
Abstract
Background
Since introduction of the MELD score in the liver allograft allocation system, renal insufficiency has emerged as an increasing problem. Here we evaluated the course of kidney function in patients with advanced renal insufficiency prior to liver transplantation (LT).
Methods
A total of 254 patients undergoing LT at the University Medical Centre Hamburg-Eppendorf (2011–2015) were screened for renal impairment (GFR < 30 ml/min) prior to LT in this observational study.
Results
Eighty (32%) patients (median 60 years; M/F: 48/32) had significant renal impairment prior to LT. Median follow-up post-LT was 619 days. Patient survival at 90 days, one year and two years was 76%, 66% and 64%, respectively. Need for dialysis postoperatively but not preoperatively was associated with increased mortality (p < 0.05). Renal function improved in 75% of survivors, but 78% of patients had chronic kidney disease ≥ stage 3 at end of follow-up. Of eight (16%) survivors remaining on long-term dialysis, so far only four patients have received a kidney transplant.
Conclusion
Postoperative dialysis affected long-term mortality. In 75% of survivors renal function improved, but still the majority of patients had an impaired renal function (CKD stage 3–5) at end of follow-up. Future studies should elucidate the impact of kidney dysfunction and dialysis on recipients’ long-term survival.
Keywords
Introduction
Acute or chronic kidney dysfunction (CKD) in liver transplant patients is a major medical need to improve diagnosis and therapy. In particular, as a consequence of the introduction of the model for end-stage liver disease (MELD) score for liver allograft allocation, the proportion of CKD emerged in candidates for liver transplantation (LT). 1 Nowadays prevalence of CKD in liver transplant recipients ranges from 20% up to 80%.2–4 Advances in postoperative care and wide use of immunosuppressant therapy with calcineurin inhibitors (CNI) such as tacrolimus and cyclosporine have improved patients’ outcome after LT.5,6 However, development of end-stage renal disease, e.g. due to CNI-associated nephrotoxicity, lowers long-term survival markedly.2,6 Ojo et al. reported a more than four-fold increased risk of death in a large cohort of non-renal transplant recipients developing CKD. 7
As a consequence introduction of the MELD system resulted in a marked increase of simultaneous liver-kidney transplantation (SLK), particularly in the United States (US).8,9 It has been shown that SLK improves renal outcome and survival in comparison to LT alone.1,10 Furthermore, similar one-year survival rates in patients with renal disease undergoing SLK compared to patients without renal dysfunction undergoing LT alone were reported.8,10
On the other hand, SLK has been criticised for shifting kidney allografts away from patients on the renal transplant waiting list. Especially in high MELD liver transplant recipients simultaneous transplantation of a kidney might represent a futile procedure because of the impaired short-term survival of these patients. In order to avoid the unnecessary transplantation of a kidney into a patient dying in the early postoperative period after LT, the option of kidney-after-liver transplantation (KALT) is offered to all liver transplant candidates with severe renal impairment in the Eurotransplant region. These patients who are listed with a KALT option prior to liver-only transplantation receive a very high prioritisation (with 500 additional points) on the renal transplant waiting list in case of a creatinine clearance of less than 15 ml/min during a period of 90 to 360 days after LT. 11 This results in a high probability of getting a graft allocated within the first year post-LT, in comparison to the very long waiting time on the waiting list for regular dialysis patients (approximately six to eight years). As KALT represents a further transplant strategy for patients developing end-stage renal disease after LT, it increases year per year.8,12
Both SLK as well as sequential KALT are well-established transplant procedures in patients with necessity for LT and renal dysfunction.8,11,13 Reduced renal allograft rejection was reported by several authors in patients undergoing SLK compared to KALT.8,14 Simpson et al. presumed a specific renal graft immunoprotection provided by the liver allograft. 14 However, in particular many European transplant centres favour the sequential approach. One main advantage of sequential KALT is that renal transplant is performed only among those LT recipients who do not recover renal function during a predefined time period of 360 days. This approach could help to save donor kidneys not needed after LT, and therefore represents a feasible alternative strategy to SLK.
However, data on renal function and long-term outcome in patients with renal insufficiency listed for LT with optional KALT are scarce. Therefore, this single-centre retrospective analysis aimed to evaluate the natural course of kidney function in patients with significant renal insufficiency prior to LT.
Patients and methods
In this retrospective observational study all adult patients undergoing LT at the University Medical Centre Hamburg-Eppendorf (n = 254) between January 2011 and August 2015 were screened for significant renal impairment prior to LT. Indication for KALT option was an estimated glomerular filtration rate (GFR) of less than 30 ml/ min as determined by the Modification of Diet in Renal Disease (MDRD) formula 2 at any time on the LT waiting list. For analysis patients were classified according to the nadir GFR value within a time period of three months prior to LT.
Data regarding demographic characteristics, aetiology of underlying liver disease, severity of hepatic impairment (MELD score), aetiology and severity of kidney dysfunction (CKD stage), laboratory data as well as necessity of renal replacement therapy (RRT) were assessed pre- and postoperatively as well as during long-term follow-up. Patients with an age below 18 years were excluded from the analysis.
Continuous variables were described as median and 25%–75% interquartile range (IQR); categorical variables were presented as absolute and relative parameters. Correlation analysis was performed using Spearman’s correlation. Continuous variables were compared using Mann-Whitney U test and categorical variables were compared using chi-square tests. Univariate and multivariate regression analysis was performed to determine independent factors of mortality. For estimation of survival, Kaplan-Meier analysis and log-rank test were performed. For data management and analyses we used MS Excel 2008 for Mac, SPSS 17 for Mac (SPSS Inc, Chicago, IL, USA). A p value of < 0.05 was considered significant.
Results
Patient characteristics
Eighty of 254 (32%) LT recipients had significant renal impairment with a GFR < 30 ml/min prior to LT and were listed for optional KALT.
Patient characteristics at baseline.
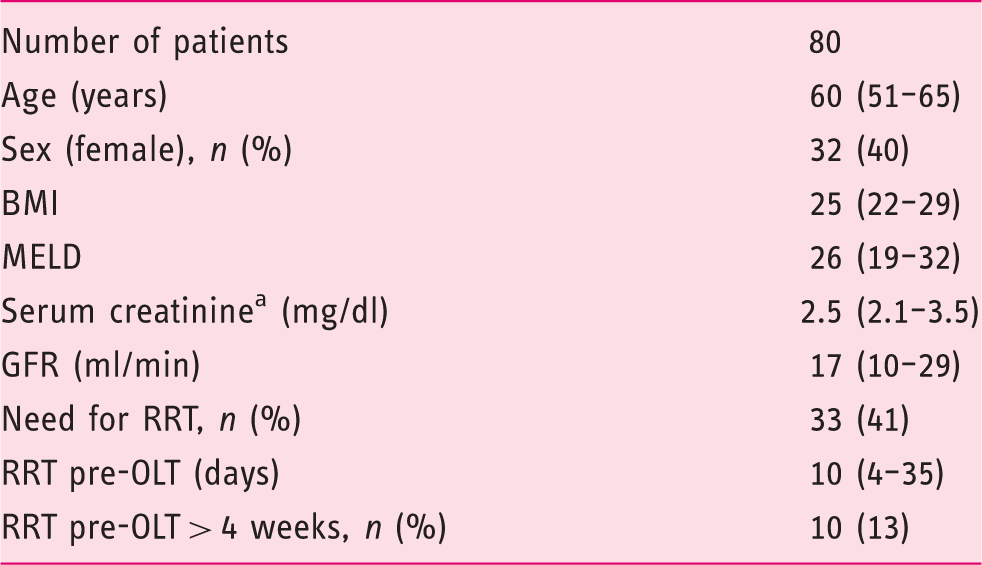
All values are presented as median (interquartile range (IQR)) or numbers (%).
Patients without need for renal replacement therapy.
BMI: body mass index; MELD: model for end-stage liver disease; GFR: glomerular filtration rate; CKD: chronic kidney disease; RRT: renal replacement therapy; OLT: orthotopic liver transplant.
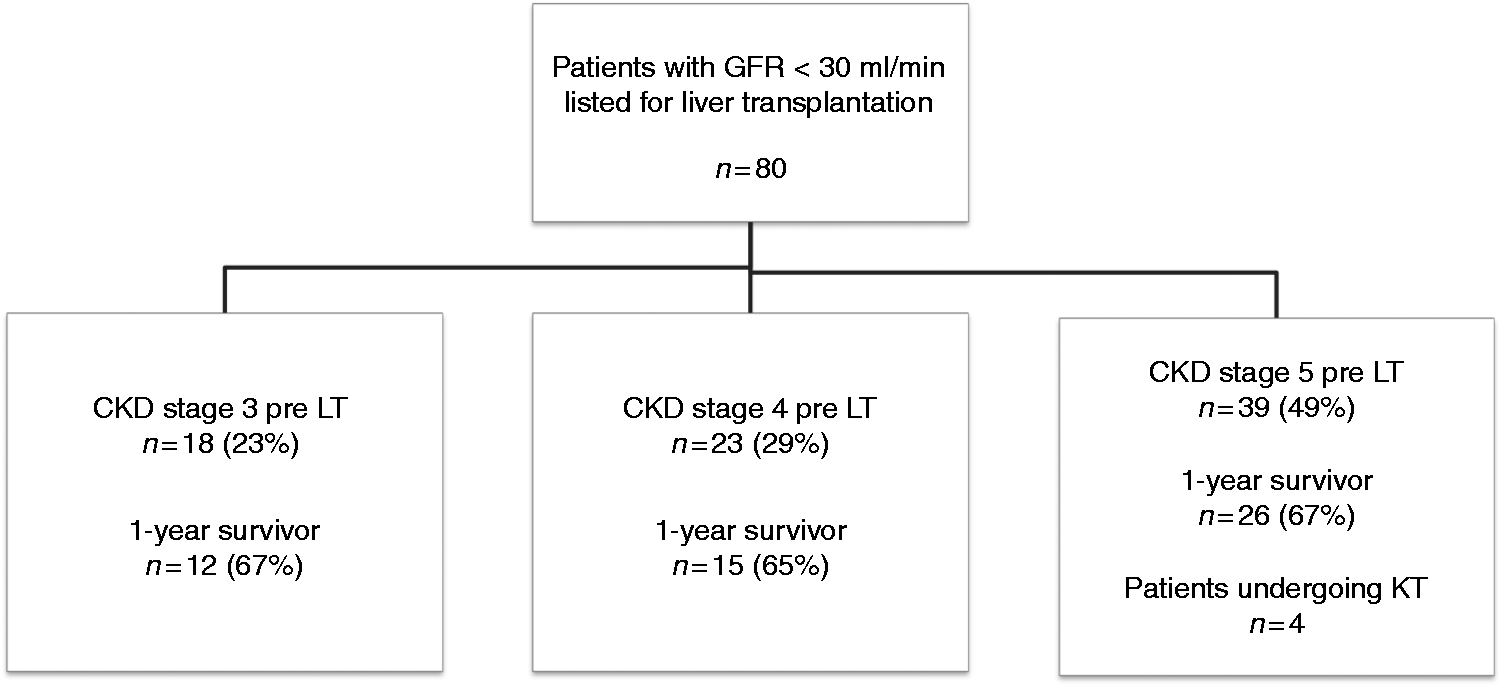
Study overview.
Development of renal function post-LT
In total RRT was needed in 53 (66%) patients peri- and postoperatively. On long-term follow-up eight (16%) patients surviving the postoperative period remained on RRT. Overall five of these patients were activated in the KALT program. Median time until activation post-LT was 5.5 months. Three patients received a KT during the predetermined KALT period of 360 days (median time from LT to KT: 7.6 months), whereas two patients failed to receive a kidney graft during this KALT period. After expiry of the KALT listing status one of these two patients received a kidney graft allocated via the European-Senior-Program (ESP) 31.3 months after LT. The other patient is still listed on the KT waiting list without prioritisation.
Clinical characteristic during follow-up.
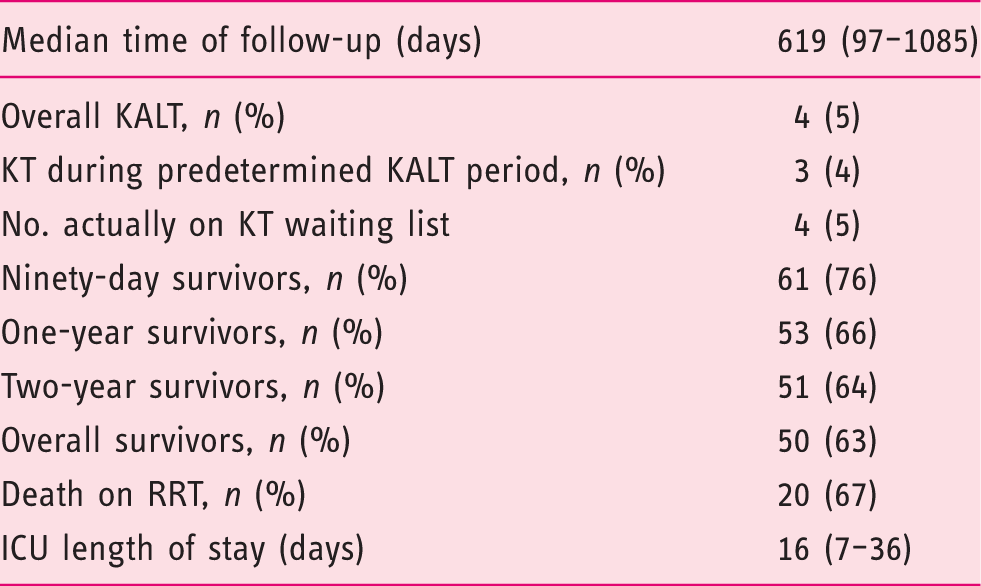
All values are presented as median (interquartile range (IQR)) or numbers (%).
KALT: kidney after liver transplantation; KT: kidney transplantation; RRT: renal replacement therapy; ICU: intensive care unit.
Development of renal function in LT recipients is illustrated in Figure 2. In general, in survivors renal function improved over the course of time:
CKD stage during the course of time in liver transplantation (LT) recipients listed for KALT.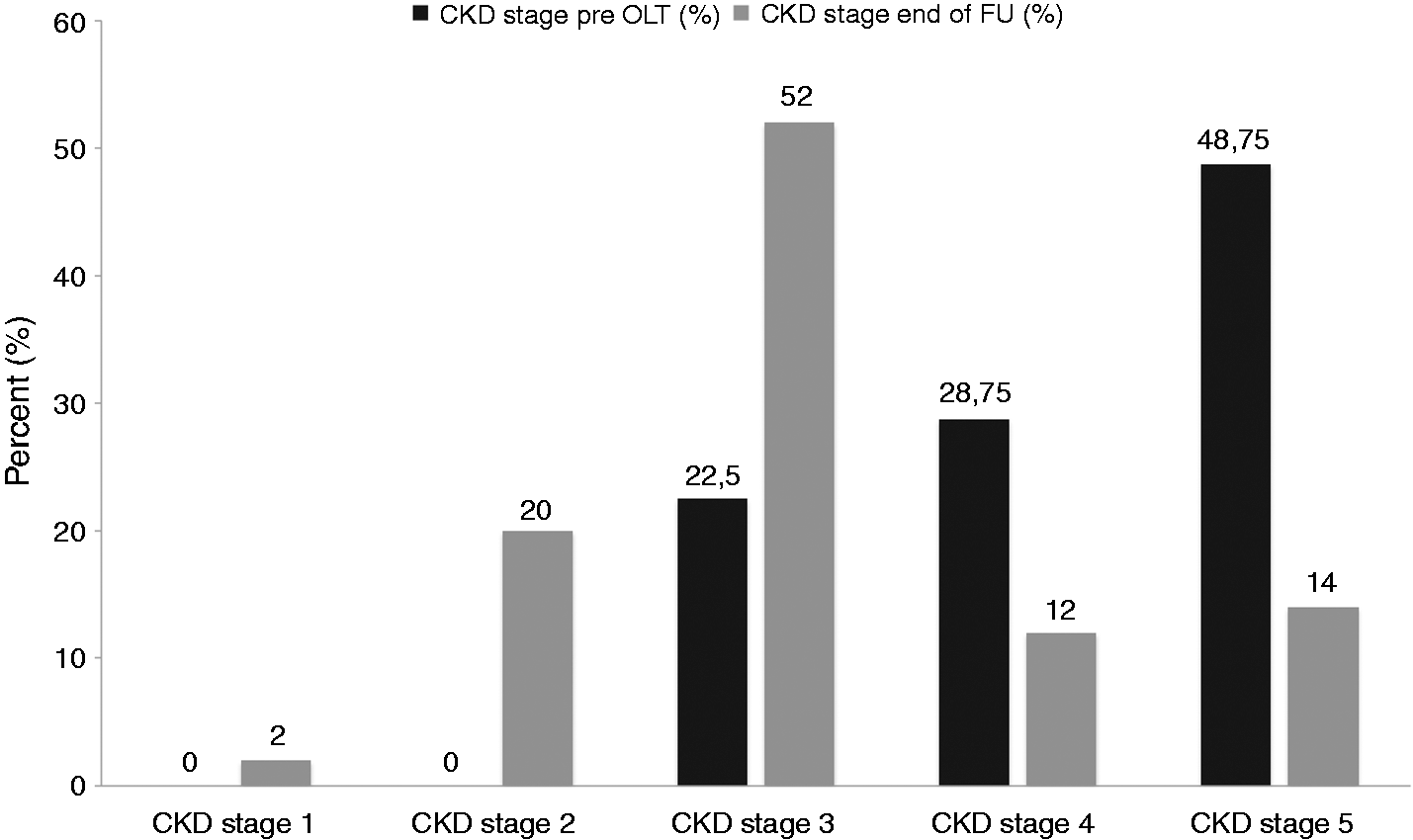
One patient (2%) with CKD 5 pretransplant showed a major improvement to a GFR of 97 ml/min (CKD stage 1). Ten patients (20%) who had CKD stage 3 (n = 2), CKD stage 4 (n = 4) or CKD stage 5 (n = 5) preoperatively improved post-LT to CKD stage 2.
Twenty-six (52%) patients who had CKD stage 3 (n = 7), CKD stage 4 (n = 7) or CKD stage 5 (n = 12) prior to LT fulfilled criteria of CKD stage 3 post-transplantation.
Six (12%) patients with CKD 4 (n = 2) and CKD 5 (n = 4) pre-LT had CKD 4 post-LT, respectively. On the other hand in four (8%) patients with CKD 3 (n = 1), CKD 4 (n = 1) and CKD 5 (n = 2) preoperatively renal function deteriorated to CKD stage 5 post-LT.
Clinical characteristics of 30 non-survivors.
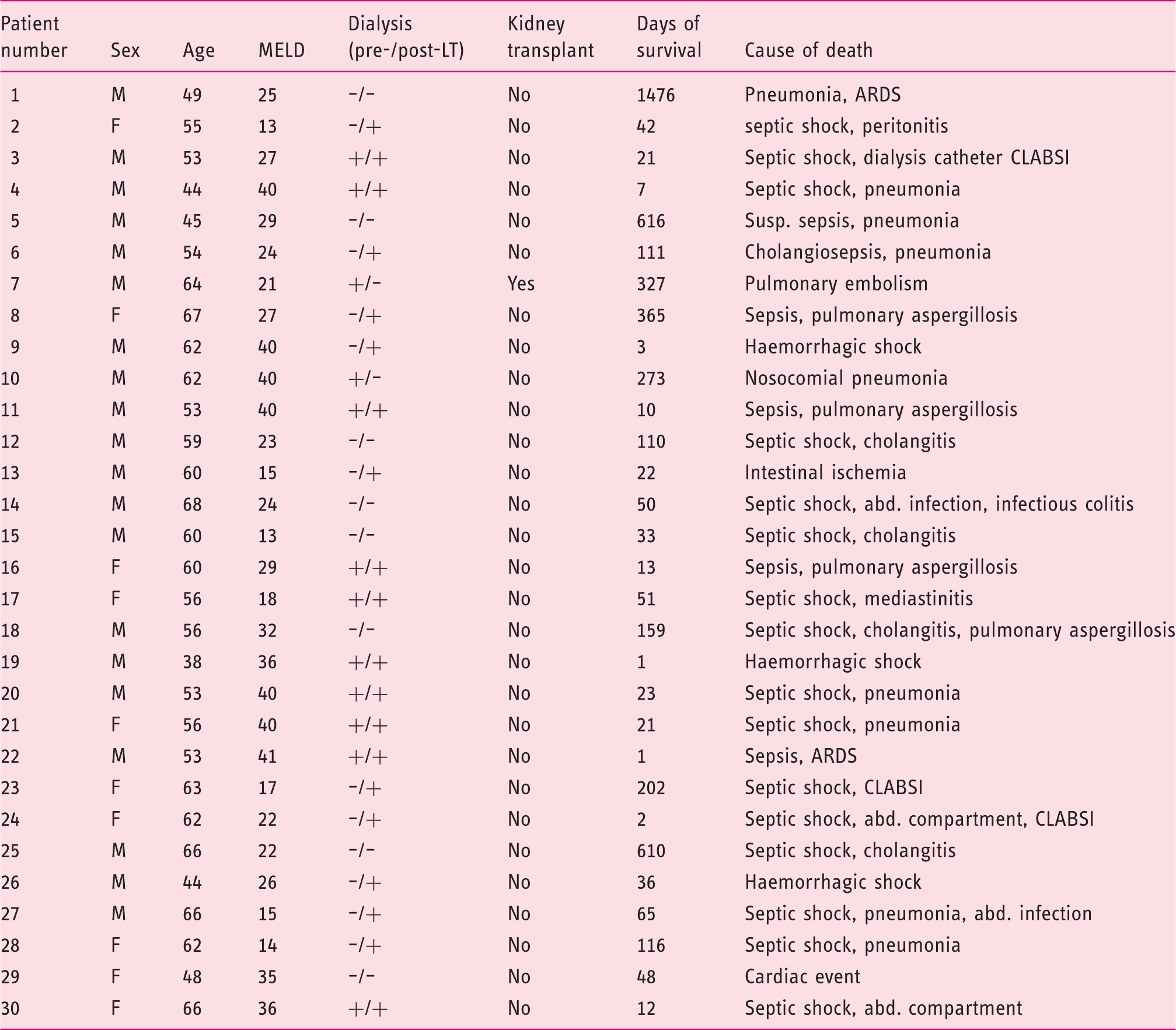
MELD: model for end-stage liver disease; LT: liver transplantation; ARDS: acute respiratory distress syndrome; CLABSI: central line-associated blood stream infection; M: male; F: female.
Patient survival
Patient survival at 90 days, one year and two years was 76%, 66% and 64%, respectively. Severity of renal dysfunction prior to LT had no impact on one-year mortality (see Figure 3(a)). Also necessity of RRT preoperatively did not affect long-term mortality (log-rank test: p = n.s.). In patients with prolonged RRT (>4 weeks) pre-LT (n = 10) there was a trend toward reduced 90-day survival (23% vs. 30%, p = n.s.).
Kaplan-Maier plot of one-year survival according to need for renal replacement therapy (RRT).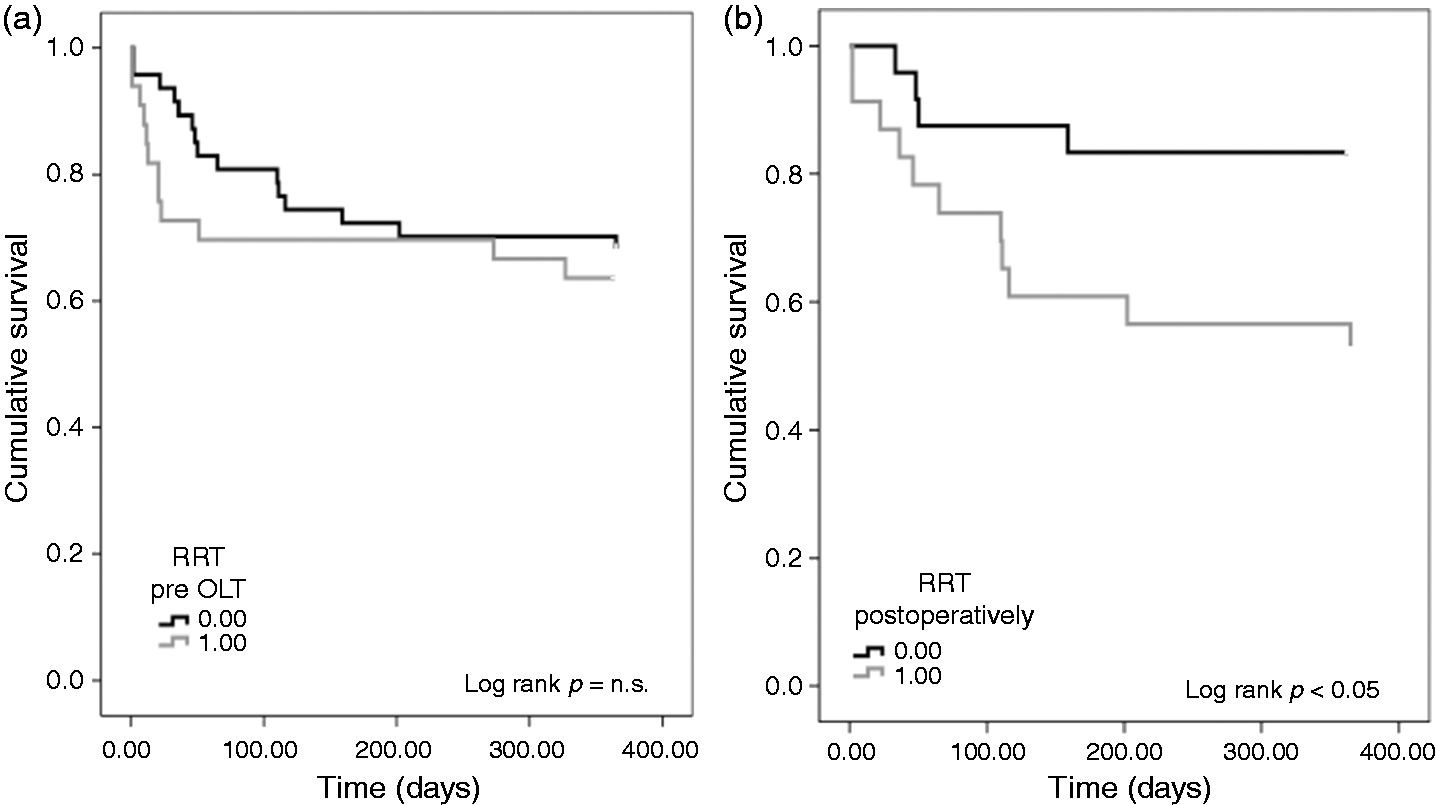
In contrast, postoperative onset of RRT was significantly associated with decreased one-year survival (Figure 3(b), log-rank test: p < 0.05). One-year survival rate in patients undergoing postoperative dialysis was 52% compared to 83% in patients without RRT. Also, need for dialysis post-LT was significantly associated with length of intensive care unit (ICU) stay (p < 0.05). However, there was no association of duration of RRT post-LT and patient survival (p = n.s.).
At last follow-up the majority of patients (n = 59; 74%) received a low-dose CNI-based immunosuppressive regimen combined with either mycophenolate mofetil (MMF), azathioprine (AZA) or steroids, while 15 patients (19%) were on low-dose CNI combined with a mammalian target of rapamycin (mTOR) inhibitor-based therapy, three (4%) patients were on mTOR-based CNI-free therapy and another three (4%) patients on CNI monotherapy.
The immunosuppressive regimen in patients with need for dialysis prior to LT was comparable to those with renal insufficiency without need for dialysis prior to LT (low-dose CNI + MMF/AZA/steroids: 41% vs. 59%; low-dose CNI + mTOR 47% vs. 53%). None of the patients with CNI monotherapy was on dialysis prior to LT.
Piggy-back LT was performed in 10 patients (13%) as compared to a conventional anastomosis in 70 patients (87%). There was no association between the surgical technique and need for RRT prior to or post-LT. However, patients undergoing piggy-back technique had slightly better CKD stage at end of follow-up (CKD stage 2 vs. 3; p = n.s.)
Discussion
CKD is a major complication in patients after LT with remarkable impact on long-term patient survival.2,15 Renal impairment in the pretransplant period due to hepatorenal syndrome (HRS) and acute or chronic kidney injury also in the peri- and post-transplant period, for example due to acute tubular necrosis or drug-associated nephropathy, directly affects long-term kidney function.6,13,16
There is lack of data regarding long-term outcome in patients with renal insufficiency pretransplant. We therefore aimed at assessing the course of renal dysfunction and long-term outcome of LT recipients with significantly impaired renal function pretransplantation.
Overall 32% of all LT recipients had significant renal impairment with a GFR of less than 30 ml/min prior to transplantation. In line with others, we observed that post-transplant renal dysfunction improved during the course of time in the majority of the surviving patients. 17 Forty-nine per cent of our patients had CKD stage 5 prior to LT, while more than half of patients fulfilled criteria for CKD stage 3 at the end of follow-up. Overall kidney function improved in 75% of survivors over the course of time, remained stable in 22% and further deteriorated in 4% after LT. However, overall renal function remained compromised in the majority of study patients and GFR was less than 60 ml/min in almost 80% of patients at the end of follow-up. Looking at the non-survivors, we found that almost 70% of them had terminal renal insufficiency with CKD stage 5 after LT.
Recovery of renal function may be due to reversible prerenal acute kidney injury (AKI) described in up to 50% of LT recipients during the early postoperative period as well as due to HRS.18,19 However, HRS is a difficult diagnosis of exclusion and often coexists with irreversible renal damage.2,13 Moreover, renal recovery may be decelerated after LT due to prerenal factors such as inflammation, hypovolemia, hemodynamic instability including usage of vasopressors or drug-induced injury such as CNI nephropathy.2,6
Patients undergoing renal transplantation for treatment of end-stage renal disease have better outcomes than those remaining on dialysis. 12 In our cohort, out of eight patients remaining on dialysis during long-term follow-up, five patients received a KALT bonus for a preferred KT within one year after LT. Four of these patients finally received a kidney graft. However, one of them received the kidney graft via ESP after an expiring KALT bonus; another one is still waiting for a kidney graft. Further, three patients were not activated for the KALT programme because they barely missed criteria for KALT bonus since their renal function deteriorated to a GFR of < 15 ml/ min only after > 1 year post-LT.
Summing up, three of eight (38%) patients had a benefit from the KALT programme by receiving a kidney graft within the predetermined KALT period of 360 days. On the other hand allocation via the KALT system failed in five of eight (63%) LT recipients with renal insufficiency and resulted in long-term need for dialysis. In Germany the average waiting time for a kidney graft is currently five to seven years.20,21 It can be assumed, but so far has not been shown, that on dialysis mortality is markedly increased for immunosuppressed LT patients as compared to other patients with CKD 5. Therefore it could be argued that LT patients should be granted a more extended KALT bonus. For instance, patients with renal insufficiency going on dialysis within three to 12 months after LT should be given priority not only for 12 months, but until receiving a kidney graft.
Furthermore, Martin et al. reported higher recipient as well as graft survival in patients undergoing KALT later than 360 days, compared to those undergoing early KALT within the first 90 days after LT. 8 Therefore, a prolongation of the KALT period would represent a favourable option for many more patients.
On the other hand a modification of the current cut-off for activation for KALT (actually creatinine clearance < 15 ml/min) might result in a larger variety of patients benefiting from the KALT bonus.
We observed a good long-term patient survival rate in our cohort with overall 63% during a median follow-up of 619 days. A large analysis of the United Network for Organ Sharing (UNOS) database showed a five-year patient survival of 50% in patients with preoperative renal insufficiency (assessed via a serum creatinine of ≥ 2.0 mg/dl). 22 Nair et al. reported an average five-year survival of 42% in patients with an average preoperative serum creatinine of 2.7 mg/dl. 23 Martin et al. reported in a retrospective analysis of the UNOS database patient survival rates for LT recipients undergoing KALT > 12 months post-LT, with a one-year survival of 76% and five-year survival rates of 46%, respectively. 8 However, it needs to be emphasised that comparability of KALT results observed in US studies mentioned before with our data is limited, as waiting time in the US patients was much longer. The aforementioned KALT option during a period of 90 to 360 days after liver-only transplantation is a specific and individual approach of the Eurotransplant network.
Pretransplant dialysis has been reported to be a negative predictor for renal recovery after LT and patient outcome.17,24 However, in line with Zand et al. we found that not preoperative dialysis but postoperative RRT is a clear predictor for death after LT. 25 Comparable to the findings of Northup et al. we observed a trend toward higher mortality in patients with pretransplant dialysis for a period of > 4 weeks. However, in our analysis this did not reach statistical significance. 17
Patients with renal dysfunction prior to LT needing postoperative dialysis had a significantly lower one-year survival rate (52%) compared to those without postoperative need for RRT (83%). We observed that postoperative RRT was associated with prolonged stay in ICU. It may be assumed that postoperative dialysis represents a complicated postoperative course and therefore directly affects mortality. 24 However, whether patients die ‘due to dialysis’ (by means of increased risk for infection, cardiovascular risk, etc.) or mainly die ‘on dialysis’, as the persistent need for dialysis is an expression of a complicated course, is a matter of debate.
The standard immunosuppressive regimen at our tertiary care centre consists of an interleukin (IL)-2 receptor antagonist (Basiliximab) on days 0 und 4 combined with a low-dose CNI therapy, followed by an early start of an mTOR inhibitor or MMF in patients with renal insufficiency.
Our study has some limitations. First, the sample size is rather small. However, this is the first study reporting long-term outcome in patients undergoing LT within the optional KALT programme. Second, it is a retrospective, single-centre analysis. Multicentre studies and large database analyses are outstanding tools for assessing a broad variety of cases. However, monocentric studies are capable of providing much more detailed information and a precise case-by-case review.
To conclude, we observed LT recipients with advanced renal insufficiency being listed for optional sequential KALT for a period of 21 months post-transplant. Overall patient survival was 63%. We found that not preoperative but postoperative dialysis clearly affected long-term mortality and length of ICU stay. Renal function improved over the course of time in 75% of survivors. However, nearly 80% of patients had a severely impaired kidney function by means of CKD stage 3 or worse at the end of follow-up. Therefore, nephroprotective immunosuppression regimens are of central importance to preserve renal function in transplant recipients. Future studies should further elucidate the impact of renal insufficiency and necessity of dialysis on recipients’ long-term survival.
Footnotes
Acknowledgement
All authors approved the final manuscript.
Declaration of conflict of interests
None declared.
Ethics approval
The study was performed according regulations of the local ethics committee.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
Since this was a retrospective analysis, no informed consent was obtained.