
Abstract
Background
Obesity is associated with changes in the intestinal microbiome and methane-producing archaea may be involved in energy homeostasis.
Objective
The objective of this article is to investigate the associations between intestinal methane production, waist circumference and body mass index (BMI) as biomarkers for obesity.
Methods
Breath methane and hydrogen concentrations were measured over five hours following fructose or lactose ingestion in 1647 patients with functional gastrointestinal disorders. The relationships between gas concentrations and measures of obesity were investigated by stratifying gas concentration-time profiles by BMI and waist circumference, and, conversely, BMI and waist circumference by peak breath hydrogen and methane concentrations.
Results
Following fructose ingestion, patients with lower BMI and lesser waist circumference had greater breath methane concentrations (all p < 0.003). Conversely, patients with increased methane concentrations had lower BMI (p < 0.001) and waist circumference (p = 0.02). After lactose ingestion, BMI and waist circumference were not associated with significant differences in methane. However, greater methane concentrations were associated with a lower BMI (p < 0.002), but not with waist circumference.
Conclusion
In this large group of patients mainly negative associations between breath methane concentrations and anthropometric biomarkers of obesity were evident. Studies investigating microbial methane production and energy homoeostasis in different populations are of substantial interest to distinguish epiphenomena from true causality.
A follow-up study was registered at Clinical trials.gov NCT02085889.
Keywords
Key summary
Summarise the established knowledge on this subject:
Obesity is linked to changes in the intestinal microbiome. Methane-producing archaea may be involved in mechanisms of energy homoeostasis. Previous smaller studies propose a possible positive association between intestinal methane production and body mass index as a marker for obesity. What are the significant and/or new findings of this study?
Strong negative associations in this cross-sectional study between intestinal methane production and anthropometric biomarkers of obesity and the metabolic syndrome were evident in patients with functional gut disorders. Fructose and lactose differ in their methanogenic potential and in their association with markers of obesity. Further studies investigating a potential causal relationship between methane production by specific sugars and energy homoeostasis in different populations are of substantial interest.
Introduction
Obesity is a significant and increasingly prevalent risk factor for the development of cardiovascular disease, hypertension, type 2 diabetes, dyslipidaemia and the metabolic syndrome. Abdominal or visceral obesity is identified by elevated waist circumference, and somatic obesity is reflected in a raised body mass index (BMI). Due to the limitations of BMI methodology, the World Health Organisation (WHO) and other organisations suggest both BMI and waist circumference be used for assessment of obesity.1,2 Obesity is increasingly linked to changes in the intestinal microbiome, such as a lower relative abundance of Bacteroidetes and a higher relative abundance of Firmicutes, and weight loss is positively correlated with the prevalence of Bacteroidetes. 3 Methane production by archaea (methanogens) such as Methanobrevibacter smithii, may be implicated in mechanisms of energy homeostasis, as methane is associated with weight gain and more efficient intestinal energy extraction, as well as impaired glucose intolerance.3–7 Previous studies have shown a link between intestinal methane production, compromised glycaemic control and obesity.3–7 Intestinal methane production has also been linked to changes in gastrointestinal (GI) motility, especially in the constipation phenotype of irritable bowel syndrome (IBS).8–13 However, no significant link between constipation and a raised BMI was found in a very large population-based, online self-assessment IBS study. 14 The relationship between symptoms and the composition of the intestinal microbiome in IBS is a matter of ongoing investigation, and multiple differences compared to healthy controls have been described. 15 The aim of this large monocentric study was to investigate the relationships between methane production after fructose and lactose ingestion and biomarkers of obesity and metabolic syndrome. Our hypothesis was that we would detect a positive relationship between the obesity risk indices and breath methane levels.
Materials and methods
All successive patients with functional gastrointestinal disorders (FGID) referred to our gastroenterology practice by general practitioners, as defined according to the Rome III criteria, were included in this study. 16 We performed lactose and fructose breath tests in all these patients and included all FGID patient data irrespective of the breath test outcome to avoid a selection bias. Exclusion criteria were evidence of organic disease, as assessed by haematology and biochemistry blood testing, and stool testing for calprotectin and pancreas elastase. Coeliac disease was excluded by tissue anti-transglutaminase antibodies or duodenal biopsies. Upper and lower endoscopies with biopsies were required in patients older than 40 years or in patients with diarrhoea or faecal blood. Parasite and bacterial stool cultures and abdominal ultrasound were performed if clinically indicated. One consultant gastroenterologist (CWS) performed all the medical and dietary history, taking and examinations. Patients completed a standardised questionnaire, which included the specific questions for classification of GI symptoms into FGID groups according to the Rome III criteria, and additional questions regarding allergies, childhood and family history, central nervous, musculoskeletal and cardiovascular system symptoms and the use of polyol-containing sweets and chewing gum. BMI was calculated using body weight and height (kg/m2) and waist circumference was measured. The study was performed in accordance with the 1975 Declaration of Helsinki. For this study analysing coded clinical data with no additional research-related procedures, no institutional ethics board approval or written informed consent was required in Switzerland at the time of initiation of the study. Approval was subsequently gained for the follow-up study from the Cantonal Ethics Committee in Bern, Switzerland (28 July 2016, 328/15) and the study was registered at Clinical trials.gov NCT02085889.
Breath test protocol
Both fructose and lactose breath tests were performed by the same technician (AM) in all patients with FGID using a standardised, previously published protocol. 17 The breath tests were performed in randomised sequence on two separate occasions at least six days apart. Breath samples were collected in sealed glass tubes (Quintron Instruments, Milwaukee, WI, USA) before and hourly for five hours after ingestion of lactose 50 g or fructose 35 g dissolved in 300 ml water. Hydrogen, methane and CO2 concentrations were measured within 72 hours using the Quintron BreathTracker SC® (Quintron Instruments, Milwaukee, WI, USA).
Statistics
The absolute gas concentration-time profiles without any baseline correction were stratified by BMI and waist circumference according to the WHO criteria, to circumvent the use of arbitrarily defined gas thresholds.1,2 BMI categories are: underweight: BMI <18.5 kg/m2, normal weight: BMI 18.5–25 kg/m2, overweight: 25–30 kg/m2, obesity: BMI >30 kg/m2. Waist circumference categories for increased risk of metabolic syndrome are: females >88 cm and males >102 cm. Additionally, for comparison with published data, participants were classified into four groups according to their peak breath gas concentrations without any baseline correction: normal (N: methane <3 parts per million (ppm) and hydrogen <20 ppm); hydrogen positive only (H+: methane <3 ppm and hydrogen ≥20 ppm); methane positive only (M+: methane ≥3 ppm and hydrogen <2 ppm), or methane and hydrogen positive (M+/H+: methane ≥3 ppm and hydrogen ≥20 ppm). 5
All data are presented as means ± SD unless otherwise indicated. Student’s t-test, analysis of variance (ANOVA), Dunn’s pairwise comparison test, chi-squared tests, Fisher’s exact or McNemar’s tests were used to compare demographic, clinical and anthropometric variables, as appropriate. In case of multiple comparisons, a Bonferroni adjustment was applied. Mixed models were used for analysis of time-gas curves with adjustment for age, gender and race as appropriate. The software package STATA version 14.2 (StataCorp LP, College Station, TX, USA) was used for statistical calculations.
Results
Demographic and anthropometric characteristics of the study cohort (n = 1647).
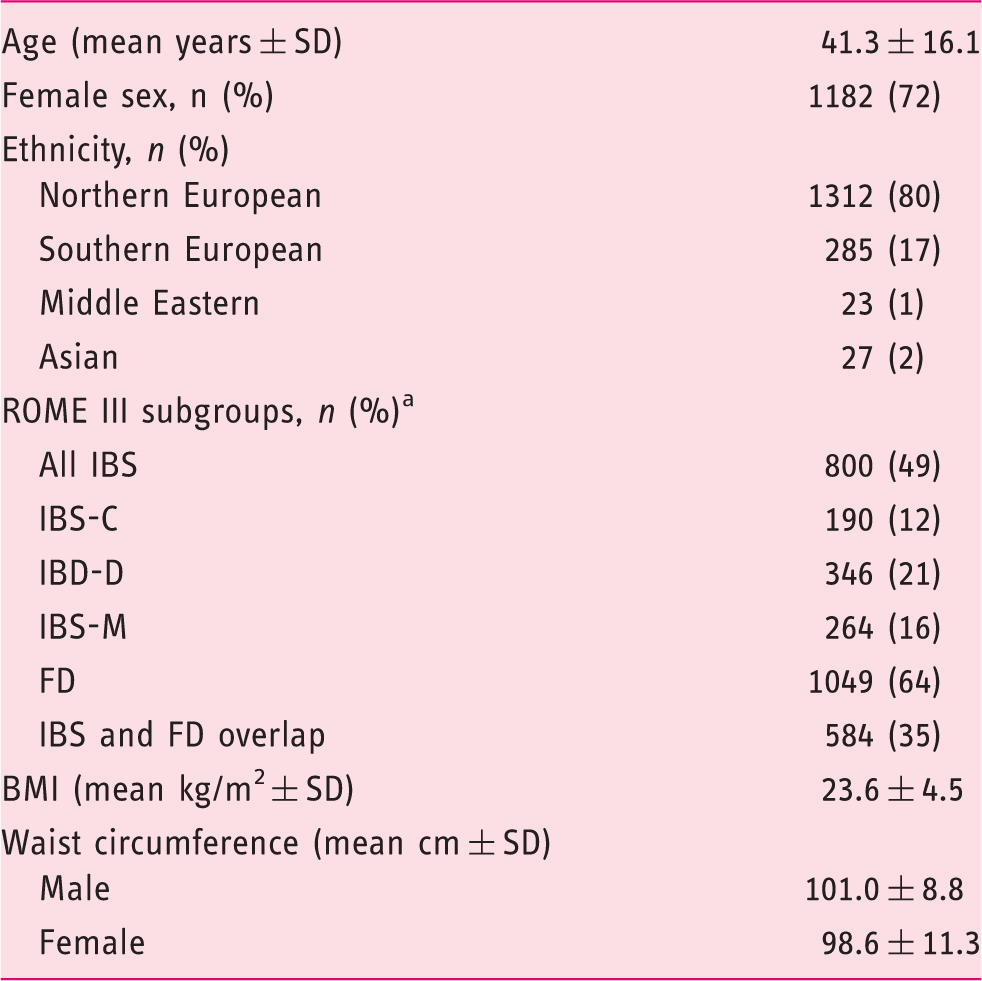
Percentages of functional gastrointestinal disorder subgroups do not add up to a total of 100% due to extensive overlap.
IBS: irritable bowel syndrome; C: constipation; D: diarrhoea; M: mixed; FD: functional dyspepsia; BMI: body mass index.
Relationships between breath gas concentrations and BMI
Demographic characteristics by body mass index (BMI) subgroups according to World Health Organisation classification a .
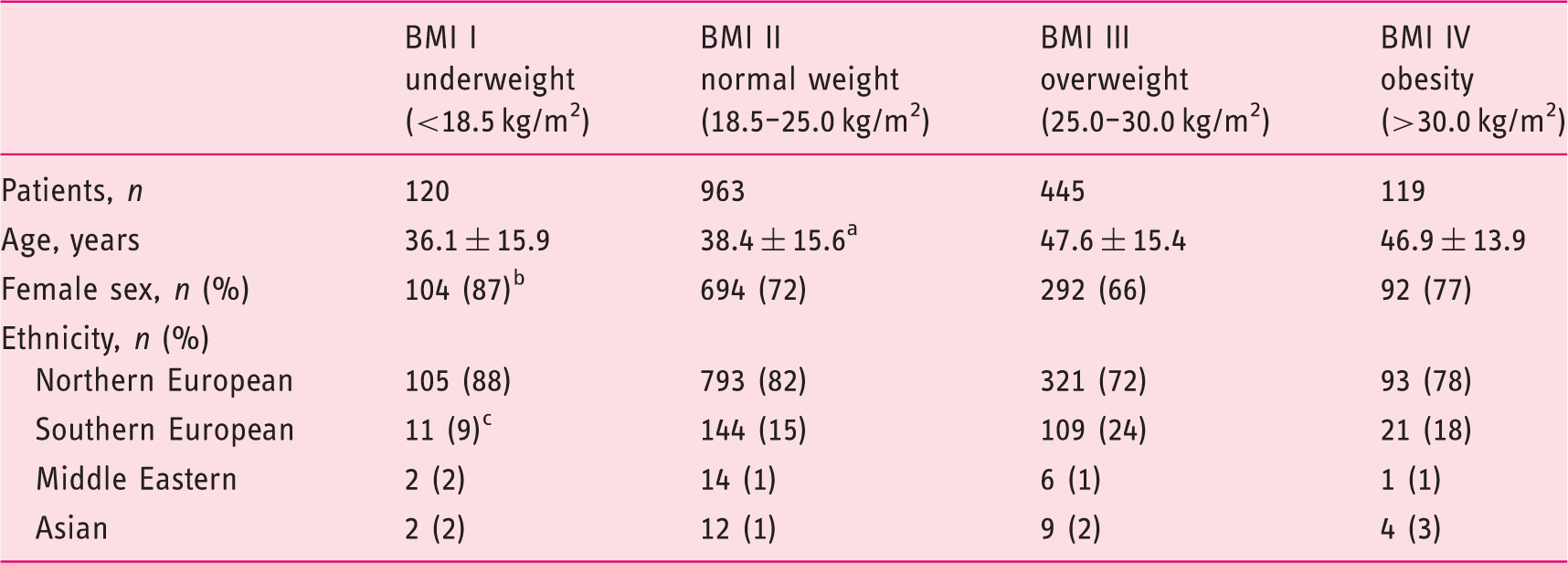
Normal weight (BMI II) versus overweight (BMI III) and obese (BMI IV): p < 0.001.
Underweight (BMI I) versus normal weight (BMI II): p < 0.001.
Underweight (BMI I) versus normal weight (BMI II): p < 0.001.
Figure 1 shows the gas concentration-time profiles of the WHO-defined BMI subgroups following fructose or lactose ingestion.
Breath methane and hydrogen concentration-time profiles of body mass index (BMI) subgroups (World Health Organisation definition
1
: BMI <18.5 kg/m2: blue, 18.5–25 kg/m2: brown, 25–30 kg/m2: green, >30 kg/m2: yellow) during fructose (top row, methane left panel, hydrogen right panel) and lactose (bottom row, methane left panel, hydrogen right panel) breath tests. Means and 95% confidence intervals are shown. See Results text for significant differences.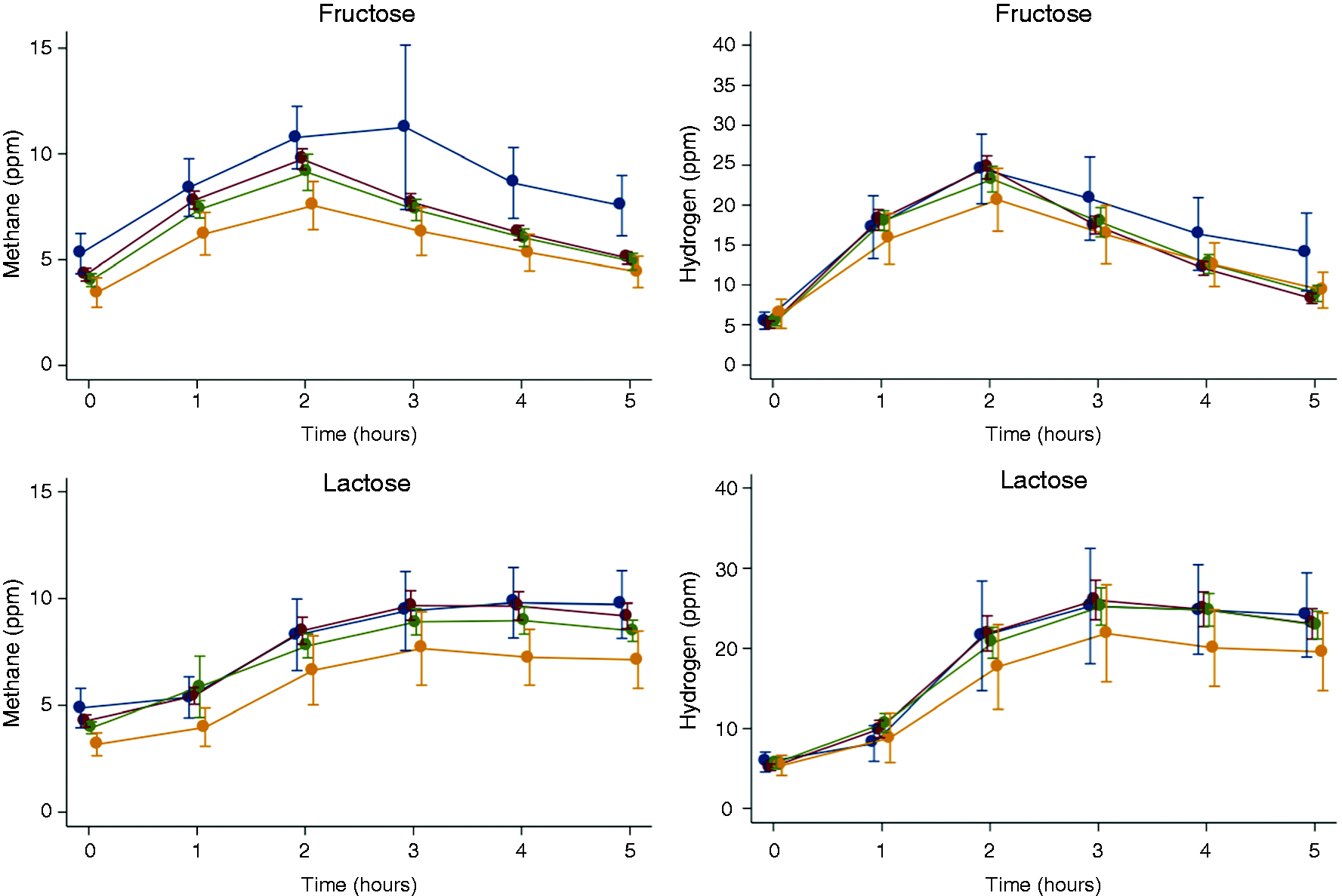
Fructose test
Overall, breath methane concentrations were significantly greater in the underweight and normal weight patients compared to their overweight and obese counterparts. Specific significance thresholds were BMI <18.5 kg/m2 vs. BMI 25.0–30.0 kg/m2, p = 0.003; BMI <18.5 kg/m2 vs. BMI >30–0 kg/m2, p < 0.0001; BMI 18.5–25.0 kg/m2 vs. BMI 25.0–30.0 kg/m2, p = 0.002; BMI 18.5–25.0 kg/m2 vs. BMI >30–0 kg/m2, p = 0.0001, Figure 1). No significant differences in breath hydrogen concentrations were observed across BMI subgroups (Figure 1).
Lactose test
Breath methane concentrations were greater in underweight and normal weight patients compared to obese patients. Specific significance thresholds were BMI <18.5 kg/m2 vs. BMI >30.0 kg/m2, p = 0.002; BMI 18.5–25.0 kg/m2 vs. BMI >30.0 kg/m2, p = 0.001, Figure 1). There were no significant differences in breath hydrogen concentrations across BMI subgroups (Figure 1).
Relationships between breath gas concentrations and waist circumference
Demographic characteristics of patients classified for visceral obesity by waist circumference. A waist circumference greater than 88 cm in females and 102 cm in males is considered an increased risk of metabolic syndrome a .
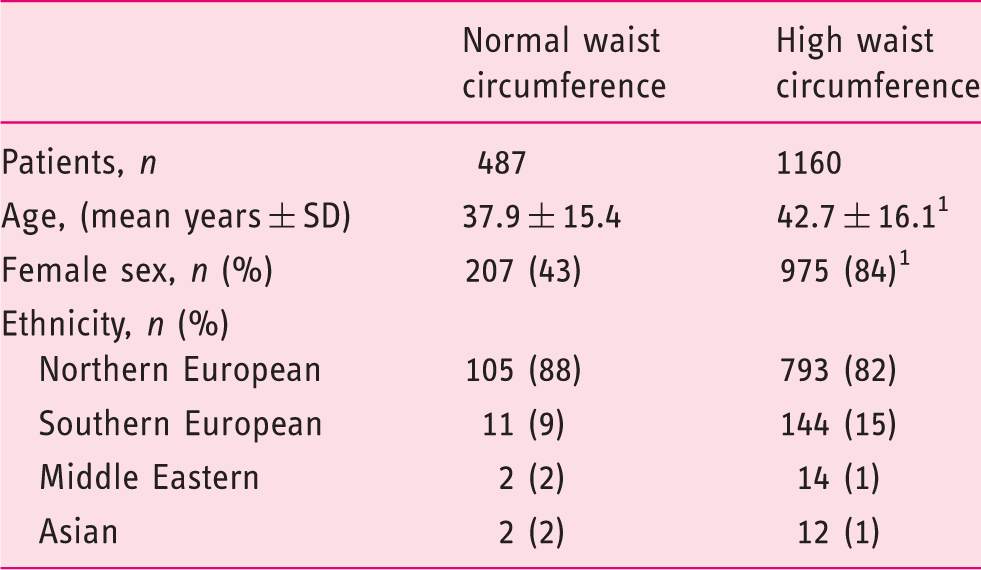
High versus normal waist circumference: p < 0.001.
Figure 2 shows the gas concentration-time profiles of the waist circumference subgroups following fructose or lactose ingestion.
Breath methane and hydrogen concentration-time profiles in patients with normal (blue) and with increased (brown) waist circumference during fructose (top row, methane left panel, hydrogen right panel) and lactose (bottom row, methane left panel, hydrogen right panel) breath tests. Increased waist circumference is defined as >88 cm for females and >102 cm for males. Means and 95% confidence intervals are shown. See Results text for significant differences.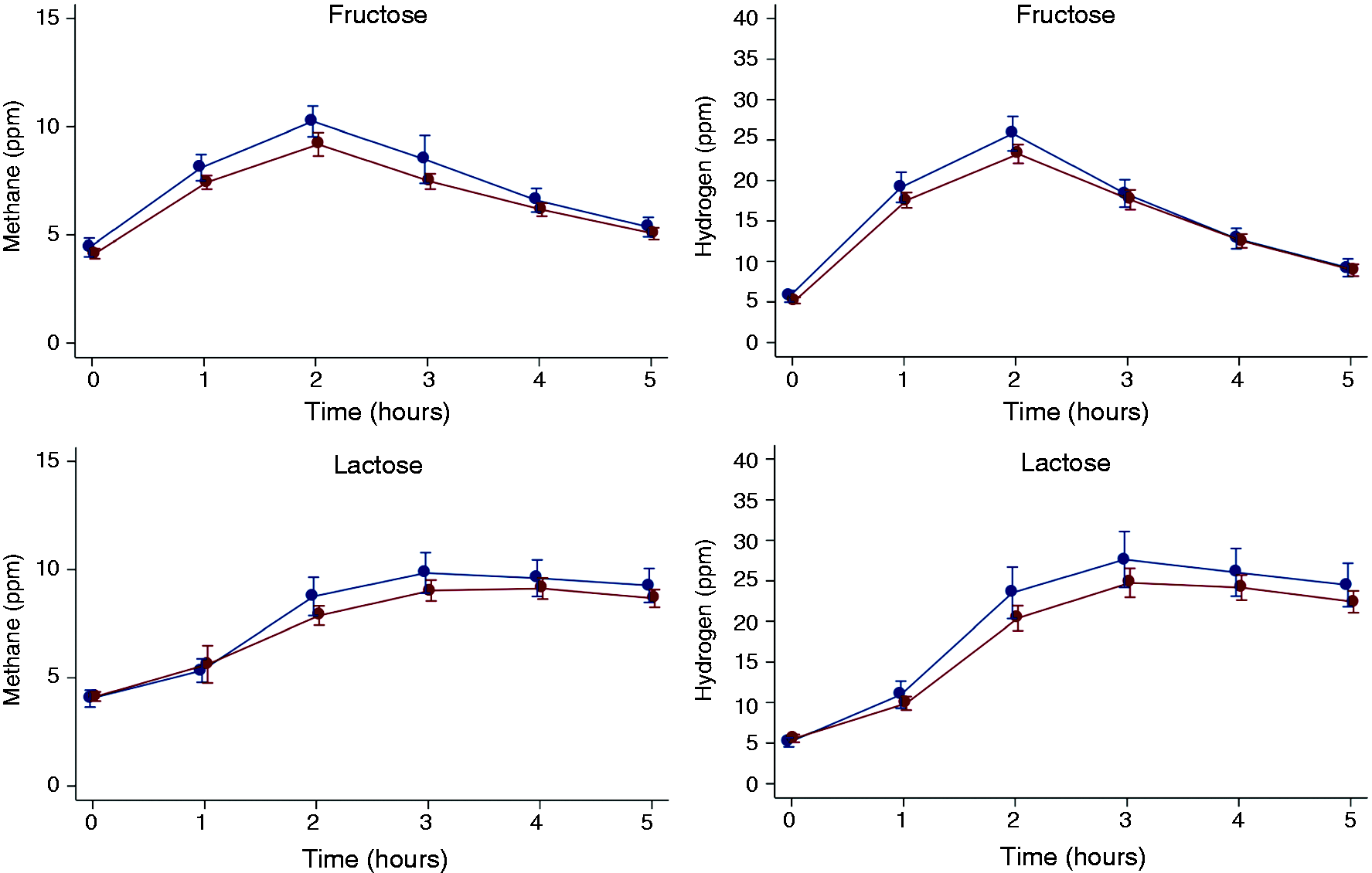
Fructose test
Breath methane and hydrogen concentrations were greater in the leaner than in the adipose patients (p < 0.001 and p = 0.016, respectively).
Lactose test
No significant differences were observed in methane or hydrogen (p = 0.53 and p = 0.42, respectively).
Relationships between BMI and waist circumference and published peak methane and hydrogen thresholds 5
Demographic and anthropometric characteristics of patients grouped according to breath methane and hydrogen concentration following fructose or lactose ingestion. 5 Threshold classifications are: normal (methane <3 ppm, hydrogen <20 ppm); hydrogen-positive only (methane <3 ppm, hydrogen ≥20 ppm); methane positive-only (methane ≥3 ppm, hydrogen <20 ppm), and methane and hydrogen positive (methane ≥3 ppm, hydrogen ≥20 ppm).
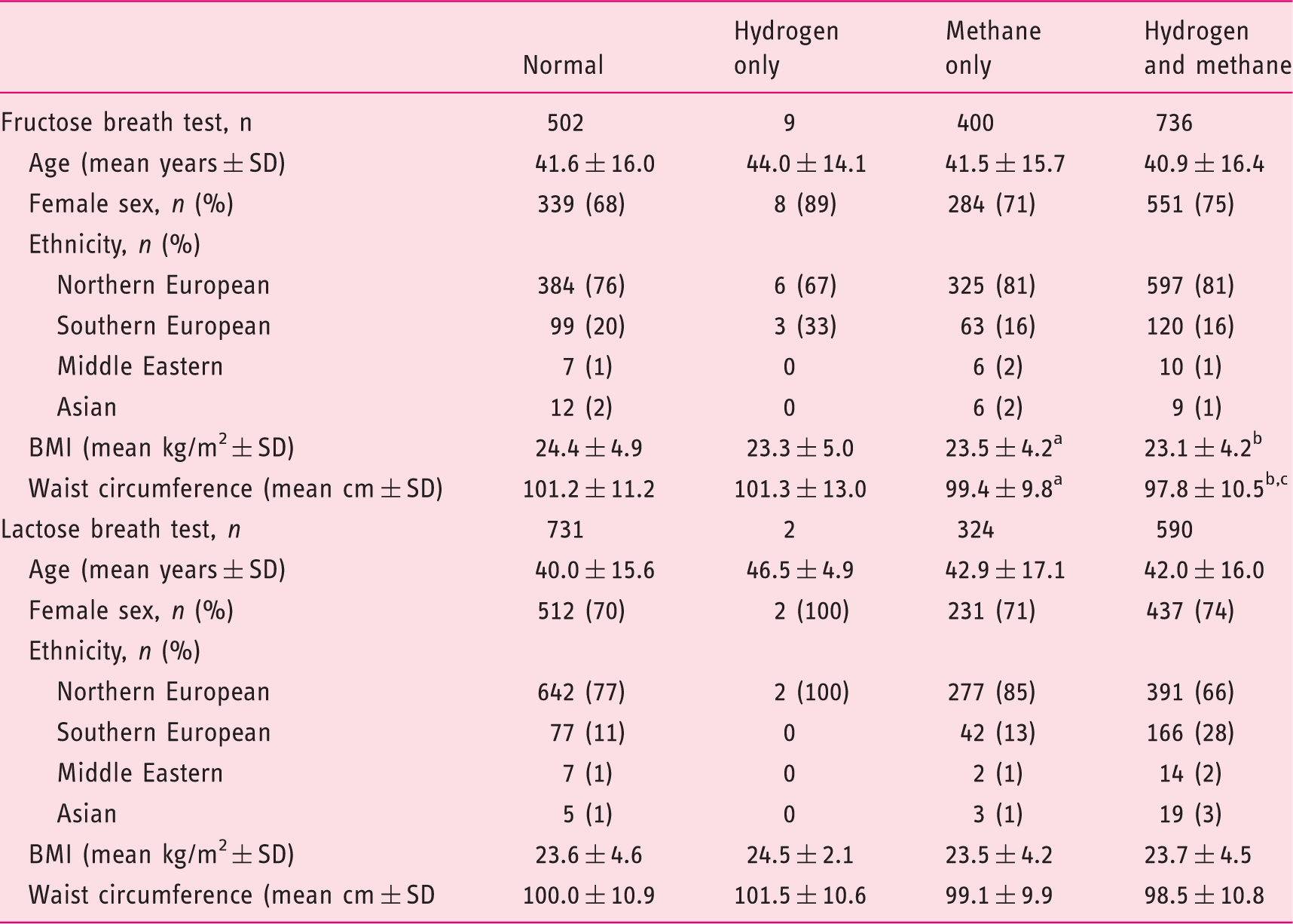
Versus normal gas concentration group: ap < 0.05; bp < 0.001.
Versus methane-only gas concentration group: cp < 0.05.
ppm: parts per million; BMI: body mass index.
Fructose test
Methane concentrations above 3 ppm were associated with a lower BMI than methane concentrations below 3 ppm, both with or without increased hydrogen production (p < 0.001 and p = 0.02, respectively) (Table 4). Similarly, methane concentrations above 3 ppm were associated with a lesser waist circumference than methane concentrations below 3 ppm, both with or without excessive hydrogen production (p < 0.001 and p = 0.04, respectively).
Lactose test
Patients with increased methane and/or hydrogen concentrations had similar BMIs and waist circumferences as patients without increased breath gas concentrations.
Discussion
Several pertinent aspects emerge from this investigation of the relationship between breath gas concentrations following fructose and lactose ingestion and measures of somatic and visceral obesity. Importantly, neither of the biomarkers for obesity and risk of the metabolic syndrome correlated positively with breath methane concentrations in this very large group of patients with FGID. In fact, a reverse association was consistently observed following fructose ingestion, by which leaner patients had greater methane gas concentrations than overweight patients. This negative association was also true for the biomarker for visceral obesity, waist circumference, following fructose ingestion. The findings were less pronounced following lactose ingestion. However, an inverse relationship between BMI subgroups and methane concentrations was also observed.
Elevated intestinal methane production as measured in breath samples does not appear to be associated with an increased risk of obesity in our setting, and the findings of Mathur’s group could not be replicated.5,6 Several potentially confounding factors need to be considered, which, nonetheless, are unlikely to fundamentally affect the qualitative comparability of the results. Genetic and environmental factors, such as diet, medication and lifestyle, are known to influence the composition and metabolism of the human microbiome.18,19 Population differences in these factors are consequently likely to affect the type and quantity of gas produced during breath tests. Nonetheless, the principal methanogens across several human populations have been shown to be methanobacteriales and methanomassillicocales, mainly Methanobrevibacter smithii and Methanosphaera stadtmanae, and breath methane is a reliable surrogate for gut colonisation with M. smithii.4,20,21–25 Furthermore, disappearance of methane from a breath test correlates strongly with a reduction of M. smithii levels in stool. Emerging evidence suggests patients with FGID may have a different microbiome compared to asymptomatic controls, but methanogens appear to be equally prevalent in IBS and in controls, although associated with a Clostridiales-enriched enterotype. 21 Most human studies have measured breath methane concentrations, which reflect only a fraction of intestinal methane production. 26 However, a recent study demonstrated colonic and breath methane production are significantly correlated, even if quantitatively markedly different. 27 Colonic gas production was similar between IBS patients, irrespective of subtype, and controls. 27 Taken together, existing data suggest quantitative but not qualitative differences in methane production between populations.
Divergent study breath test protocols may also explain some of the variation between study results. Between 55% (lactose) and 69% (fructose) of our patients with FGID produced measurable amounts of breath methane, whereas in the largest previous study of the relationship between BMI and breath methane in patients probably investigated for FGID, only 16% were methane producers. 5 According to the published literature, approximately 30%–60% of most populations would be expected to have positive methane breath tests, and up to 100% of humans are likely colonised by methanogenic bacteria.22–24,26,27 Based on previous validation studies, we collected hourly breath samples for five hours after ingestion of fructose or lactose, and have repeatedly shown that average peak methane as well as hydrogen concentrations occur after approximately two hours with fructose and three hours with lactose.17,28 Thus, the sampling period of only 90 to 120 minutes in studies by Mathur et al. 5 is likely to yield results preferentially reflecting the small intestinal microbiome, or patients with rapid intestinal transit. Methanogens appear to favour a slow-transit environment, and an association between a methanogenic microbiome and the constipation phenotype has been postulated.8,10,24 It has, on the other hand, been proposed, that 19% of duodenal bacteria may be methanogenic, suggesting the low frequency of positive breath methane responders may well be due to the short sampling period in these studies. 29
Different fermentable sugars have been used in the assessment of methane production, with few comparisons between them. Differences in fermentation between glucose and lactulose are well known in the assessment of small intestinal bacterial overgrowth and we have already alluded to the consistent and significant differences in peak breath gas concentrations between fructose and lactose.17,28 Our data uniquely demonstrate that fructose and lactose differ in their methanogenic potential and also in their association with markers of obesity in malabsorbers. Different bacteria have been shown to preferentially ferment specific sugars and divergent topographic intestinal distributions of bacteria or archaea would be expected to yield varying breath gas patterns. 30 Different sugar probes may consequently highlight divergent responses from either different or overlapping microbial populations with potentially varying clinical phenotypes. The use of different sugars between studies may, therefore, also explain some of the quantitative differences between the studies.
This study of cross-sectional associations clearly does not allow conclusion regarding underlying mechanisms. The clinical study of the relationships between intestinal methanogenic archaea and obesity, glycaemic control, improved glucose and insulin levels, successful bariatric surgery and weight loss has so far yielded ambiguous results; however, there are strong indications of the involvement of methanogenic pathways.31–35
In conclusion, at present the association between obesity and methanogens remains contradictory in humans, despite some suggestive, poorly translatable evidence in rodents. Further studies investigating a potential causal relationship between microbial methane production from specific sugars and energy homoeostasis in different human populations are of substantial interest to distinguish epiphenomena from true causality.
Footnotes
Declaration of conflicting interests
None declared.
Ethics approval
This study was performed in accordance with the 1975 Declaration of Helsinki. Approval was subsequently gained for the follow-up study from the Cantonal Ethics Committee in Bern, Switzerland (28 July 2016, 328/15) and the study was registered at Clinical trials.gov NCT02085889.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
For this study analysing coded clinical data with no additional research-related procedures, no institutional ethics board approval or written informed consent was required in Switzerland at the time of initiation of the study.