
Abstract
Background
Studies have found an association between proton pump inhibitor (PPI) use and Clostridium difficile infection. The purpose of this study was to determine whether the mechanism by which PPIs induce an increased risk of C. difficile infection is supported by the same mechanism acting in another cause of achlorhydria, pernicious anaemia.
Methods
Using a database of anonymised primary care records between 1990 and 2013, we selected exposed patients with a diagnosis of pernicious anaemia treated with vitamin B12 therapy. Each exposed patient was matched by age, gender and general practice to up to 10 controls. Cox regression analysis was used to estimate the hazard ratio (HR) and 95% confidence interval (CI) for C. difficile infection with pernicious anaemia, adjusted for potential confounders.
Results
We identified 45,467 exposed patients matched to 449,635 controls. The crude incidence rate of C. difficile infection was 1.85/1000 person-years for the exposed cohort and 1.09/1000 person-years for controls. Patients with pernicious anaemia had a greater risk of C. difficile infection than the controls (adjusted HR 1.57, 95% CI 1.40–1.76).
Conclusions
Pernicious anaemia patients have an increased risk of C. difficile infection. This supports the theory that severe achlorhydria is the mechanism that increases the risk of C. difficile infection in long-term PPI users.
Introduction
Clostridium difficile infection is the most commonly identified cause of nosocomial and community associated diarrhoea.1–3 Although exposure to antibiotics, advanced age and hospitalisation have been recognised as risk factors for C. difficile infection, 3 recent evidence has described C. difficile infection in populations that lack these traditional risk factors.4,5 Prior studies have suggested that acid-suppressing medication, in particular proton pump inhibitors (PPIs), may cause a risk of C. difficile infection.6–10 A meta-analysis reported a 65% increase in the incidence of C. difficile infection among PPI users. 11 Although the current observational studies mainly focused on the studying the association between C. difficile infection and the use of PPIs, the precise mechanism of this association has remained elusive.
Previous studies have found that PPIs, which act by reducing acid secretion, influence upper and lower gastrointestinal intestinal microflora and potentially increase a patient’s susceptibility to enteric infection. 10 Although this mechanism seems widely acceptable, it has not been conclusively proven and other studies have found that C. difficile spores, which are the major mode of transmission of C. difficile infection, are acid resistant. 10 In addition, emerging evidence suggests it is other factors within patients who are prescribed PPI, rather than the PPI itself that are responsible for the increased risk of other gastrointestinal infections in those patients. 12 It remains unclear, therefore, if the reduction in acid secretion (achlorhydria) in patients who use PPI on a long-term basis is an independent risk factor associated with the increased risk of C. difficile infection, or whether potential confounders, such as comorbidities, can explain the observed associations.
The chronic and persistent achlorhydria observed in long-term PPI users is, at least, as marked as that generally associated with pernicious anaemia patients who also exhibit achlorhydria (the absence of hydrochloric acid in the gastric secretions). Herein, the achlorhydria observed in pernicious anaemia was applied to bridge the gap in understating of the casual mechanisms that are at play in the relationship between using PPI and C. difficile infection. The primary objective of the study was to determine whether people with pernicious anaemia are more likely to develop C. difficile infection than those without it. Demonstrating this association would provide further evidence that the achlorhydria induced by acid-suppressing medications could directly cause the increased risk of C. difficile infection in patients who receive them.
Methods
Data source and study design
We performed a matched cohort study using routinely collected electronic healthcare data from UK primary care practices that were extracted from the Clinical Practice Research Datalink (CPRD).13,14 This database consists of anonymised primary care records from around 681 participating practices, and the data included in it represent around 7% of the UK population. The data within CPRD includes information on patients’ demographics, clinical diagnosis, drug prescription, investigation history, and any referral. 13 More than half of the records contained within the CPRD are linked to secondary care data in the Hospital Episode Statistics (HES) database. The HES data include records of all hospital admissions along with the primary and secondary diagnosis coded using ICD-10 for each admission, date of admission, and discharge status. 15
Study population
We identified all individuals with an acceptable registration status within the CPRD from 1990 to 2013 who had at least one year of active registration following the date of current registration or the date the practice became ‘up to standard’ (UTS) on CPRD, 13 whichever was the latest. We identified within these a subgroup of patients for whom linked HES data was available to increase the sensitivity of detecting outcomes by including hospital data. Within this subgroup we used both CPRD and HES data to define the cases and outcome events where the first diagnosis recorded in either data source was selected as the event date. For this subset, the follow-up period was also modified to ensure it was consistent with the linkage coverage period from 1997 to 2012.
Identification of exposed and unexposed cohort
From the list of eligible patients, we selected adult patients who had a coded diagnosis of vitamin B12 deficiency anaemia or pernicious anaemia and who had been prescribed concurrent vitamin B12 therapy, the current standard of care for this condition. We excluded patients from the exposed cohort who were receiving vitamin B12 therapy, but had a pre-existing alternative aetiology, such as gastrectomy, intestinal resection, generalised malabsorption, or PPI use. PPI use was considered to be the indication if the date of the B12 prescriptions fell within the period of continuous use of PPI prior to cohort entry. The start of follow-up for the exposed group was the date of diagnosis or the first date of UTS prospective data if the UTS date was later than the date of diagnosis.
Ten unexposed patients for each case were randomly matched for age (within five years), gender, general practice, and the start date of follow-up with a matched exposed patient. All patients that met the inclusion criteria for the exposed cohort group, and all those who were receiving vitamin B12 prescriptions for indications other than pernicious anaemia, were excluded from the control group.
The end of the follow-up was defined as the date of the first outcome event on record, the date of the patient’s exit from the database, or the last download from their practice (whichever was the earliest). Patients were censored if they developed one of the alternative aetiologies after commencing vitamin B12 therapy. If the patients issued PPI prescription after the cohort entry and B12 prescription date fell within continuous use of PPI, they were censored on the date of the PPI prescription.
Outcome and covariates
We defined C. difficile infection in the CPRD by the presence of a clinical diagnosis of C. difficile infection codes recorded in the medical record by the general practitioner and/or positive C. difficile toxin assay. We used information from both primary care and HES data in the subgroup of patients with available linked data to additional outcomes with an ICD code (A04.7 for C. difficile colitis). The first C. difficile diagnosis recorded in either data source was considered to represent the event date.
The following variables were considered as potential confounders: socioeconomic status (using individual IMD quintiles), comorbidity as measured by the Charlson index, 16 smoking, hospitalisation and the use of acid-suppressing medication, immunosuppressant drugs, antibiotics and corticosteroids. As it is likely that there will be non-random missing data particularly for smoking, we will model ‘missing’ as a separate category.
Statistical analyses
Descriptive analyses were carried out to compare the baseline characteristics between cases and control groups. A two-sided likelihood ratio chi-square test was used to analyse the categorical variables. We carried out a multivariable Cox regression analysis to estimate the hazard ratio (HRs) and 95% confidence interval for the risk of C. difficile infection (first failure) in the exposed cohort compared to the unexposed cohort. We checked for violation of the proportional hazards assumption in these models via log–log plots and Stata’s estat phtest command.
Use of antibiotics and hospitalisation were included in the multivariate model as a priori,17,18 and other potential confounders were entered if they were significantly associated with the outcome in univariate analysis (p ≤ 0.05), and retained in the final model if their inclusion altered the apparent effect size of the univariate Cox model by at least 10%. We considered drug exposure variables as time-varying covariates (acid-suppressing medication, use of immunosuppressant drugs, antibiotics and corticosteroids). Specifically, each patient's follow-up time was first converted into year-long blocks of time, and the drug exposure status was then determined for each yearly block. Medical comorbidities were measured at baseline, and categorised using the Charlson index derived from primary care data. 19
All statistical analyses were performed using STATA 12.0 (College Station, TX)
Sensitivity analyses
In order to assess the robustness of our results, we carried out the following sensitivity analyses. First, to ensure that the results were not altered by any survival bias in cases, we restricted the analysis to the subgroup of exposed patients who were diagnosed with pernicious anaemia for the first time with at least one year of follow-up in CPRD within the study period. In addition to ensure that any inaccuracy in definition of pernicious anaemia did not cause bias we carried out an analysis restricting the exposed group to patients with both a specific pernicious anaemia diagnosis code(i.e. excluding patients with vitamin B12 deficiency anaemia due to other causes) and vitamin B12 therapy.
Furthermore, as antibiotic prescriptions are often prescribed for a short term and considered as markers of illness severity, we modelled the antibiotic use as the number of prescriptions during the follow-up period in a separate analysis and categorised usage as follows: no antibiotic use,<4, and 4 or more antibiotic prescriptions to account for the complex changes in use of the antibiotic as a risk factor in the analysis.
Sample size calculation
An initial feasibility count in CPRD identified 38,842 cases (patients with pernicious anaemia). Of these, 312 had a record of C. difficile subsequent to pernicious anaemia diagnosis. Previous studies have estimated that the odds ratio for C. difficile is above 2(6) in patients who take PPIs. Using 10 controls per case, we expected to achieve 99% power to detect an effect of this size or larger in those with pernicious anaemia and to achieve >90% power using HES-linked cases alone.
Results
Study population
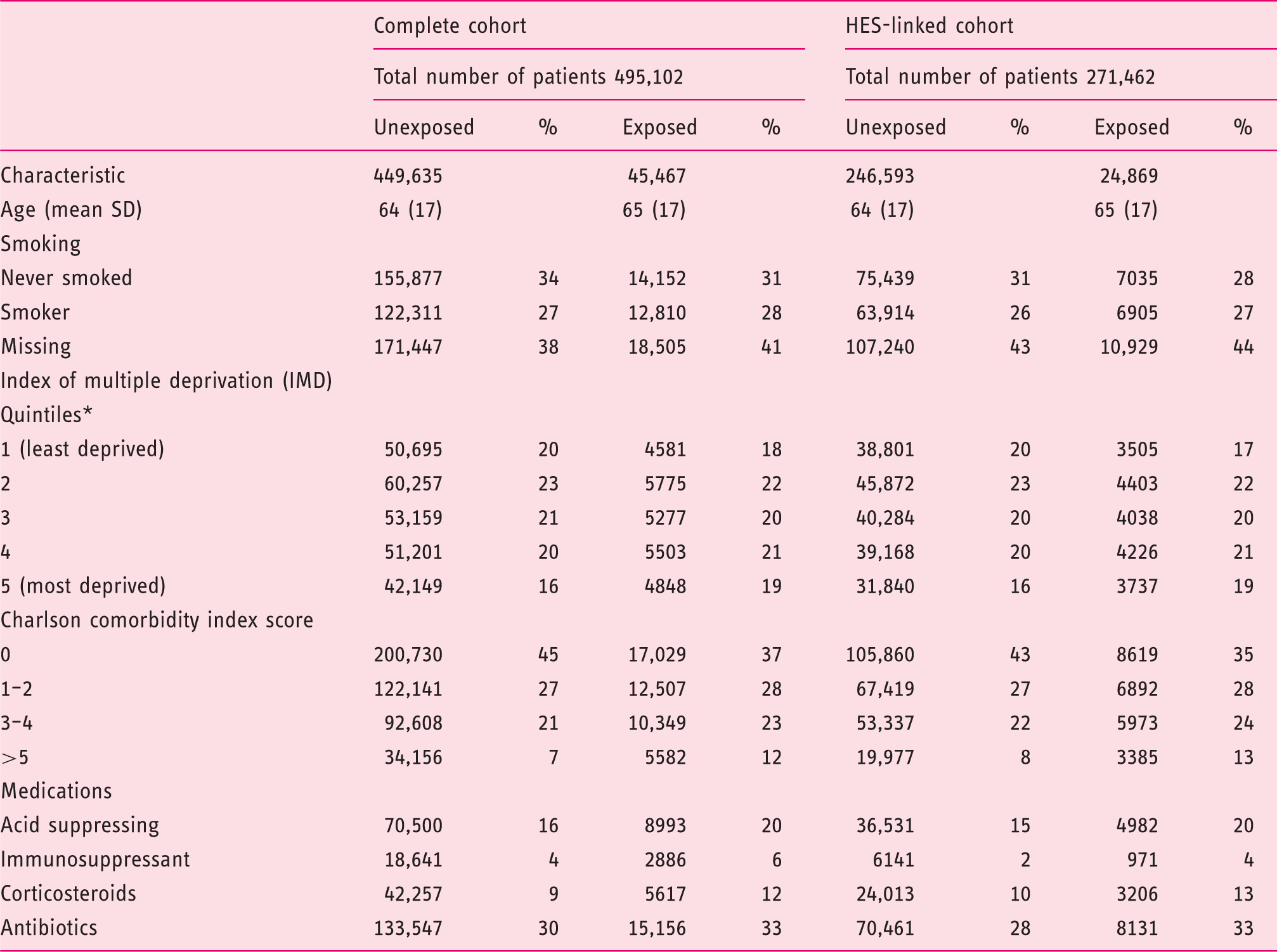
We identified 45,467 patients within CPRD who had a diagnosis of vitamin B12 deficiency anaemia or pernicious anaemia and had received vitamin B12 therapy for at least one year. To these cases we successfully matched a total of 449,635 unexposed patients on age, gender and general practice (Figure 1). The CPRD-HES linked information was available for 24,869 exposed patients and their 246,593 controls. Table 1 presents the characteristics of the study population at the start of follow-up. The exposed cohort was more likely to have a higher burden of comorbidity and had used more medication compared to the control group.
Flow diagram of patient selection from the Clinical Practice Research Datalink (CPRD) population. Demographic and clinical characteristics of the study population included in the cohort study by exposure status at cohort entry into the study period, for all CPRD patients and for the subset of patients with HES-linked data. HES, Hospital Episode Statistics. Socioeconomic status is based on index of multiple deprivation (IMD) and figures are the percentage of the patients eligible for inclusion in the linkage to patient level deprivation data.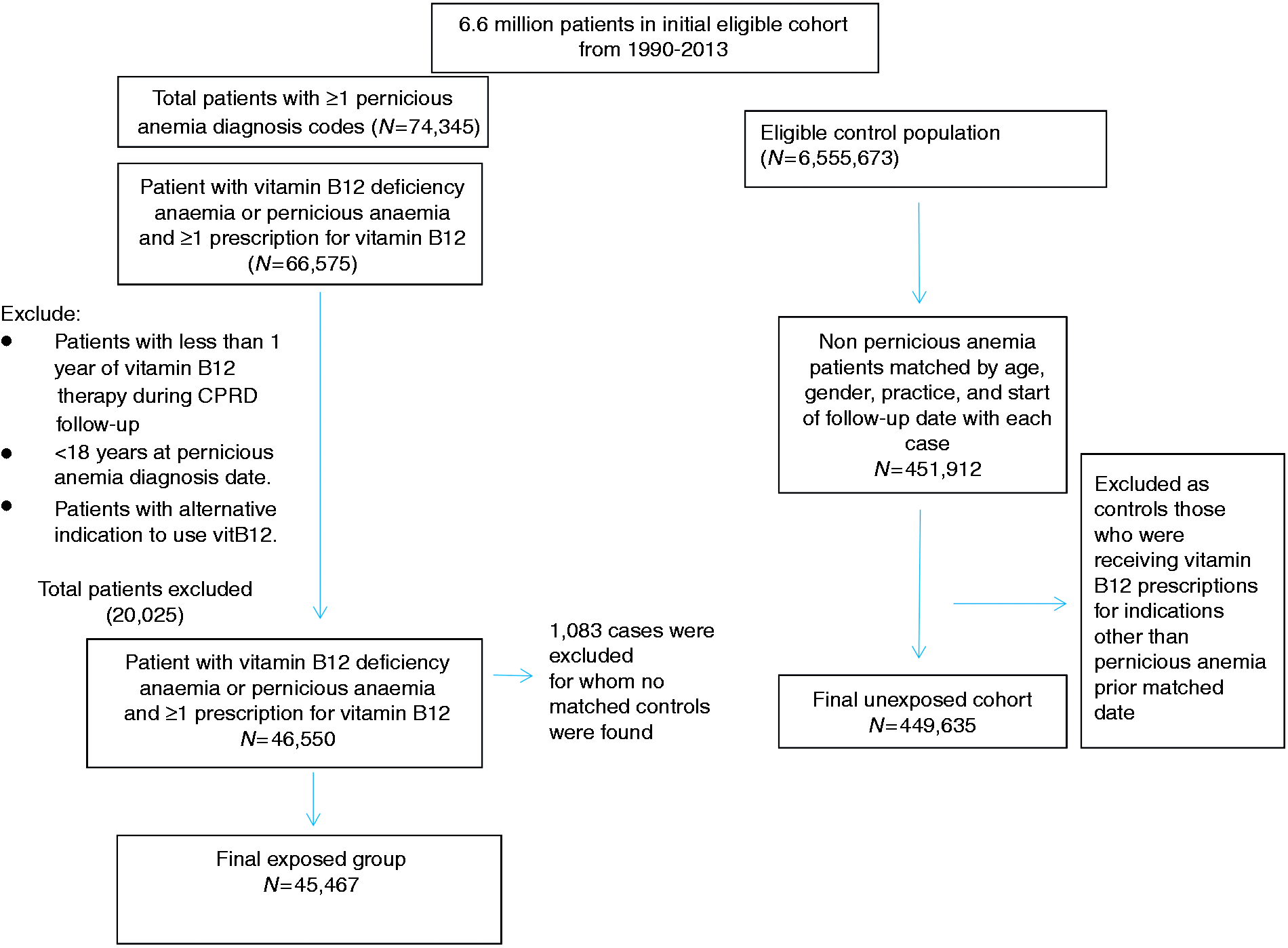
Primary analysis
Adjusted and unadjusted hazard ratios and 95% confidence intervals (95% CI) for the association of Clostridium Difficile infection with pernicious anaemia.
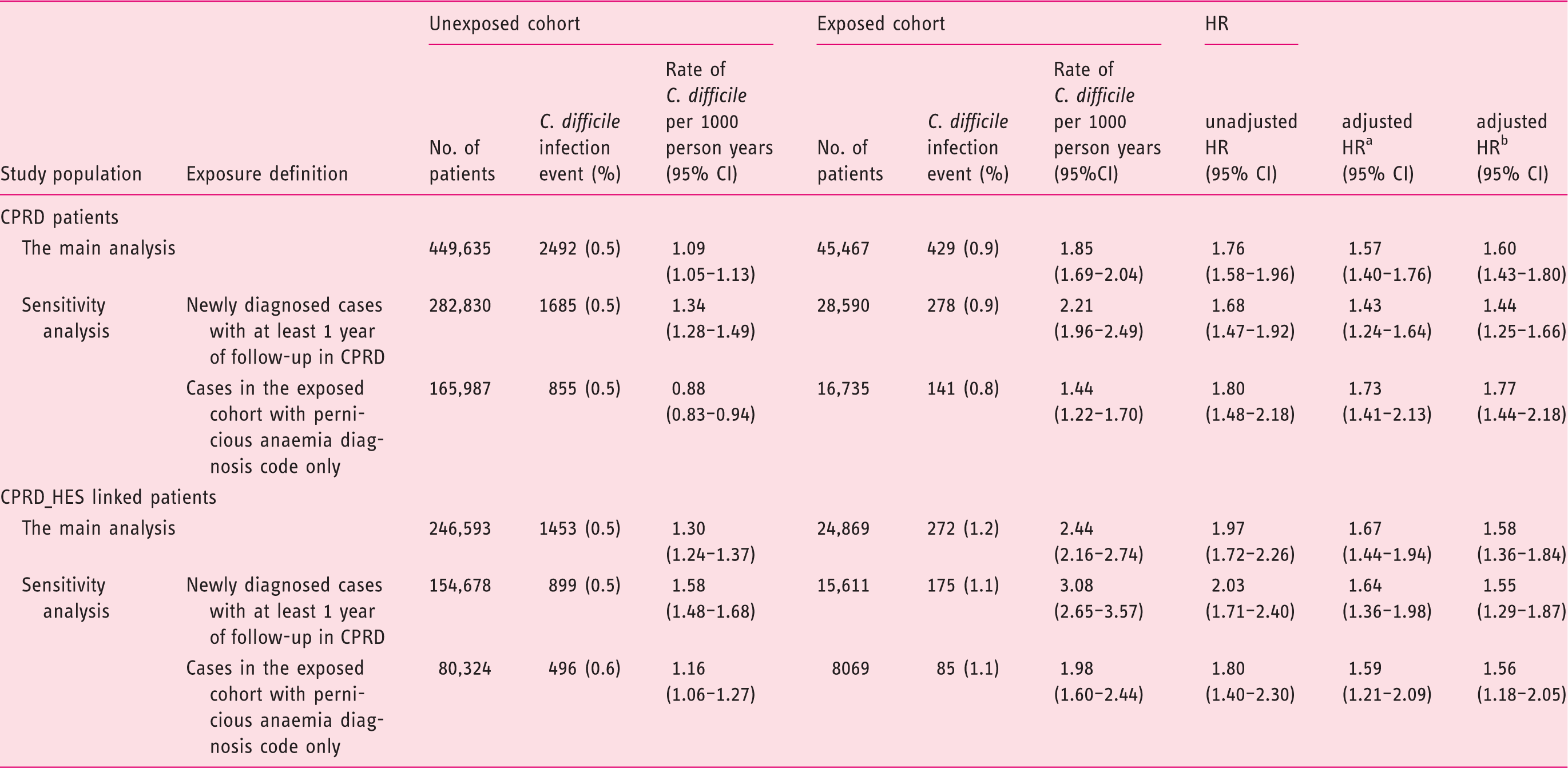
CPRD, Clinical Practice Research Datalink; HES, Hospital Episode Statistics data; HR, Hazard ratio; CI, confidence interval.
Model adjusted for comorbidity index, hospitalisation and use of antibiotics, acid-suppression therapy and immunosuppressant drugs.
Model adjusted for comorbidity index, hospitalisation and use of antibiotics (as number of prescriptions), acid-suppression therapy and immunosuppressant drugs.
The adjusted HR for C. difficile infection in the HES subset was similar at 1.67 (95% CI 1.44–1.94).
Sensitivity analyses
The analysis of pernicious anaemia patients who had an incident diagnosis of pernicious anaemia and who were on vitamin B12 therapy yielded similar results to our primary analysis (Table 2). The analysis of those patients who had been diagnosed with pernicious anaemia based only on pernicious anaemia diagnosis codes and B12 injections showed a slightly higher adjusted HR (1.73; 95% CI 1.41–2.13). The result of the adjusted analysis in which we modelled the antibiotic usage as number of prescriptions showed very similar hazard ratio to our primary analysis (Table 2).
Discussion
In this cohort study, patients with a pernicious anaemia diagnosis had an increased risk of C. difficile infection. This association persisted when we limited the analysis to a subgroup with a more restrictive definition of pernicious anaemia diagnosis, or to incident cases.
Limitations and strengths of the study
As our study was conducted using anonymised electronic patient records, we were not able to confirm the diagnoses of both the exposure and outcome. However, we believe that, although these individual diagnoses have not been specifically validated in CPRD data, the numerous previous studies that have validated the information contained in the CPRD suggest that errors in the assigned diagnoses are not likely to be common.20–22 In addition, since it is unlikely any such error would be more or less common in either group, any bias resulting is likely to merely reduce the apparent association observed. Furthermore, we have attempted to further reassure ourselves in this regard, by insisting on a record of vitamin B12 therapy to define our exposure which should have minimised the risk of misclassification, and our sensitivity analysis restricted to patients with pernicious anaemia specific diagnosis codes, where this definition had been previously used in a study that utilised similar database, 23 further supports our belief that misclassification did not have a major impact on our results. In addition, this study was limited to the data recorded in our dataset and we attempted to control for a variety of confounders through applying both matching and adjustment techniques in the analyses; still, we cannot be certain that there is not residual confounding by unmeasured factors. However, our results were similar to those previous studies that have found an association between the use of PPI therapy and C. difficile infection.6,11 This suggests, we think, that given the differences between pernicious anaemia patients and PPI using patients, it would be a remarkable coincidence that confounding alone caused the associations that were observed in both studies. Rather, the generalisability of the result to a further cause of achlorhydria supports the possibility that the association is causal.
In addition to the limitations outlined above, the data employed in this study had a number of significant advantages. Firstly, the large number of records within the CPRD gave us an adequate power to detect rare diseases and their outcomes. Since the data was collected independently of the research, this should greatly reduce the risk of information bias. 13 Similarly, the selection of all available cases and a random subset of appropriate controls should mean that our study is free from selection bias. To further assure ourselves of this with regard to survivorship, we conducted a sensitivity analysis of incident cases. The results of this analysis were similar to those of the overall analysis. Finally, since the CPRD population is representative of the general UK population, 13 our results are likely to be generalisable to the UK population or similar populations.
Comparison with previous literature:
The idea that achlorhydria might predispose to C. difficile infection dates back to at least 1982 when Gurian et al. reported a case that demonstrated that the killing of the organism and neutralisation of toxin by gastric juice were pH dependent, 24 and that achlorhydria may increase the susceptibility and severity of enteric infection. Recently, several,6,8,25 but not all,26,27 observational studies supported this idea and demonstrated a significant elevated risk of C. difficile infection in patients on PPI. Two meta-analyses that combined these observational studies using slightly different methods showed a significant increase in the incidence of C. difficile infection among patients on PPI therapy with an overall risk estimate between 1.65 (95% CI 1.41–1.93) and 1.74 (95% CI 1.47–2.85).11,28 This caused enough concern that the US Food and Drug Administration (FDA) issued a drug safety statement that PPIs may be associated with C. difficile infection. 29
To date, no randomised placebo-controlled trials have been conducted to solidify the causality of this effect because the associated ethical issues and challenges related to the rarity of the outcome to be studied in such trials entails that conducting such studies is challenging. Although the reduction in stomach acidity decreases the body’s ability to protect itself against C. difficile proliferation, as outlined above, 10 it is biologically plausible that users of PPIs are different in many ways to other members of the population; as such, it is not possible to be confident that all confounding has been corrected in the observational studies that have been performed to date. The chronic and persistent achlorhydria seen in pernicious anaemia is at least as marked as that generally associated with long-term PPI use. The association between pernicious anaemia and C. difficile infection demonstrated in this research therefore suggests, that severe achlorhydria can predispose to C. difficile infection independent of any confounding present in the prescription of PPIs, and is likely therefore to be the mechanism for increased C. difficile infection in people who have received long-term acid-suppression medication.
Conclusion
In this population-based cohort study, patients with pernicious anaemia exhibited an increased risk of C. difficile infection. The results suggest that achlorhydria in chronic PPI therapy is likely to be the underlying mechanism of the increased risk of C. difficile infection. This contributes additional data to the evidence that PPI use is a potentially modifiable risk factor for C. difficile infection. Given the increasing number of patients who are taking long-term PPIs, this finding suggests that practitioners should be vigilant when prescribing a PPI, particularly to patients who have other risk factors for developing C. difficile infection.
Footnotes
Ethical approval
This study was approved by the Independent Scientific Advisory Committee (ISAC) with CPRD number 15_240R, and 15_240RMn for minor amendment.
Declaration of conflicting interests
FO has received a scholarship award from King Saud bin Abdulaziz University for Health Sciences, Saudi Arabia, which sponsors her studies at University of Nottingham; there was no support or financial relationships with any other organisation for the submitted work. TC and CC were independent of the funder and disclose no other conflicts.
Funding
This work was supported in part by a scholarship award from King Saud bin Abdulaziz University for Health Sciences, Saudi Arabia, to FO that sponsors her studies as part of a PhD programme at University of Nottingham.