
Abstract
Background
Colorectal lesions are generally evaluated during the withdrawal phase of colonoscopy. Minimising the risk of missed lesions is crucial to determine an appropriate future surveillance colonoscopy interval.
Objective
This study aimed to evaluate the clinical significance of detecting sigmoid colon lesions during the insertion phase.
Methods
This retrospective study included 172 consecutive patients undergoing colonoscopy between October 2017 and April 2018. The total number of detected polyps, mean polyps per procedure, mean polyps per positive procedure, and histological and clinical characteristics of detected lesions were recorded. The primary endpoint was the difference in sigmoid colon polyp detection rates during insertion and withdrawal.
Results
A total of 172 colonoscopies were performed for each patient and 322 lesions were detected. Sixty-two (19%) polyps were detected during insertion, 312 (97%) during withdrawal, and 52 (16%) during both insertion and withdrawal. Although all polyps except for those in the sigmoid colon could be detected during withdrawal, 10 of 87 (11%) polyps in the sigmoid colon could only be detected during insertion.
Conclusions
In this study, attempts to detect polyps, even in the insertion phase, showed the clinical significance to decrease the risk of missed adenomatous polyps in the sigmoid colon.
Key summary
Summarise the established knowledge on this subject:
The appropriate screening colonoscopy interval should depend on the endoscopy findings, including the number, size and histological findings of detected lesions. Colorectal lesions are generally evaluated during the withdrawal phase of colonoscopy. What are the new findings of this study?
About 10% of polyps in the sigmoid colon could only be detected during the insertion phase. Insertion phase detection can minimise the risk of missing adenomatous lesions in the sigmoid colon.
Introduction
Colonoscopy has a wide range of clinical significance; notably, screening colonoscopy reduces colorectal cancer (CRC) incidence and mortality in the age-adjusted average-risk population.1–5 It is widely recognised that an appropriate screening colonoscopy interval should depend on the endoscopy findings. This includes the number, size and histological findings of detected lesions, and this approach has been adopted by the US Multi-Society Task Force on Colorectal Cancer Screening and European Society of Gastrointestinal Endoscopy.6,7 Hence, to ensure the efficacy of screening colonoscopy for CRC prevention, the quality of polyp detection should be improved to reduce the missed lesion rate.8,9 Regarding the location of missed polyps, the ascending colon has been reported as the most frequent site of missed polyps because of its anatomical features, that is, they can be behind deep folds or curvatures.10–12 Considering the clinical practice of colonoscopy, intraluminal appearance in the sigmoid colon often changes compared to those in other sites of the colon because the volume of air insufflation or patient position influences the shape of the bowel lumen, depth of the fold, and angle of the flexure. Therefore, accurate evaluation of missed lesions is likely different in the sigmoid colon compared to other sites of the colon.
Lesion detection is usually performed during the withdrawal phase after reaching the caecum, and it could be challenging to detect lesions during the insertion phase. During colonoscopic insertion, air insufflation should be reduced as much as possible to reach the caecum easily and quickly, 13 and the colonic lumen tends to be narrower in the withdrawal phase. Therefore, withdrawal time and lesion detection are considered important parameters in evaluating the quality of colonoscopy.
Missed lesions, especially in the sigmoid colon, can be detected at the insertion phase but not in the withdrawal phase, because the folds of the sigmoid colon often appear to originate at a steep angle after skilful colonoscope insertion using a shortening or hooking technique, and polyps can actually be easily identified on insertion rather than on withdrawal. Polyp detection in the sigmoid colon specifically at the insertion phase is crucial, but such data are lacking. In this study, we aimed to evaluate the clinical significance of polyp detection in the sigmoid colon during the colonoscope insertion phase.
Methods
Objects
We retrospectively reviewed our colonoscopy database between October 2017 and April 2018. First, we selected colonoscopy records performed by a single endoscopist (T.S.) to avoid the effect of colonoscopy experience. During this period, TS performed a total of 384 colonoscopies. Records of patients who underwent colonoscopy for the following indications were included in this study: age and risk-appropriate colon cancer screening, colonoscopic evaluation of positive faecal occult blood test and surveillance colonoscopy after endoscopic resection of colorectal neoplasms. Exclusion criteria were poor bowel preparation, diagnostic colonoscopy prior to treatment, had undergone colectomy, emergent colonoscopy, hereditary polyposis syndrome and inflammatory bowel disease.
Colonoscopy
All examinations were performed using an endoscope system (LL-4450; Fujifilm Co, Tokyo, Japan) and high-definition colonoscope (EC-600ZP, EC-600ZP7; Fujifilm Co., Tokyo, Japan). A single experienced endoscopist, who has performed more than 5000 colonoscopies, recorded the following parameters on each colonoscopy: images of detected lesion immediately after insertion to the end of withdrawal, number of detected lesions on both insertion and withdrawal, time to reach a caecum, pure observation time (withdrawal), clinical features of detected lesion and endoscopic diagnosis of detected lesions (location, size, macroscopic type and estimated histology). All detected lesions diagnosed as non-invasive cancers were treated endoscopically during the withdrawal phase and the lesions diagnosed as invasive cancers were referred to surgery. We allowed the ‘resect and discard strategy’ for lesions less than 10 mm in diameter, which were diagnosed as non-index lesion adenoma or sessile serrated adenoma using magnification with blue laser optical imaging.14–19 Lesions that were diagnosed as hyperplastic polyps or non-adenomatous/neoplastic nodules less than 10 mm located between the sigmoid colon and the rectum were not counted.
Outcomes
The total number of detected polyps, mean polyps per procedure, mean polyps per positive procedure (positive procedure was defined as a procedure in which one or more polyps were detected), and histological and clinical characteristics of detected lesions were our outcomes of interest. The primary endpoint of this study was to compare the polyp detection rates in the sigmoid colon during the insertion phase and withdrawal phase, and to examine clinically significant differences.
Statistical analysis
All continuous values in this study were presented as mean (SD) and categorical variables as percentage (95% confidence interval).
Ethics
The study was conducted according to the guidelines of our Institutional Review Board, which approved this study and waived the requirement for subjects’ informed consent. All patients provided written informed consent for colonoscopy and endoscopic treatments.
Results
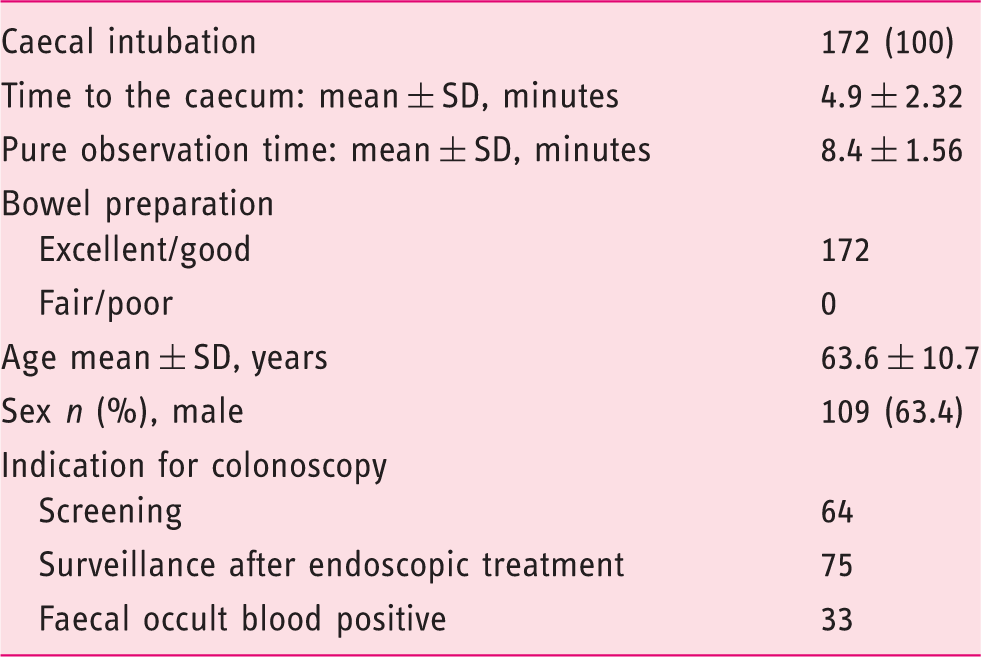
Characteristics of colonoscopic examination.
Clinical features of detected polyps.
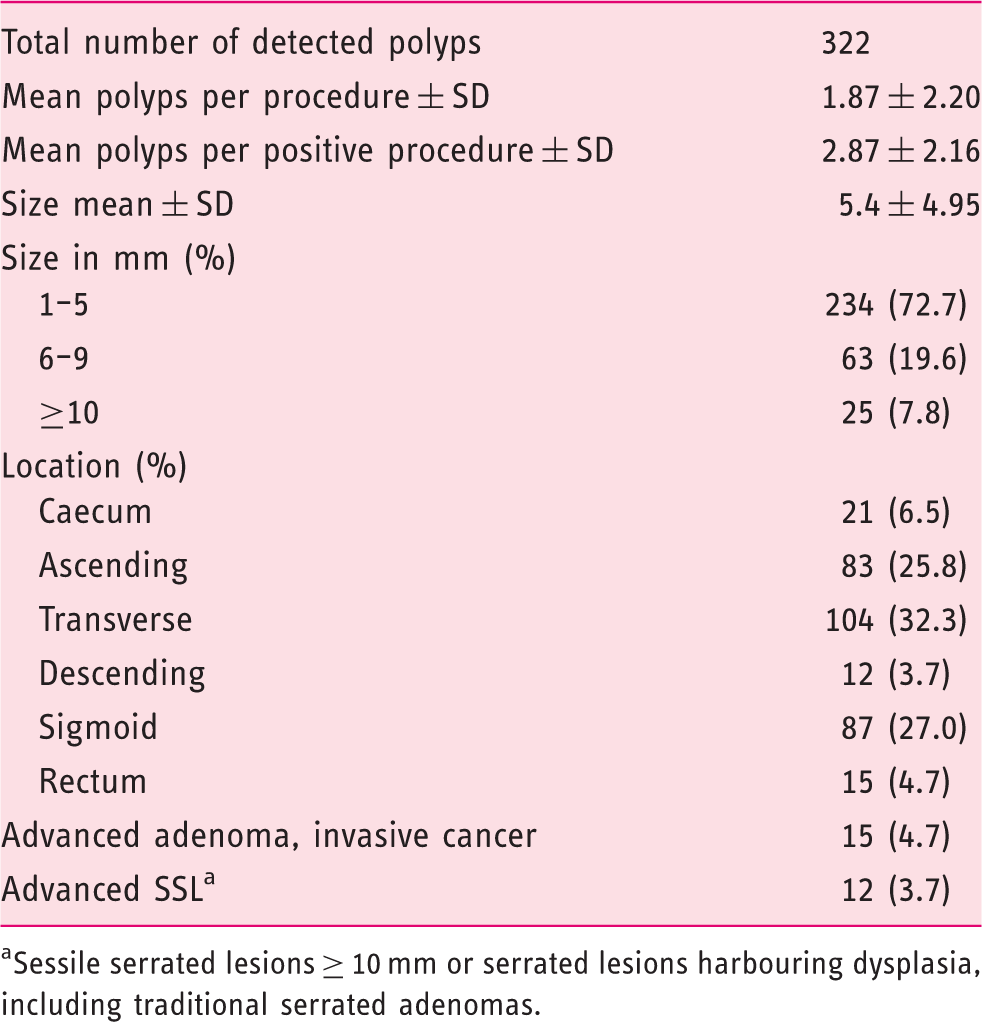
Sessile serrated lesions ≥ 10 mm or serrated lesions harbouring dysplasia, including traditional serrated adenomas.
Comparison of lesions detected during insertion and withdrawal.
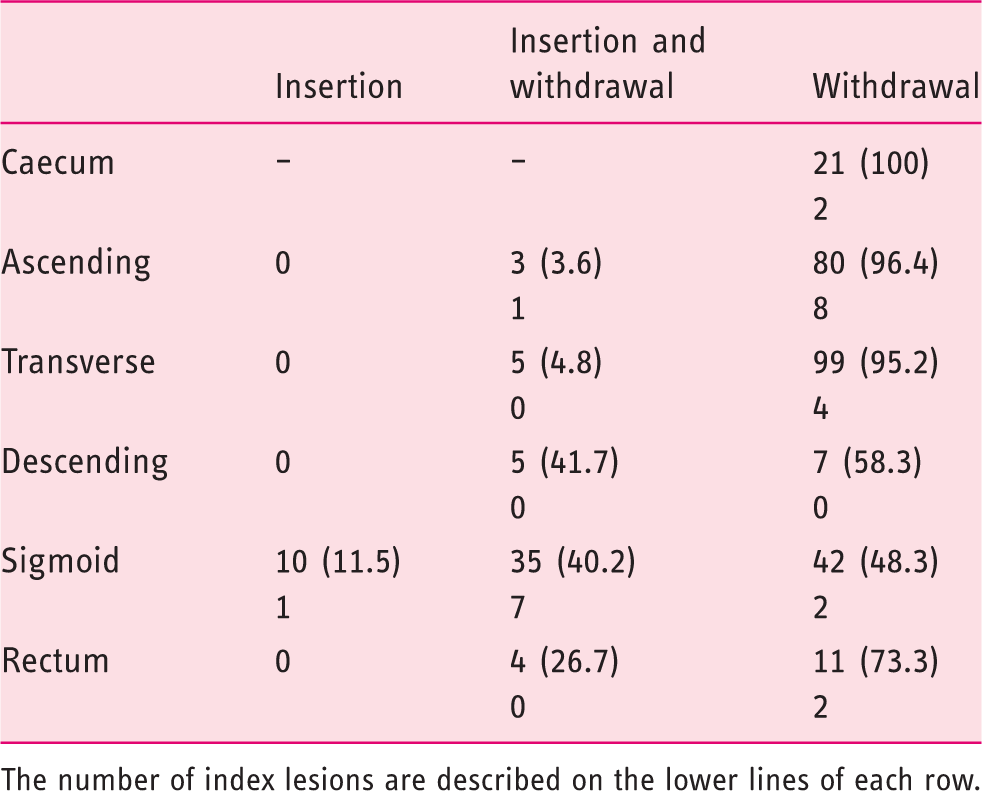
The number of index lesions are described on the lower lines of each row.
Discussion
Our results support the clinical significance of polyp detection in the sigmoid colon during the colonoscope insertion phase. The importance of polyp detection during the insertion phase was previously reported by Morini et al. 20 and our study results are consistent with their conclusions.
The insertion phase of colonoscopy should be performed to reach the caecum quickly and safely with minimal air insufflation. After an ideal colonoscope insertion with a shortening technique, the sigmoid colon folds often appear to originate at a steeper angle during the withdrawal phase than during the insertion phase; therefore, there is an increased risk of missing lesions behind or between the folds in the sigmoid colon on scope withdrawal. This situational irony occurs between an ideal colonoscope insertion technique and missing lesions behind or between the colonic folds on colonoscope withdrawal. Therefore, we propose the clinical significance of not missing sigmoid colon lesions on withdrawal while identifying them during the insertion phase, and propose the importance of capturing images of lesions in the sigmoid colon and treating them simultaneously during the insertion phase at the endoscopist’s discretion. Marking near the detected sigmoid colon lesion during the insertion phase and resecting it during the withdrawal phase might be allowed, because endoscopic resection during the insertion phase might increase the amount of infiltration, which makes it difficult to achieve total colonoscopy, especially for less-experienced endoscopists. In our study, only 10 lesions were detected during the insertion phase and these lesions were actually missed during the withdrawal phase. Seven of 10 lesions were identified again by reinsertion to the sigmoid colon after returning to the rectum, and three lesions, which were macroscopically considered diminutive adenomas, were not reidentified by scope reinsertion.
In terms of screening colonoscopy quality assurance, the adenoma detection rate (ADR) is widely recognised as a reliable measurement, and some factors such as withdrawal time, caecal intubation rate and quality of bowel preparation have been reported to affect the ADR. In our study, these factors certainly contributed to the ADR, and our results suggested that ADR during the insertion phase should be considered a quality indicator in screening colonoscopy, particularly for left-sided lesions.
Some modalities have been developed to increase the ADR, such as full-spectrum endoscopy system, third-eye endoscopy and some distal attachments for unfolding a colonic fold. These modalities have been reported as promising to decrease the rate of missed lesions; however, these modalities also have disadvantages, including higher costs of equipment and decreased scope manoeuvrability. In contrast, our proposal of paying attention to the lesions during insertion, especially in the sigmoid colon, is simple, easy to follow and most likely cost-effective.
These efforts may detect non-significant lesions that have a minimal risk of developing CRC; however, appropriate colonoscopic surveillance intervals are recommended based on the number of adenomas, regardless of the lesion size, by the societal guidelines of the European Society of Gastrointestinal Endoscopy and the American Society for Gastrointestinal Endoscopy. Moreover, most CRCs have developed via the adenoma–carcinoma sequence, and removing all precursor lesions ought to decrease the risk for the morbidity of CRC. Therefore, an approach to finding lesions regardless of their size is justified.
There are some limitations to this study. First, we matched the detected lesions between the insertion and withdrawal phases by comparing the numbers, sizes, locations and morphologies of detected lesions. Hence, there is some possibility of mismatching, especially for diminutive polyps. Fortunately, the mean number of polyps per positive procedure was 2.87, and we did not have so much trouble matching detected lesions through the examination. Second, all examinations were performed by a single experienced endoscopist, which raises a question regarding external validity. Third, the sample size might have not been large enough to reach statistical significance. Moreover, in this study, most detected lesions were diminutive polyps, and it is crucial to investigate the efficacy of detecting index lesions such as flat, depressed or larger lesions. To overcome these weaknesses, a prospective, randomised control study among multiple institutions should be considered. This pilot study could be utilised to determine the design of a future larger-scale, prospective randomised trial.
In conclusion, our study highlights the clinical significance of detecting sigmoid colon lesions during the insertion phase, and the fact that insertion phase detection can minimise the risk of missing adenomatous lesions in the sigmoid colon. This approach should be considered to be one of the quality measurement indicators in screening colonoscopy.
Footnotes
Acknowledgements
The authors are grateful to Hiroyuki Takamaru, Masau Sekiguchi and Masayoshi Yamada for their valuable comments on this study.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethics approval
The procedures in this study were in accordance with the Helsinki Declaration of 1964 (2013 revision). The study was conducted in accordance with the guidelines of our institutional review board and approved by the Ethics Committee of the National Cancer Centre on 18 March 2017.
Informed consent
All patients provided written informed consent for the colonoscopy and endoscopic treatments.