
Abstract
Background
Symptomatic invitees are advised not to participate in colorectal cancer (CRC) screening but to directly consult their general practitioner (GP), because fecal immunochemical test (FIT) sensitivity for cancer is not optimal. This recommendation may not always be followed in daily practice. We evaluated how many FIT-positive participants had CRC-related symptoms and whether the presence of symptoms was associated with the presence and location of CRC/advanced neoplasia.
Methods
We prospectively collected data on CRC-related symptoms in all FIT-positive participants in the Dutch CRC screening program, referred to our endoscopy centers between 2014 and 2016, and evaluated whether symptoms were associated with detected CRC/advanced neoplasia at colonoscopy.
Results
Of 527 FIT-positive participants, 314 had advanced neoplasia, of which 41 had CRC. Overall, 246 (47%; 95% confidence interval (CI) 0.42–0.51) reported CRC-related symptoms. A change in bowel habits (odds ratio (OR) 2.86, CI 1.23–6.62) and visible blood in stool (OR 8.65, CI 2.34–32.0) were associated with the detection of CRC at colonoscopy. We did not observe significant associations between evaluated symptoms and advanced neoplasia.
Conclusions
A large proportion of FIT-positive screening participants have CRC-related symptoms. This suggests that current instructions do not retain symptomatic screening invitees from participation and awareness of CRC-related symptoms is inadequate.
Introduction
Screening an average risk population for colorectal cancer (CRC) using fecal occult blood tests (FOBTs) has been shown to reduce CRC-related mortality through the detection of CRC in an earlier stage and the removal of precancerous lesions.1,2 Even though the fecal immunochemical test (FIT) is more sensitive than the guaiac FOBT, detection of advanced neoplasia (AN) is not perfect.3,4 A total of one out of four patients with CRC and two out of three with advanced adenomas (AA) are still missed in one single round of FIT. 5 , 6 It has also been suggested that FIT may be less sensitive in detecting proximally located AN as compared with distally located advanced lesions.7–9
People at high risk of CRC, such as those with CRC-related symptoms, are usually advised not to participate in screening. Instead, they are encouraged to directly consult their general practitioner (GP) because the relatively low sensitivity of FIT may lead to false negative results or a diagnostic delay. Clinical symptoms potentially indicative for the presence of CRC are visible blood in the stool, a change in bowel habits, unintentional weight loss and abdominal pain, although these symptoms are not very specific.10–17 Tenesmus is not included in international CRC referral guidelines but has been associated with the detection of CRC, individually or in combination with other obstructive symptoms.11,18 Some of these symptoms seem to be associated with tumor location. Visible rectal blood loss, tenesmus and a change in bowel habits, for example, are considered more common for distal than proximal CRC.11,19,20
Leaflets are a key way for the organizers of screening programs to communicate with the target population. The information leaflet of the Dutch screening program explicitly advises screening invitees not to participate in screening but to see their GP for a consultation instead if they experience a change in bowel habits and/or visible blood in their stool. In case of doubt, invitees should also consult their GP and not participate in screening. Although there is evidence that leaflets can increase knowledge about CRC screening, 21 we do not know whether these recommendations are always followed.
We studied the percentage of FIT-positive screening participants undergoing colonoscopy that reported CRC-related symptoms, and evaluated whether these symptoms are related with the detection and, if so, location, of CRC or AN at colonoscopy.
Methods
Study population and design
We collected data in all FIT-positive participants in the Dutch CRC screening program, referred to two certified colonoscopy centers (Bergman Clinics, Amsterdam and Bilthoven, The Netherlands) between January 2014 and March 2016. Exclusion criteria for the Dutch CRC screening program were: participants undergoing current treatment for CRC, with a history of inflammatory bowel disease or proctocolectomy, and with a life-expectancy of less than 5 years, as well as those who opted for active deregistration from screening. Organizational details of the Dutch CRC screening program can be found elsewhere. 22 In short, all people 55–75 years old are invited biennially to perform a FIT at home (FOB-Gold, Sentinel, Italy) and to send it by postal mail to one of the certified laboratories. All participants with a positive FIT (January to June 2014: ≥15 µg of hemoglobin/g of feces; from July 2014: ≥47 µg of hemoglobin/g of feces) were invited for an interview before planning a colonoscopy.
Data collection and quality assurance
Prior to the pre-colonoscopy interview, participants in this study were asked to fill in a validated consultation form including the question whether they experienced one or more of the coded CRC-related symptoms. Symptom definitions are specified in the following paragraph and a copy of the consultation form is provided in Appendix 1. During the pre-colonoscopy interview, trained nurses verified the answers with participants, and helped with language or literacy-related difficulties if needed. Data on symptoms and participant characteristics (age, sex, postal code and familial risk for CRC) were systematically collected in the electronic patient records (Chipsoft, ChipSoft BV, The Netherlands).
If a FIT-positive screening participant was eligible, based on the inclusion and exclusion criteria previously described, a colonoscopy was performed within 2 weeks after the interview by an accredited screening endoscopist in one of the certified colonoscopy centers. For all colorectal lesions, the endoscopic location, size and morphology were reported using the automated, structured colonoscopy reporting system EndoALPHA (Endobase Olympus, Winter & Ibe GmbH, Hamburg, Germany). Participants that did not undergo a colonoscopy after pre-colonoscopy interview were excluded for analysis.
All lesions were collected in separate jars, enabling per polyp histopathological assessment. Colonoscopy quality was assessed using the European Society of Gastrointestinal Endoscopy quality indicators: cecal intubation (confirmed by images of the ileocecal landmarks and/or insertion into the terminal ileum); bowel cleansing of at least 6 on the Boston Bowel Preparation Scale (BBPS); and net withdrawal time of at least 6 minutes. 23 If quality indicators were not met, the reason for incompleteness was reported and participants were excluded for analysis. Participants with an incomplete colonoscopy due to a stenosing tumor were not excluded because we considered CRC as the most advanced possible lesion for detection. Neither excluded were participants with incomplete colonoscopies in which visualization of the colon was completed by computed tomography (CT) colonography.
Outcome measures and definitions
Participant characteristics
Socioeconomic status was assessed on the area social status score, developed by the Netherlands Institute of Social Research. 24 This score combines the socioeconomic indicators unemployment rate, education level, average income, and position on the labor market. Socioeconomic status was grouped in quintiles, with 1 being the highest status and 5 being the lowest. Familial risk for CRC was defined according to the Dutch guideline on hereditary and familial CRC: having a first-degree relative with CRC younger than 50 years, or at least three first- or second-degree relatives with CRC <70 years, or two first-degree relatives with CRC aged 50–70 years, or one first-degree relative aged 50–70 years and one second-degree relative with CRC aged <70 years. 25
Symptoms
We studied the following self-reported CRC-related symptoms: visible rectal blood loss (in the last 3 months), a change in bowel habits (loose stools or constipation in the last 3 months), unintentional weight loss (during the last months in kg/month), tenesmus (on a regular basis) and abdominal pain (or cramps). The first two are explicitly mentioned in the Dutch screening information leaflet as the most frequent CRC-related symptoms.
Colorectal lesions
CRC diagnosis was confirmed by pathology. AN was defined as either CRC or AA. AA were adenoma of at least 10 mm in size, with a ≥25% villous component and/or with high-grade dysplasia.26,27 Polyp size was based on the endoscopic estimate in mm. Polyp histology was categorized as tubular, tubulo-villous (25–75% villous component) or villous (≥75% villous component).26–28 Grades of dysplasia were no dysplasia, low-grade dysplasia and high-grade dysplasia, based on the pathology report.
Location colorectal lesions
Lesions were located per colonic segment, but for analysis colonic locations were grouped into proximal (cecum to splenic flexure) or distal (descending colon to rectum).
Analysis
Participants were grouped per presenting symptom and also characterized as symptomatic (≥1 symptom) or not. As participants could experience more than one symptom, symptom subgroups may overlap. We calculated odds ratios (ORs) and corresponding 95% confidence intervals (CIs) to express the strength of the association between symptoms and CRC and AN. CIs of proportions were calculated using Wilson’s method. 29 To evaluate the association between symptoms and tumor location, while correcting for the number of tumors per location, we compared the proportions of participants with and without symptoms per tumor location. A p-value less than 5% was considered to indicate statistically significant differences or associations. SPSS version 23 was used for statistical analysis (SPSS Statistics for Windows, Armonk, NY, USA: IBM Corp).
Results
Participants
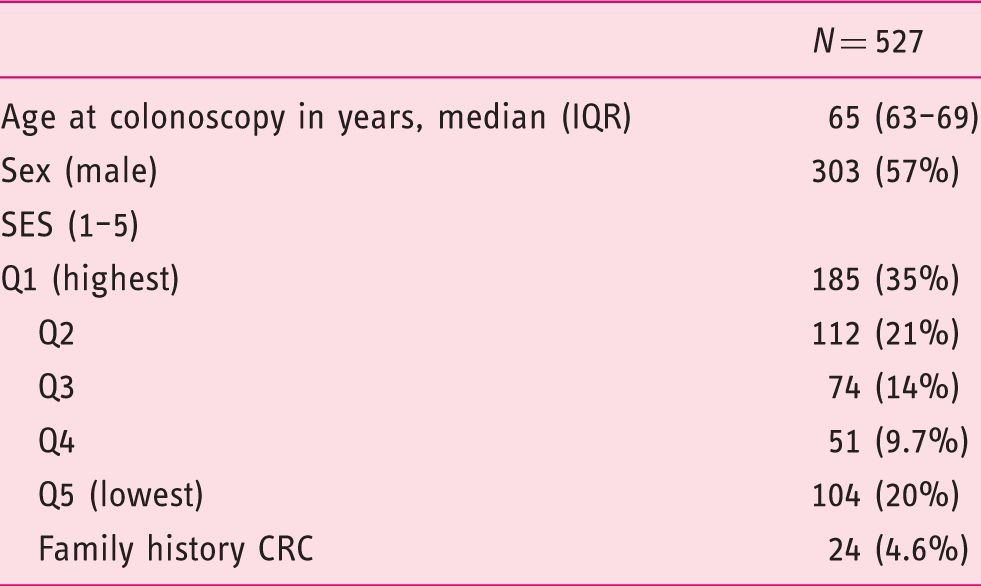
Of 598 FIT-positive screening participants, 71 had to be excluded for analysis (Figure 1). A total of 62 participants did not undergo a colonoscopy after the pre-colonoscopy interview, due to their medical condition or because they decided not to participate. Overall nine participants did not meet the endoscopy quality indicators (BBPS < 6, withdrawal time < 6 min, or no achieved cecal intubation other than due to a stenosing tumor). A total of 11 participants had an incomplete colonoscopy due to a stenosing tumor and in 2 participants visualization of the colon was completed with CT-colonography; these were not excluded. Basic characteristics of the 527 participants available for our analysis are shown in Table 1. The median age was 65 years, 57% were male. A total of 24 (4.6%) reported having a familial risk for CRC.
Included participants. Participants characteristics. CRC: colorectal cancer; IQR: interquartile range; SES: socioeconomic status index in quintiles, defined by area level (postal code).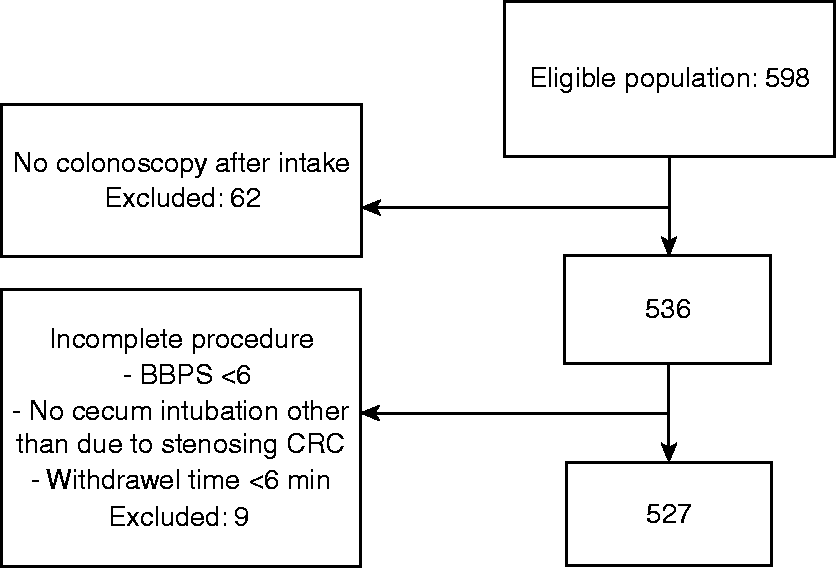
Colonoscopy findings
Colonoscopy findings (by sex).
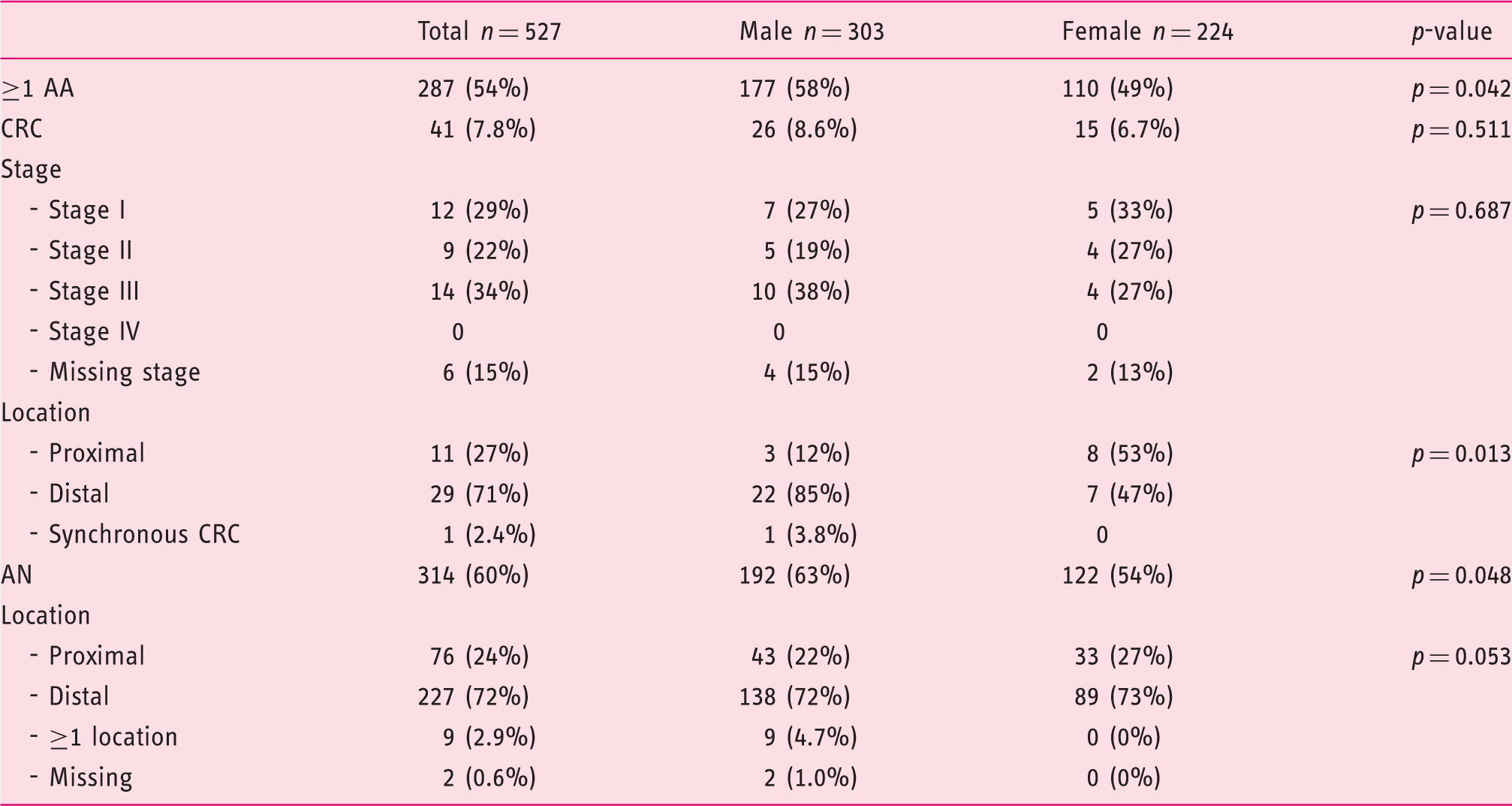
AA: advanced adenoma; AN: advanced neoplasia: CRC and/or AA; CRC: colorectal cancer.
CRC was more often located in the distal colon (n = 29, 71%) than in the proximal colon (n = 11, 27%) but this differed by sex. In males 85% of CRC tumors were located distally and only 12% proximally; in females, most tumors were detected in the proximal colon (53%). Overall one participant had synchronous CRCs in both the distal and proximal colon. AN had a similar localization pattern without sex-differences.
Symptoms and advanced neoplasia
In total, 246 of the 527 participants (47%) reported having one or more of the evaluated CRC-related symptoms. Within this symptomatic group, 21 (8.5%) had CRC and 142 (58%) had AN. In asymptomatic participants (n = 281) CRC was detected in 20 (7.1%) and AN in 172 (61%). A total of 33% of participants had one of the symptoms that were explicitly mentioned in the Dutch screening information leaflet (visible rectal blood loss or change in bowel habits).
Symptoms in FIT-positive participants and CRC/AN detection.
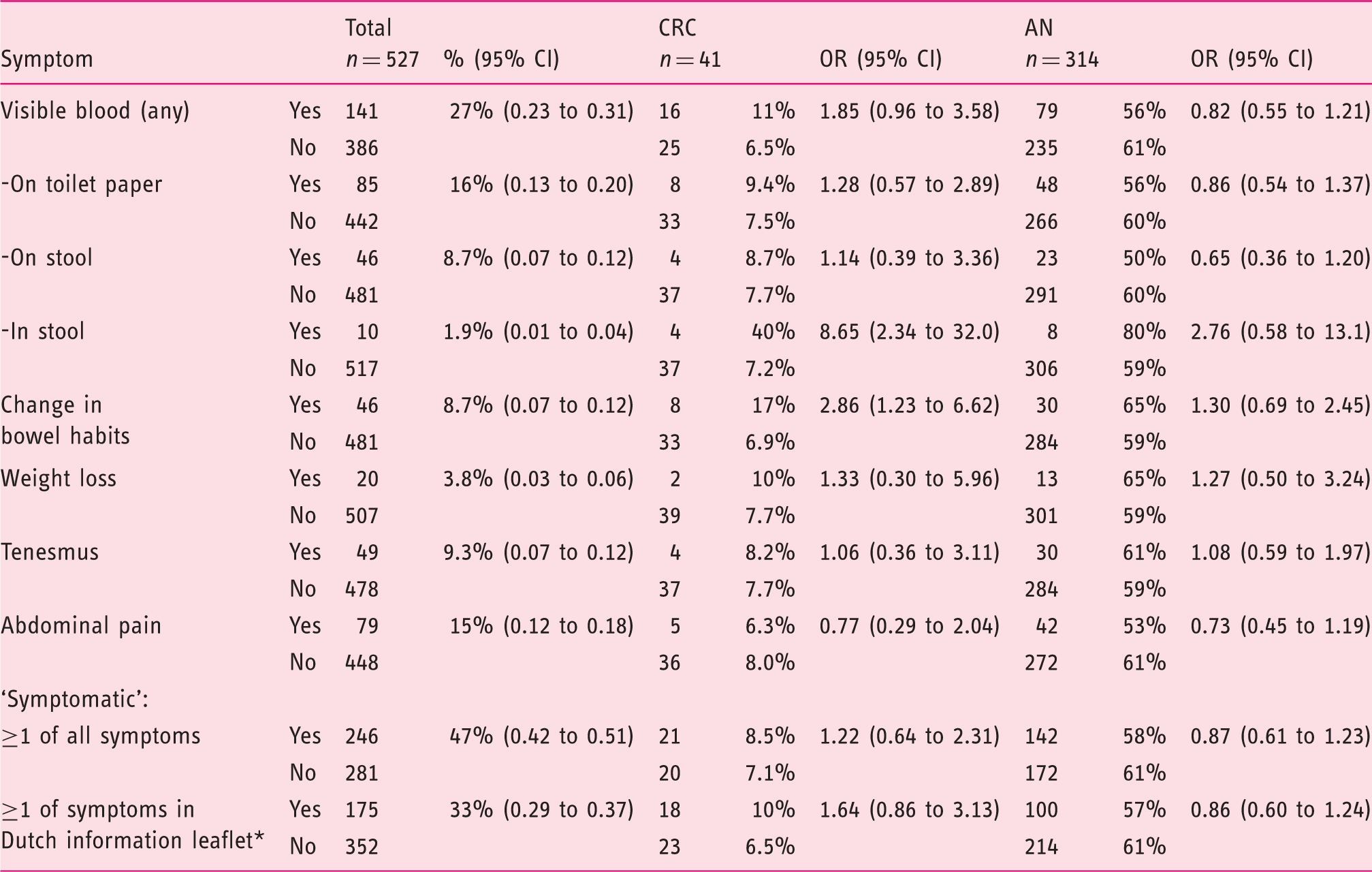
Bowel habits change and visible rectal blood loss are described as reasons to consult the GP and not participate in population-screening in the Dutch CRC screening information leaflet.
AN: advanced neoplasia; CI: confidence interval; CRC: colorectal cancer; FIT: fecal immunochemical test; GP: general practitioner; OR: odds ratio.
In contrast, not all estimated ORs between the CRC-related symptoms and the detection of AN exceeded unity (Table 3), and none of these associations reached statistical significance.
Symptoms and CRC location
Symptoms in FIT-positive participants and CRC location.

CRC: colorectal cancer; FIT: fecal immunochemical test.
Excluded for analysis: one participant with synchronous proximal and distal CRC.
Discussion
Although symptomatic invitees are advised not to participate in screening and to directly consult their GP instead, we observed a disturbingly large proportion of FIT-positive participants having CRC-related symptoms. Of these symptoms, having a change in bowel habits and visible blood in the stool were significantly associated with the detection of CRC at colonoscopy. None were associated with the detection of AN.
This study used prospectively and systematically collected data on symptoms and colonoscopy findings, relying on complete and high-quality data. Since symptoms were recorded before the colonoscopy results were disclosed, and symptoms were not communicated to the endoscopist, blinding was guaranteed, and recall bias was minimized for our evaluation of the associations between symptoms and findings.
Some limitations have to be acknowledged. First, we relied on self-reporting of symptoms. Since these were all FIT-positive participants, symptoms are associated with the detection of CRC, and participants knew they had a FIT-positive test at time of symptom reporting, some form of recall bias cannot be ruled out. Therefore, the proportions of participants with symptoms cannot be taken as an estimate that can be generalized to all screening invitees or all screening participants. Second, we studied five symptoms only, including the two that are mentioned in the Dutch screening information leaflet. We are aware that other findings, such as anemia, might also be related to CRC. The exclusion of this and other possible symptoms does however not affect the proportions reported here. Last, though our study group was an unselected sample from the Dutch screening population, the proportion of symptomatic patients may differ across screening programs. Yet we have reasons to believe that most FOBT-based screening programs include participants with CRC-related symptoms.
The two previous studies similarly assessed symptoms in a FOBT-positive screening population and observed even higher proportions of symptomatic participants. Saldanha et al. reported that 52% of Scottish FOBT-positive screening participants had CRC-related symptoms. 30 Ahmed et al. described 78% symptomatic FOBT-positive Scottish screening participants. 31 In contrast with our study setting, the Scottish information leaflet did not explicitly recommend symptomatic invitees to decline screening but instead directly consult their GP, possibly explaining the higher proportion of symptomatic participants.
The proportion of symptomatic participants is influenced by the definition of ‘symptomatic’, in other words: the included symptoms. Abdominal pain for example, is one of the most common complaints in the general population and might lead to an overestimation of the total number of symptomatic participants. 32 Also, tenesmus itself is not explicitly mentioned as CRC referral criterion in the NICE guideline and its status of CRC alarm symptom is debatable. 17 To assess to what extent these symptoms influences the symptomatic participant prevalence rate, we recalculated the symptomatic proportion in our study population if abdominal pain had been excluded and found a symptomatic proportion of 39%.
It is not yet clear why symptomatic invitees participate in screening, rather than seeking help from their GP. In our study population, one out of three reported at least one of the two symptoms that are explicitly mentioned in the screening information leaflet as reason to not participate in the population-based program. Kobayashi et al. interviewed 1307 English CRC screening invitees and concluded that 22% had not read any of the information provided and that only 52% had read all. 33 Among the participants in screening, 4% had not read any information. De Wijkerslooth et al. reported an effect of the information material on invitees behavior; 1% of 973 intending non-participants in a Dutch colonoscopy/CT-colonography screening trial declined participation because they had seen blood in stool and 1–3% because they experienced a change in bowel habits. 34 Unfortunately also a large proportion of invitees who declined screening reported an absence of symptoms as the main reason for non-participation (23–32%), which also suggests that the information material and general CRC knowledge is not optimal.
We found a significantly higher risk of CRC detection in FIT-positive participants who report visible blood in the stool or a change in bowel habits. These FIT-positive participants did benefit from screening because they were invited for colonoscopy, unlike the FIT-negative participants. We are however not informed about the prevalence of CRC-related symptoms among FIT-negative participants.
The consequences of low CRC awareness should invite new initiatives to facilitate the early detection of CRC and its precursors. Efforts to increase CRC awareness should not be limited to the eligible screening population. With mass campaigns or through individual consultation with health care professionals, people who have the key symptoms should be invited to go to their doctor without delay. Currently, such strategies are studied in England where a major public cancer awareness campaign called ‘Be clear on cancer’ started in 2010. Promising interim results in 2014 showed an increased awareness of key CRC-symptoms and another pilot on awareness on abdominal symptoms will start in 2017. 35 This is promising, and more is needed to specifically increase awareness of CRC-related symptoms in screening, to avoid diagnostic delays, aiming to eventually reduce CRC morbidity and mortality.
Conclusion
The two studies, performed within the organized Scottish guaiac-FOBT screening program, showed a proportion of 52% and 78% FIT-positive symptomatic participants. No association between symptoms and presence of CRC was found. This is the first study describing the proportion of screening participants with specific CRC-related symptoms within a FIT-based program that actively endeavors to prevent symptomatic invitees from participating in screening. We found a large proportion of 47% symptomatic FIT-positive screening participants and an association between visible rectal blood loss and a change in bowel habits with the presence of colorectal cancer.
Footnotes
Author contributions
Conception and design: CK, MV, ED; Literature search: CK; Data acquisition: CK, MV, ED; Data analysis and interpretation: all authors; Drafting the manuscript: CK, MV; Critical revision of the manuscript: all authors; Statistical analysis: CK, PB; Supervision: MV, PB, ED.
Funding
This research received no specific grant from any funding agency in the public, commercial, or non-profit sectors.
Declaration of conflicting interests
None of the authors (CK, MV, PB, ED) had any conflict of interest that could have influenced the research or results of this manuscript.
Ethics approval
Medical Ethics Review Committee of the Academic Medical Center confirmed that ethical approval is not required as this research does not involve human subjects.
Informed consent
The local medical ethics review committee confirmed that this study did not require individual informed consent, as participant data had been collected during standard care, no additional interventions were performed, and all data were analyzed anonymously (reference W16_103#16.121).