
Abstract
Background and Aims
Endoscopic mucosal resection is an effective and safe procedure to manage large non-pedunculated colonic polyps for which residual/recurrent adenoma is the main drawback. Size/Morphology/Site/Access score determines polypectomy difficulty. We aimed to describe residual/recurrent adenoma rate according to Size/Morphology/Site/Access and to select the ize/Morphology/Site/Access cut-off to predict low residual/recurrent adenoma.
Methods
This was a retrospective cohort study of endoscopic mucosal resection for large non-pedunculated colonic polyps performed in a tertiary centre.
Results
Three hundred and sixteen procedures were included. The mean size of lesions was 34.5 ± 17.1 mm, 59.5% were sessile, 60.4% were in the right colon and in 17.7% (n = 56) the access was difficult. Of the lesions, 83.6% were Size/Morphology/Site/Access 3–4. Residual/recurrent adenoma at first and second follow-up was significantly lower in Size/Morphology/Site/Access 2 (1.9% and 0.0%, respectively) when compared to Size/Morphology/Site/Access 3 (18.2%, p = 0.004 and 6.7%, p = 0.049) and Size/Morphology/Site/Access 4 (30.8%, p < 0.001 and 22.7%, p = 0.030). The negative predictive value of Size/Morphology/Site/Access 2 for residual/recurrent adenoma at second follow-up was 86.1%. On multivariate analyses, Size/Morphology/Site/Access 3–4 predicted residual/recurrent adenoma at first (odds ratio 11.96, 95% confidence interval 1.57–91.13) and second follow-up (odds ratio 2.47, 95% confidence interval 1.51–4.22) and had higher cumulative incidence of residual/recurrent adenoma compared to Size/Morphology/Site/Access 2 (p ≤ 0.003).
Conclusion
Use of the Size/Morphology/Site/Access score allows cases to be identified with a low risk of residual/recurrent adenoma.
Key summary
Endoscopic mucosal resection (EMR) is an effective, safe and relatively cheap way to manage large non-pedunculated colonic polyps. Incomplete resection and residual/recurrent adenoma (RRA) is the main limitation of EMR. The use of the Size/Morphology/Site/Access (SMSA) scoring system is recommended to define complexity of polypectomy. SMSA 2 lesions (vs SMSA 3–4) have lower RRA1 and RRA2 and lower cumulative incidence of residual/recurrent adenoma. SMSA 3–4 independently predicts residual/recurrent adenoma.
Introduction
With the increasing number of colonoscopies due to bowel screening programmes, the number of identified colonic polyps has increased. 1 Large (>20 mm), flat or sessile lesions (large non-pedunculated colonic polyps (LNPCPs)) can be challenging to resect endoscopically. Most are removed by endoscopic piecemeal mucosal resection, whilst some require endoscopic submucosal dissection. 2 While the former procedure is associated with an increased risk of incomplete excision, the later has a high complication rate and is resource-intensive both in terms of time needed for the procedure and direct cost of the equipment. 3 Indeed, endoscopic mucosal resection (EMR) is an effective, cheaper and safer way of managing LNPCPs both compared with endoscopic submucosal disssection (ESD) and with surgery.4–6 Residual and/or recurrent adenoma (RRA) is the main drawback of this technique. In most cases an early follow-up within the first six months is indicated.2,7 After the early follow-up, a second one-year follow-up before entering the regular post-polypectomy surveillance has also been recommended to exclude late recurrence.3,6,8 This is obviously associated with an increase in colonoscopy burden and associated costs and risks. Although the reported RRA rates might be as high as 50%, the RRA is successfully managed endoscopically in up to 93.1% of cases.6,8
Size/Morphology/Site/Access (SMSA) score.
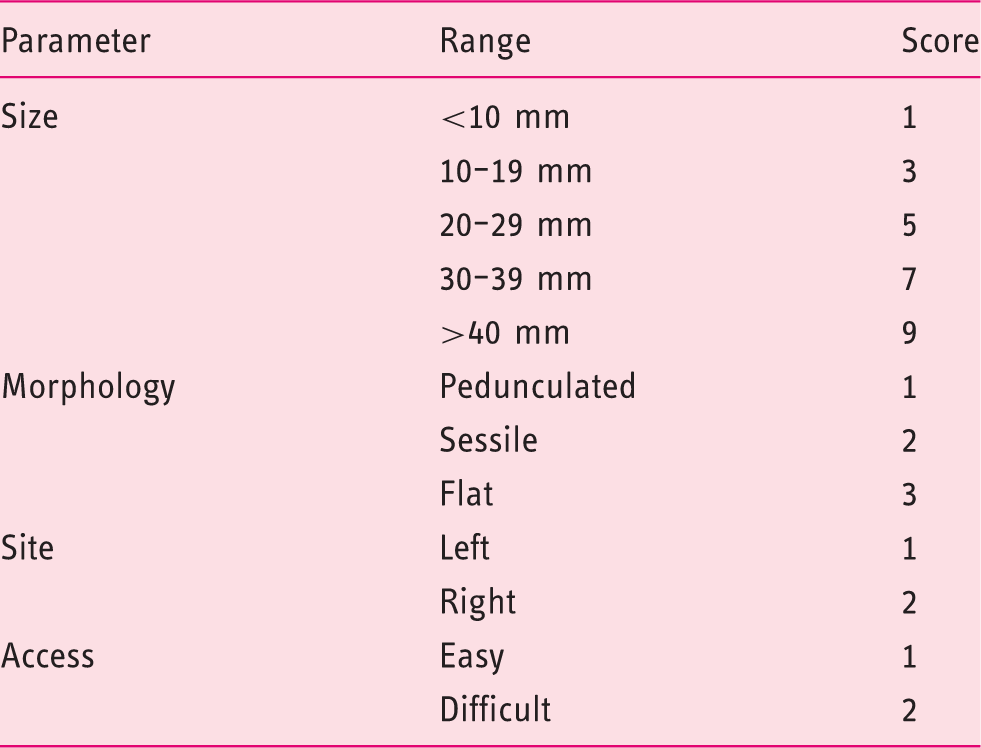
SMSA grade 1: 4–5 points, grade 2: 6–8 points, grade 3: 9–12, grade 4: > 12 points
We aimed to (a) describe the RRA according to SMSA score in a cohort of patients with LNPCPs and to (b) identify the best SMSA score cut-off to predict low RRA.
Methods
Study design
This was a retrospective cohort study of patients submitted to EMR for LNPCPs in a tertiary referral centre between January 2010–May 2016.
Patients
We included all adult patients with at least one year of follow-up referred for EMR of LNPCPs. Patients with familial syndromes (namely Lynch syndrome, familial adenomatous polyposis – classic or attenuated, MUTYH-associated polyposis, Peutz–Jeghers syndrome, juvenile polyposis syndrome or serrated polyposis syndrome), lesions in inflamed/previously inflamed mucosa in the context of inflammatory bowel disease (IBD) and patients without a follow-up colonoscopy in our centre were excluded.
All colorectal lesions were assessed using high resolution colonoscopies (GIF H260, GIF-HQ290, CF H260D, and CF-HQ290 – Olympus Medical Systems Corporation, Tokyo, Japan) and narrow band imaging (NBI) and/or conventional chromoendoscopy with indigo carmine solution were used as per protocol. EMR was performed by experienced endoscopists (including expert EMR endoscopist, nurse endoscopist and surgeons) or by an endoscopy fellow under the supervision of the advanced endoscopist. Lesions were lifted with submucosal injection of a solution of succinylated gelatin, indigo carmine and diluted adrenalin. Diathermy was performed using blended current (Endocut Q, effect 2-3, electrosurgical unit ERBE VIO 300D, Elektromedizin, Tubingen, Germany). When used, sedation was given in a combination of fentanyl, midazolam and/or nitrous oxide. After EMR of LNPCPs, a follow-up procedure was planned for the next 3–6 months and a second follow-up within one year after the first follow-up. Being a tertiary referral centre, a local follow-up was allowed for patients referred from the farthest centres, owing to the difficulty in travelling, old age, and to avoid any inconvenience to the patients.
This study protocol follows the Declaration of Helsinki, was approved by local ethic committee (Leeds Teaching Hospitals Trust clinical ethics committee) and the requirement for individual informed consent was waived.
Data collection
Demographic, clinical, endoscopic and histological data were collected from the clinical files of each patient. RRA was defined as any adenoma found at the place of or at the identified scar of previous EMR. When endoscopic features were not clear biopsies were taken and RRA was considered if the histology showed adenoma. Late recurrence was defined as the presence of a lesion found at the place of or at the identified scar of previous EMR during the second follow-up procedure when there was no RRA in the first follow-up. RRA1 and RRA2 were defined as the presence of RRA in the first and second follow-up procedure after EMR, respectively. Intraprocedural bleeding (IPB) was defined as bleeding requiring further endoscopic treatment such as using tip of the snare, coagulation forceps, adrenalin injection and/or clips to control the bleeding. If endoscopic treatment was unsuccessful surgical or radiological approach was considered as per protocol. The SMSA score was applied retrospectively: size was determined by the endoscopist at the time of LNPCP assessment; morphology was classified according to endoscopist description as Paris classification (0–Is: sessile, 0–II: flat) and lateral spreading tumours were also included as flat lesions; lesions were classified as right colon when localised proximally to the splenic flexure; difficult access was considered whenever the endoscopist reported the position for EMR as difficult or polyps hidden on the proximal side of a colonic fold, involving anorectal junction, appendix orifice or ileocaecal valve were found. Advanced adenomas were defined as adenomas with villous histology or high grade dysplasia/adenocarcinoma. When considering adenocarcinoma arising in adenomas (malignant polyps) the following histological criteria were considered unfavourable: lesions extending deeper than Kikuchi sm1 or 1000 µm into the submucosa, with poor differentiation, lymphovascular invasion, piecemeal resection of the adenocarcinoma and/or resection margins of < 1 mm.
Statistical analysis
Statistical analysis was performed using SPSS software version 21 (SPSS, Chicago, Illinois, USA). Normality was assessed using the Kolmogorov–Smirnov test. Mean and standard deviation or median and interquartile range (IQR) were used for continuous variables. Frequencies were used for categorical variables. Continuous variables were compared using Student’s t-test or Mann–Whitney test, and Chi-square test or Fisher test were used for categorical variables.
The performance of size in predicting RRA was analysed calculating the area under the receiver operating characteristics (AUROC) curves from which the best cut-off was selected by the Youden index test using the MedCalc software version 12.5 (MedCalc Software, Mariakerke, Belgium).
The significant predictors from the initial univariate analysis were selected for multivariate analysis. Collinearity diagnosis was performed on these predictors before entering the multivariate binary logistic regression model. The selected predictor of RRA was then tested using Kaplan–Meier survival curves. A p-value < 0.05 was considered statistically significant.
Results
A total of 701 patients were screened, of whom 316 were finally enrolled. Of the patients excluded, 242 did not have a follow-up colonoscopy in our centre or were lost to follow-up, 111 underwent surgery following the endoscopic resection, 23 had lesions in colonic IBD, five had familial syndromes, and four died of other conditions before the first follow-up – Figure 1.
Study enrolment flow diagram. EMR: endoscopic mucosal resection; NLS: non-lifting sign.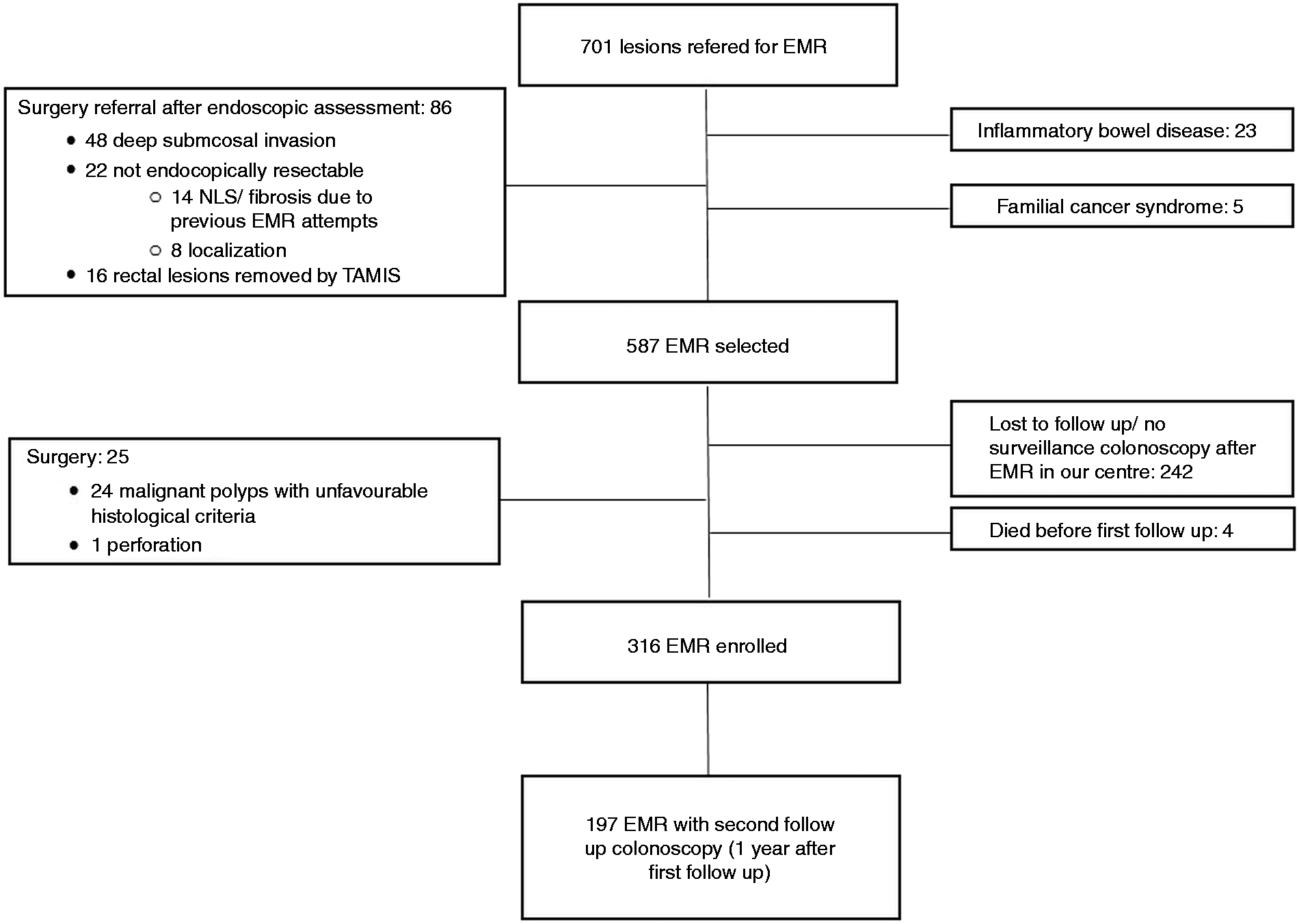
Baseline characteristics of included patients and lesions.
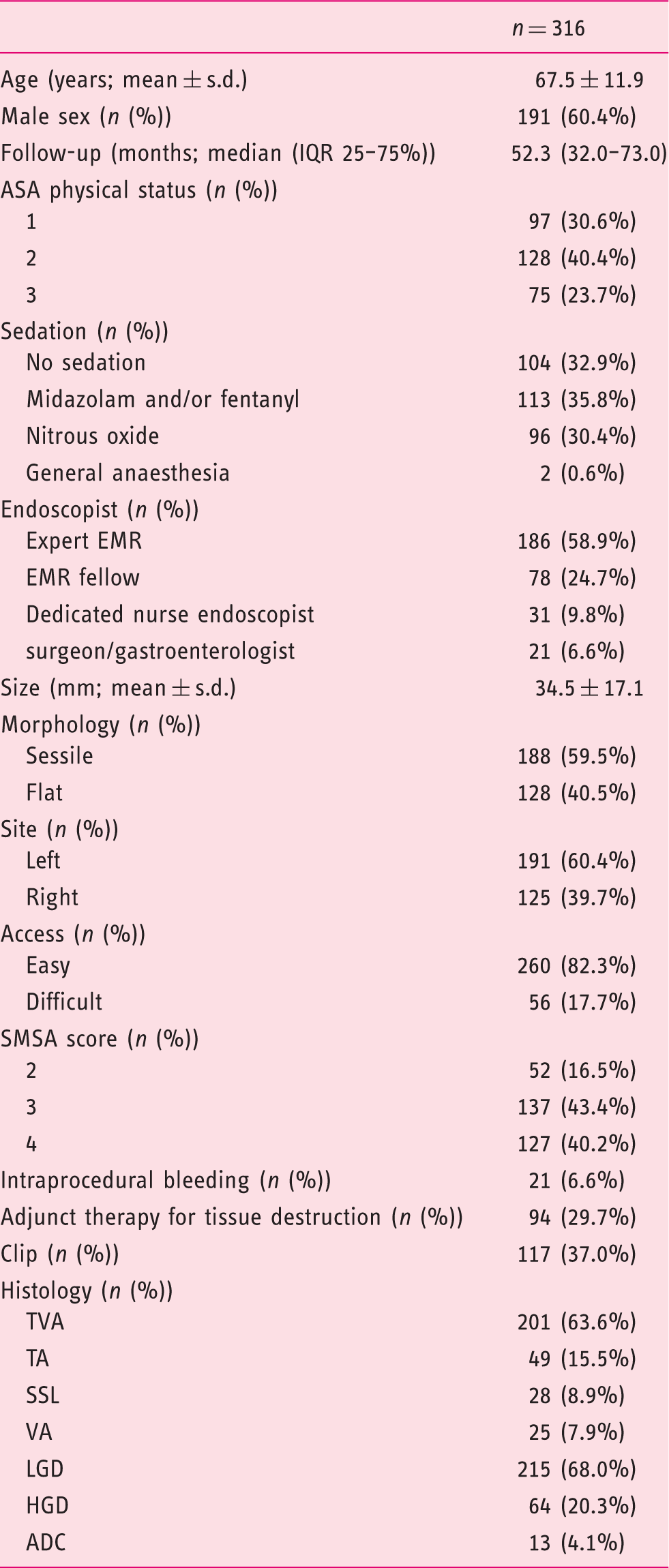
ADC: adenocarcinoma; ASA physical status: American Society of Anesthesiologists physical status classification system; EMR: endoscopic mucosal resection; HGD: high grade dysplasia; IQR: interquartile range; LGD: low grade dysplasia; s.d.: standard deviation; SMSA: Size/Morphology/Site/Access; SSL: sessile serrated lesion; TA: tubular adenoma; TVA: tubulovillous adenoma; VA: villous adenoma.
Residual and/or recurrent adenoma (RRA) according to Size/Morphology/Site/Access (SMSA).
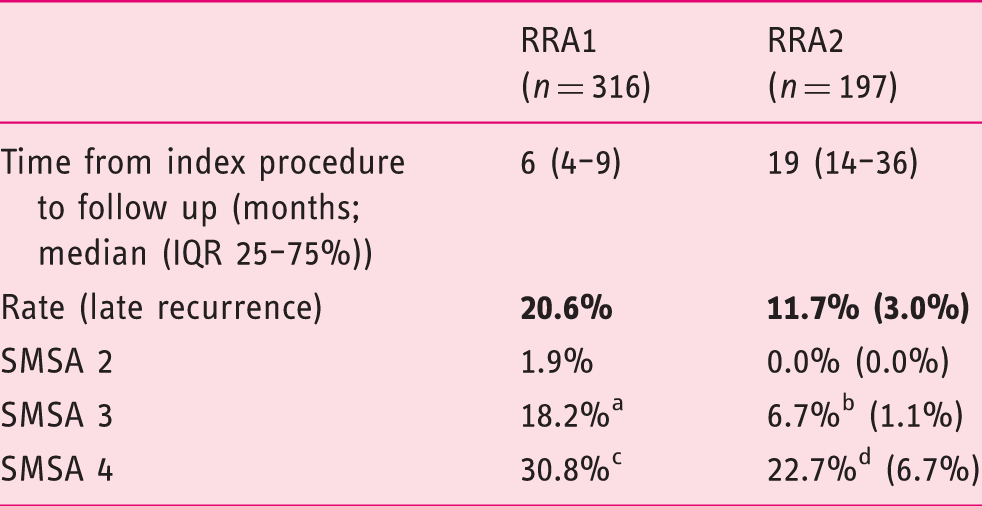
IQR: interquartile range.
SMSA 2 vs SMSA 3 p = 0.004; bSMSA 2 vs SMSA 3 p = 0.049; cSMSA 2 vs SMSA 4 p < 0.001; dSMSA 2 vs SMSA 4 p = 0.030.
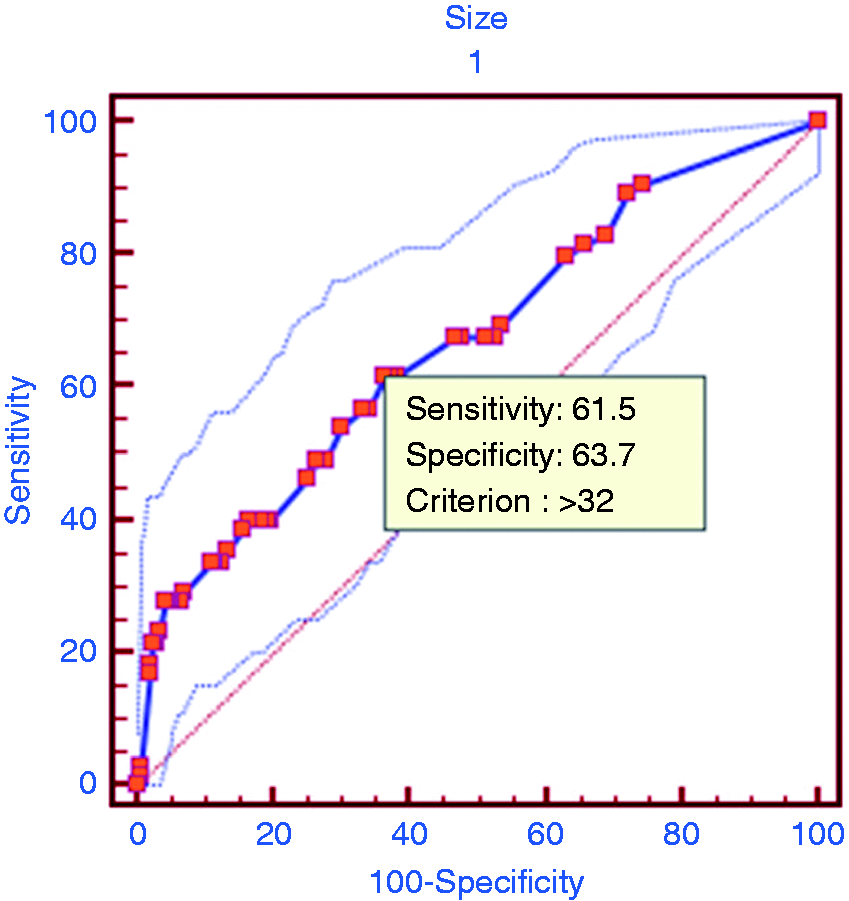
Area under the receiver-operating characteristics (AUROC) curve of size in predicting residual and/or recurrent adenoma (RRA).
IPB occurred in 6.6% of the cases (n = 21) and was controlled endoscopically in all cases. Adjunct therapy was used in 29.7% of the cases (n = 94), mainly argon plasma coagulation (APC). Clips were applied in 37.0% of the cases (n = 117), including 15 IPB cases – Table 2.
Histologically, adenocarcinoma arising from within the polyp was found in 13 (4.1%) cases, 25 (7.9%) were villous adenomas and 28 (8.9%) sessile serrated lesions. High-grade dysplasia was found in 20.3% of the LNPCPs removed – Table 2.
Predictors of residual and/or recurrent adenoma (RRA)1.
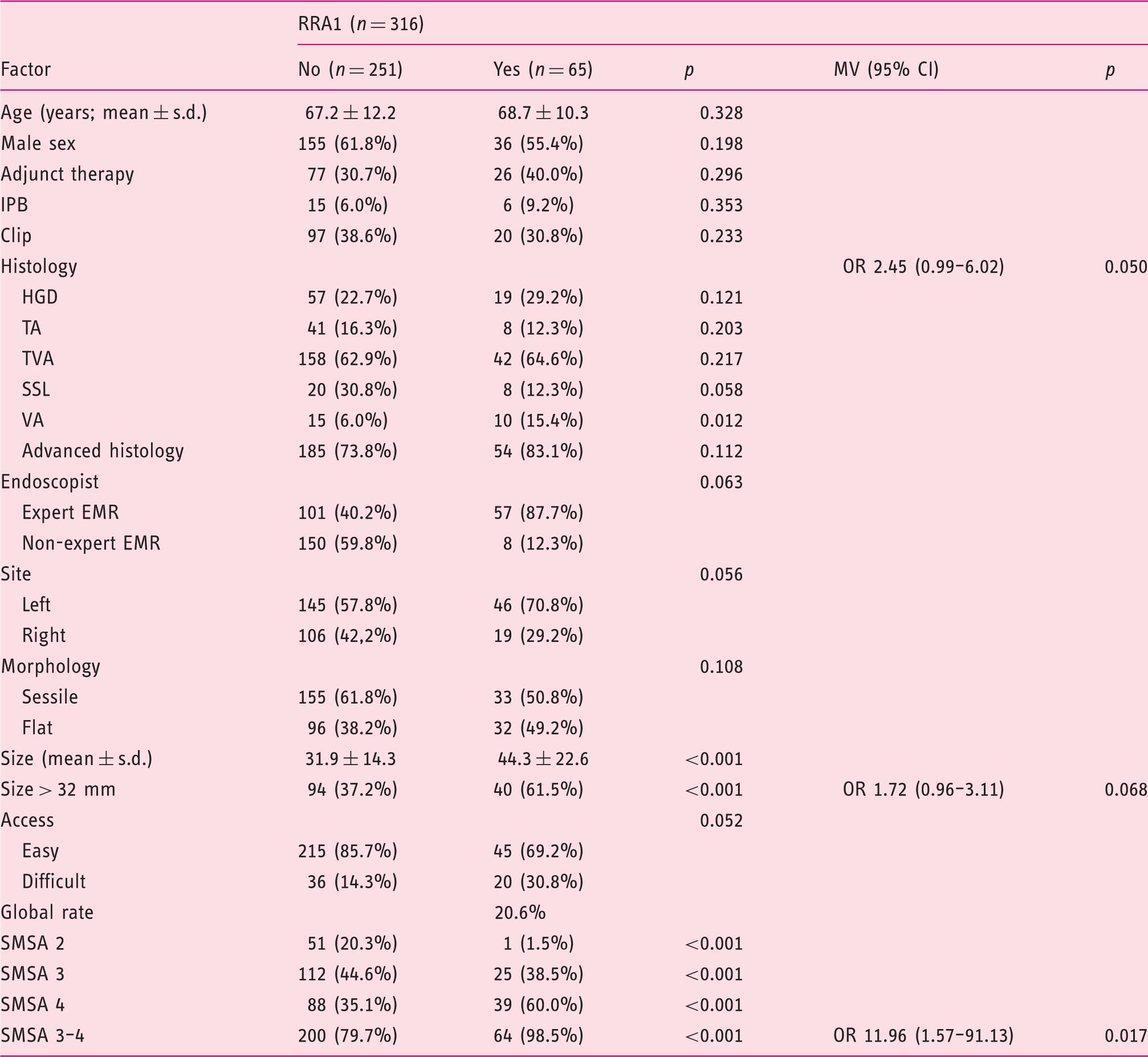
MV: multivariate analysis; CI: confidence interval; EMR: endoscopic mucosal resection; HGD: high grade dysplasia; IPB: intraprocedural bleeding; OR: odds ratio; s.d.: standard deviation; SMSA: Size/Morphology/Site/Access; SSL: sessile serrated lesion; TA: tubular adenoma; TVA: tubulovillous adenoma; VA: villous adenoma.
After collinearity diagnosis, significant predictors not at risk of collinearity entered multivariate modelling.
One hundred and ninety-seven patients had a second follow-up procedure in our institution, within a median time of 19 months (IQR 25–7%5: 14–36) after the index procedure. RRA2 was found at the second follow-up procedure in 23 cases (11.7%) and late recurrence was seen in six cases (3.0%). RRA2 was also significantly less likely in SMSA 2 lesions when compared with SMSA 3 and 4 (0.0% vs 6.7%, p = 0.049 vs 22.7%, p = 0.030, respectively) – Table 3.
Predictors of residual and/or recurrent adenoma (RRA)2.
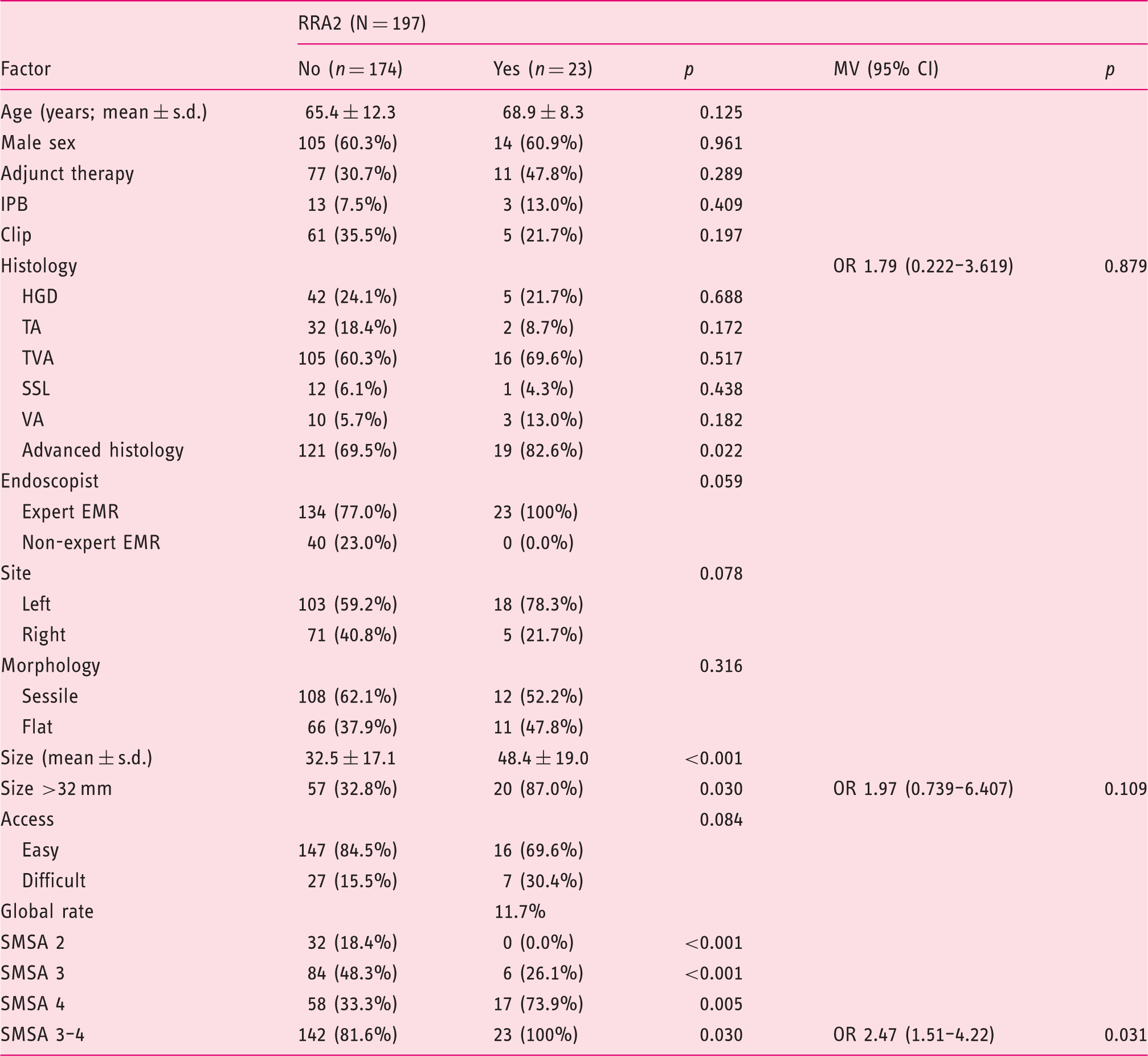
MV: multivariate analysis; CI: confidence interval; EMR: endoscopic mucosal resection; HGD: high grade dysplasia; IPB: intraprocedural bleeding; s.d.: standard deviation; SMSA: Size/Morphology/Site/Access; SSL: sessile serrated lesion; TA: tubular adenoma; TVA: tubulovillous adenoma; VA: villous adenoma.
After collinearity diagnosis, significant predictors not at risk of collinearity entered multivariate modelling.
On multivariate analysis, only having a SMSA 3–4 remained predictive of RRA, with an odds ratio (OR) of 11.96 to predict RRA1 and OR 2.47 to predict RRA2 – Tables 4 and 5.
Kaplan–Meier survival curves describe the cumulative incidence of RRA to longest follow-up according to the SMSA score (SMSA 2 vs SMSA 3–4) – Figure 3. These two types of lesion clearly behave differently, with a significantly lower cumulative incidence of RRA for SMSA 2 lesions (log rank, Breslow and Tarone–Ware ≤ 0.003).
Kaplan–Meier curves for cumulative incidence of residual and/or recurrent adenoma (RRA) according to Size/Morphology/Site/Access (SMSA) grade (2 vs 3–4).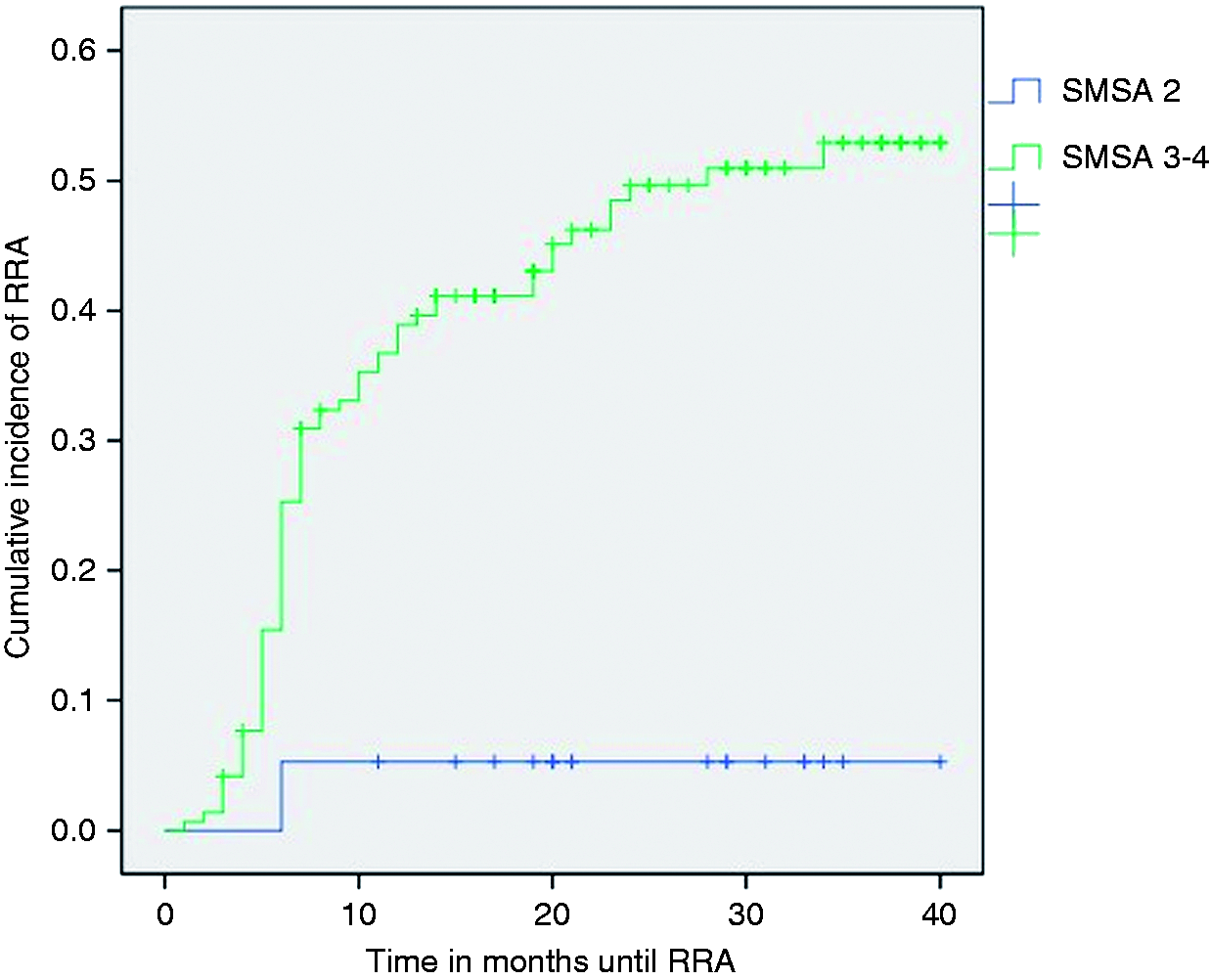
Discussion
The SMSA scoring system was described to grade difficulties in polypectomy. 9 It is a user-friendly classification that takes account of most described risk predictors and has been shown to correlate with outcomes such as complication and endoscopic clearance rates.6,9,11–13 European guidelines recommend that complex polyps are referred to an expert centre.2,10 Our study confirms the utility of the SMSA score to predict relevant outcomes. In fact, RRA1 and RRA2 were significantly lower in LNPCPs classified as SMSA grade 2 when compared to lesions at SMSA 3–4. Furthermore, SMSA was the only independent predictive factor for RRA that remained significant after multivariate analysis, emphasising the value of conjugation of balanced factors over the use of a single factor. 11 Also noteworthy is the fact that LNPCPs graded as SMSA 2 presented a high negative predictive value for RRA2 with high specificity. No late recurrences were found in these patients (as opposed to SMSA 3–4). The clear distinction between a high and a low risk group is confirmed by Kaplan–Meier survival curves, where statistically significant differences are maintained over time. These findings suggest that SMSA not only has implications in planning the index procedure (allocating to adequate centres and experienced EMR endoscopists), but also on the decision of the most appropriate follow-up. LNPCP SMSA grade 2 may not require a one-year follow-up after the first assessment at 3–6 months, as long as it is not recommended for other reasons. Our conclusions obviously have impacts on costs, workload of endoscopy units and patients’ quality of life.
The use of APC to ablate small residual tissue not amenable to snare resection was not associated with higher RRA. Also, the occurrence of IPB was not associated with higher risk of RRA. 14 It is worth noting that, on univariate analysis, villous histology was a predictor of RRA, with a trend towards significance in multivariate analysis for prediction of RRA1. Size is one of the most important and well-described characteristics determining outcomes and difficulty of polypectomy.6,13,14 Our study corroborated this finding. Indeed, several studies have demonstrated this relationship and proposed different cut-offs to define worse outcomes.13,14 Using the area under the ROC curve of size to predict RRA, we defined a statistically defined cut-off at 32 mm which can be used to reliably predict higher RRA rates.
One of the limitations of our study was its retrospective design and being conducted in a single centre. As with any tertiary centre experience, a vast number of patients were allowed local follow-up after the initial EMR. Needless to say this had significant impact on the timing of the scheduled follow-up procedures. However, this may reflect the day-to-day reality of endoscopy units and it is worth noting that the median time for the first and second follow-up was within that which was planned (median six and 19 months after index procedure, respectively). Although the retrospective grading of SMSA scores may not be as accurate; size, site and morphology criteria are prospectively described and difficult access definition was refined by adding previously described factors associated with difficult EMR.6,15–17 This was a single tertiary centre study including LNPCPs removed by more than one operator. This may be seen as a limitation to the applicability of our conclusions. However, the EMR of LNPCPs should preferably be referred to specialised centres and reflects the reality in which these recommendations are applied.
Conclusion
SMSA score can also be used to predict RRA by categorising LNPCPs as high (SMSA 3–4) and low (SMSA 2) RRA risk. Given the low cumulative incidence of RRA among patients with SMSA2 lesions, a routine endoscopic check at 12 months may not be needed.
Footnotes
Acknowledgements
Author contributions were as follows: RB designed the study, acquired and interpreted the data and drafted the manuscript; NM and BR designed the study, interpreted the data, drafted the manuscript and critically reviewed the manuscript for important intellectual content. All authors approved the submitted manuscript.
Declaration of conflicting interests
The authors declare no conflicts of interest.
Ethics
This study was approved by local health research ethics boards and the requirement for individual informed consent was waived.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
See above Ethics statement.