
Abstract
Lactose malabsorption is a common condition caused by reduced expression or activity of lactase in the small intestine. In such patients, lactose intolerance is characterized by abdominal symptoms (e.g. nausea, bloating, and pain) after ingestion of dairy products. The genetic basis of lactose malabsorption is established and several tests for this condition are available, including genetic, endoscopic, and H2-breath tests. In contrast, lactose intolerance is less well understood. Recent studies show that the risk of symptoms after lactose ingestion depends on the dose of lactose, lactase expression, intestinal flora, and sensitivity of the gastrointestinal tract. Lactose intolerance has recently been defined as symptoms developing after ingestion of lactose which do not develop after placebo challenge in a person with lactose maldigestion. Such blinded testing might be especially important in those with functional gastrointestinal diseases in whom self-reported lactose intolerance is common. However, placebo-controlled testing is not part of current clinical practice. Updated protocols and high-quality outcome studies are needed. Treatment options of lactose intolerance include lactose-reduced diet and enzyme replacement. Documenting the response to multiple doses can guide rational dietary management; however, the clinical utility of this strategy has not been tested. This review summarizes the genetic basis, diagnosis, and treatment of lactose malabsorption and intolerance.
Keywords
Digestion of lactose
Definition of important concepts
Lactose is the main source of sugar from milk and milk products from all mammals except the sea lion. Inadequate lactase activity allows lactose to reach the large intestine. There, the gut flora provides a salvage pathway for lactose digestion by cleaving lactose into short-chain fatty acids (SCFA) and gas, mainly hydrogen (H2), carbon dioxide (CO2), and methane (CH4). Non-digested lactose can cause osmotic diarrhoea; products of its bacterial digestion can lead to secretory diarrhoea and gas distending the intestines, events that are likely to lead to clinical symptoms. 2
Causes of lactase deficiency
The most frequent cause of lactose malabsorption is lactase non-persistence, a common condition in which lactase expression decreases during infancy. In contrast, congenital lactase deficiency due to complete lack of the enzyme is a rare condition that presents with severe symptoms in newborns. In addition, lactase malabsorption may be secondary to acquired conditions including small bowel bacterial overgrowth, infectious enteritis (i.e. giardiasis), or mucosal damage due to coeliac disease, inflammatory bowel disease, drugs, gastrointestinal surgery, short bowel syndrome, or radiation enteritis, conditions that lead to either reduction of absorptive capacity or downregulation of lactase expression in the small intestine.
Genetics of lactase non-persistence
Lactase activity changes during development. In most humans, lactase activity reaches a maximum in late pregnancy but declines after 2–3 years of age and reaches a stable low level at age 5–10, a process which might help weaning. However, a proportion of the human population, especially Caucasians from Northern Europe or northern European descent, retain high lactase levels during adulthood (lactase persistence). Both, lactase persistence and non-persistence (leading to lactose malabsorption) are thus normal human phenotypes. 3
Prevalence of lactase persistence is high in most regions in Scandinavia, the British islands, and Germany (80–95%); however, this condition is observed in only 20–40% of Indian adults, 30% of Mexicans, 30% of African Americans, and <10% of adults in Southeast Asia4,5 (Figure 1). Lactase persistence is thought to be related to the development of farming during the last 10,000 years. The genetic polymorphism responsible for most cases of lactase persistence in Caucasian individuals is the −13910C/T variant (thereby, T at position 13910 upstream of the lactase gene within a putative regulatory DNA-region causes persistence; C leads to non-persistence).
6
In contrast, in African tribes that herd cattle in Sudan, Kenya, and Tanzania), lactase persistence is mediated by the −14010*G, −13915*G or −13907*C polymorphism,3,7 and in Saudi Arabia by the −13915*G polymorphism.
8
Thus, lactase persistence developed several times independently in human evolution in different areas of the world (for review, see Ingram et al.
3
).
Interpolated frequency of the lactose malabsorption phenotype in the Eastern Hemisphere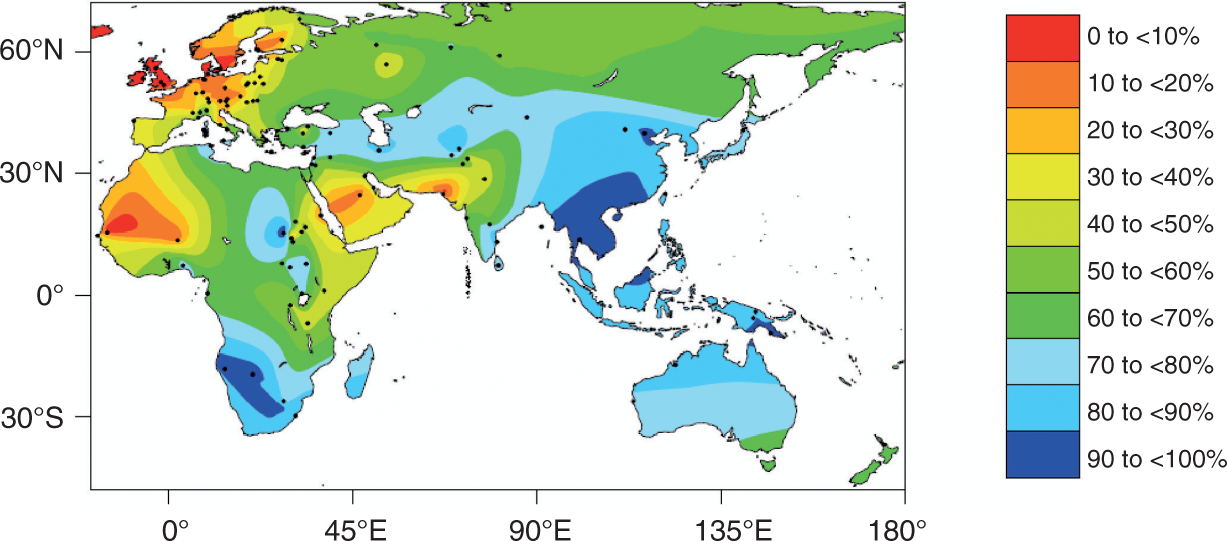
Statistical calculations of genetic data estimated that selection for lactase persistence commenced relatively recently, during the last 10,000 years.3,9,10 Lactase persistence was beneficial for our ancestors by providing a clean source of fluid and a source of protein, fat, and carbohydrates. 3 Lactase persistence generated a selective advantage of 1.5–19% in each generation.7,9 This indicates a strong selection pressure comparable to malaria resistance genes (2–5% for G6PD deficiency, 5–18% for sickle-cell trait) in various parts of the world.
The exact molecular mechanism for lactase persistence is unknown but factors enhancing gene transcription appear to be responsible by binding to a regulatory region 13,000 to 14,030 base pairs upstream of the lactase gene.3,11–13 In adult patients with homozygous lactase persistence, enzyme levels at the jejunal brush border are 10-times higher than for patients with homozygous non-persistence, heterozygous individuals showing intermediate levels. 14
Definition of lactose intolerance
The lactose-rich diet in Western countries can cause symptoms in individuals with the lactase non-persistence phenotype. Typical gastrointestinal complaints are diarrhoea, nausea, bloating, borborygmi, and abdominal pain. A wide range of systemic problems have also been associated with lactose malabsorption including skin disease, rheumatological complaints, chronic fatigue, and failure to thrive in children, 15 although the concept of ‘systemic lactose intolerance’ is still controversial. It is important to realize that lactose malabsorption (lactase non-persistence) is not equivalent or synonymous to lactose intolerance. Lactose malabsorption in many cases will not come to clinical attention. Development of symptoms depends on several individual factors including diet, oro-cecal transit time, distribution and fermentation capacity of gut flora, 16 sensitivity towards chemical and mechanical stimulation of the gut, and psychological factors. 17
A recent NIH conference defined lactose intolerance as ‘the onset of gastrointestinal symptoms following a blinded, single-dose challenge of ingested lactose by an individual with lactose malabsorption, which are not observed when the person ingests an indistinguishable placebo’. 1 This new concept of lactose intolerance is provoking because it requires, in addition to evidence of lactase deficiency or lactose malabsorption, the development of symptoms after a blinded, placebo-controlled lactose challenge, which currently is not clinical practice.
Testing of lactose malabsorption
Typical symptoms of lactose intolerance are common among patients in a primary care setting but no consensus exists concerning which patients should be referred for further testing. In a recent meta-analysis, no specific complaint could predict lactose malabsorption, with sensitivities ranging from 0 to 90% and specificities ranging from 18 to 96% for symptoms such as bloating, diarrhoea, flatulence, and abdominal pain in individual studies. 18 Self-reported milk intolerance was also of little value, showing sensitivities from 30 to 71% and specificities from 25 to 87%. 18
Summary of tests for lactose malabsorption and tolerance
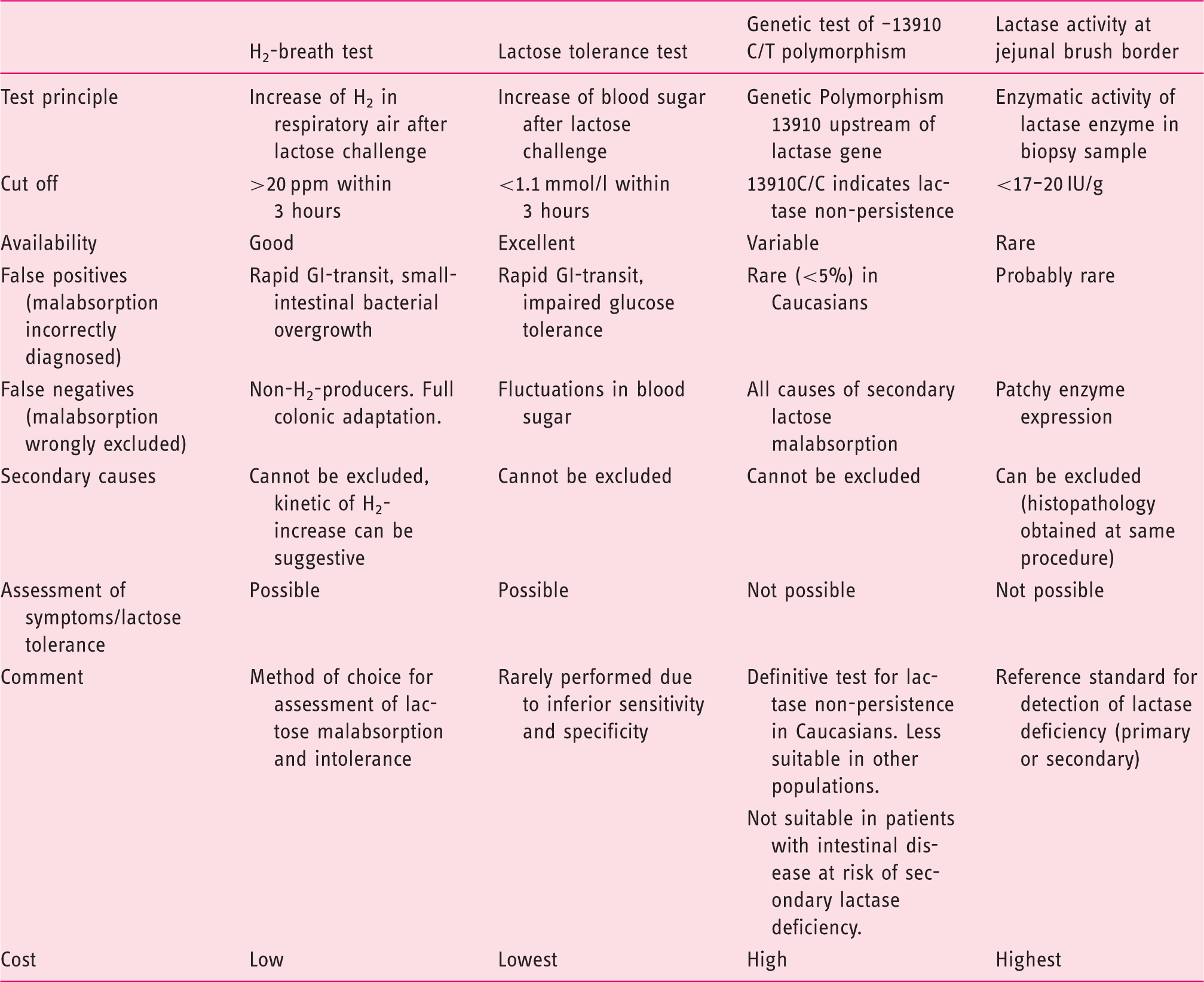
Genetic tests establish lactase non-persistence in Caucasian patients and the −13910*T genotype correlated closely (86–95%) with other tests for lactose malabsorption in European countries.6,23,24 Since lactose malabsorption is a recessive condition, a heterozygous genotype has to be considered a negative test result. Current testing for the −13910*T genotype is of limited use in certain African, Arabic, or Asian subpopulations where lactase persistence may be linked to different polymorphisms, as already discussed. Future genetic tests will likely cover a range of genetic polymorphisms, potentially eliminating this limitation. Clearly, genetic tests will be negative in patients with secondary causes of lactase deficiency. Importantly, no information about clinical symptoms lactose intolerance is obtained during testing.
Lactose digestion can also be assessed by the lactose tolerance test 25 and the H2-breath test.2,19,20 Both tests include an oral challenge with a standard dose of lactose (usually 20–50 g, corresponding to the lactose content of approximately 400–1000 ml cow milk). While the lactose tolerance test relies on an increase in blood glucose, the H2-breath test detects H2 produced by intestinal bacteria in expiratory air. The lactose tolerance test can be confounded by fluctuations of postprandial blood sugar in patients with impaired glucose tolerance or diabetes. The H2-breath test can be false-positive in the presence of small intestinal bacterial overgrowth. 26 False-negative results for the H2-breath are observed for ‘H2-non-producers’, the 2–43% of individuals (<10% in most studies) in whom the bowel flora does not produce hydrogen. 2 For these patients, test sensitivity can be improved by simultaneous measurement of methane. 2 A related cause of false-negative results in some individuals may be ‘full colonic adaptation’ to lactose ingestion, in which repeated intake of lactose selectively favours the growth of colonic flora that rapidly ferment lactose without producing hydrogen.27,28 Currently, the genetic test (in Caucasians) and the H2-breath test are widely used in clinical practice. Studies in Caucasian populations without gastrointestinal comorbidity report a high degree of agreement for diagnosis of lactose malabsorption between the H2-breath test, intestinal lactase level, and genetic tests.14,23,24,29
Assessment of lactose intolerance
The presence of lactose malabsorption is necessary but is not sufficient to establish lactose intake as the cause of patient symptoms. Lactose intolerance is defined by the occurrence of typical symptoms (i.e. nausea, bloating, diarrhoea, borborygmi, abdominal pain) during the H2-breath test procedure. However, interpretation of patient reports may be complicated by placebo responses.
Self-reported food intolerance is reported by a large proportion of the community in population-based studies, with frequency rates ranging from 9.5 to 25%30–32 and is even higher in patients with functional gastrointestinal diseases such as IBS.33,34 However, when subjected to controlled and blinded testing, only 25–40% of these patients react to the offending food.30,32 Similarly, an open label challenge with 240 ml of milk induced symptoms in 59% of patients with lactose malabsorption 35 but had no significant effects in a placebo-controlled challenge of subjects that self-reported severe lactose intolerance (indeed nine out of 30 patients did not have lactose malabsorption on breath testing). 36 These findings demonstrate a high frequency of placebo response to lactose in patients referred for investigation of digestive symptoms. Such a response might still impact on patient well being and could be referred to as ‘functional lactose intolerance’ (Box 1). These studies also demonstrate that blinded testing would increase the specificity of diagnosis and guide more rational dietary management of lactose intolerance. Double-blind placebo-controlled challenges for testing of food allergies has been criticized; 37 however, these arguments do not apply to lactose intolerance for which procedures can easily be standardized and anaphylactic reactions will not occur.
Blinded multiple dose testing for lactose intolerance
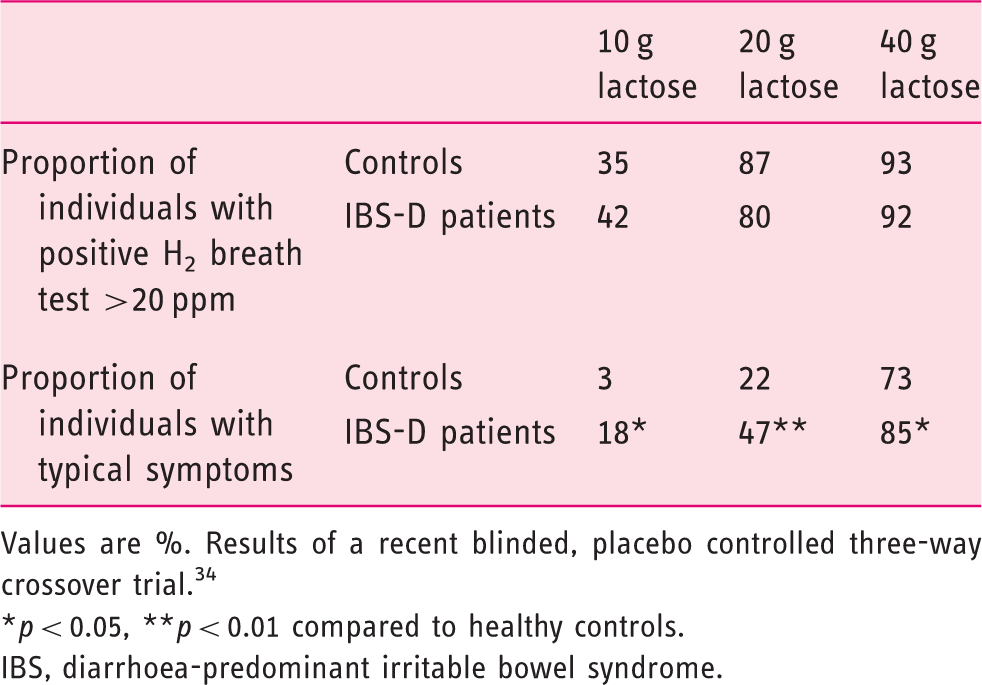
Values are %. Results of a recent blinded, placebo controlled three-way crossover trial. 34
p < 0.05, **p < 0.01 compared to healthy controls.
IBS, diarrhoea-predominant irritable bowel syndrome.
In current practice, lactose tolerance testing is performed as an open label procedure during the H2 breath test. The negative predictive value of these tests is high and lack of symptoms after a 40–50 g lactose challenge excludes lactose intolerance.38,39 In contrast, if symptoms develop, the possibility of a ‘placebo-response’ should not be ignored especially in patients without lactose malabsorption and those with functional gastrointestinal disease or self-reported food intolerance or allergies. Currently, placebo-controlled or multiple-dose testing is not performed outside research studies and would be difficult to implement in clinical practice. One solution to this practical issue would be, after confirming lactase deficiency in the laboratory, to perform blinded testing at multiple doses in the home environment. This approach could facilitate widespread implementation of appropriate dietary management rather than absolute exclusion of lactose intake. A diagnostic algorithm for lactose malabsorption and intolerance is provided in Figure 2.
Diagnostic algorithm for diagnosing lactose malabsorption and lactose intolerance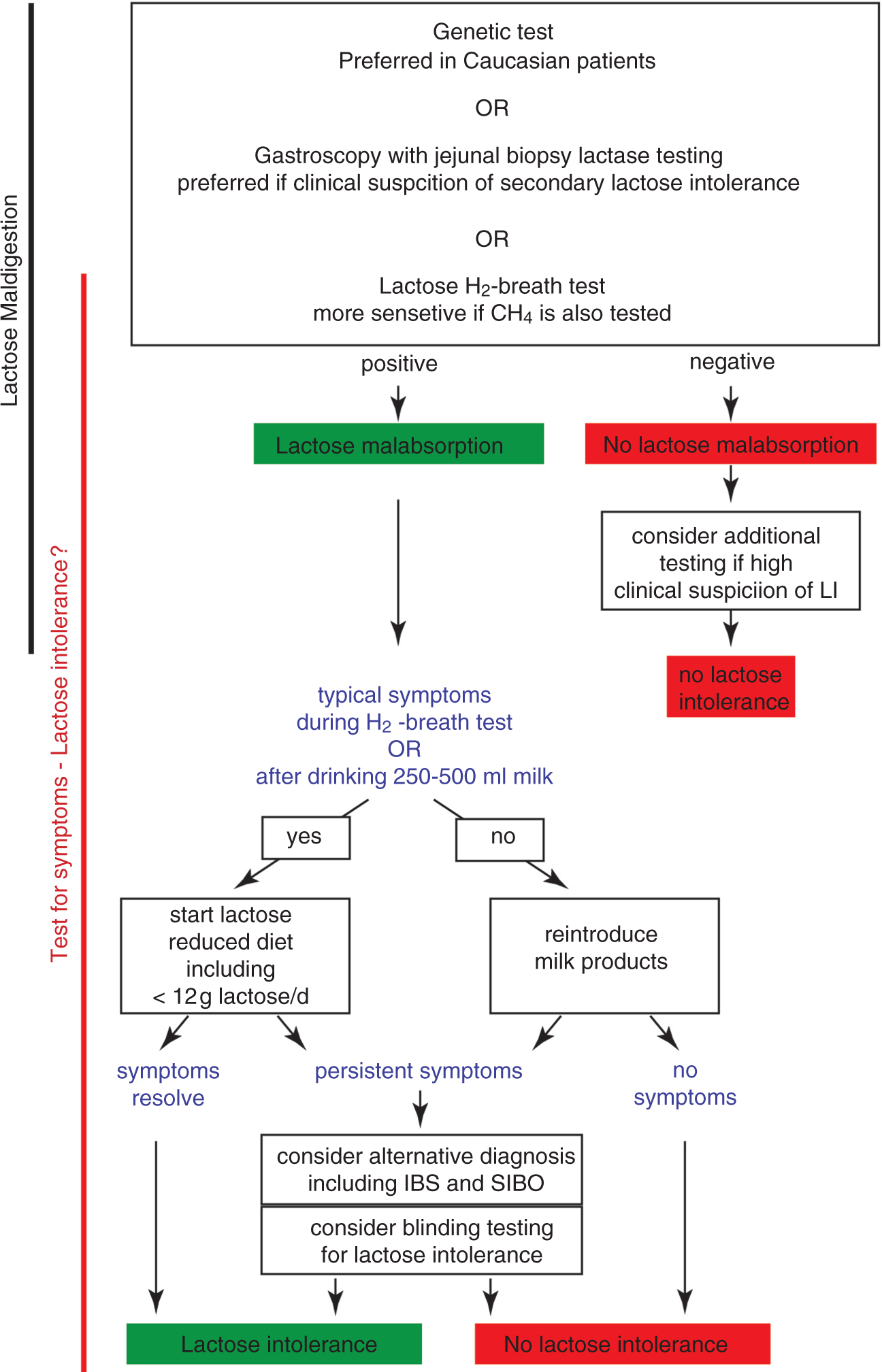
Treatment of lactose intolerance
Lactose and calcium content of different milk products
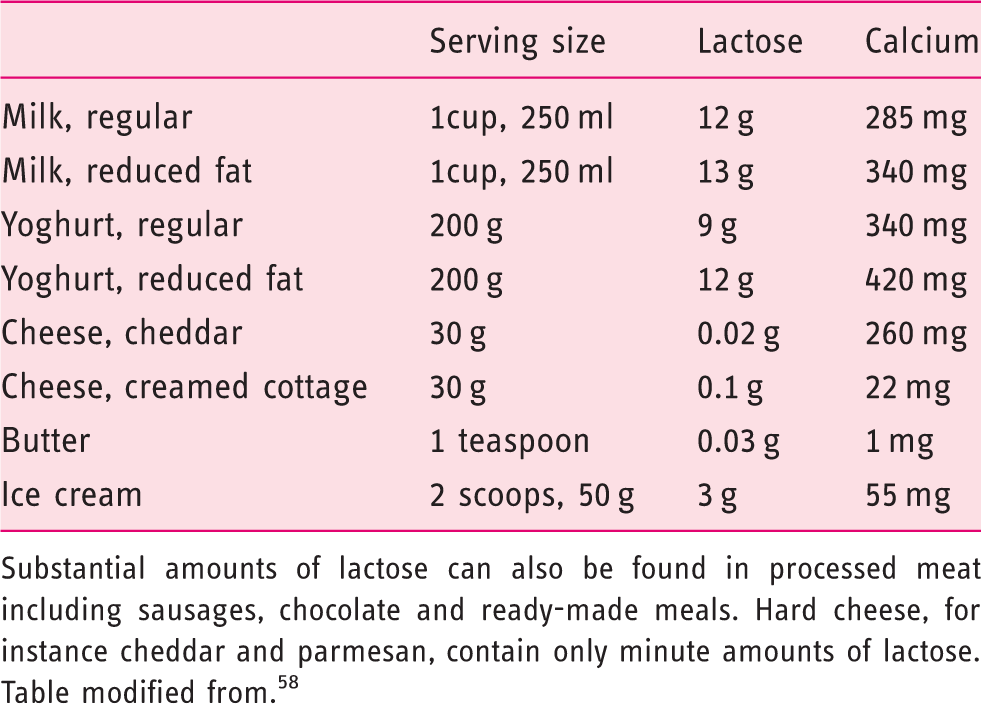
Substantial amounts of lactose can also be found in processed meat including sausages, chocolate and ready-made meals. Hard cheese, for instance cheddar and parmesan, contain only minute amounts of lactose. Table modified from. 58
Lactase enzyme replacement is another option although this changes the taste of the food when mixed with the dairy products because glucose and galactose produced by lactose digestion are sweeter than the original sugar. A variety of preparations are available over the counter but may not be equally effective. 49 Another strategy involves probiotics that alter the intestinal flora and may have beneficial effects in IBS patients that persist even after treatment. 50 Finally, although lactase expression is not upregulated by lactose ingestion, tolerance may be induced by repeated lactose dosing due to adaptation of the intestinal flora. 41 Further studies are required to provide high-quality evidence to support/compare the efficacy of these strategies. 41
In summary, restricting lactose intake is sensible treatment for lactose intolerance but patients should be reassured that absolute exclusion is unnecessary. If patients are unwilling to reduce milk intake, then lactase supplementation is appropriate. If typical abdominal symptoms persist despite these measures, then a trial of a diet low in FODMAPs may be more effective.
Long-term effects of lactose restriction
Although restricting dietary lactose may improve gastrointestinal complaints, long-term effects of a diet free of dairy products may be of concern. 51 Dairy products are the major source of calcium in many individuals (Table 3). Current guidelines suggest a daily calcium intake of 1000 mg per day for adults, 1300 mg for adolescents, and 1200 mg for people over 50 years. 52 Drinking three cups of milk per day has been recommended to obtain this amount. 52 It has been shown that adults and adolescents with a homozygous −13910*C genotype or self-reported milk intolerance consume less milk or lactose and less calcium than controls.51,53 There is also some evidence that a low intake of dairy products is associated with a higher risk of fractures in women, although much less so in men.51,54 Similarly, the −13910*C genotype was a risk factor for osteoporosis in some studies51,55,56 but not in others.51,57 No study has addressed the safety and effectiveness of calcium replacement for patients with lactose intolerance; however, it seems reasonable to recommend increasing calcium intake from other sources in patients that restrict intake of dairy products and to have a low threshold for calcium replacements in the presence of other risk factors for osteoporosis.
Conclusions
Progress has been made in our understanding of lactose malabsorption and intolerance. Sensitive and specific tests for lactase deficiency are now available. Diagnosis of lactose intolerance is less definitive as it requires concurrent assessment of lactose digestion and abdominal symptoms. Due to high rates of self-reported intolerance of dairy products and the fact that even patients with lactase deficiency can often tolerate up to 20 g lactose, such tests may be best performed as a series of blinded procedures at multiple doses. This approach provides information that can guide rational dietary management; however, the practical implementation of such testing is still unresolved. Once the optimal diagnostic method has been established, studies will be needed to assess the long-term outcome of dietary interventions.
Sources and selection criteria
We identified randomized controlled trials for diagnosis and treatment of lactose malabsorption and intolerance. This research had been done by an NIH evidence report 51 and others;18,41 however, high-quality, evidence-based guidelines were not available. We identified additional studies through Medline using search terms ‘lactose malabsorption’, ‘lactose maldigestion’, ‘lactose intolerance’, ‘intolerance AND dairy OR milk’, and also examined our own database for appropriate publications that tackle these issues.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.