
Abstract
Background and aims
Brushing cytology is useful for diagnosing biliary strictures. With regard to biliary stricture brushing at the distal common bile duct in the surrounding of the papilla, the risk of post-endoscopic retrograde cholangiopancreatography pancreatitis is unknown. Our study aimed to evaluate the risk of post-endoscopic retrograde cholangiopancreatography pancreatitis by using this procedure.
Methods
A total of 150 endoscopic retrograde cholangiopancreatography-naïve patients undergoing endoscopic retrograde cholangiopancreatography including biliary stricture brushing were retrospectively analyzed. Patients were divided into two groups: the surrounding of the papilla group (n = 25) and the other group (n = 125). The primary outcome was the post-endoscopic retrograde cholangiopancreatography pancreatitis incidence. We analyzed the risk of post-endoscopic retrograde cholangiopancreatography pancreatitis by using inverse probability of treatment weighting based on propensity scores to adjust for selection bias.
Results
The overall incidence of post-endoscopic retrograde cholangiopancreatography pancreatitis was 11.3%, and post-endoscopic retrograde cholangiopancreatography pancreatitis of the surrounding of the papilla group occurred significantly more frequently than in the other group (32.0% vs 7.2%, p < 0.01). Multivariate analysis showed that this procedure was a risk factor for post-endoscopic retrograde cholangiopancreatography pancreatitis (odds ratio, 10.6; 95% confidence interval, 2.82–40.2; p < 0.01). In the propensity-weighted model, this procedure was an independent risk factor for post-endoscopic retrograde cholangiopancreatography pancreatitis (odds ratio, 8.42; 95% confidence interval, 2.12–32.4; p < 0.01) by multivariate analysis.
Conclusions
Biliary stricture brushing at the distal common bile duct in the surrounding of the papilla may increase the risk of post-endoscopic retrograde cholangiopancreatography pancreatitis compared with brushing other portions.
Keywords
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is often used as a useful diagnostic and therapeutic tool for biliary tract diseases. Pathological evidence for biliary stricture is usually obtained from standard endoscopic trans-papillary tissue samplings, such as brush cytology and forceps biopsy. ERCP conducted for biliary drainage could easily incorporate biliary cytology. However, post-ERCP pancreatitis (PEP) remains one of the most common and serious adverse events. The risk factors of PEP are well investigated and generally divide into two groups: patient-related (sphincter of Oddi dysfunction, female sex, and previous pancreatitis) and procedure-related risk factors (cannulation attempt duration, pancreatic guidewire insertion, and pancreatic injection).1–4 Endoscopic papillary balloon dilation (EPBD) was also reported to be a procedure-related risk factor for PEP.5,6 EPBD and long duration of cannulation attempts have been reported to cause edema or pancreatic orifice spasm due to papilla stimulation; this may impair the outflow of pancreatic juice and eventually induce pancreatitis.1,5,7,8 We consider that biliary stricture brushing at the distal common bile duct in the surrounding of the papilla may be a risk factor for PEP, because it becomes a load for the papilla due to friction at the common channel of the papilla. However, few reports are available on the risk of PEP based on the use of biliary stricture brushing. We could not perform randomization of bile duct stricture brushing for each malignant stricture area, so we used the inverse probability of treatment weighting (IPTW) method based on the propensity score to create quasi-randomization. The aims of this study were to evaluate whether biliary stricture brushing at the distal common bile duct in the surrounding of the papilla increased the risk of PEP, and to identify the risk factors influencing PEP for patients with biliary stricture after quasi-randomization.
Methods
Patients
We retrospectively analyzed consecutive patients who had biliary stricture (caused by carcinoma of the bile duct, pancreatic cancer, metastasis, or invasive cancer of other portions, and inflammation) with naïve papilla undergoing therapeutic and diagnostic ERCP using biliary brushing at the Osaka City University Hospital between January 2009–June 2016. Exclusion criteria were as follows: history of ERCP, Billroth II gastrectomy, Roux-en-Y reconstruction, age younger than 20 years, biliary stricture caused by carcinoma of the papilla of Vater, or concomitant acute pancreatitis. This study was approved by the ethics committee at the Osaka City University Hospital.
Endoscopic examinations
All ERCP procedures were performed using a side-viewing duodenoscope (JF240, JF260V, TJF240, TJF260V; Olympus Optical Corporation, Tokyo, Japan) by a trainee with a career experience of less than 500 ERCP procedures or expert endoscopists. ERCP was performed under conscious sedation with intravenous injection of midazolam (3–10 mg) supplemented with pentazocine (15 mg) as needed. These sedative drugs were appropriately supplemented during the procedure. Prophylactic antibiotics and gabexate mesilate were administered to all patients for prevention of cholangitis and pancreatitis. After selective cannulation of the bile duct by using 0.035-inch or 0.025-inch guidewire (Hydra Jagwire; Boston Scientific, Marlborough, Massachusetts, USA or VisiGlide 2; Olympus), routine cholangiography using a cannula (MTW Endoskopie; Wesel, Germany) or sphincterotome (CleverCut3; Olympus), and intraductal ultrasound (US) if needed were performed. Subsequently, we performed brush cytology for the diagnosis of malignant biliary stricture. In addition, biliary biopsy was performed as needed. Biliary drainage using a drainage tube (Flexima Biliary 7Fr or 8.5Fr; Boston Scientific or Flexima Nasobiliary Catheter Kit 7.5Fr; Boston Scientific or QuickPlace V ENBD 6Fr; Olympus) was performed in the presence of obstructive jaundice. The total procedure time was defined as time from endoscope insertion to endoscope removal. The endoscopist decided which device was used during the procedure. All patients were hospitalized for at least 72 h after the procedure. Serum amylase levels were measured at 4 h and 24 h after ERCP. Abdominal computed tomography (CT) was performed if needed. Demographic, procedural, and follow-up data were recorded by research coordinator.
Cytology brushing
Biliary stricture brushing was performed using cytology brush (RX cytology brush; Boston Scientific or Howell Biliary Brush; Cook Medical, Bloomington, Indiana, USA) as follows. The cytology brush device was inserted along the guidewire above the biliary stricture and push out brush outer-sheath. The top of the outer-sheath below the biliary stricture was pulled while taking out the brush. The brush was vibrated at the biliary stricture 5–10 times.
Biliary stricture
We classified the patients who had biliary stricture into two groups according to the cholangiography images. The surrounding of the papilla group was defined by the distance from the distal end of the biliary stricture to the bottom end of the contrasting bile duct as less than 1 cm. The length of the brush was approximately 1 cm, so the cytology brush device reached the papilla at the brushing of the biliary stricture. This means brushing cytology may become a load for the papilla because of friction from the brush device. We diagnosed biliary stricture using CT or magnetic resonance imaging, and ERCP with pathological evidence obtained through brushing or biopsy.
Study endpoints and evaluation of post-ERCP pancreatitis
The main outcome of this study was the occurrence of PEP, including mild, moderate, and severe PEP. PEP was defined as a medical condition with abdominal pain persisting for at least 24 h after the procedure and high serum amylase levels (>360 IU/l) more than three times the upper normal limit at 4–24 h after the procedure. Elevation of serum amylase levels without abdominal pain was defined as post-ERCP hyperamylasemia. The severity of PEP was based on consensus criteria. 9 It was graded based on the duration of no food intake for PEP. Mild PEP required 2–3 days; moderate PEP required 4–10 days; and severe PEP required more than 10 days, necessitating surgical or intensive treatment, or contributing to death.
Statistical analysis
Categorical variables were compared using χ2 test or, when more appropriate, Fischer exact test. Continuous variables were compared using Mann-Whitney U-test. Univariate and multivariate logistic regression analyses were performed to identify factors associated with PEP. The model included age, sex, body mass index, American Society of Anesthesiologists (ASA) physical status (PS) classification, intake of nonsteroidal anti-inflammatory drugs (NSAIDs), pre-ERCP laboratory test involving C-reactive protein (CRP) and total bilirubin levels, underlying history, procedure time, time of cannulation in the bile duct, ERCP by trainees, biliary stricture brushing and biopsy, brushing portion, intraductal US, biliary stenting, pancreatic guidewire cannulation, pancreatic injection, and prophylactic pancreatic stenting. For each factor considered to have a potential association with PEP, the odds ratio (OR) with 95% confidence interval (95% CI) were calculated. Factors with p < 0.25 by univariate analysis and known risk factors of PEP (age, previous pancreatitis, time of cannulation in bile duct, pancreatic guidewire cannulation, and pancreatic injection) were further analyzed in the multivariate analysis. This study was a retrospective study and not a randomized controlled study because we could not control biliary stricture assignment. Thus, we used propensity scores to create quasi-randomization. The propensity score method including IPTW is used to balance baseline characteristics between two groups statistically to mimic a randomized controlled study. IPTW based on propensity scores can adjust for selection bias between two groups and reduced potential confounding effects in an observational study. Logistic regression was used to create propensity scores from the baseline characteristics. We used our clinical experience and knowledge to select possible confounders for their potential association with the outcomes as follows; age, sex, body mass index, pancreatic injection, ASA PS classification, intake NSAIDs, intraductal US, precut sphincterotomy, pancreatic stenting, pancreatic wire cannulation, trainee endoscopist, time of cannulation in the bile duct, underlying history of heart disease, and diabetes mellitus. Analyses involving propensity score-weighted linear regressions for PEP were performed. A two-sided p value less than 0.05 was considered to indicate statistical significance. All statistical analysis was performed by using R version 3.2.2 (The R foundation for Statistical Computing, Vienna, Austria) and SPSS version 23.0 (SPSS, Tokyo, Japan).
Results
Patients
Among 1996 ERCPs performed at the Osaka City University Hospital between January 2009–June 2016, 873 ERCPs were initial ERCP sessions. Among the 873 initial ERCPs, we excluded 35 ERCPs for pancreatic intervention and 221 enteroscopy-assisted ERCPs. Among 617 ERCPs for biliary intervention, we enrolled 150 initial therapeutic ERCPs that had biliary stricture and performed biliary stricture brushing in this study (Figure 1).
Flowchart of patients included in the study. ERCP: endoscopic retrograde cholangiopancreatography.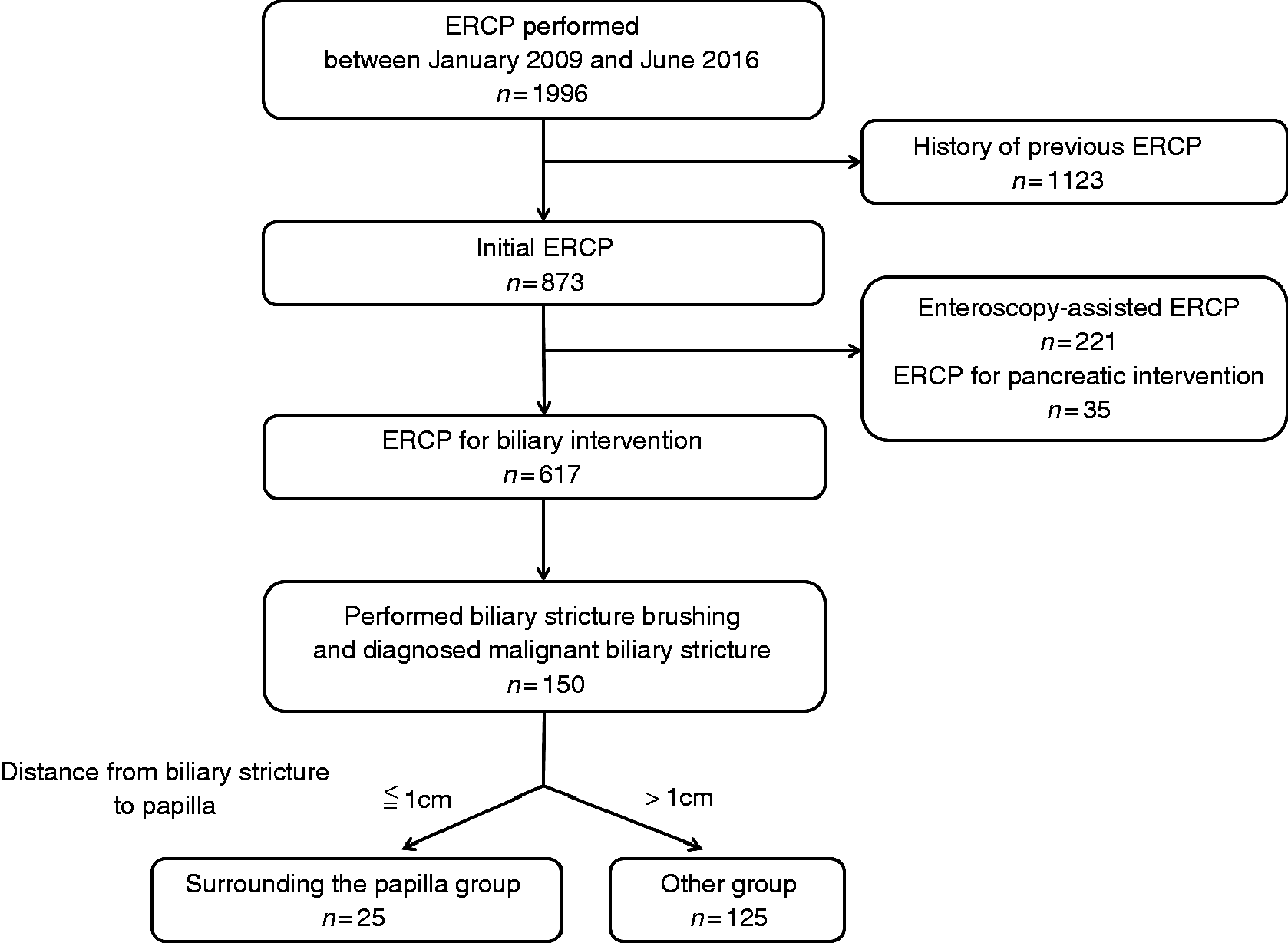
Baseline characteristic of patients in the two groups.
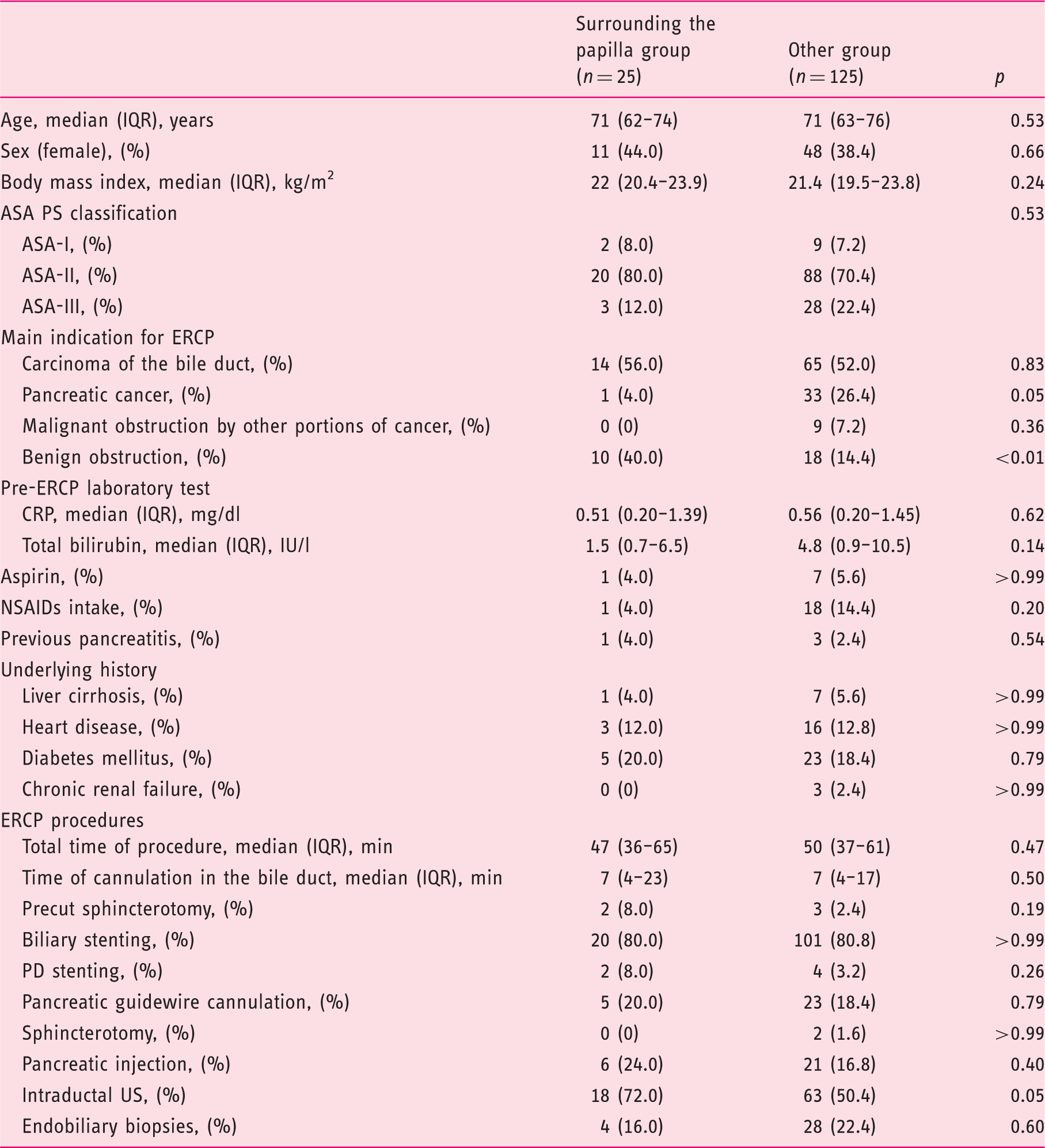
ASA: American Society of Anesthesiologists;CRP: C-reactive protein; ERCP: endoscopic retrograde cholangiopancreatography; IQR: inter-quartile range; NSAIDs: nonsteroidal anti-inflammatory drugs; PD: pancreatic duct; PS:physical status; US: ultrasound.
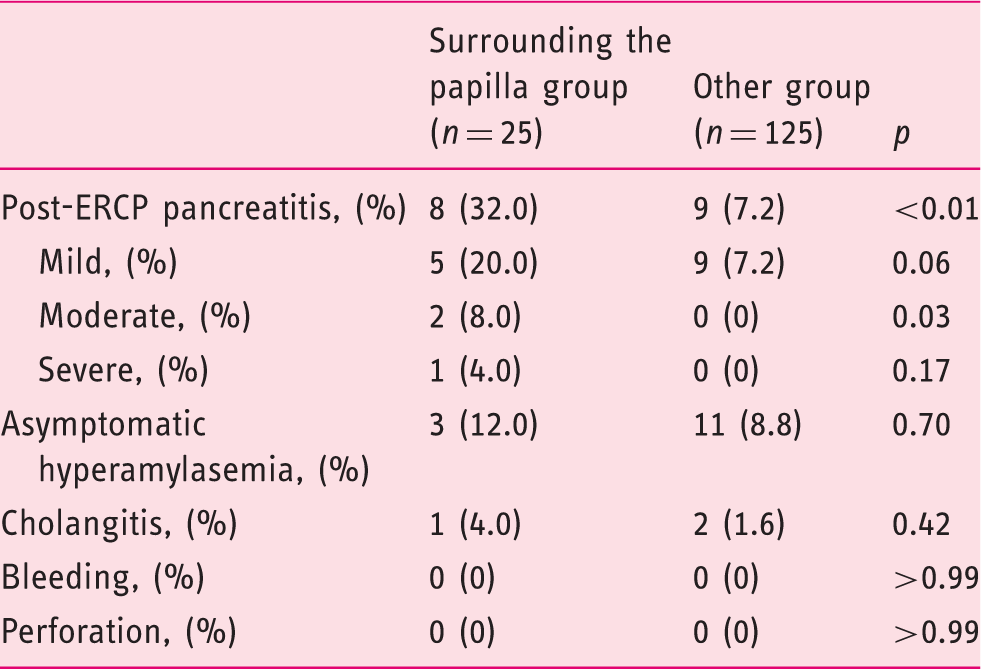
Outcome measures and other adverse events afterendoscopic retrograde cholangiopancreatography(ERCP) in the two groups.
Univariate and multivariate analyses of risk factors of post-endoscopic retrograde cholangiopancreatography pancreatitis (PEP).
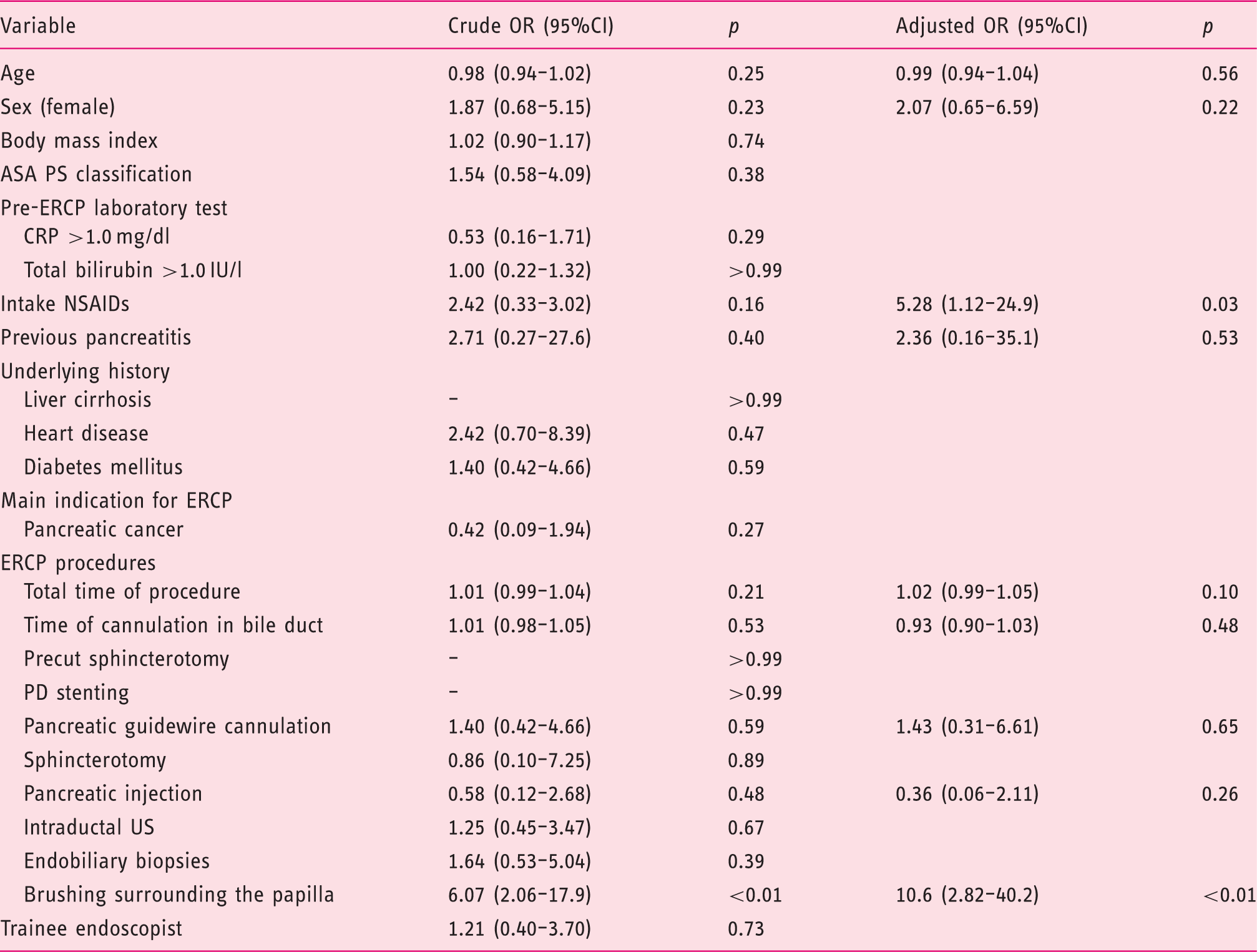
ASA: American Society of Anesthesiologists;CI: confidence interval; CRP: C-reactive protein; ERCP: endoscopic retrograde cholangiopancreatography; OR: odds ratio; PD: pancreatic duct; PS:physical status; US: ultrasound.
Propensity score weighted generalized estimating equation of risk of biliary stricture brushing surrounding the papilla.
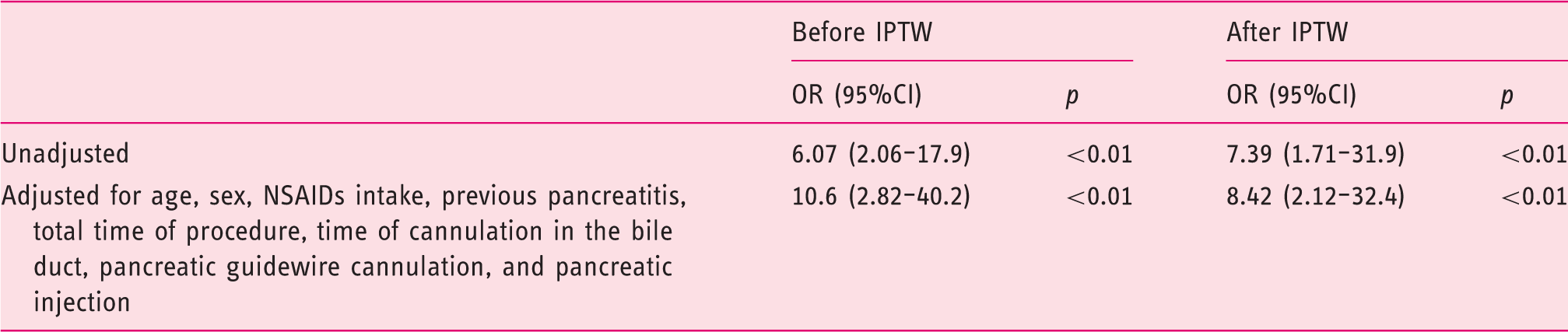
CI: confidence interval; IPTW: inverse probability of treatment weighting; NSAIDs: nonsteroidal anti-inflammatory drugs; OR: odds ratio.
Biliary stricture brushing
Patients were classified into two groups: 25 cases in the surrounding of the papilla group, and 125 cases in the other group. The baseline patient characteristics were compared between the two groups (Table 1). The incidence of benign obstruction in the surrounding of the papilla group was higher (p < 0.01) than that in the other group. However, the incidence of pancreatic cancer in the surrounding of the papilla group was lower (p = 0.05) than that in the other group. Other factors had no significant difference between two groups.
In malignant biliary stricture, the sensitivity in detecting malignant obstruction did not show a significant difference between two groups (surrounding of the papilla group was 40.0% (6/15) and the other group was 37.4% (40/107), p > 0.99).
PEP and asymptomatic hyperamylasemia
Adverse events after ERCP are shown in Table 2. PEP developed in 17 cases (11.3%). PEP was mild in 14 cases (9.3%), moderate in two cases (1.3%), severe in one case (0.7%). Asymptomatic hyperamylasemia was observed in 14 cases (9.3%). Bleeding and perforation were not observed. PEP in the surrounding the papilla group occurred significantly higher than other group (32.0% vs 7.2%, p < 0.01). Moreover, moderate and severe PEP occurred higher than in the other group (12.0% vs 0%, p < 0.01). No significant differences in the rate of asymptomatic hyperamylasemia were observed between the surrounding the papilla and the other group (12.0% vs 8.8%, p = 0.70).
Univariate and multivariate analyses for risk factors of PEP are shown in Table 3. Brushing the surrounding the papilla was an independent risk factor for PEP based on univariate (p < 0.01) and multivariate analyses (OR, 10.6; 95% CI, 2.82–40.2; p < 0.01).
Other factors, including age, sex, pancreatic injection, and pancreatic wire cannulation, were not significantly related to PEP.
Evaluation using IPTW
We can create a quasi-randomized study by using the propensity score. The confounding factors in the two groups seem to have no differences after IPTW. The propensity-weighted model was well calibrated (Hosmer Lemeshow test, p = 0.25). Using generalized estimating equations, brushing the surrounding of the papilla was the risk factor for PEP (OR, 7.39; 95% CI, 1.71–31.9; p < 0.01). In addition, by multivariate analysis adjusted for age, sex, NSAIDs intake, previous pancreatitis, total time of the procedure, time of the cannulation in the bile duct, pancreatic guidewire cannulation, and pancreatic injection, brushing the surrounding of the papilla was a risk factor for PEP (OR, 8.42; 95% CI, 2.12–32.4; p < 0.01) (Table 4).
Discussion
The results of our study indicated that biliary stricture brushing at the distal common bile duct in the surrounding of the papilla increased the risk of PEP compared with brushing other portions. This also increased the risk of moderate and severe PEP. There were no prospective randomization studies for biliary stricture brushing, and it was difficult to randomize bile duct stricture brushing for each biliary stricture area. Hence, we performed a new attempt of creating quasi-randomization using the IPTW method by propensity score because bias from confounding variables was minimized. 10 We could clarify the robustness that biliary stricture brushing at the distal common bile duct in the surrounding of the papilla was an independent risk factor of PEP.
Acute pancreatitis remains the most common and serious adverse event after ERCP with reported incidence ranging from 1–15% in most prospective studies.7,8,11–13 In our study, PEP occurred in 11.3% of procedures, similar to previous reports. In contrast, PEP occurred at a high rate (32%) when brushing the distal common bile duct. The risk factor of PEP has been reported in many prospective reports;1,2 however, only few previous studies have reported that biliary stricture brushing was a risk factor of PEP. The multivariate analysis identified only biliary stricture brushing at the distal common bile duct in the surrounding of the papilla as an independent risk factor of PEP. We speculated the reason why biliary brushing stimulated the papilla orifice as well as EPBD or many cannulation attempts. Compartment syndrome from post-EPBD hemorrhage or edema and an uncut sphincter of Oddi have been reported as the mechanism of pancreatitis. 14 The sphincter of Oddi is composed of three distinct parts, the sphincter choledochus, the sphincter pancreaticus, and the outermost sphincter ampullae, which wraps around the distal end of the bile and pancreatic ducts or the common channel. 15 Biliary stricture brushing at the distal common bile duct in the surrounding of the papilla may limit volume expansion of the sphincter of Oddi, and worsening compression of the pancreatic orifice from brushing edema. Obstruction of the pancreatic orifice may impair the outflow of pancreatic juice and eventually induce pancreatitis. The higher the pancreatic intraductal pressure is, the higher the risk of the severity of PEP. 16 In this study, moderate and severe PEP in the surrounding of the papilla group occurred significantly more frequently than in the other group; the reason might be that edema of the pancreatic orifice by brushing caused high pancreatic intraductal pressure. Another reason could be direct injury of the pancreatic duct as brushing possibly damaged the common channel and pancreatic duct of the papillary region by vibration of the brush without direct vision. Both PEP and asymptomatic hyperamylasemia have been reported to occur because of injury to the pancreatic tissue induced by ERCP techniques, and asymptomatic hyperamylasemia was associated with mild injury of pancreas without an inflammatory response. 17 In this study, the rate of asymptomatic hyperamylasemia was not different among the two groups, but PEP in the surrounding of the papilla group occurred significantly more frequently than in the other group. This might indicate that all ERCP procedures damaged the pancreatic duct mildly, but brushing at the distal common bile duct in the surrounding of the papilla damaged the pancreatic duct to a greater extent.
Age was known to be an important risk factor for PEP.3,13,18,19 In this study, age was not a risk factor for PEP. This could be explained by the higher mean age (median, 71 years) of the population in this study. Pancreatic injection was also a related risk factor of PEP,12,20,21 which was not significantly related to PEP in this study. The degree of contrast agent injection into the pancreatic duct was varied in this study; which might be underestimated because we recorded pancreatic injection even if only a slight amount of contrast agent was injected into the pancreatic duct.
In this study, endoscopic sphincterotomy was not performed in the surrounding of the papilla group, despite benign biliary obstruction being present in 40% of the patients in this group. The reason was that all ERCP procedures were initial ERCP, and we could not determine whether the biliary stricture was malignant without pathological evidence. The European Society of Gastrointestinal Endoscopy’s guidelines recommend placing a plastic stent for biliary drainage if a diagnosis of the biliary obstruction is still not ascertained. 22 It has been reported that a biliary stent can be deployed without the need for biliary sphincterotomy. 23
We usually could not estimate whether biliary stricture was malignant by only using endoscopic retrograde cholangiography imaging without pathological evidence. Thus, endoscopic transpapillary bile duct brushing or biopsy was performed for diagnosing biliary stricture. We found that the sensitivity in detecting malignant biliary stricture on using brushing cytology (40.0%) at the distal common bile duct in the surrounding of the papilla was equal to that seen in previous reports (30–48%),24–26 but brushing was a risk factor for PEP. In contrast, the usefulness of repeated cytological sampling of bile obtained via endoscopic nasobiliary drainage (ENBD) tube was reported.27,28 The sensitivity for detection of malignant biliary stricture on using brush cytology was only 30–48%, but that seen on performing repeated cytological sampling of bile obtained via the ENBD tube sensitivity was 55–75%.27,29 However, several problems were noted. First, knowing how often ENBD cytology should be repeated is difficult. Second, the ENBD tube often causes discomfort in patients. Endoscopic ultrasound-guided fine needle aspiration for the ampulla of Vater has been reported to be safe and accurately performed. 30 We may consider these methods instead of the usual biliary stricture brushing for diagnosing malignant biliary stricture at the distal common bile duct.
This study had several limitations. First, this study was a retrospective study design in a single center and not a randomized study. So, we created quasi-randomization by using the IPTW method based on propensity scores. However, when we created the propensity scores, it is possible that our selected confounding factors were not sufficient and we did not reduce any selection bias adequately. This study was a single-center study; hence, multiple endoscopists, including trainees, were involved. Thus, the results could be more generalized than studies that were performed by a single endoscopist. Finally, the number of cases was relatively small. Further research with a multicenter study may overcome this limitation.
In conclusion, we found that biliary stricture brushing at the distal common bile duct in the surrounding of the papilla increased the risk of PEP compared with brushing other portions.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.