
Abstract
Background
Nodular regenerative hyperplasia is an uncommon liver condition associated with several autoimmune disorders and drugs. The clinical symptoms of nodular regenerative hyperplasia vary from asymptomatic to severe complications of portal hypertension (nodular regenerative hyperplasia-syndrome).
Objective
The purpose of this study was to identify the prognosis and optimal management, as well as the role of liver transplantation, in nodular regenerative hyperplasia.
Methods
The pathology databases of all three Dutch liver transplant units were retrospectively scrutinised for explanted livers diagnosed with nodular regenerative hyperplasia or without clear diagnosis. Pre- and post-transplantation clinical, biochemical, radiological and histological information was obtained from electronic and paper records.
Results
In total, 1886 patients received a liver transplant. In 255 patients, nodular regenerative hyperplasia could not be excluded. After detailed chart review, the native livers of 11 patients (0.6%) (82% male, median age: 44 years) displayed nodular regenerative hyperplasia. Seven patients (64%) had underlying disorders or drug exposure which possibly caused nodular regenerative hyperplasia. Laboratory and imaging abnormalities were present in all patients but did not contribute to the diagnosis of nodular regenerative hyperplasia. Five-year survival was 73% (median follow-up: four years, range: 2–248 months).
Conclusion
Nodular regenerative hyperplasia is a rare finding in patients, predominantly young males, transplanted for end-stage liver disease with unknown aetiology. Nonetheless, liver transplantation may have an important role in end-stage nodular regenerative hyperplasia-syndrome.
Keywords
Introduction
Nodular regenerative hyperplasia (NRH) is an uncommon condition of the liver which can cause intrahepatic portal hypertension in the absence of liver cirrhosis.1–3 Recently, it has been shown that NRH is frequently asymptomatic and that the histological diagnosis has to be distinguished from the NRH-syndrome, in which patients present with symptoms from portal hypertension. 4
The pathophysiology of NRH is still poorly understood, but seems to be related to alterations in the hepatic blood flow due to obliterative vasculopathy and/or secondary to damage of the sinusoids. 5 The development of NRH has been associated with a variety of systemic disorders including myelo- and lymphoproliferative diseases, autoimmune diseases, inflammatory and immunodeficiency disorders as well as certain medications. 6 Drugs associated with NRH are highly active anti-retroviral therapy, 7 platin-based chemotherapy 8 and thiopurines, in particular azathioprine (AZA) and thioguanine (TG).9–11
The diagnosis of NRH is challenging since the clinical presentation is variable and the majority of patients present without symptoms or abnormalities in laboratory parameters. 12 If symptoms are present, these are mainly due to portal hypertension, such as thrombocytopenia, oesophageal varices, splenomegaly and ascites. 13 Mildly increased liver enzymes, in particular alkaline phosphatase (AP), have been reported in one out of 10 patients. 6 Imaging methods, such as magnetic resonance imaging (MRI) and computed tomography (CT) could demonstrate nodularity and heterogeneous hepatic parenchyma suggestive of NRH. Nevertheless, diagnosis has to be confirmed with histological evaluation and a reticulin stain is necessary to characterise the transformation of the hepatic parenchyma into hyperplasia and atrophy. 14 Interestingly, the level of interobserver agreement on the histopathologic diagnosis of NRH is poor, even between experienced liver pathologists, confirming that NRH should be diagnosed using the combination of clinical presentation and histopathologic findings. 15
The clinical significance and prognosis, as well as the optimal management of NRH are still not completely clarified. In a large cohort study by Wanless in 1990, NRH was present in 64 of 2500 (2.6%) consecutive autopsies. 16 Among these 64 persons, only one had symptoms of portal hypertension and the other cases were asymptomatic. It seems that the prognosis in NRH patients is more related to the severity of the underlying condition than to liver involvement itself. 17 Therefore, treatment should be focused on the associated diseases and complications of non-cirrhotic portal hypertension (NCPH), in particular variceal bleeding which is the main cause of NCPH-related mortality.1,18
Liver transplantation might be indicated in NRH-syndrome and should be considered in patients with severe complications of NCPH or hepatic failure. 19 Frequently, it occurs that the diagnosis of NRH-syndrome is missed before transplantation and patients undergo liver transplantation due to a presumptive diagnosis of liver cirrhosis. 13 Overall, there is limited data available on the natural course of NRH and the role of liver transplantation as a treatment. Therefore, we aimed to determine the number of patients transplanted due to NRH-syndrome in a retrospective study in The Netherlands and to evaluate the indications and limitations of this treatment. Here, we describe the clinical characteristics of the patients and the histological features of the explanted livers affected with NRH.
Methods
Patient selection
In this retrospective database study we collected data from the three liver transplant units in The Netherlands; University Medical Center Groningen (UMCG) in Groningen, Erasmus University Medical Center (EMC) in Rotterdam and Leiden University Medical Center (LUMC) in Leiden. Access to the surgical pathology databases was obtained and the records of patients transplanted in the period from January 1995–April 2016 were searched for explanted livers diagnosed with either NRH, non-cirrhotic or cryptogenic liver disease on post-transplant histological evaluation. We included all adult patients in our initial analysis. Explanted livers with hepatic malignancy, hepatitis B/C virus infection, alcoholic liver disease, primary biliary tract disease, autoimmune hepatitis or metabolic liver diseases were excluded. Furthermore, cases of pre- and posthepatic (e.g. Budd-Chiari syndrome) portal hypertension were excluded. Cases with liver failure due to other causes of NCPH, such as hepatoportal sclerosis, perisinusoidal fibrosis or incomplete septal cirrhosis were excluded, unless NRH co-existed in the major part of the explanted liver. Cases with acute liver failure related to (recreational) drugs and medication were included.
Data extraction
Pre- and post-transplantation clinical, biochemical, radiological and histological information obtained from electronic and paper records were analysed. We collected data on demographics, clinical presentation, medical and surgical history and (historical) lifestyle (i.e. smoking and alcohol usage) of the patients. Biochemical parameters we collected were: haemoglobin (Hb), white blood cell count (WBC), platelet count (PC), alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (AP), gamma-glutamyl transferase (GGT), serum bilirubin, serum creatinine, prothrombin time (PT), international normalised ratio (INR) and Model for End-Stage Liver Disease (MELD) scores. Human immunodeficiency virus (HIV) serology was obtained. Further collected data were macro- and microscopic histological liver features related to NRH and characteristics of NCPH, defined as liver atrophy, heterogeneous parenchyma, presence of ascites, portal vein thrombosis, portosystemic collateral veins or splenomegaly at ultrasonography (US), CT or MRI. The use of potential hepatotoxic medications (e.g. thiopurines, platin based chemotherapy and highly active anti-retroviral therapy) was recorded.
NRH-syndrome
To distinguish histopathological diagnosis of NRH without symptoms of portal hypertension from patients with NCPH due to NRH, patients having symptomatic NRH are classified as having NRH-syndrome.
Histological analysis
Diagnosis of NRH was based on reports of the histological assessment of the explanted livers. The macro- and microscopic features of the liver were explored and searched for NRH characteristics as defined by Jharap et al. 15 The definitive diagnosis of NRH based on the histological reports was made by the pathologist at the liver transplantation centre.
Data analysis
Categorical variables were described as absolute and relative numbers. The continuous variables were described as mean ± standard deviation (for normal distribution) or median with range (for skewed distribution). Due to the (expected) low number of patients, no further statistical analysis was performed.
Ethical considerations
This study was approved by the Medical Ethics Review Committee (METC) of the VU University Medical Center (file number 2016-095).
Results
Patient characteristics
In the past 20 years, 1886 transplantations (UMCG: 660, EMC: 905 and LUMC: 321) have been performed in adult patients in the three Dutch liver transplant units. The database of the LUMC was initiated in 2000. A total of 255 transplanted patients (UMCG: 79, EMC: 128 and LUMC: 48) matched the inclusion criteria for this study and their charts were reviewed. NRH was histologically diagnosed in 11 patients (0.6%) (UMCG: seven, EMC: three and LUMC: one) (Figure 1).
Flowchart of patient selection. Post-transplantation diagnoses causing exclusion were: hepatic malignancy, hepatitis B/C virus infection, alcohol abuse, primary biliary tract disease, autoimmune hepatitis and metabolic liver diseases. EMC: Erasmus Medical Center Rotterdam; LUMC; Leiden University Medical Center; Tx: transplantation; UMCG: University Medical Center Groningen.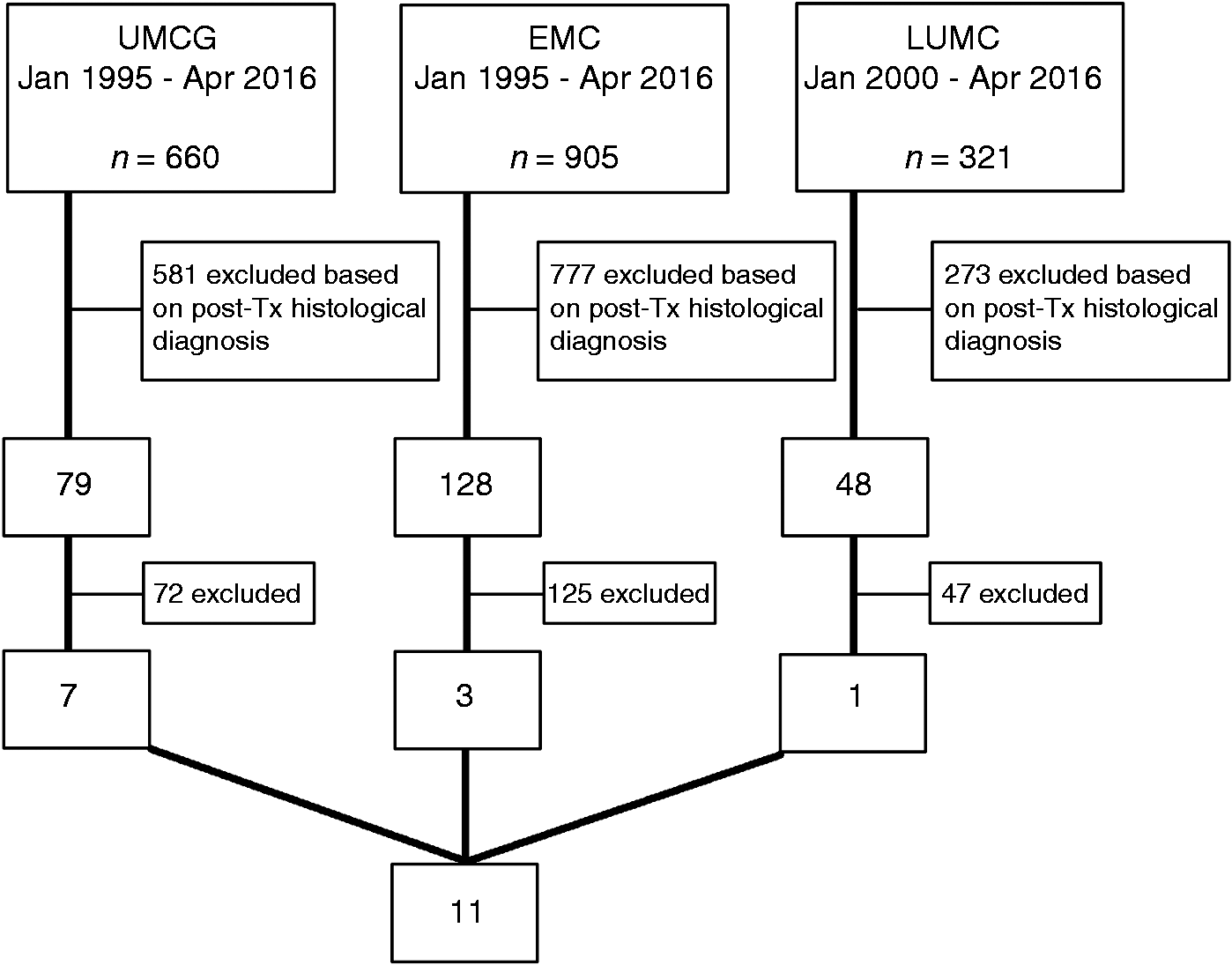
One of these 11 patients was re-transplanted 14 years after the initial liver transplantation, both times due to NRH-syndrome. In this study, we only describe the second liver transplantation, since the first transplantation was before 1995. One case has been published before. 20
Clinical findings in the patients with nodular regenerative hyperplasia (NRH) before orthotopic liver transplantation (OLT).
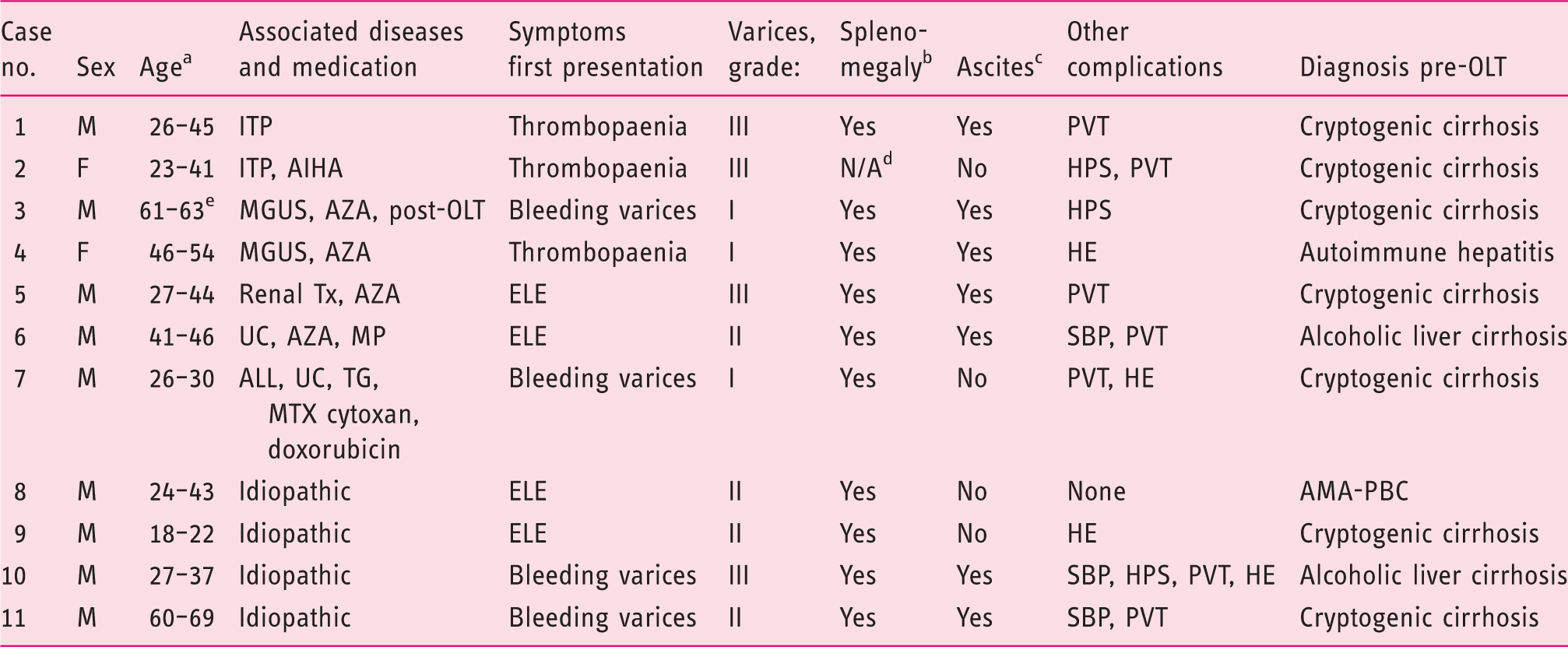
AIHA: autoimmune haemolytic anaemia; ALL: acute lymphoblastic leukaemia; AMA-PBC: antimitochondrial antibody-negative primary biliary cirrhosis; AZA: azathioprine; ELE: elevated liver enzymes; F: female; HE: hepatic encephalopathy; HPS: hepatopulmonary syndrome; ITP: immune-mediated thrombocytopenia; M: male; MP: mercaptopurine; MGUS: monoclonal gammopathy of undetermined significance; MTX: methotrexate; PVT: portal vein thrombosis; SBP: spontaneous bacterial peritonitis; TG: thioguanine; Tx: transplantation; UC: ulcerative colitis.
Age at first presentation and age of OLT; bsplenomegaly was defined as a longest diameter above 11 cm; cascites was evaluated using abdominal ultrasound; dthis patient underwent a splenectomy prior to the development of NRH; ethis patient underwent a liver transplantation for the second time due to NRH.
The pre-transplantation diagnosis was cryptogenic cirrhosis for seven patients (7/11; 64%), alcoholic cirrhosis for two patients (2/11; 18%), autoimmune hepatitis (AIH) for one patient (1/11; 9%) and one patient was diagnosed with antimitochondrial antibody (AMA)-negative primary biliary cirrhosis (PBC) (1/11; 9%).
Clinical presentation of the NRH patients
Four patients (4/11; 36%) had unexplained liver test abnormalities, four patients (4/11; 36%) were bleeding from gastro-oesophageal varices and three patients (3/11; 28%) had thrombocytopaenia at first clinical presentation (Table 1). Therapeutic management to treat the acute variceal bleeding was endoscopic band ligation (2/4; 50%) or sclerotherapy followed by a surgical portocaval shunt (1/4; 25%) or splenorenal shunt (1/4; 25%). During the pre-transplantation course, more complications of portal hypertension occurred in all patients. The most frequently occurring complications were gastro-oesophageal varices (11/11; 100%), splenomegaly (10/11; 91%), portal vein thrombosis (7/11; 64%), ascites (7/11; 64%) and hepatic encephalopathy (4/11; 36%). Furthermore, three patients had spontaneous bacterial peritonitis (3/11; 28%) and three patients developed hepatopulmonary syndrome (HPS, 3/11; 28%), which is an important cause of dyspnoea and hypoxia in the setting of end-stage liver disease.
Diseases and drugs associated with NRH
An associated disease and/or drug use with NRH was observed in seven of 11 patients (7/11; 64%), of which five patients (5/11; 45%) were treated with thiopurines. These seven patients together had a median age of 27 years (23–46 years) when first liver symptoms developed and a median age of 44 years (30–54 years) when orthotopic liver transplantation (OLT) was performed. Patient #3 underwent OLT for the second time, both times due to NRH-syndrome. After first OLT, this patient was treated with AZA for nine years and eventually developed liver failure 14 years after initial OLT. Patient #4 was previously diagnosed with autoimmune hepatitis (AIH) and was treated with AZA 150 mg/day for six months before manifestation of NRH-syndrome. Revision of the histology did not confirm AIH, and AZA was subsequently discontinued. The remaining four patients (36%) were neither diagnosed with an associated disease nor treated with hepatotoxic drugs and presumably developed idiopathic NRH. Three of them (#8–10) were transplanted at a median age of 37 years (22–43 years).
Biochemical and imaging results in the NRH patients
Laboratory and imaging findings in the patients with nodular regenerative hyperplasia (NRH) before orthotopic liver transplantation (OLT).
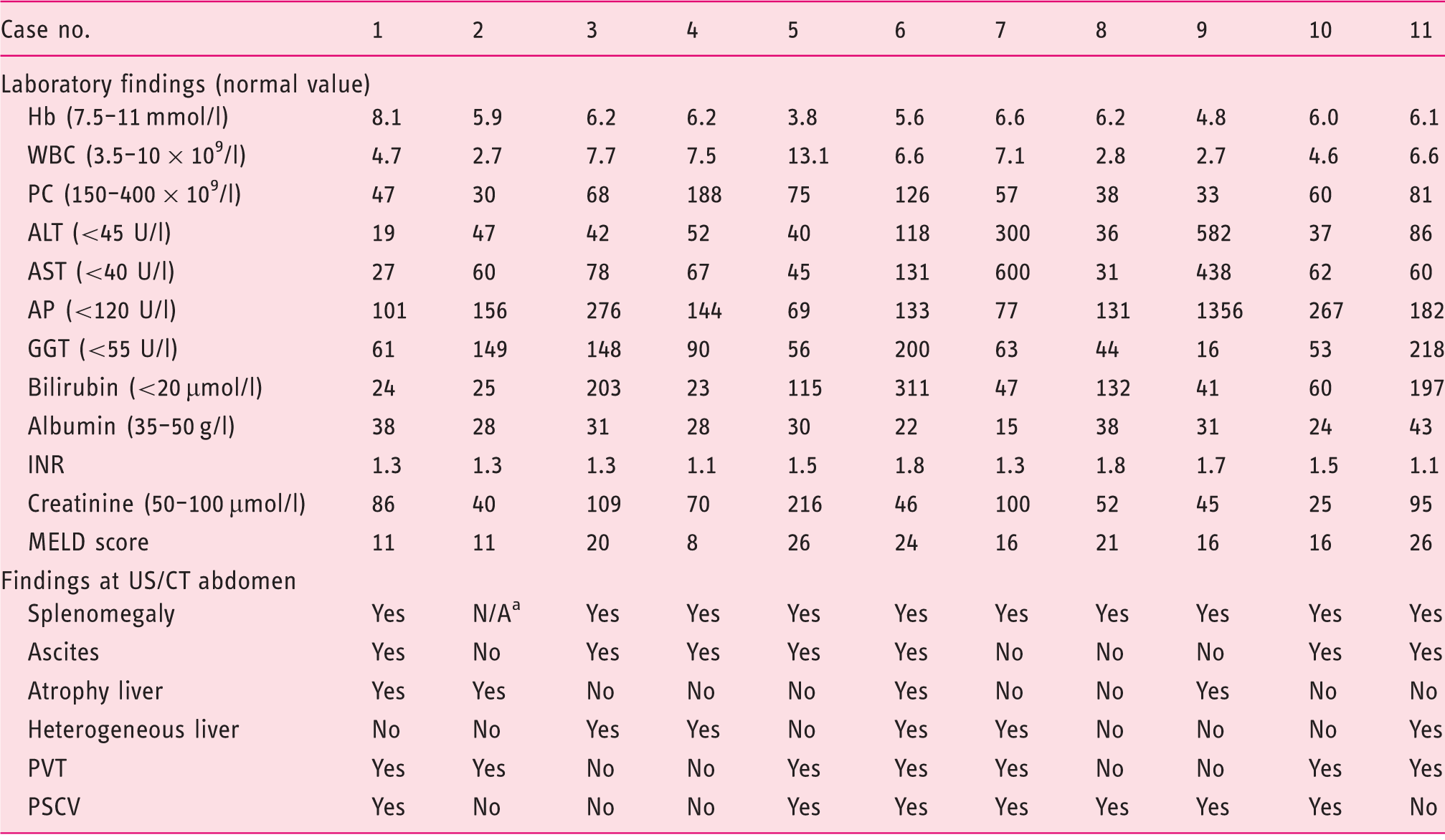
ALT: alanine aminotransferase; AP: alkaline phosphatase; AST: aspartate aminotransferase; CT: computed tomography; GGT: gamma-glutamyl transferase; INR: international normalised ratio; Hb: haemoglobin; MELD: Model for End-Stage Liver Disease; N/A: not applicable; PC: platelet count; PSCV: portosystemic collateral veins; PVT: portal vein thrombosis; US: ultrasonography; WBC: white blood cell count.
This patient had a splenectomy in the surgical history.
The MELD scores at time of referral for OLT varied from 8–24 with a median of 18. In all patients Hepatitis B virus (HBV), Hepatitis C virus (HCV) and HIV serology, rheumatoid factor, protein C and antibodies for autoimmune liver diseases were negative. Furthermore, levels of ferritin, copper, α-foetoprotein and α1-antitrypsin were within normal limits.
In the pre-transplantation course, signs of portal hypertension were observed by imaging methods in all patients, but NCPH and/or NRH was not diagnosed in any of the patients by the radiologist (Table 2). The most frequent characteristics of portal hypertension, detected at US or CT were splenomegaly (10/11, 91%), portal vein thrombosis (7/11, 64%), portosystemic collateral veins (7/11, 64%), ascites (7/11, 64%), heterogeneous liver parenchyma (5/11, 46%) and an atrophic liver (4/11, 36%).
Histological analysis of the explanted livers
Histopathological findings in the livers at liver biopsy and orthotopic liver transplantation (OLT).
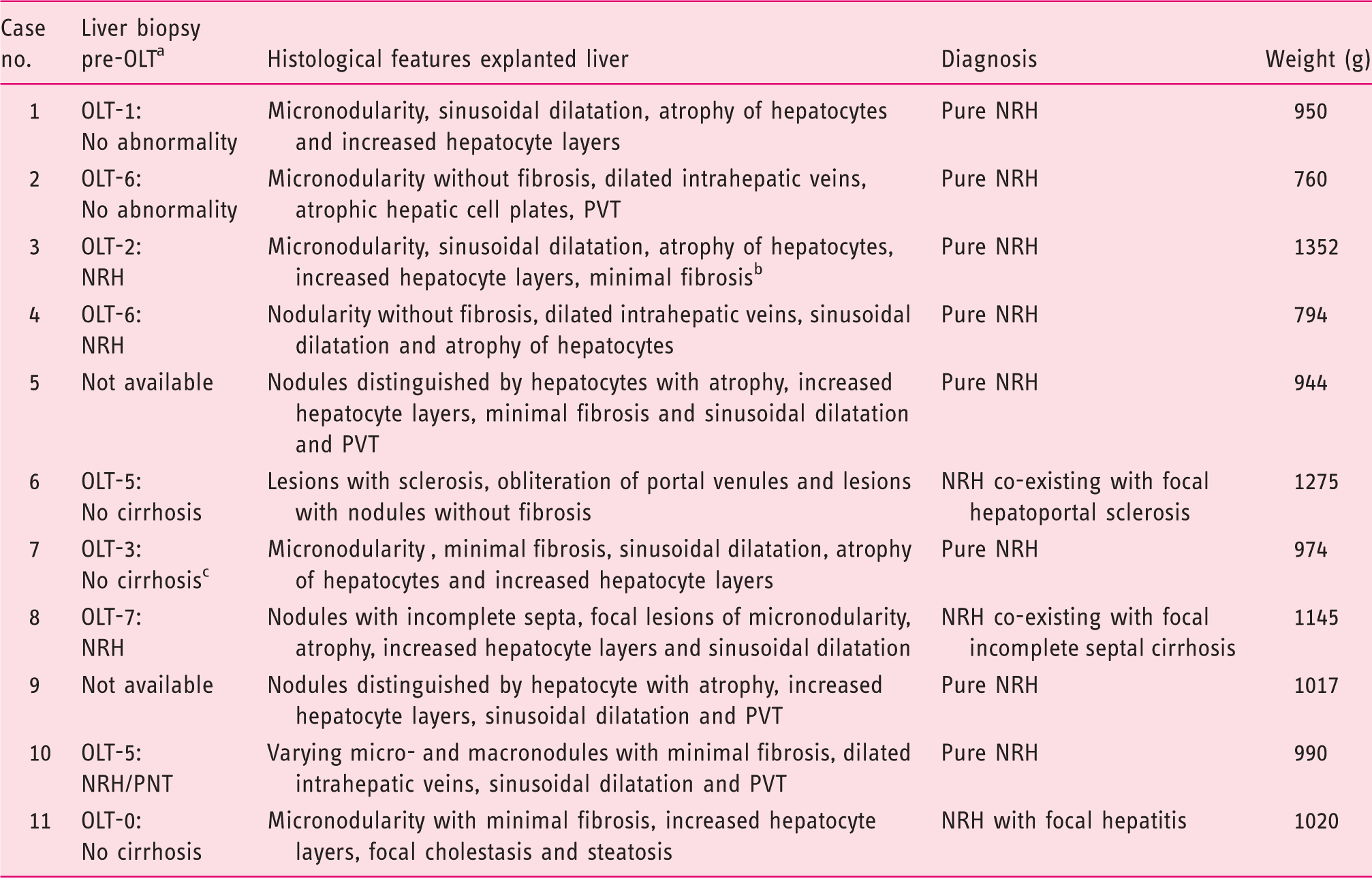
NRH: nodular regenerative hyperplasia; PNT: partial nodular transformation; PVT: portal vein thrombosis.
OLT-x: x = number of years between the time of liver biopsy and OLT; bpatient with re-transplantation due to NRH, the same histological features were seen in the first as second explanted liver; cthis patient was treated with methotrexate for acute lymphoblastic leukaemia, there were no signs of liver damage due to methotrexate in particular.
Histopathological examination of the explanted livers was performed in all 11 cases. Histological criteria of cirrhosis was lacking in all explanted livers. Explanted livers were atrophic with a mean weight of 1020 ± 110 g. In liver #6 NRH co-existed with focal hepatoportal sclerosis and in liver #8 NRH co-existed with focal incomplete septal cirrhosis. The other nine livers (9/11; 82%) were diagnosed with pure NRH. Dysplasia or neoplasia was not reported in any of the explanted livers.
Post transplantation; mortality and follow-up
The post-transplantation course in the patients with nodular regenerative hyperplasia (NRH).
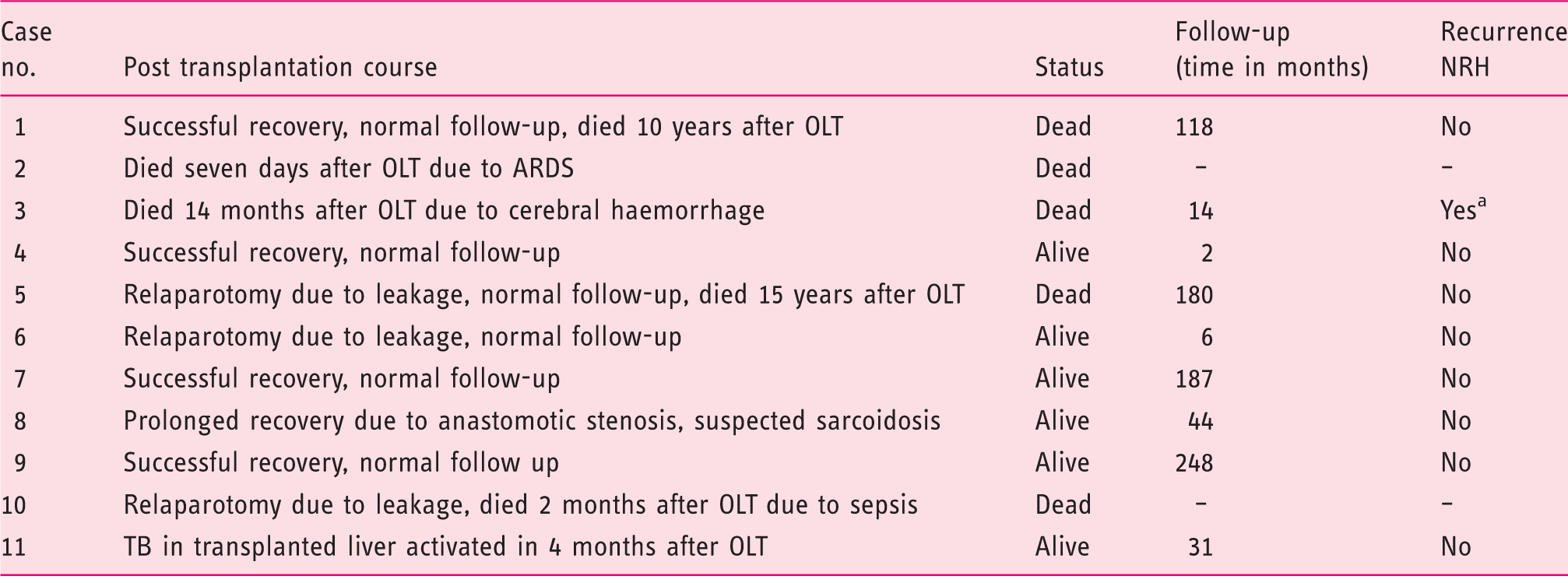
ARDS: acute respiratory distress syndrome; OLT: orthotopic liver transplantation; TB: tuberculosis.
This patient had a recurrence of symptomatic NRH at 14 years after first liver transplantation, there was no recurrence of NRH after second OLT.
During the follow-up, no acute rejection was observed in any of the patients. Recurrence of severe NCPH complications did occur in patient #3 due to NRH, 14 years after initial OLT. In the 14 months after his second OLT, no recurrence of liver disease has been observed. Complications of NCPH did not re-occur in the other patients, nor was histological recurrence of NRH observed in the patients who underwent liver biopsy.
Discussion
This is the largest study reported to date, describing the number of patients transplanted due to NRH-syndrome in a 20-year cohort study amongst all liver transplant centres in the Netherlands. Out of 1886 performed liver transplantations, records of 255 patients who underwent OLT for NRH, non-cirrhotic- or cryptogenic liver disease were scrutinised. Eleven patients with NRH on histological evaluation of their explanted livers were identified, suggesting a percentage of 0.6% of liver transplantations due to NRH-syndrome based on nationwide pathology data.
We reported clinical, biochemical, radiological and histological findings of 11 patients and their explanted livers. A male predominance (9/11; 82%) with a median age of 44 years at OLT was detected, similar to the numbers which are reported on NRH and liver transplantation in the literature.21–23 This male predominance in severe NRH-syndrome needing OLT has been reported before, however the explanation remains unclear. All our presented patients had a progressive clinical course including severe complications of NCPH. The abnormalities in biochemical and imaging studies were not suggestive for NCPH or NRH and all of our patients were presumed to have liver cirrhosis in the pre-transplantation course. The majority of our patients (55%) did not have elevated liver enzymes, but anaemia (91%) and thrombocytopaenia (91%) were present in almost all of them. Six patients (55%) had portal vein thrombosis alongside NRH, which is consistent with other reports showing coagulation disorders in NRH patients. 24
Published studies on patients transplanted due to nodular regenerative hyperplasia (NRH) and their patient characteristics.
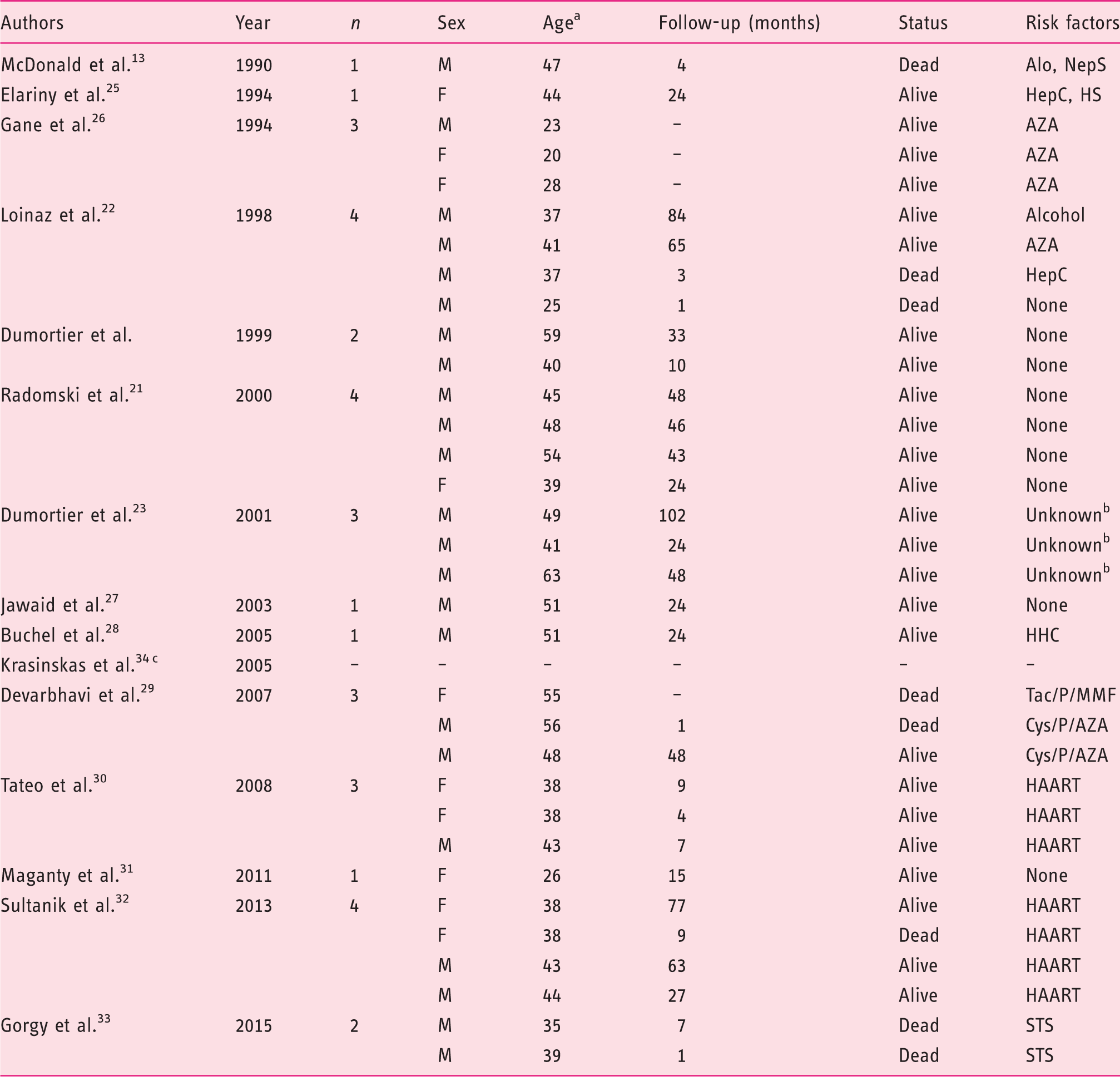
Alo: alopecia totalis; AZA: azathioprine; Cys: cyclosporin; F: female; HAART: highly active anti-retroviral therapy; HepC: chronic hepatitis C infection; HHC: hyperhomocysteinaemia; HS: haemosiderosis; M: male; MMF: micophenolate mofetil; NepS: nephrotic syndrome; P: prednisone; STS: short telomere syndrome; Tac: tacrolimus.
This table is modified from the systematic review on liver transplantation for NRH by Manzia et al. 19 and completed till April 2016 with the studies by Maganty et al., 25 Sultanik et al., 26 Gorgy et al. 27 and Krasinkas et al. 28
Age at time of liver transplantation; brisk factors not mentioned in article; cthis study was neither included in the systematic review by Manzia et al., nor in our analysis due to the lack of significant data.
The MELD score at referral for OLT was highly variable and varied from 8–24, without predicting progression and severity of NRH-syndrome, probably due to the fact that liver synthesis function in NRH patients remains normal in severe NRH, which was underlined in the systematic review on liver transplantation for NRH by Manzia et al. 19 before. One of the suggestions for further research is to determine mortality in NRH patients on the waiting list for liver transplantation, to justify modifying the MELD score for NRH patients.
Histological NRH is associated with several autoimmune diseases and drug exposure. Interestingly, not all patients in our cohort had a medical history of diseases and/or drug use related to NRH and we presume that NRH occurred idiopathically in some of the patients (36%). Five patients (45%) were treated with chemotherapy and thiopurines, in line with other reports.10,11,35 In one of these studies, an NRH incidence rate of 62% in patients treated with high-dose TG was reported and it was concluded that TG should not be considered as a therapy for patients with inflammatory bowel disease (IBD). 10 However, in some studies, it was shown that the formation of NRH appears to be dose dependent and that histopathological liver abnormalities are relatively common in IBD patients, even without exposure to thiopurines.36–38 Lastly, two of our patients were known with immune-mediated thrombocytopenia (ITP) without exposure to thiopurines or other NRH-related drugs, a relation which has been described previously. 39
One of the limitations of our study design is the fact that we recruited our patients based on the histological evaluations made by the pathologists on location in the participating centres. Whereas all our included patients had symptoms of portal hypertension, the histological diagnosis of NRH remains challenging due to different interpretations of histological features by pathologists, as demonstrated in a study by Jharap et al. 15 For our study, we did not histologically reassess the explanted liver specimens of our patients. Reviewing the liver specimens by an experienced pathologist would improve the methodological power of this study.
In our study, we determined a small number (0.6%) of patients transplanted due to NRH-syndrome, which is lower than reported in several other studies, especially in thiopurine users.10,11,35 Many of these studies reported the incidence rate of histological NRH, which was not associated with a clinically significant liver disease.4,40 However, our study is not comparable to these studies since we only assessed patients with a clinically significant liver disease needing OLT. Nevertheless, some patients with NRH-syndrome are appropriate candidates for liver transplantation, but may have absolute or relative contraindications for OLT. These individuals were not included in our study, probably leading to selection bias and an underestimation of the incidence of disease.
Conclusion
In conclusion, a small number of patients, predominantly young males, were transplanted due to severe NRH-syndrome, concluding that this is a rare treatment indication for liver transplantation. The clinical manifestation of progressive NRH-syndrome is mainly revealed by severe complications of portal hypertension. Furthermore, non-specific abnormalities in laboratory parameters and imaging studies could reveal the presence of NRH. Whilst it is known that NRH is associated with several diseases and drugs, the diagnosis should also be considered in patients without a related medical history. Liver transplantation may have an important role in NRH-syndrome but vigilance is required, especially in patients suffering from HPS and other severe portal hypertension complications.
Footnotes
Acknowledgements
NdB designed and was the guarantor of the article. RdM, MC, HB, GD and MS collected the data. BM and MS drafted the first manuscript of the article. RdM, MC, HB, GD, CvN, CM and NdB critically revised the manuscript. BM completed the manuscript after author’s revisions. All authors agreed to the final version of the manuscript.
Conflicts of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.