
Abstract
Background
Celiac disease has been linked to decreased quality of life and certain mood disorders. The effect of the gluten free diet on these psychological aspects of the disease is still unclear.
Objectives
The objective of this article is to review the literature on psychological morbidity of celiac disease.
Methods
We performed a PubMed search for the time period from 1900 until June 1, 2014, to identify papers on psychological aspects of celiac disease looking specifically at quality of life, anxiety, depression and fatigue.
Results
Anxiety, depression and fatigue are common complaints in patients with untreated celiac disease and contribute to lower quality of life. While aspects of these conditions may improve within a few months after starting a gluten-free diet, some patients continue to suffer from significant psychological morbidity. Psychological symptoms may affect the quality of life and the dietary adherence.
Conclusion
Health care professionals need to be aware of the ongoing psychological burden of celiac disease in order to support patients with this disease.
Introduction
Celiac disease (CD) is a chronic immune-mediated enteropathy 1 characterized by a large spectrum of symptoms and signs that generally improve with good adherence to a gluten-free diet (GFD). 2
In recent years, there has been an increased interest in how celiac patients perceive the impact of their disorder, how this perception relates to the clinical presentation of the disease and how their health is modified by treatment with a GFD. It has been recognized that the aspects of health that should be addressed go beyond the usual biological parameters and extend also to social functioning and psychological issues. 3 Mood disorders such as anxiety, depression and fatigue are often linked to CD, before and after diagnosis, and therefore may influence the patient’s quality of life (QoL) and adherence to GFD.
Methods
This work is part of a project initiated by the Oslo group and British Society of Gastroenterology on the clinical management of CD. 2 We examined the literature on the QoL of celiac patients and some psychological aspects associated with CD (anxiety, depression and fatigue), asking how treatment with a GFD may modify them. A PubMed search identified papers on QoL, anxiety, depression and fatigue published between 1900 and June 1, 2014. Four authors (FZ, GLS, TRC, JCB) carried out the literature searches and the data collection and took the main responsibility for the writing of the paper. DSS and JFL reviewed the paper, giving important feedback.
Results
QoL
Several reports have described the difficulties of living with CD in adults, in particular as regards the impact of this condition on physical, social and emotional factors.4–23 Unfortunately, interest in the health perception of celiac patients has been affected by the lack of CD-specific QoL instruments allowing measurement of specific aspects of the disorder. Most studies exploring the QoL in CD patients used generic multi-item and multi-dimensional instruments developed for chronic disorders.24–28 The most widely used generic tools to estimate health-related QoL in CD were the Short Form Health Survey questionnaire
26
and the Psychological General Well-being index.
28
It is only recently that CD-specific questionnaires have been developed for pediatric29,30 and adult patients31,32 and translated into other languages.33–36 Although screen-detected37,38 and asymptomatic CD patients
39
seem to have a better QoL than symptom-detected patients at the time of diagnosis, the effect of the GFD is still unclear. Mustalahti et al. reported a positive effect of the GFD both in symptomatic and screen-detected patients,
37
Johnston et al. suggested the benefits were limited to those presenting with symptomatic disease,
38
Vilppula et al.
40
reported no change of the QoL in screen-detected patients on GFD and finally, Ukkola et al. described that the QoL improved in symptomatic and in screen-detected symptomatic patients but not in screen-detected asymptomatic patients
41
(Figure 1). Interestingly, a time-course assessment of the effect of treatment showed that, in symptomatic patients, the most significant quantitative improvement of most items is seen in the first three months after starting the GFD, with some additional improvement up to one year
39
(Figure 1). Compared to biological parameters, including serology, the time course for improvement of QoL measures seems to be earlier and faster.
39
Paavola et al., analyzing CD patients on long-term GFD, reported that the QoL was unimpaired in screen-detected celiac patients and lower in symptom-detected patients, when compared to healthy controls.
42
A recent randomized study showed that asymptomatic CD patients benefited from a GFD for anxiety and better health (based on the visual analog scale), but not for social function, when compared to similar patients following a gluten-containing diet.
43
Finally, Roos et al. showed similar psychological well-being in long-treated celiac patients and healthy controls.
16
Poor dietary adherence was associated with a poor QoL8,10 but whether one causes the other remains unknown, and consequently it is unclear which is the cause and which the effect. A recent long-term longitudinal study suggested that subsequent deterioration in QoL was associated with a lack of dietary adherence.
44
However, other studies45,46 reported no differences in QoL scores between patients with full adherence and patients with partial/nonadherence to GFD. Several papers reported lower QoL in women with CD than in celiac men.9,11–13,18 Finally, Paarlahti et al.
47
reported that a long duration of symptoms before diagnosis, psychiatric, neurologic or gastrointestinal comorbidities and persistent symptoms were predictors of a reduced QoL.
Quality of life (QoL) in screen-detected and symptom-detected celiac disease (CD) patients after one year of gluten-free diet. *QoL improved in symptomatic screening-detected patients.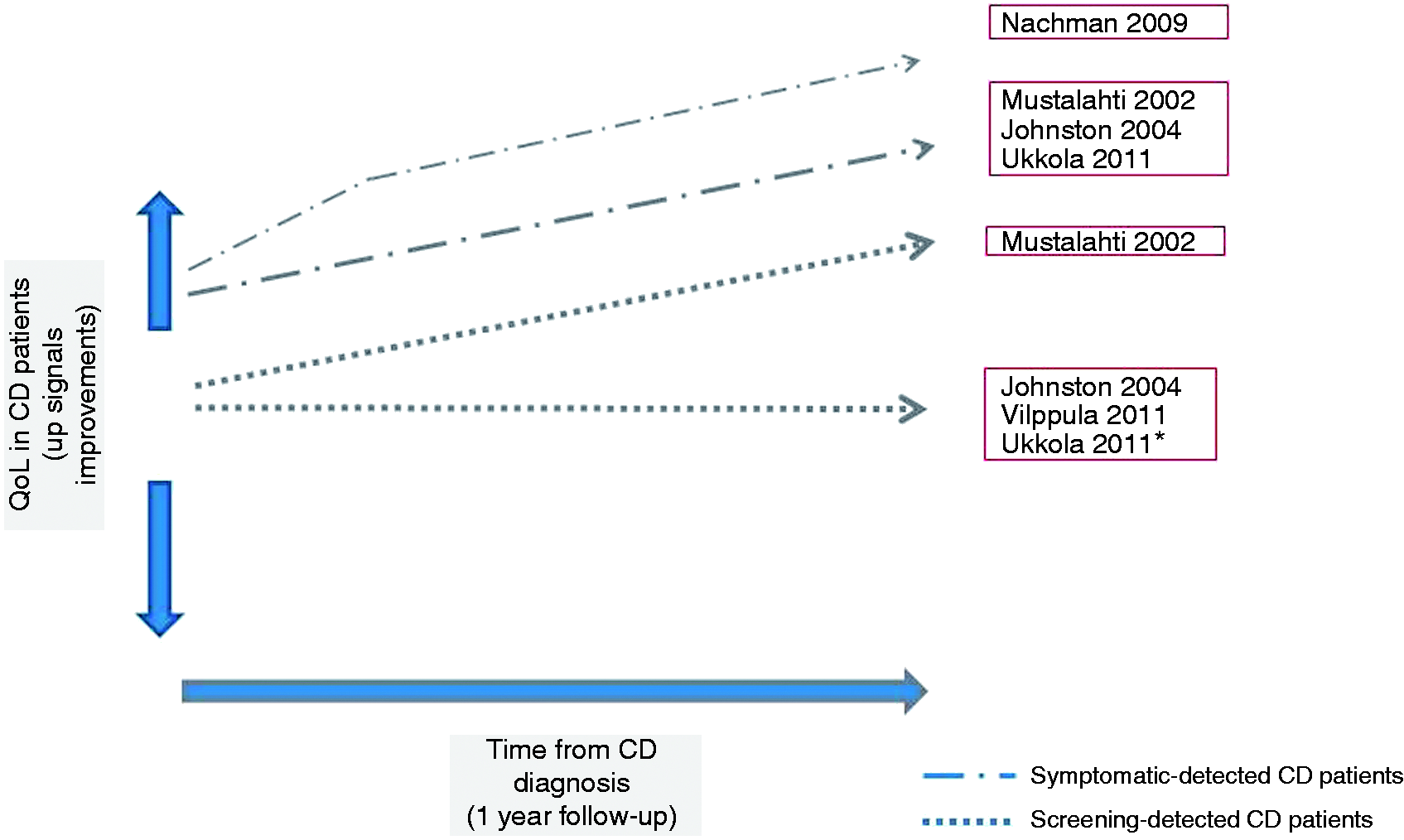
Anxiety
Previous literature on depression and anxiety in CD

BDI: Beck Depression Inventory; CD: celiac disease; CFS: chronic fatigue syndrome; CPH: chronic persistent hepatitis; FSS: Fatigue Severity Scale; GP: general practice; GFD: gluten-free diet; HADS: Hospital Anxiety and Depression Scale; IBQ: Illness Behavior Questionnaire; IBD: inflammatory bowel disease; IBS: irritable bowel syndrome; MSDS: Modified Zung self-rating Depression Scale; PSQI: Pittsburgh Sleep Quality Index; SF36: Short Form 36 Health Survey; STAI: State & Trait Anxiety Inventory; DM: diabetes mellitus; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders, 4th ed.
Depression
Depression has been associated with CD. 48 Morris et al. 55 and Hallert et al. 56 were among the first to describe this association. Though numerous papers have followed the causes of this association and the effect of a GFD on depression, these are still poorly defined (Table 1).
Using the modified Self-Rating Depression Scale, Addolorato et al. 51 described persistent depression after one year of GFD in celiac patients, Zingone et al. 57 and Siniscalchi et al. 58 showed that depression was present in CD at diagnosis, but that it persisted or even worsened in patients on a GFD. Nachman et al., 44 using the Beck Depression Inventory, showed that depressive symptoms were highly prevalent in untreated CD and there was a significant improvement in psychological symptoms after one year and four years of GFD. 44 However, the Beck Depression Inventory score at four years showed a significant worsening compared to one year, though CD patients at the four-year visit still had less depression than at CD diagnosis. A low adherence to GFD might be considered either a cause or a consequence of the persistent depression on GFD. This has been suggested in a 2004 study by Addolorato et al., which showed a beneficial effect of psychological support for CD patients on a GFD both in relation to psychological disorders and to improved dietary adherence. 59 Fera et al., 60 in a study of 100 patients treated for eight years, found a high rate of depression, detected by the modified Self-Rating Depression Scale, which tended to improve with time, but which was not correlated with dietary compliance. Similarly, a 2013 cross-sectional study, 61 reporting a self-reported depression prevalence of 39% among 2265 adult CD patients (based on the Major Depression Questionnaire), described that the long-term adherence to the GFD (>5 years) was associated with a reduced risk of depression, but they found no association between insufficient adherence and current depression symptoms. Finally, Häuser et al. 52 did not find any difference in depression between celiac patients on GFD and the general population. The authors reported no evidence that depression was predicted by diet adherence, years of GFD, presence of associated diseases, or delay in CD diagnosis. Finally, Barratt et al. 62 described that patients on a GFD, at risk of anxiety and depression according to the Hospital Anxiety Depression Scale, reported more symptoms in response to occasional dietary gluten exposure.
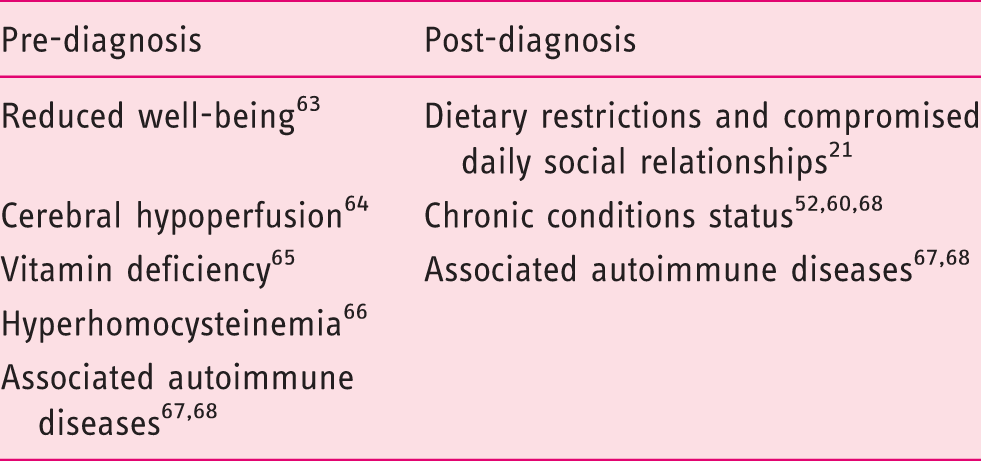
Mechanisms explaining psychological morbidities
Mechanisms potentially leading to psychological morbidity in celiac disease
Depression and anxiety may be associated with other factors including an unsatisfactory sexual life, 13 fatigue 58 and poor quality of sleep. 57 Furthermore, functional disorders, such as IBS72–74 and functional dyspepsia74,75 are frequently diagnosed in CD patients at diagnosis and in those on a long-term GFD. Since these disorders are also associated with reduced QoL and increase the likelihood of anxiety and depression in CD,76,77 treating these comorbidities may improve QOL and mood disorders in CD. 73
CD has been linked to a number of neurological disorders: ataxia, 78 neuropathy, 79 epilepsy, 80 and headache 81 while the evidence in multiple sclerosis has been mixed.79,82 Several of the above neurological disorders have been linked to poor QoL,83–85 and we cannot rule out that psychological dimensions of neurological comorbidity have thereby influenced QoL in CD patients. Neurological and psychological morbidities in CD patients might be caused by the mechanisms reported above, such as vitamin deficiency and hyperhomocysteinemia, as well as by the presence of antineuronal antibodies 86 and brain dysfunctions. 87 For example, a similar gray matter loss described in particular in the gyrus rectus and anterior cingulate gyrus of CD patients with neurological disturbances 87 has also been reported in individuals with depression.88,89
Fatigue
There is now good evidence to show not only that fatigue can be a symptom of CD, but also that it is a common clinical presentation.90–93 Serological screening for CD is now recommended in the workup of chronic fatigue. 94 Case finding studies suggest a CD prevalence of about 3% among those presenting with chronic fatigue, i.e. similar to that in patients with IBS. 92 Less is known about the prevalence of fatigue among those already on a GFD, or whether treatment of CD with a GFD successfully treats this symptom. In the last decade a small number of studies have more directly addressed these issues. Siniscalchi et al. in 2005 demonstrated that celiac patients both at diagnosis and when on a GFD had higher levels of fatigue than healthy controls using a variety of validated scales. 58 Perhaps more surprisingly, fatigue was not significantly different between newly diagnosed celiac patients and those on an established GFD. The same researchers from Naples have since shown that both treated and untreated celiac patients experience a worse quality of sleep than healthy volunteers 57 perhaps offering an explanation of the mechanisms behind this condition. Again, treated celiac patients did not show significantly different characteristics compared with their untreated counterparts. More recently, a large questionnaire study of 5912 Canadian celiac patients has suggested that “extreme weakness/tiredness” is reported by patients to improve over a prolonged period on GFD, such that of those on GFD for more than five years 72.4% reported this symptom had recovered. 95 Interpretation of these findings is made more difficult by the fact that data originate from cross-sectional studies, rather than from either randomized controlled trials of the effect of GFD, or cohort studies to permit examination of the alteration in state within individuals after establishment of a diet. It is therefore unwise to conclude too firmly that GFD either does or does not alleviate fatigue in CD from the available evidence. One other potentially relevant finding is the suggestion that dietary supplementation with L-carnitine may treat fatigue in CD. 96 Since carnitine is absorbed in the small intestine, 97 it is tempting to assume that resolution of malabsorption should facilitate the intestinal uptake of carnitine. However, the range of gastroenterological and non-gastrointestinal conditions in which similar effects have been suggested indicates that mechanisms other than the correction of a deficiency may be operating.98,99
Summary
Our search of the available literature suggests that CD has a considerable psychological impact. Some elements of this may relate to the disease and its biochemical effects, but other aspects relate to the patient’s subjective perception of the disorder and of the GFD used to treat it. The treatment of CD results in a significant improvement in QoL for symptomatic patients, but patients with subclinical CD often report no such effect. However, a proportion of subclinical patients may report improvement in QoL parameters after commencing treatment. Overall, levels of anxiety and depression are greater in patients with CD (Table 1). However, the causes of this may vary at different stages (Table 2). Prior to CD diagnosis, patients may express concerns about unexplained symptoms and may feel frustrated about repeated consultations that offer no adequate explanation of their problems. At the time of diagnosis, there may be concerns about investigations and a diagnosis of a long-term condition, although this may be accompanied by a feeling of relief that a diagnosis has finally been made. While some psychological problems may lessen with time as knowledge of the condition improves and perhaps biochemical abnormalities are corrected, it appears that many patients have ongoing concerns about coping with the diet and do not adhere to it, particularly when going out and in social interaction. Fatigue is sometimes the unique symptom at CD presentation. Conversely, 3% of patients with chronic fatigue may be found to have CD. The available studies have not been able to show a consistent positive effect of the GFD in diminishing perception of fatigue.
Conclusion
The literature on the effect of treatment in the outcome of depression, anxiety, fatigue and QoL in CD is not consistent. However, it is important to consider that ongoing problems with anxiety and depression in particular may affect dietary adherence and QoL. Thus, health care professionals need to be aware of the ongoing psychological burden of CD in order to support their patients. The lack of clear evidence of improved QoL in asymptomatic CD after treatment makes mass screening, where a majority of patients may be subclinical or asymptomatic, controversial if the aim of screening is to improve QoL. Further studies are required to better understand this specific aspect.
Clinical implications
Celiac disease (CD) has a considerable psychological impact. Biochemical effects and the patient’s subjective perception of the disorder and of the gluten-free diet (GFD) may be causes of the psychological morbidities. GFD improves quality of life (QoL) in symptomatic patients, but not always in asymptomatic patients. Anxiety and depression may affect dietary adherence and QoL. Fatigue is sometimes the unique symptom at CD presentation. Health care professionals need to support CD patients on GFD. There is no evidence to support mass screening as the GFD fails to improve the QoL in asymptomatic, screen-detected CD patients.
Footnotes
Funding
JFL was supported by grants from The Swedish Society of Medicine and the Swedish Research Council – Medicine (522-2A09-195). TC derives his salary from the University of Nottingham and the Nottingham University Hospitals NHS trust.
Conflict of interest
TC has received grant support from Coeliac UK: Crohn’s and Colitis UK. DSS has received an educational grant from Dr Schär (a gluten-free food manufacturer) to undertake an investigator-led research study on gluten sensitivity. He also has received an educational grant both from Biocard and Simtomax to undertake an investigator-led research study on point-of-care tests.