
Abstract
Background
Celiac disease is challenging to recognize, predisposing to long diagnostic delay. Currently, associated factors and significance of the delay remain obscure.
Objective
The objective of this article is to investigate associated sociodemographic risk factors and health consequences of diagnostic delay in celiac disease.
Methods
Altogether 611 patients were surveyed at diagnosis and after one year on a gluten-free diet regarding sociodemographic variables, well-being and use of medicines and health care services. Quality of life was measured by a validated Psychological General Well-Being (PGWB) questionnaire. The results were compared between patients with and without delayed (≥3 years) diagnosis.
Results
A total of 332 (54%) individuals reported a delay of ≥3 years. Associated with the delay were being a student or homemaker, but not gender, marital or occupational status, site of diagnosis or place of residence. Patients with the delay also had decreased self-perceived health and poorer PGWB scores compared to those without delay; in anxiety and general health this was seen even on a gluten-free diet. Days of sickness and doctor visits as well as use of drugs for dyspepsia and antidepressants were increased in the delay group both before and after diagnosis.
Conclusion
A delay in celiac disease diagnosis predisposes to reduced well-being and incremental use of medicines and health care services, both before diagnosis and one year after diagnosis.
Key summary
Established knowledge on this subject:
Celiac disease is a very common but markedly unrecognized condition. Median diagnostic delay of the disease is as long as from three to 13 years. At present, factors underlying and consequences of the delay remain mostly obscure.
New findings of this study:
A diagnostic delay of only three years is associated to decreased quality of life and excess doctor visits, days of sickness and use of pharmaceutical agents before diagnosis. Many of the detriments associated with the delay may remain overrepresented even during the year after diagnosis. Being a student or homemaker is associated with reduced risk of delay, whereas no other associations with socioeconomic factors were found.
Introduction
Celiac disease is a gluten-induced immunological disorder with an estimated prevalence of as high as 1%–2% in Western countries. 1 The diverse clinical picture of the disease is a challenge to physicians, and at present approximately 75%–90% of affected individuals remain unrecognized.2,3 In clinical practice, a mean diagnostic delay of up to even 13 years has been reported.4–8 Long-term untreated celiac disease predisposes to severe complications such as osteoporosis, infertility and lymphoma,9–11 and there is also evidence to suggest that in undiagnosed but symptomatic patients incremental use of health care services and pharmaceutical agents is likely.4,8,12,13
Another concern possibly associated with a delay in diagnosis is poor quality of life, as many untreated celiac patients suffer reduced psychological well-being, which improves on a gluten-free diet.14–16 Currently it remains unclear what factors are associated with the delay, and whether the delay affects patients’ self-perceived health. In addition, it is not known whether the delay predisposes to long-term increased consumption of medicines and consultations with physicians, which could be prevented by early diagnosis and dietary treatment of celiac disease.
In this prospective study, we investigated a number of patient-centered factors associated with diagnostic delay in celiac disease, and the effect of one year on a gluten-free diet on these. In particular, we aimed to evaluate the role of variable sociodemographic factors in the delay, and whether the delay is associated with individual health burden and increased use of health care services and pharmaceutical agents.
Methods
Participants and study design
The study was conducted in collaboration with the Finnish Celiac Society, which approximately 70% of new celiac disease patients in Finland join soon after diagnosis. 14 During a nationwide enrollment, a structured and validated questionnaire was sent to all new members joining the society in years 2007 and 2008. The patients were diagnosed at all health care levels from primary to tertiary care. Respondents older than 16 years of age with biopsy-proven celiac disease diagnosed within one year were considered eligible and continued in the study. Exclusion criteria were uncertain celiac disease diagnosis and lack of information on the duration of symptoms leading to the diagnosis. A follow-up questionnaire was sent to all participants after one year on a gluten-free diet. No ethical committee review was obtained because this was a questionnaire-based survey. However, informed consent was obtained from all participants after a written explanation of the aims of the study, including considerations regarding ethics and data protection and the anonymous deposition of the questionnaire.
Celiac disease diagnosis was considered delayed (“delay group”) if the disease-related symptoms had lasted at least three years before diagnosis, according to the previously shown median diagnostic delay in Finland. 8 Specific symptoms leading to celiac disease diagnosis have been defined elsewhere in detail. 14 Participants were further categorized on the basis of place of residence into individuals living in the South/West and those living in the North/East areas of the country, and also into those living either in urban or in rural areas. The South/West region of Finland has a markedly higher population density (41.7 inhabitants/km2) than the North/East (6.4 inhabitants/km2). 17 An urban area was defined as a population center with more than 15,000 inhabitants according to the Finnish Environmental Administration. 18
Questionnaires
The baseline and follow-up questionnaires were designed in cooperation with celiac disease patients and the Finnish Celiac Society. They comprised questions on a variety of sociodemographic aspects and the patients’ perceptions of the impact of the diagnosis on their overall health and well-being. Particular attention was paid to the duration of symptoms before diagnosis, occupational and working position, place of residence, site of first suspicion and diagnosis of celiac disease (primary, secondary or tertiary care), and self-rated health, concern for health, burden of symptoms and reaction to the celiac disease diagnosis both at the time of diagnosis and after one year on a gluten-free diet. Self-estimated health was rated on a four-point Likert scale as excellent, good, fair or poor; in analysis excellent and good were combined. Concern for personal health and burden of symptoms ranged from “not at all” to “extremely” on a three-point Likert scale. The participants also reported the number of all-cause visits to health care providers, consumption of pharmaceutical agents and days of absence from work during the year before diagnosis and in the first year on a gluten-free diet. Moreover, patients were asked about adherence to the gluten-free diet after one year on the diet.
Health-related quality of life
In addition to the above survey, self-estimated quality of life was measured by the structural Psychological General Well-Being Questionnaire (PGWB) both at diagnosis and after one year of a gluten-free diet. PGWB is a well-validated and widely used questionnaire in general and also in celiac disease research.15,16,19 It consists of 22 items, each using a six-grade Likert scale, with higher scores indicating better psychological well-being. The questionnaire is further subdivided into six subdimensions, each containing three to five separate items: anxiety, depression, well-being, self-control, general health and vitality. The total PGWB score is the sum of all 22 items and may thus range from 22 to 132 points.
Statistics
Association between diagnostic delay a and sociodemographic characteristics at diagnosis in 611 adults with celiac disease.
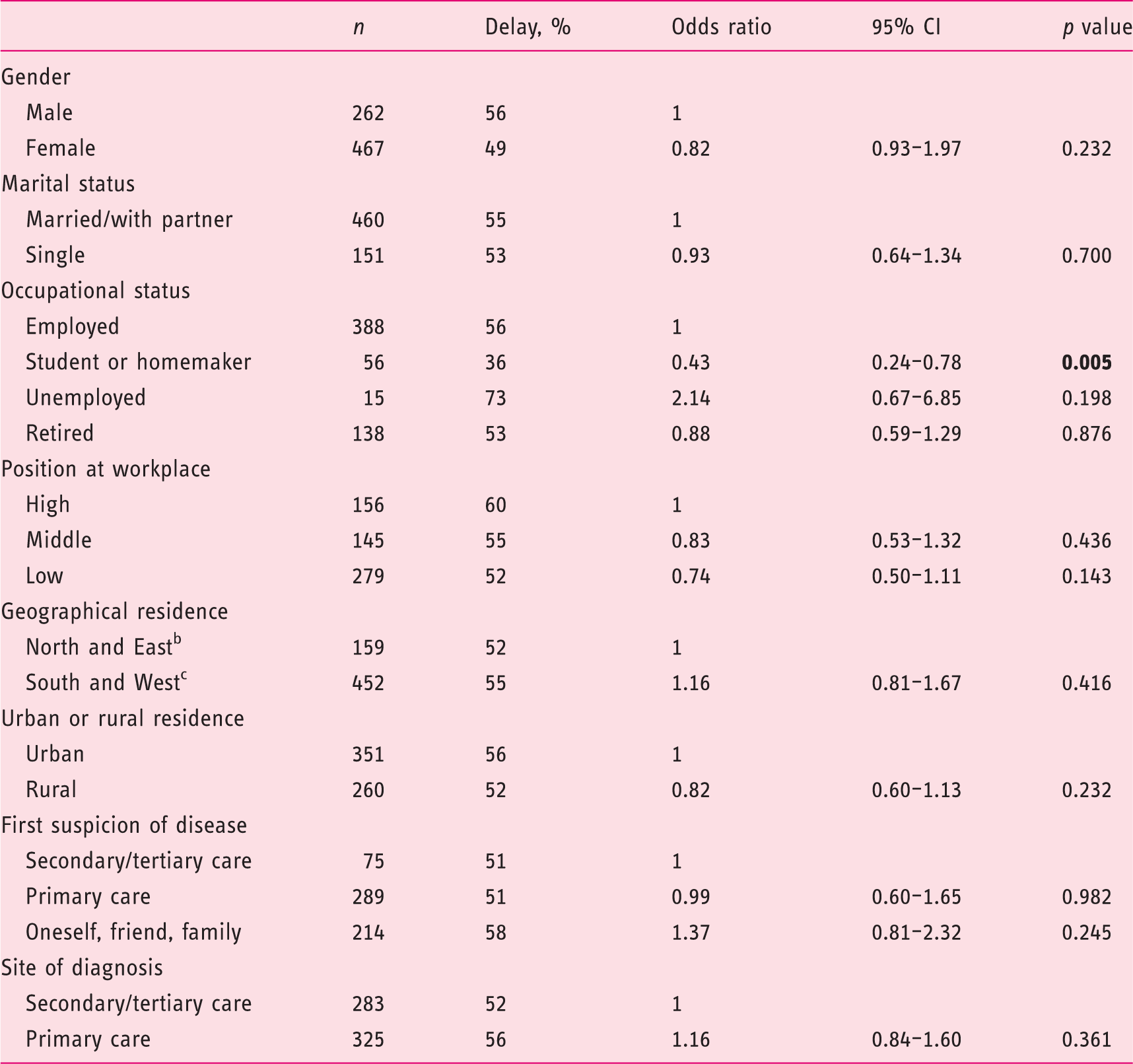
Celiac disease-related symptoms for three years or more before diagnosis. bPopulation density 6.4/km2. cPopulation density 41.7/km2.
CI: confidence interval.
Results
Altogether 1062 (57%) of the 1864 new members joining the Celiac Society during the study period responded. Of these, 451 were excluded: 157 as not being diagnosed within one year, 132 for being younger than 16 years of age, 89 for a lack of information regarding the duration of symptoms or otherwise substantially missing data and 73 owing to unclear celiac disease diagnosis. Of the 611 eligible individuals, 559 (91%) also completed the follow-up questionnaire. Seventy-six percent of the final study cohort were women.
The median duration of symptoms before celiac disease diagnosis was three (range 0–50) years and in 332 (54%) cases diagnosis was delayed by at least three years. Median age at diagnosis was 50 (16–75) years in patients with a delay and 48 (17–82) years in those without a delay (p = 0.363).
Associations between diagnostic delay a and self-rated perceptions of health at diagnosis and one year after diagnosis in 611 adults with celiac disease.
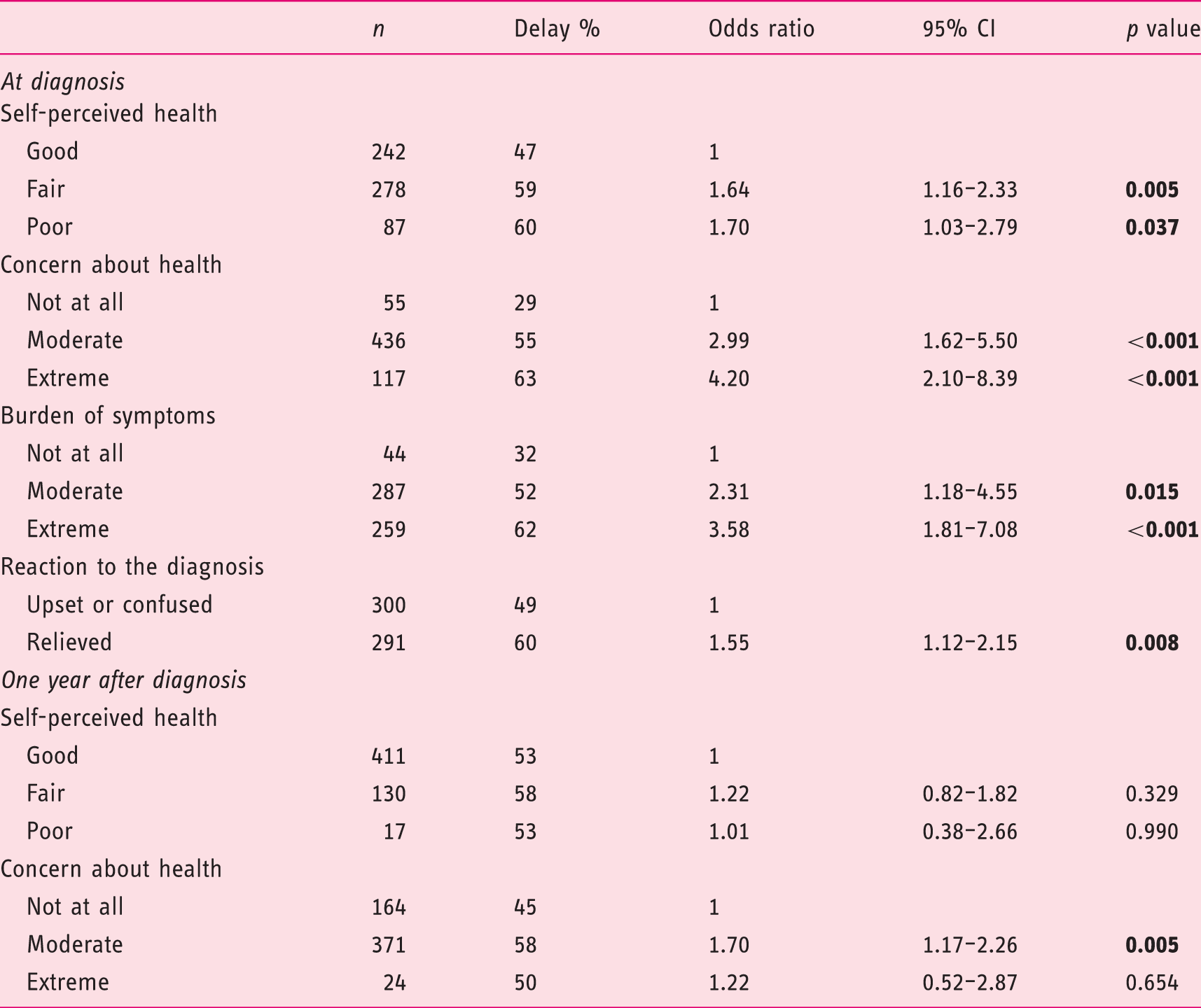
Celiac disease-related symptoms for three years or more before diagnosis.
CI: confidence interval.
All 559 individuals who returned the follow-up questionnaires were on a gluten-free diet, but 64 (11%) reported occasional lapses. On the diet the symptoms disappeared completely in 130 (23%), were alleviated in 337 (60%), remained unchanged in 71 (13%) and increased in three (0.5%) people. The likelihood of symptoms persisting on a gluten-free diet was increased in those with diagnostic delay (OR 1.61, 95% CI 1.08–2.42, p = 0.022).
Psychological General Well-Being scores of 592 celiac disease patients a at diagnosis and one year after diagnosis, categorized by length of diagnostic delay.
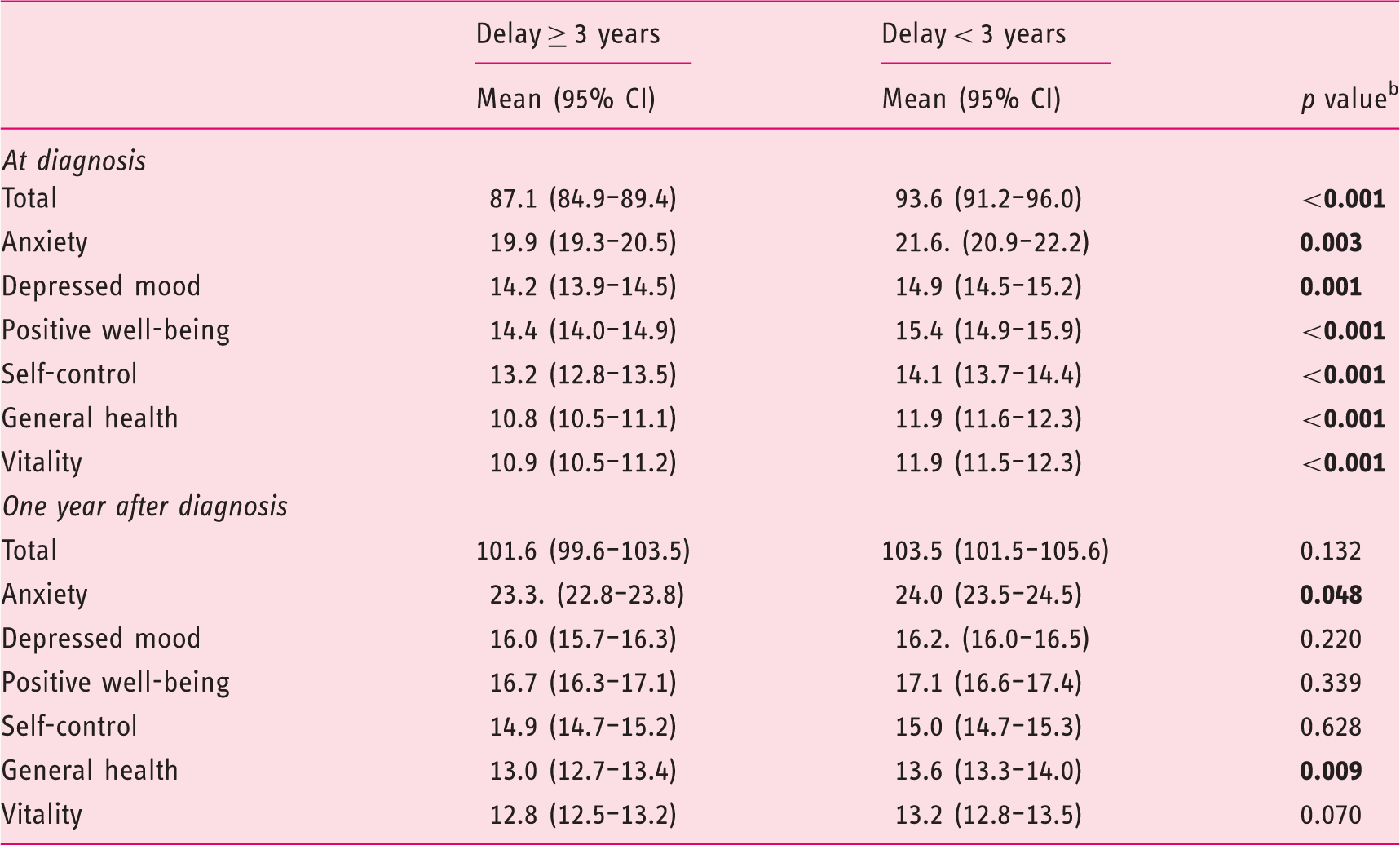
592 patients at diagnosis and 580 after one year. bIndependent-samples t test.
CI: confidence interval.
Use of health care services in the year prior to and following diagnosis in 611 celiac disease patients, categorized by length of diagnostic delay.
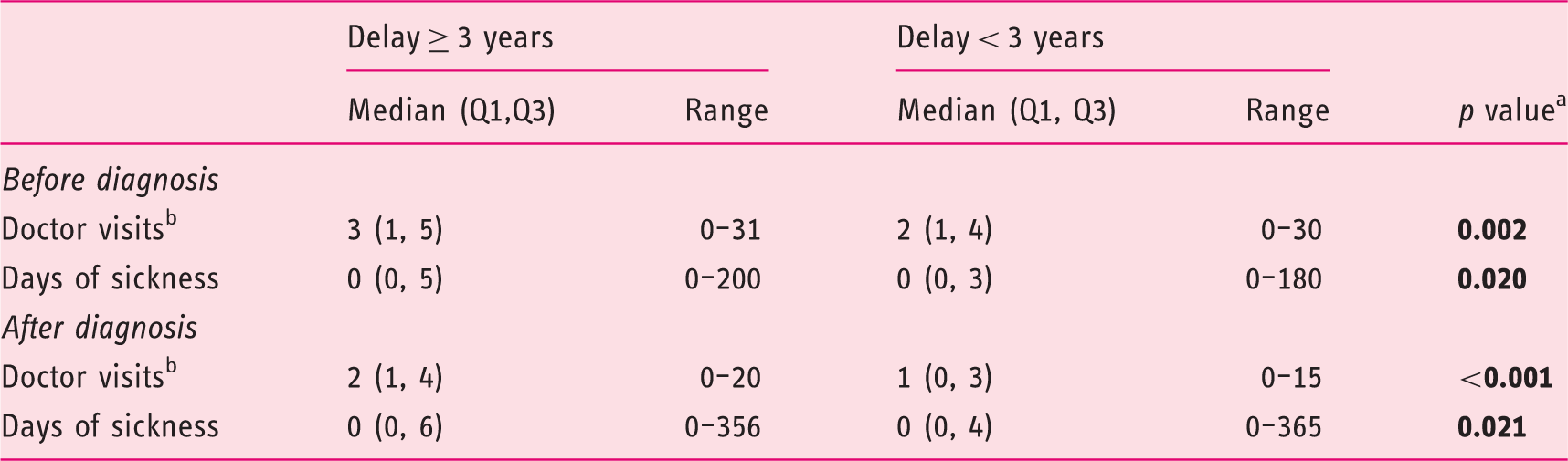
Mann-Whitney U test. bIn primary care.
Q1, Q3: lower and upper quartiles; CI: confidence interval.
The numbers of outpatient visits in primary health care and days of sickness during the year prior to celiac disease diagnosis were higher in individuals with diagnostic delay compared to those without (Table 4). The frequency of visits decreased in both groups during the year following diagnosis, but the difference remained significant. In contrast to outpatient visits, the number of days of sickness increased in both groups on a gluten-free diet (Table 4).
Proportion of patients using pharmaceutical agents in the year prior to and following diagnosis in 611 celiac disease patients, categorized by length of diagnostic delay.
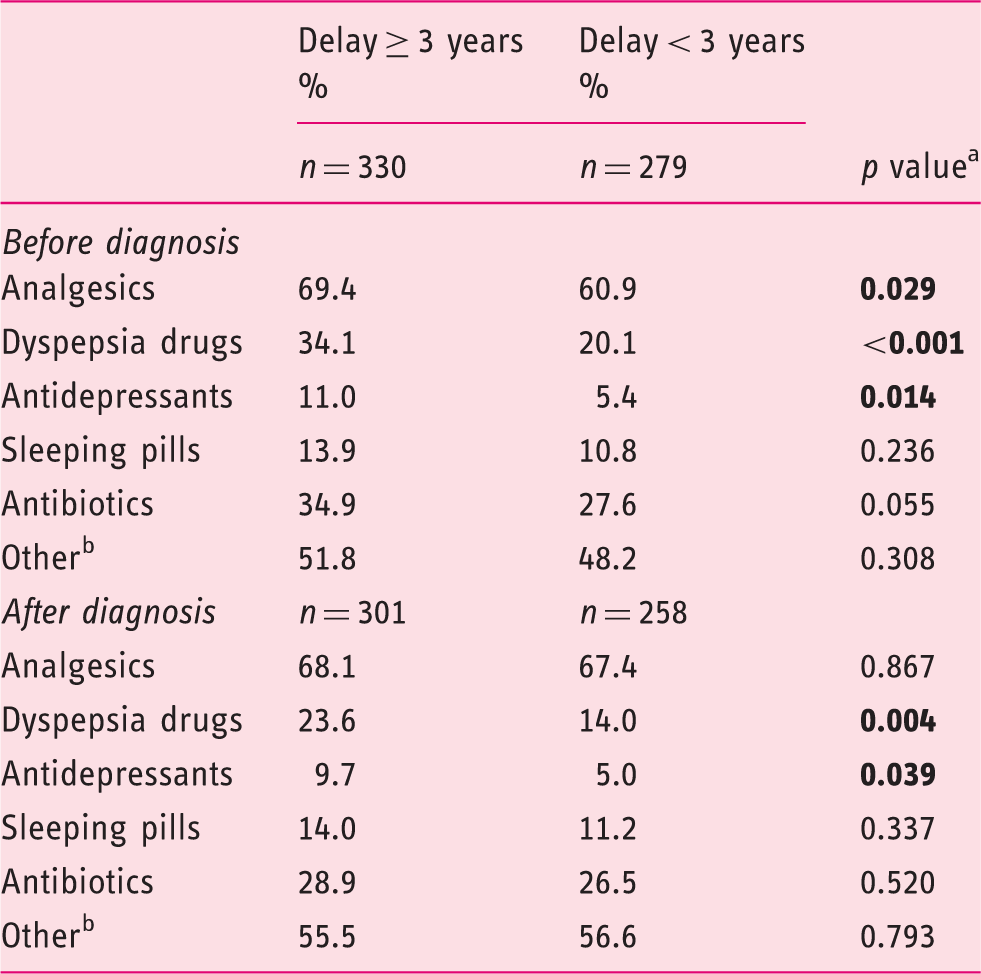
Chi-square test.
Vitamins, micronutrients, herbal products.
Discussion
Our main finding was that as little as three years’ diagnostic delay in celiac disease is associated with reduced health and well-being and increased use of health care and medicines. In fact, many of these detriments remained overrepresented in the delay group even during the year after diagnosis. Since in many countries the median delay is as high as 9–13 years,4–7 the morbidity observed here in patients with a substantially shorter period is alarming. Although part of these problems may eventually be alleviated on a gluten-free diet, it seems that a considerable number of celiac patients suffer from an excess health and economic burden avoidable by earlier diagnosis.
One of the key findings here was the reduced self-perceived health and psychological well-being in patients with a diagnostic delay. This is in accord with a previous Swedish study likewise showing poorer quality of life at diagnosis in those with a long delay. 7 Here, some of these important clinical outcomes remained poorer even after one year on a gluten-free diet, indicating that recovery from the psychological burden associated with long-term unrecognized celiac disease takes some time. Moreover, although the matter remains somewhat controversial,15,21 there is previous evidence that a subgroup of patients may continue to suffer from persistent poor health and mental problems even after years on a gluten-free diet.7,16 It is therefore essential that physicians and other health care professionals devote particular attention and support to those with a markedly delayed celiac disease diagnosis.
Somewhat surprisingly, we found no association between different socioeconomic factors and diagnostic delay except for a lower risk in students and homemakers compared to those who were employed. The lack of other associations might be related to the long-term political goal to reduce inequalities in health and health care in Finland. 22 Here, inexpensive and easily accessible public health care diagnoses and treats the great majority (in the present study 89%) of celiac disease patients. Because of the differences in health care systems, some caution is needed before extrapolating our findings to other countries. For example, more variability exists in terms of health care accessibility in the United States, where low income has been shown to be a major barrier to celiac disease diagnosis. 23 Significant regional and socioeconomic variation in the prevalence of celiac disease has also been observed in the United Kingdom, possibly reflecting disparities in health-seeking behavior and/or access to correct diagnostic pathways. 24 The somewhat counterintuitive lower risk of delay in students and homemakers noted here might be explained by the well-organized student health care and maternity clinics in Finland.25,26 Although there are no other similar studies, Vavricka and colleagues 27 have previously shown age younger than 30 years, the typical age for students and homemakers, to be associated with reduced risk of diagnostic delay.
Neither place of residence nor level of health care at which the celiac disease diagnosis was made was associated with the risk of diagnostic delay. This is compatible with our previous findings in patients with a delay of 10 years diagnosed mostly in the area of one tertiary center, 28 whereas the earlier mentioned British study reported significant regional differences in the diagnostic delay. 24 The low regional variation in Finland is very likely affected by the frequently updated nationwide Current Care Guidelines for celiac disease. 29 The guidelines aim to increase awareness and diagnostic efficacy in celiac disease particularly in primary care.
As a result of this decentralization the prevalence of diagnosed celiac disease in Finland is among the highest in the world.28,30 There are no studies from other countries evaluating the effect of such a reorganization of celiac disease diagnostics, but the issue has been investigated for instance in inflammatory bowel disease and chronic lung diseases, with somewhat less promising results.31,32 We believe that primary care diagnostics can be very successful, but only if combined with practical diagnostic tools and continuous education of physicians.
Patients in the delay group reported more primary health care visits and days of sickness both in the year prior to and following the diagnosis. One reason leading to excess visits and ill health could be the often vague and unspecific symptoms not being recognized as celiac disease. 33 The higher use of health care even after the diagnosis might be related to our previous observation that diagnostic delay predisposes individuals to persistent symptoms on a gluten-free diet. 16 The increased number of days of sickness probably occurs for the same reasons as the excess health care visits. Interestingly, a similar association between delayed diagnosis and increased work absence has been reported in endometriosis patients, 34 further demonstrating difficulties encountered in cases of chronic diseases with a diverse clinical picture. The increased work absence in both study groups in the year following diagnosis can be explained for example by a severe infection season.
There was also incremental use of analgesics, antidepressants and medicines for dyspepsia in the delay group in the year prior to the diagnosis. Previous studies have already shown excessive use of pharmaceuticals preceding celiac diagnosis,8,35 and this problem would appear to be further aggravated by delay. We could not trace the indications for these drugs, but they might have been prescribed for example in an attempt to ameliorate persistent gastrointestinal and depressive symptoms caused by unrecognized celiac disease.13,36 A parallel association between delay and excessive analgesic use before diagnosis has again been observed in endometriosis patients. 37 In line with the lower quality of life and excess health care visits, the increased drug use continued even after the diagnosis. Besides slow resolution of symptoms, this might be due to patients’ reluctance to discontinue drugs they have used with some benefits perhaps for several years.
The main strengths of the study were its prospective design, the large nationwide patient cohort, validated questionnaires and broad range of relevant study outcomes. There was also an excellent response rate in the follow-up survey. On the other hand, questionnaire-based studies are prone to overrepresentation of healthy individuals who feel well, the risk of which is further aggravated by participants being members of celiac societies. It is also noteworthy that, although the treatment response was followed prospectively, outcomes and duration of symptoms before diagnosis were assessed retrospectively and are thus prone to recall bias. However, a recall period covering a maximum of one year in self-reported use of health care services and pharmaceutical agents has previously been shown to be reliable. 38 The fact that the patients were enrolled almost 10 years ago might in theory have an effect, but there have been no major changes in our health care system or celiac disease diagnostics, and we believe that the results are still representative. Finally, because of a lack of original patient records, we were unable to verify the self-reported medical information including celiac disease diagnosis, and to evaluate the possible impact of different comorbidities on results.
Conclusions
We found even a relatively short diagnostic delay in celiac disease to be associated with increased health burden both at the individual and society level. Improved awareness of the diversity of the disease among physicians and at-risk group screening could be an effective means to reduce the delay at the population level.
Footnotes
Declaration of conflicting interests
None declared.
Ethics approval
No ethical committee review was obtained because this was a questionnaire-based survey.
Funding
This work was supported by the Competitive Research Funding of Tampere University Hospital, the Sigrid Juselius Foundation, the Yrjö Jahnsson Foundation and the Foundation for Pediatric Research.
Informed consent
Informed consent was obtained from all participants after a written explanation of the aims of the study, including considerations regarding ethics and data protection and the anonymous deposition of the questionnaire.