomy bleeding. Using this cutoff would have allowed a prediction of 70% of post-polypectomy bleeding episodes.
We have also identified as independent risk factors the malignancy of the lesions detected. The detection of an AA had an OR of 4.92 (CI 95% 3.29–7.36) and the detection of stage I adenocarcinoma 9.44 (CI 95% 4.46–20.0). Related to histology and malignancy, Consolo et al. 29 reported that post-polypectomy bleeding was associated with large polyps, malignancy, heart disease and hyperplastic polyps.
Male sex has a 1.68 (CI 95% 1.18–2.39) higher risk of an adverse event. This result is not in accordance with the OR of 2.85 (CI 95% 1.17–7.09) for female sex reported by Buddingh et al. 13 However, some studies report that complications are more common in men than women.17,21 In a univariate analysis, Heldwein et al. 16 reported the relation of ASA as an independent factor (OR 1.10, CI 95% 0.63–1.93), but not statistically significant. However, we have estimated an OR of 1.73 (CI 95% 1.53–3.69) for ASA ≥ II.
Related to the participant characteristics, we have identified two independent factors: on the one hand, previous surgical abdominal intervention (OR 2.37, CI 95% 1.72–4.08) and on the other diverticular disease (OR 2.89, CI 95% 1.94–4.30). We have also estimated an OR of 1.73 (CI 95%, 1.3–2.27) for history of heart disease. In this context we have not identified as risk factors hypertension as Watabe et al. 26 described, nor body mass index >25 kg/m2.
According to the ESGE guidelines 30 for the management of antiplatelet/anticoagulant therapy in patients undergoing a high-risk endoscopic procedure (polypectomy), all patients in the BCCSP followed the recommendations. In the univariate analysis, we did not identify anticoagulant therapy as a risk factor. In the case of antiplatelet therapy, we found a significant relation in single (OR 1.88, CI 95% 1.28–2.77) and dual treatment (OR 12.79, CI 95% 1.63–100.47) while comparing with no antiplatelet treatment. Also, Kim et al. 19 identified anticoagulant therapy as a risk factor (OR 3.71, CI 95% 1.05–13.05) and Heldwein et al. 16 nonsteroidal anti-inflammatory drug intake (OR 4.00, CI95% 0.55–29.41), but these were not statistically significant.
Cecal intubation rates and bowel cleansing scores are very important quality indicators in colorectal screening programs, as reported in several studies.31–34 In fact, the quality of bowel preparation is important for the efficacy of colonoscopy. As pointed out in the ESGE guidelines, 23 the quality of bowel preparation is associated with two other important performance measures, adenoma detection rate and cecal intubation rate. Suboptimal bowel preparation results in further costs and inconvenience, because the examination has to be repeated or an alternative examination has to be arranged. 35 In the BCCSP the cecal intubation rate was 97.7%, higher than the desirable level in the European guidelines, 8 and the rate of adequate bowel preparation 95.1% (target standard rate for an adequate bowel preparation is 95% by ESGE). 34 In the univariate analysis, we identified lack of cecal intubation as a risk factor (OR 2.99, CI 95% 1.05–8.46) and in the multivariate analysis, inadequate bowel cleansing had almost 30 times more risk of severe complications than adequate cleansing (OR 29.35, CI 95% 6.52–132.17).
Bearing in mind the results of this and other studies, it would be interesting to carry out future studies in which, based on the risk of suffering a complication, different strategies are implemented and analyzed when considering which individuals should undergo a colonoscopy. Today there are less-invasive tests such as the endoscopic capsule or computed tomography colonography. These tests could be considered in those individuals with a higher risk of complication.
Finally, our study has some limitations. One of the most important limitations is that this is a retrospective study nested to a cohort prospective study. However, it should be noted that the quality and completeness of the screening electronic records in the BCCSP is very high. It has already been indicated that colonoscopies, once performed, are recorded prospectively, collecting all the data from endoscopies’ reports, as well as reports of pathological anatomy, with all data regarding the polyps and lesions identified.
It should be noted as one of the main strengths of the study that we present is that it is one of the few published studies, as far as we know, that tries to identify risk factors related to the performance of a colonoscopy in a population screening program with FIT. Furthermore, the study has been carried out in the context of real-world practice. This increases the interest for the figures provided and the importance of the countermeasures, in order to improve the quality and minimization of the risks of the program itself.
CRC population-based screening program analyses have been centered on the assessment of major outcomes and costs of required colonoscopies without paying much attention to the risks associated with the procedures themselves and related costs. This study reflects the risk associated with colonoscopies within the framework of a well-established program with a high participation rate and real-world conditions. The outcomes observed provide insight as to how to minimize the adverse event rates of colonoscopies and how to increase the efficiency of existing programs while ensuring that the goals of morbi-mortality are reached.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This study was approved by the Basque Country’s Ethics Committee (no. PI2014171; November 4, 2014). The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a prior approval by the institutions' human research committee.
Informed consent
All participants provided written informed consent.