
Abstract
Background
Cirrhosis represents the end stage of chronic liver disease, characterized by high mortality and morbidity. The prevalence of liver disease is difficult to assess, given its clinical latency up to the late stage.
Objective
We aimed to assess the prevalence of unrecognized chronic liver disease and cirrhosis using surrogate indicators from medical records of family physicians.
Methods
Medical records of 139,104 subjects, collected from 99 family physicians of the Veneto region, were used. Persistently high transaminases were used as indicators of occult chronic liver disease; thrombocytopenia, unrelated to haematological malignancies, was used as indicator of occult cirrhosis. Diagnosis of chronic liver disease and cirrhosis was assessed using ICD9-CM-1997 codes.
Results
Alteration of transaminases was found in 32.7% of the subjects, and among them only one-third had an already diagnosed liver disease. Patients with diagnosis of cirrhosis were 0.3%, while thrombocytopenia, indicator of occult cirrhosis, was detected in 1.3% of the remaining population. Patients with overt and occult cirrhosis showed a higher metabolic profile, with significantly higher prevalence of arterial hypertension, obesity and diabetes than the general population.
Conclusion
A large proportion of patients with chronic liver disease is still undiagnosed. Surrogate biochemical indicators might be useful for disease recognition.
Keywords
Introduction
Chronic liver disease and liver cirrhosis are among the leading causes of morbidity and mortality in many developed countries. 1 Deaths from liver cirrhosis and liver cancer have increased by more than 30% and 50%, respectively, over the past two decades. 2 Liver cirrhosis accounted for 1.2% of global disability-adjusted life years with a nearly equal share related to hepatitis B and C virus infections and alcohol. 3 Nevertheless, the actual prevalence of cirrhosis is difficult to assess and probably higher than reported because the course of chronic liver disease is usually long and asymptomatic 4 and, as a result, often goes undiagnosed. 5 Indeed, only 60% of patients with cirrhosis show signs or symptoms of liver disease, while the remaining 40% are discovered occasionally during routine testing or autopsy. 6 Since compensated cirrhosis often goes undetected for extended periods, a reasonable estimate of up to 1% of the population could have histological cirrhosis. 7 These data concur with recent observations that many patients had ongoing advanced liver disease upon their initial chronic hepatitis C diagnosis, which is associated with higher costs and diminished health benefits, despite multiple involvements with the healthcare system over the years, and resulting in high hospitalization and mortality rates. 8 The main causes of cirrhosis are infection by hepatitis B and C viruses, alcohol misuse, and non-alcoholic liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH). 1 NAFLD and NASH have become major causes of liver disease in Europe in the past few decades, 5 with prevalence estimates ranging from 25% to 45% in most studies, with a parallel increase of obesity and diabetes. 9
To date, limited studies reported reliable epidemiological data of chronic liver disease and cirrhosis in the general population. A prospective cohort study, published 1994, reported the prevalence of chronic liver disease in the general population of two towns in Northern Italy. 10 In this study 17.5% of the subjects were found with persistently abnormal liver tests and the prevalence of cirrhosis was 1%, which was higher than expected. 10 A more recent screening of French males with no history of liver disease provided a prevalence of liver cirrhosis of 0.3% and of liver fibrosis of 0.7–1.4%, when assessed with non-invasive techniques. 11 The most common attributable cause of liver fibrosis in this study was NAFLD associated or not with alcohol abuse. 11 In another community-based population study, using transient elastography, liver cirrhosis was detected in 0.7% of apparently healthy subjects and NAFLD was the most frequent cause of intermediate fibrosis.12,13 The analysis of recorded cirrhosis or portal hypertension in a UK general practice research database revealed a 68% increase in the prevalence of the disease from 1993 to 2001. 13
Updated epidemiological data on the prevalence of liver disease burden in Italy are lacking, and no data on the estimation of occult liver disease are available to date. The purpose of the present study was to estimate the prevalence of still-undiagnosed liver disease in the Veneto region, in order to provide data that might help to plan more accurate policies for primary and secondary liver disease prevention.
Methods
Epidemiological analysis
For the epidemiological analysis, a general practitioners’ database (MilleinRete dataset), consisting of anonymous computerized primary care records of 139,104 subjects, was used. Data contained within this database, including diagnosis, clinical test results, observations, prescriptions and major medical events, were recorded through direct entry, during face-to-face general practice appointments and also following information received from secondary care, including hospital letters and discharge summaries. Medical records were stored by 99 general practitioners distributed among 86% of Veneto region districts, from 1 January 2011 to 31 December 2011. In order to ensure a representative sample, we matched the standardized prevalence of some chronic diseases obtained from general practitioners’ dataset with the records available at the regional epidemiological centre database (Health Search – CSD LPD), subject to various rigorous validation procedures (VII Health Search report, 2012) (Supplemental Figure 1) with sex and age distribution overlapping the adult Italian general population.
The general practitioners who contributed to the MilleinRete database have shown higher performance in indexing medical records than those affiliated with the Italian Health Search database, as confirmed by the ITOT index (0.74 vs. 0.72, respectively).
Surrogate markers of overt liver disease
ICD9-CM-1997 (International Classification of Diseases) sanitary codes were used to identify patients with already diagnosed acute or chronic liver disease. Alcohol abuse was defined by ICD9 codes or with recorded alcohol consumption higher than 36 g/day. ICD9-CM-1997 codes relative to the presence of acute and chronic hepatitis of viral or non-viral origin and of hepatic steatosis were used (Supplemental Table 1). Viral aetiology was defined using the positivity for HCV-RNA, HCV antibodies or the HBsAg positivity in the dataset. Body mass index was calculated as weight (kg)/height (m2). Arterial hypertension and diabetes mellitus were diagnosed following international validated criteria. 14 Overt chronic liver disease was defined by the combination of ICD9 codes and/or recorded important alcohol consumption and viral infection by hepatotropic viruses. Overt cirrhosis was defined using ICD9-CM-1997 codes for liver cirrhosis and its complications (Supplemental Table 1). The Charlson Comorbidity Index 15 was calculated in the general population and in patients with diagnosis of liver cirrhosis.
Surrogate markers for occult liver disease
As indicator of occult chronic liver disease, elevation of transaminases more than 1.5 time normal values at least in two occasions (with an interval of at least 1 month) was considered, in agreement with previous studies.4,16 Taking into account that patients with thrombocytopenia due to haematological disorders were excluded from the analysis, thrombocytopenia (platelet count <120,000/μl) was chosen as indicator of occult liver cirrhosis.
Statistical analysis
The prevalence of overt and occult chronic liver disease, cirrhosis and its comorbidities was calculated by dividing the number of affected people by the number of all the subjects tested in the control population. The Chi square test for categorical variables and the Student’s t tests for continuous data were used.
Data analyses were performed with a SPSS PC statistical package (SPSS, Inc., Chicago, IL). All reported p-values are two-tailed.
Results
Prevalence of liver disease and epidemiological characteristics of patients included in the study.

Overt cirrhosis and overt and overt chronic liver disease (CLD) were classified by ICD9-CM-1997 codes; occult cirrhosis was defined as platelet count <120,000 μ/l; occult chronic liver disease (CLD) was defined as transaminases above 1.5 normal values.
Overt and occult CLD vs. overt and occult cirrhosis: p < 0.0001.
When comorbidities typically associated with metabolic syndrome were considered, patients with overt cirrhosis showed higher prevalence of overweight and obesity (71.6%), diabetes mellitus type II (38.3%) and arterial hypertension (58.1%) than the overall population, and similar features were also observed in patients with occult cirrhosis (Figure 1).
Prevalence of comorbidities related to metabolic syndrome. Prevalence of overweight and obesity, diabetes mellitus type II and arterial hypertension in patients with overt and occult cirrhosis and in overall population.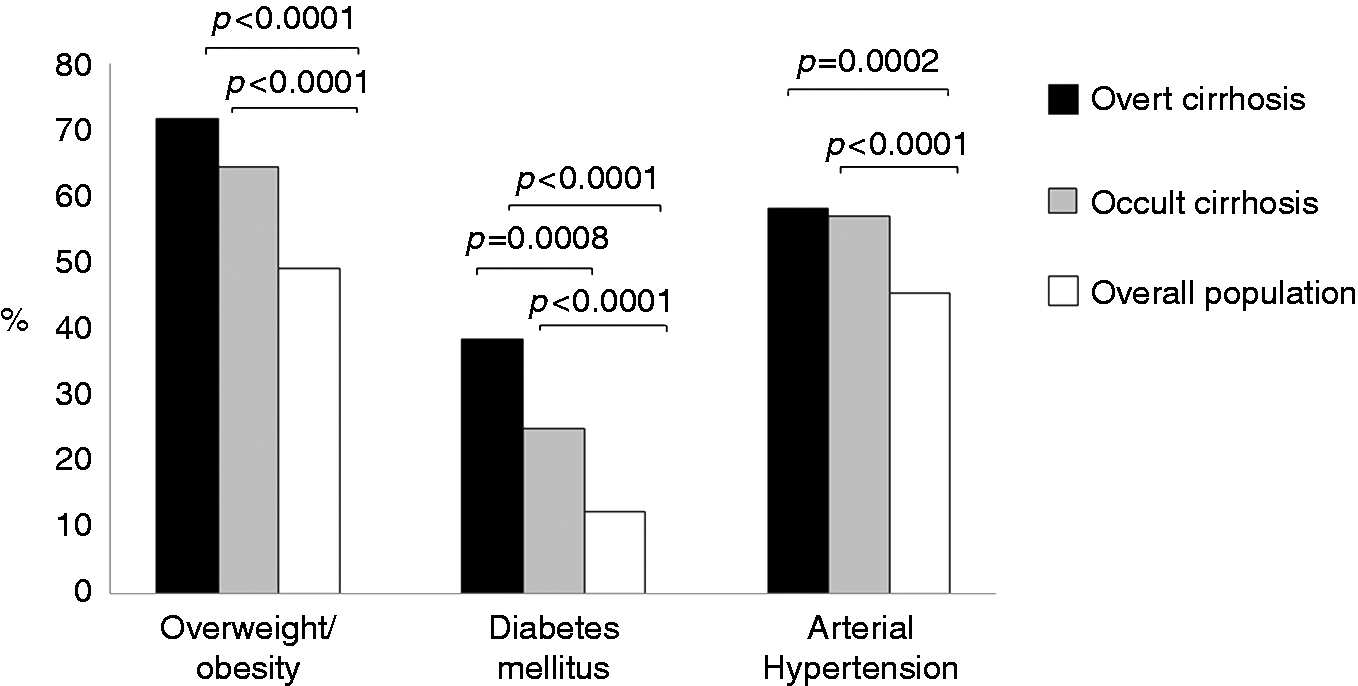
Discussion
Chronic liver disease is often undiagnosed, due to its asymptomatic course, and its real prevalence is still underestimated.17,18 Moreover, it has been shown that at least 50% of patients with chronic liver disease are not aware of their status, and therefore they cannot receive appropriate treatment. 18 For these reasons medical records stored by general practitioners might be a useful tool to achieve real-life data of the general population. 13
In this study we have compared, for the first time, the prevalence of patients with overt diagnosis of chronic liver disease and cirrhosis with the estimated prevalence of patients with not yet recognized liver disease, using surrogate indicators from a general practitioners’ dataset of a large general population. Our findings have shown that the burden of chronic liver disease is at least two times higher than that currently recorded, and the difference between the real and the estimated diagnosis of liver cirrhosis is even higher.
According to our data, among subjects with recorded transaminases, 65% of the patients with elevated transaminases did not have a recorded diagnosis of liver disease. This finding is well in keeping with Clark et al., who showed that elevation of aminotransferases was unexplained in the majority (69%) of apparently healthy subjects. 16 This surrogate marker, despite its limitations, has been tested in previous studies, showing very high sensitivity and specificity to identify patients with chronic liver disease.4,16 Moreover, in the study of Pendino et al., 4 more than two-thirds of the subjects with initial alteration of transaminases showed a persistent alteration at the second assessment, undertaken at a range of 3–36 weeks after the first screening. In our study, although we cannot exclude causes other than chronic liver diseases, such as simple infection with hepatic involvement, this surrogate marker was sufficient to define a population of subjects with epidemiological characteristics similar to that of the patients with overt chronic liver disease.
In relation to the prevalence of occult liver cirrhosis, we assumed that thrombocytopenia was an indicator of occult liver cirrhosis, taking into account that patients with thrombocytopenia due to haematological disorders were excluded from the analysis. This criterion was selected for two main reasons: (a) platelet count is one of the parameters more frequently measured in routine blood tests, and (b) thrombocytopenia occurs frequently in advanced stages of chronic liver disease as a result of portal hypertension, 19 as confirmed in a recent work showing that thrombocytopenia was present in 73% of the patients with cirrhosis. 20 Using this approach, we found a prevalence that was four-fold higher than that of currently recorded cirrhosis. Prevalence of overt and occult cirrhosis detected in our study was comparable with previous reports.7,10-12 In addition, patients with overt and occult cirrhosis had a similar epidemiological profile, since age and sex distribution were almost identical.
This finding has important health and social implications for three main reasons: (a) liver cirrhosis has a deep negative impact on survival and quality of life; (b) we are dealing mainly with males still of working age; (c) liver cirrhosis is often associated with comorbidities with a consequent higher need of care. 15
Looking at the potential aetiology, in patients with occult cirrhosis as well as in those with overt cirrhosis, we found a higher prevalence of diabetes, arterial hypertension and obesity than that detected in the overall population. In agreement with these findings, in a recent large study a strong relationship was reported between liver fibrosis and metabolic comorbidities. 21
Our study has some methodological limitations, such as: (a) its retrospective nature, (b) thus use of a pre-existing dataset where only 25% of the subjects had transaminase values recorded in their medical records, and (c) the need to confirm the accuracy of our biochemical approach to detect still unrecognized chronic liver disease and cirrhosis by more accurate biochemical profiles and by imaging techniques. Nevertheless, the strengths of this study encompass: (a) the use of already available data on a large number of subjects, not requiring additional tests for the patients and costs for the health care system, (b) the reproducibility of the obtained data, compared with previous studies, 21 and (c) the easy feasibility of the approach that, however, requires close collaboration between the general practitioner and the hepatologist.
In conclusion, this study demonstrates that a large proportion of patients with chronic liver disease is still undiagnosed. Surrogate biochemical indicators might be useful for liver disease recognition in apparently healthy subjects that could benefit from the correction of identified risk factors and from suitable treatment strategies, when indicated.
Footnotes
Acknowledgements
The authors are deeply grateful to Dr. Alessandro Battaggia, scientific manager of the MilleinRete dataset and to Dr. Bruno Franco Novelletto (Italian Society of General Medicine, SIMG, and Venetian School of General Medicine, S.Ve.M.G) for their invaluable contribute in the acquisition of epidemiologic and clinical data.
Declaration of conflicting interests
None declared.
Funding
This study was supported in part by a grant from the National Ministry of Health (Project Code: RF-2009-1492312).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.