
Abstract
Background
Endoscopic full thickness resection (EFTR) by the Full Thickness Resection Device (FTRD) has recently been introduced as a method to allow resection of certain lesions such as adenomatous polyps that would not be resectable by standard polypectomy techniques. We report our clinical experience with FTRD procedures, assessing technical success, completeness of resection (R0 status), rate of histologically proven FTR and safety.
Patients and methods
We conducted a retrospective analysis of 33 consecutive patients with colonic polyps treated with FTRD from May 2015 to November 2016.
Results
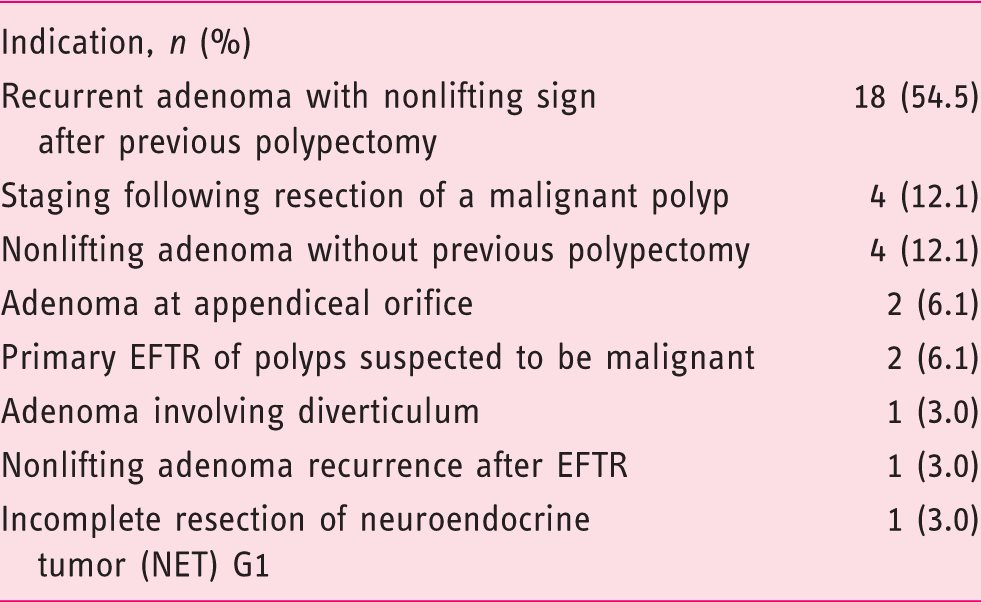
Indications mainly were adenoma recurrence or residual adenoma with nonlifting sign after previous polypectomy. In the 31 cases amenable to EFTR, resection was en bloc and histologically complete (R0) in 87.9% (29/33) of patients. Histologically confirmed complete full thickness resection (FTR) was achieved in 80.6% (25/31). Three post-procedure bleedings and one perforation were seen.
Conclusion
FTRD offers an additional endoscopic approach to treat nonlifting colorectal lesions. EFTR by FTRD appears to be feasible and efficacious in the resection of benign neoplasms of up to 30 mm in diameter and may be an alternative to surgery in selected patients. Given a significant rate of complications, safety is a concern and needs to be assessed in larger prospective studies.
Keywords
Key summary
Introduction
Removal of colorectal adenomas prevents cancer and reduces colorectal cancer mortality by up to 50%. Thus the detection and resection of all adenomas is one of the key goals of colonoscopy. 1
Various resection techniques are available to interventional endoscopists. Pedunculated lesions are easily resectable with snare polypectomy, whereas the resection of flat and sessile lesions may be challenging. Such lesions can be removed by endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD). Nowadays both of these methods are well studied and established in clinical practice, particularly for the resection of large sessile colorectal lesions.2–8
The technique of EMR occasionally requires large sessile polyps to be removed in a piecemeal fashion. The drawback of this technique is a recurrence rate of greater than 20%. Incomplete resection, however, contributes to the risk of developing interval cancers.8,9
ESD yields a higher rate of en bloc R0 resections as compared to EMR but is associated with a higher complication rate (perforations up to 14%, bleeding up to 22%). Furthermore ESD is more time consuming and requires a high level of expertise.10–14
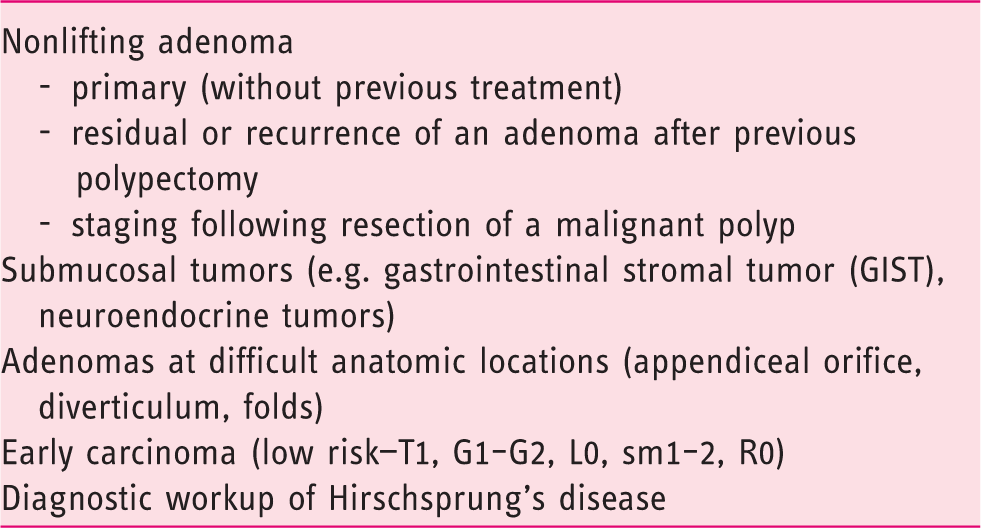
Not all adenomatous lesions in the gastrointestinal tract are amenable to EMR or ESD. In particular nonlifting lesions may pose a problem to EMR and ESD. In most instances, the nonlifting sign is a secondary phenomenon due to fibrosis and scaring following previous polypectomy; less frequently it is classified as primary. Further examples of polyps difficult to resect by conventional techniques are lesions at difficult anatomical locations such as the appendiceal orifice, colonic diverticula or behind folds. Such resections carry a high risk of complications, particularly perforation. 2
General indications for endoscopic full thickness resection (EFTR).
In Europe, the Full Thickness Resection Device (FTRD, Ovesco, Tübingen, Germany) was introduced into clinical practice in September 2014. FTRD is an over-the-scope device designed for one-step colonic EFTR (Figure 1). It is used for flexible EFTR in the colon as well as in the rectum. This report describes the clinical experience in two tertiary referral centers in Switzerland using FTRD to resect difficult colorectal lesions that would otherwise have had to be treated surgically.
Schematic illustration of an endoscopic full thickness resection (EFTR) by Full Thickness Resection Device (FTRD) (www.ovesco.com).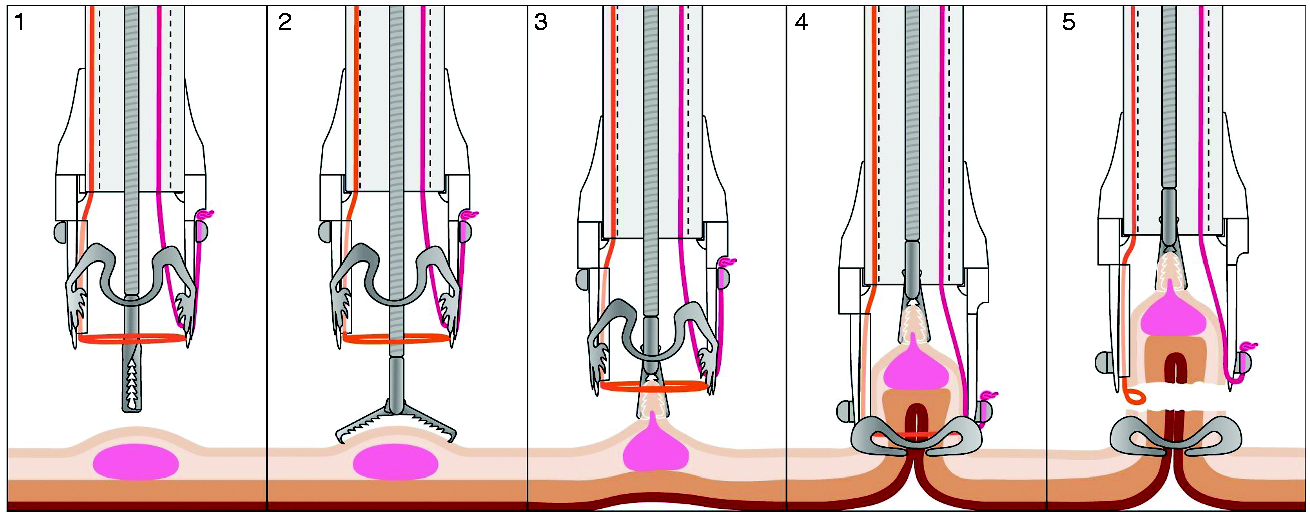
Patients and methods
This is a retrospective study from two tertiary referral centers in Switzerland (Luzerner Kantonsspital, Lucerne and Kantonsspital St. Gallen, St. Gallen), which was performed in accordance with the 1975 Declaration of Helsinki, good clinical practice and all applicable regulatory requirements. The study was approved by Swiss Ethics (Project-ID 2016-01238 17/098) July 25, 2016.
From May 2015 through November 2016, 33 consecutive patients undergoing EFTR by FTRD were included. EFTR was offered to patients as an experimental but less-invasive alternative to surgical resection after written informed consent was obtained from all patients prior to endoscopic procedures. Treatment outcome parameters (target lesion reached, target lesion resected, R0 resection and full thickness resection (FTR) as proven by histology, mean diameter of resected specimens), technical success, procedure time and adverse events were recorded and analyzed.
Description of the FTRD device
The FTRD is a pre-assembled over-the-scope device. It consists of a transparent cap with a modified, preloaded 14-mm over-the-scope clip (OTSC) and an integrated monofilament 13-mm polypectomy snare at its distal end. Compared to the classical OTSC the clip used in the FTRD has additional lateral teeth in order to ensure a safe closure of the defect before resection. The FTRD cap is longer compared to the standard OTSC (23 mm vs 6 mm) and thus accommodates a tissue volume of approximately 3 cm3. This allows the capture of lesions of up to 30 mm in diameter. The snare itself runs along the outside of the scope covered by a plastic sheath. The working channel is exclusively used for the grasper to catch the lesion and to pull it into the cap before clipping and resecting. The system is easily mounted over the tip of a standard colonoscope (diameter 11.5–13.2 mm), similar to variceal band ligation systems or OTSCs.
The FTRD has a Conformité Européenne mark and has been commercially available since September 2014 throughout Europe but not yet in the United States.
Description of the EFTR procedure
All our patients provided written informed consent before the EFTR procedure and received prophylactic antibiotic therapy. Blood tests were obtained to check for coagulopathy. All interventions were performed by three interventional endoscopists. Procedures were performed under propofol conscious sedation. Blood pressure and oxygen saturation were constantly monitored during the procedure.
As a first step the target lesion was identified using a standard colonoscope (diameter 11.5–13.2 mm) without mounted FTRD system.
The lateral margins of the lesion were marked using the marking probe that is part of the set. Then the endoscope was retrieved and reintroduced after mounting the FTRD, until the target lesion was reached again. The lesion was seized with the grasping forceps and pulled into the cap, until the circumferential markings were visible. Then the preloaded clip was released, thus creating a pseudopolyp that could be resected with the snare integrated in the system.
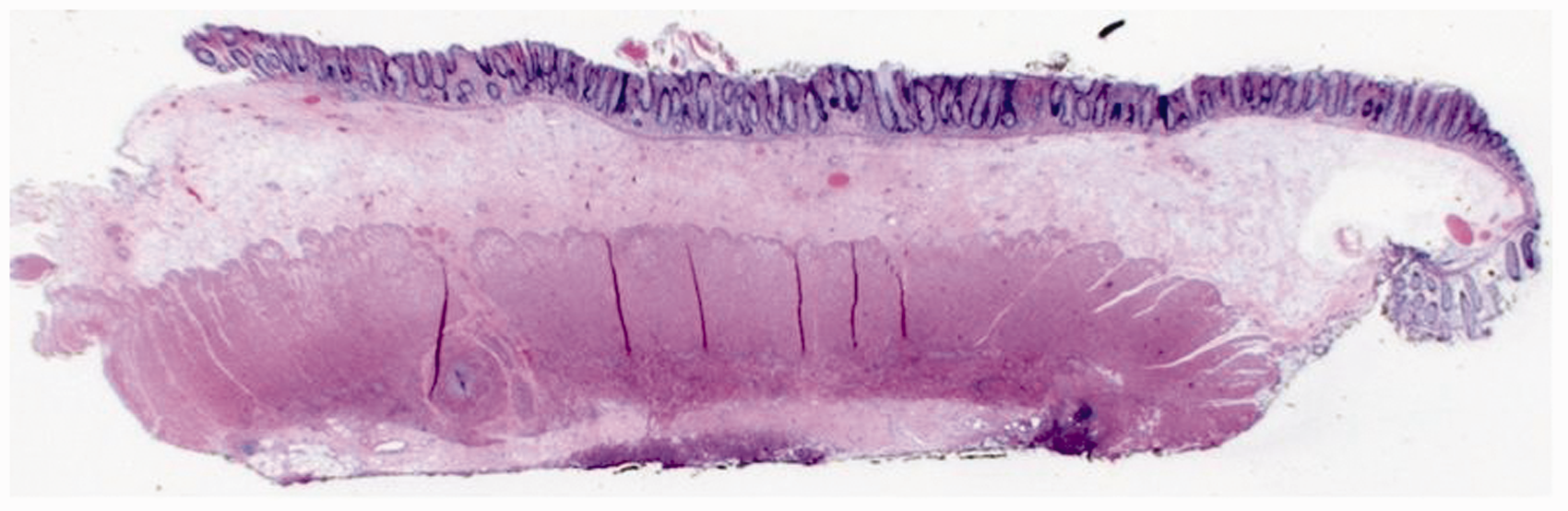
After resection the endoscope is extracted with the resection specimen harbored in the cap. Finally the colonoscope was inserted a third time for inspection of the resection site (Figure 2). All specimens were sent to pathology (Figure 3). Patients were hospitalized for one to two nights post-intervention and were monitored for signs of complications, in particular bleeding or perforation. Blood tests or imaging (abdominal X-ray or computed tomography (CT) scan) were performed as needed according to the clinical course.
Resection site after endoscopic full thickness resection (EFTR) with Full Thickness Resection Device (FTRD). Histology of a full thickness resection specimen showing all four layers (mucosa, submucosa, muscle layer, serosa).
Patients were started on clear liquids three to four hours after the procedure if there were no signs of peritonitis. A normal diet was started the following morning.
Follow-up
Follow-up colonoscopy was scheduled according to histological findings in the resection specimen.
Results
Patients’ characteristics and indications for EFTR
Indications for endoscopic full thickness resection (EFTR) in present series.
Resection site characteristics.
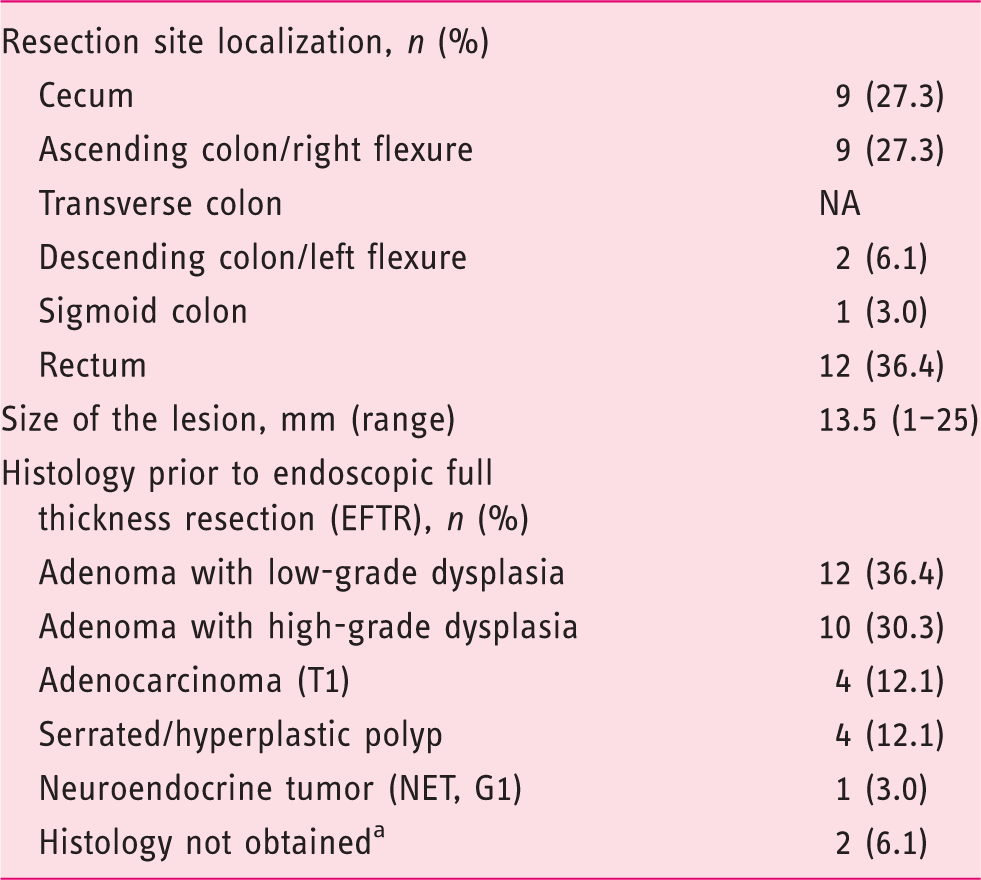
One adenoma with nonlifting sign without previous polypectomy and one neoplasm suspected to be malignant.
Results.
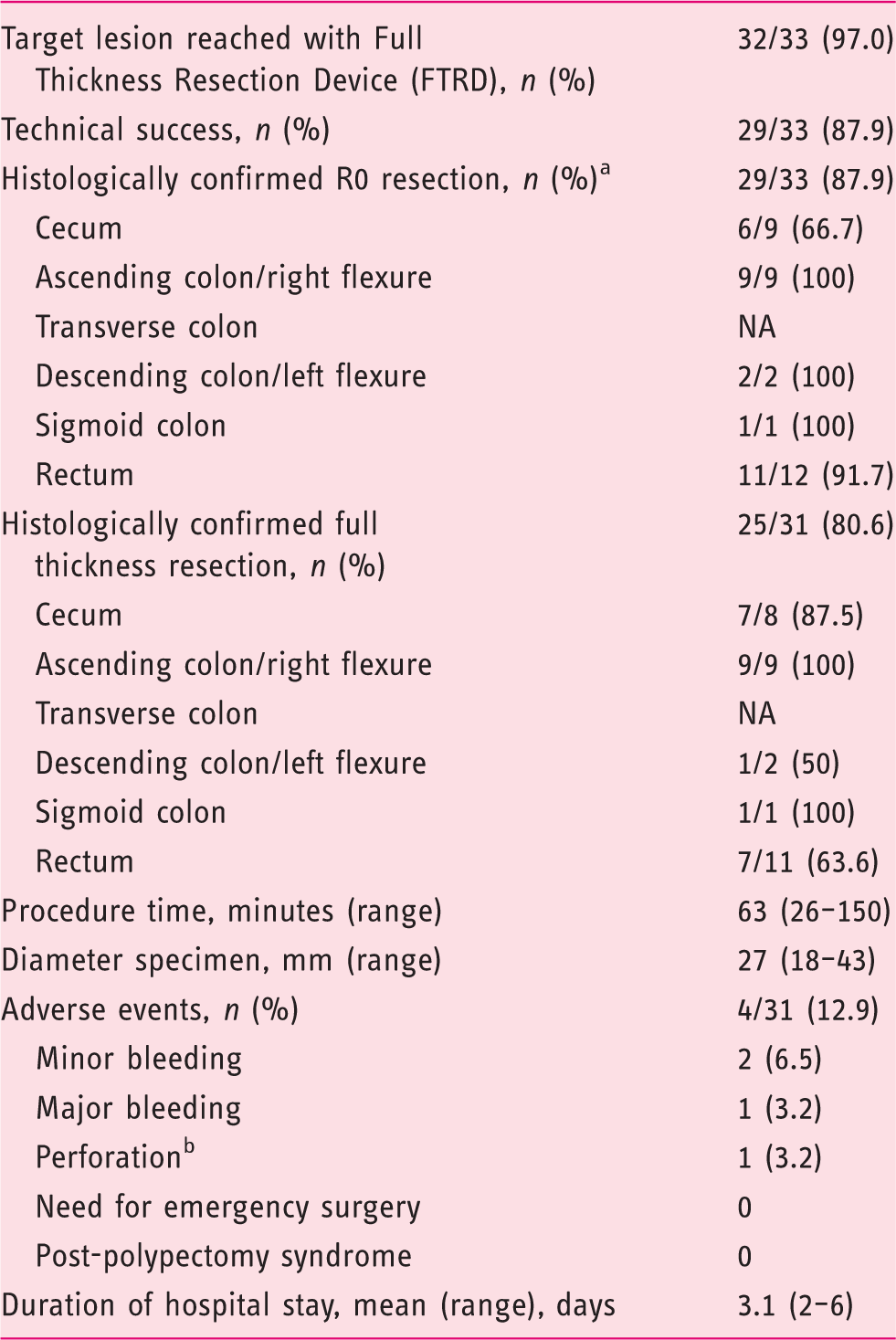
n = 33 inclusive of two failures to obtain resection specimen (one due to not reachable target lesion with mounted FTRD system, one due to snare malfunction).
Procedural data, technical success and histopathology (Table 4)
The primary technical success rate was 87.9% (29/33). In one case the target lesion (located at the appendiceal orifice) could not be reached because of diverticulotic sigmoid stenosis; another three failures were due to snare malfunction. In two of three instances of snare malfunction, secondary resection with a conventional snare was successful as a salvage procedure during the same session.
In the 31 cases amenable to EFTR, resection was en bloc and histologically complete (R0) in 93.5% (29/31), resulting in an R0 resection rate of 87.9 (29/33) as calculated on an intention-to-treat (ITT) basis. Histologically confirmed FTR was achieved in 80.6% (25/31), i.e. 90.0% (18/20) in the colon and 63.6% (7/11) in the rectum. The mean overall procedure time was 63 minutes (range 26–150 minutes). The mean diameter of resected specimens as assessed by the pathologist was 2.7 cm (range 18–43 mm). Incomplete resection occurred in one case with a 2 cm lesion at the appendiceal orifice, but the adenoma residues were amenable to a standard snare resection during the same session. In another case of incomplete resection a primary nonlifting cecal polyp had been resected that turned out to be adenocarcinoma reaching the lateral resection margins. Owing to high age and comorbidity, the patient refused surgery. At follow-up colonoscopy 10 weeks later, the OTSC was not in situ anymore, allowing for a second EFTR to resect the residual lesion. Histology showed no residual carcinoma, but adenoma with high-grade dysplasia.
Complications (Table 4)
The overall complication rate was 12.9% (4/31). Three post-procedural bleedings were noted, two of which were minor. One major bleed required blood transfusions and re-colonoscopy for endoscopic hemostasis with injection of adrenalin and application of an endoclip to a visible vessel at the resection site. The most serious complication was a delayed perforation (three days post-procedure) at the resection site. This patient required a right-sided hemicolectomy.
Device malfunction
Snare malfunction occurred in three cases. In one case the snare could not be closed once the clip was released. The endoscope was withdrawn and the adenoma ligated by the clip was completely resected using a standard monofilament snare. In the second case the snare showed a complete rupture during the resection process, resulting in incomplete resection. Again the residual adenoma was resected with a monofilament snare. In the third case the snare twisted into an 8-shape, rendering resection impossible.
Clinical outcome and follow-up
In one patient (aged 60 years) with a previously treated nonlifting lesion in the cecum, classified as tubulo-villous adenoma with high-grade dysplasia, histology of the subsequent EFTR specimen revealed pT1 L0 V0 G2 sm3 adenocarcinoma. Thus the patient was referred to surgery for right-sided hemicolectomy. The surgical resection specimen was free of residual neoplasia and contained no lymph node metastases.
In an 82-year-old patient, a primary nonlifting lesion in the cecum was incompletely resected and histology revealed an adenocarcinoma reaching the lateral resection margins. This patient refused surgery because of comorbidity and high age. Two months later a follow-up colonoscopy was performed. The OTSC had fallen off and the remaining lesion was resected with a second FTRD procedure. Histology revealed an adenoma with high-grade dysplasia. Follow-up one year later with colonoscopy and CT scan showed no signs of recurrence.
The patient with a lesion at the appendiceal orifice not amenable to EFTR due to sigmoid stenosis underwent surgical resection. The final diagnosis was tubulo-villous adenoma with focal high-grade dysplasia.
Discussion
Introduced in Europe in September 2014, the FTRD system is still investigational, with limited data available so far. To our knowledge, this is the largest series of FTRD in consecutive patients so far. To date, four case reports15–18 and two retrospective studies have been published,19,20 the latter two comprising a total of 45 cases. More data are expected from the Wall Resect Study, which completed patient recruitment in April 2016 and at present provides preliminary data from 181 patients. 21
In this paper we present our experience of 33 consecutive patients treated with FTRD, selected on the grounds that they would otherwise have had to undergo surgical resection. Nonlifting adenomatous polyps after previous polypectomy represented the great majority of treatment indications (for further details see Table 2). The procedure was accomplished successfully in 31 patients (93.9%). The failures were attributable to diverticulitic sigmoid stenosis in one case, in which the passage of the colonoscope was impossible once the FTRD was mounted, and to device malfunction in another case.
In cases in which the target lesion could be reached, the intervention proved to be very efficacious. En bloc-R0 resection was achieved in 29/33 patients (87.9%), which compares favorably to the results of previous studies (75%–80.6%)19,20 as well as to the preliminary data available from the Wall Resect Study (76.6%). The overall rate of histologically proven FTR of 80.6% (colon 90.0%, rectum 63.6%) was slightly below the rate of 87.5% published by Schmidt et al. This may be explained by the higher percentage of lesions located in the rectum in our study (36.4% vs 8%). An FTR is more difficult to achieve in the rectum as compared to the colon, since the rectal wall is thicker and less mobile. However, the relatively high rate of “non-FTRs” in the rectum did not negatively affect the rate of R0 resections, which reached 100% in rectal lesions. In all non-FTR resections, the muscularis propria layer was included, thus accurate assessment of submucosal invasion depth was not compromised in any case.
The mean diameter of resected specimens was 27 mm (18–43 mm), which is in accordance with published data. In preclinical porcine experiments the maximum size of colonic resection specimens was 40 × 42 mm. 22 In humans lesions with a diameter of up to 30 mm are considered as manageable by FTRD. The maximum size of the lesions is one of the major limitations of the FTRD system. Furthermore, the tissue volume that can be mobilized into the cap strongly depends on the elasticity of the lesion and the individual physical properties of the colonic wall at the resection site. Not only the diameter, but also the shape of the target lesion has to be taken into account. Flat lesions are more suitable than polypoid ones. The size of the FTRD cap does not allow accommodating more than 3 cm3.
The procedure was adequately safe. Bleeding is known to be the most common post-interventional adverse event after EFTR. We observed early bleeds (i.e. within 24 hours) in three cases (9.7%), two of which were classified as minor. One major bleeding required blood transfusions and colonoscopic hemostasis by clipping of a visible vessel. Schmidt et al. 20 and the Wall Resect Study 21 reported lower bleeding rates of 4% and 2.8%, respectively.
The most severe complication in our series occurred after EFTR of a polyp in a difficult location, i.e. around a diverticulum. One delayed perforation (3.2%) was diagnosed three days after the primarily uneventful procedure. The patient underwent right-sided hemicolectomy. Richter-Schrag et al. 19 reported a late perforation following a failed EFTR due to snare malfunction, which necessitated completion of the procedure with a conventional snare resection. In the Wall Resect Study a similar perforation rate of 3% was reported. 21 Therefore perforations remain a concern. Further studies will have to assess the true risk more precisely. Theoretically, safety should be assessed in comparison to surgical resection in a prospective, randomized fashion.
Another safety concern relates to the theoretical possibility of incorporating adjacent extracolonic anatomical structures into the resection specimen. However, no such events have been published in the literature so far. The risk may be reduced by diligent handling of the device. Caution should be exerted when mobilizing the target lesion into the cap; pulling the lesion with the forceps is preferable over aspirating it by suction.
Technical performance of the device deserves special attention when a new method is introduced. Technical failure, i.e. snare malfunction, was encountered in three instances during our study (9.7%). In one case the snare did not close properly after the clip had been released and in a second case the snare ruptured while closing. As a salvage procedure in these two cases, a conventional snare polypectomy was added to resect the clip-ligated specimens. The therapeutic success was not compromised, as full thickness R0 resections were nevertheless achieved. In a third case the snare took the configuration of an 8-shape, rendering resection impossible. Snare malfunctioning has been reported previously in the series by Richter-Schrag et al. 19 They describe three similar events (15%), leading to late perforation in one case, as mentioned above. These events prompted the manufacturer to modify the device. Hopefully this will help to avoid technical problems of this nature in the future.
While safety can be rated as good in standard indications, EFTR in difficult situations deserves special consideration. FTRD has been applied to resect adenomatous polyps in difficult locations such as the appendiceal orifice 20 or diverticular openings. 16 However, experience is limited yet. We performed EFTR at the appendiceal orifice in two cases. Both patients had their appendix in situ (i.e. no previous appendectomy). Both cases took an uneventful post-interventional course. Theoretically, closure of the appendiceal orifice by FTRD may result in acute appendicitis or mucocele. The study by Schmidt et al. 20 reports on five patients with cecal adenomas treated by EFTR, resulting in a full resection of the appendiceal orifice. Two out of five patients (40%) developed a post-polypectomy syndrome with pain, fever and elevated C-reactive protein (CRP). Both patients responded well to conservative treatment and recovered within three days.
We performed EFTR of a lesion located around a diverticulum opening in one case only. This patient experienced a delayed perforation, which was the only severe complication observed in this series, as described above. Taken together, these observations suggest that EFTR procedures in the above-mentioned difficult locations carry a higher risk than when performed under standard indications. Further studies will have to define the definitive place of this method in these special situations.
Conclusion
FTRD offers an additional, non-surgical option in the management of nonlifting colorectal lesions. EFTR by FTRD appears to be feasible and efficacious in the treatment of lesions up to 30 mm in diameter. It can be considered as an alternative to surgical therapy in selected patients. However, the risk of adverse events (particularly perforations) needs further consideration. More studies are needed to define the definite place of EFTR by FTRD.
Limitations of our study
Limitations of the study include its retrospective character, the relatively small number of patients and the non-standardized follow-up after resection.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethics approval
The study was approved by Swiss Ethics (Project-ID 2016-01238 17/098), 25 July 2016.
Informed consent
All our patients provided written informed consent.