
Abstract
Background and aims
Pancreatic cystic lesions (PCLs) are commonly diagnosed incidentally and are often preneoplastic. Their presence may influence the management of patients with chronic diseases such as liver cirrhosis (LC). This study evaluated the prevalence and nature of PCLs in LC patients.
Methods
The images of 192 LC patients and 192 controls who underwent either computed tomography scan or nuclear magnetic resonance were reviewed for the presence and nature of PCLs. The prevalence of PCLs in both groups and differences between LC patients with and without PCLs were analysed. Multiple logistic regression analysis was used to investigate factors associated with PCLs.
Results
Thirty-five of 192 LC patients (18%) and 19/192 controls (10%) had PCLs (p = .027). The prevalence of presumptive intraductal pancreatic mucinous neoplasm (IPMN) was double in LC patients compared with controls (14% vs 7%; p = .065). In multivariate analysis, age, LC and having undergone a magnetic resonance cholangiopancreatography were factors associated with PCLs and IPMNs. LC patients with PCLs were older at the time of imaging and had a longer history of liver disease (67 vs. 43 months; p = 0.039) compared with LC patients without PCLs.
Conclusions
PCLs are more common in LC patients than in controls, and most are IPMNs. The occurrence of PCLs in LC patients seems to be related to age and disease duration.
Introduction
The prevalence of incidental pancreatic cystic lesions (PCLs) in the adult population is high, ranging from 2.6% to 19.6%. 1 Moreover, the prevalence, size and number of PCLs increase with age, with an impressive figure in autopsy series, from 8% below 70 years of age to 35% in individuals aged >90 years.2–5 In clinical practice, most PCLs are detected incidentally, when cross-sectional abdominal imaging studies are performed for unrelated indications.
The management of patients with PCLs varies depending on their nature, and it is therefore important to characterize cystic pancreatic neoplasms (CPNs) and to distinguish them from pancreatic pseudocysts (PP). Although different histologic types of CPNs have been reported, serous cystadenomas, mucinous cystic neoplasms and intraductal papillary mucinous neoplasms (IPMNs) represent the vast majority. 6 Serous cystadenomas are benign neoplasms that do not require surgical excision in asymptomatic patients, whereas most mucin-producing lesions, such as IPMNs and mucinous cystic neoplasms, have malignant potential and warrant surveillance or surgery.7–9
The diagnosis of CPNs in patients with other serious disorders could result in difficult therapeutic choices. Interestingly, the impact of pancreatic comorbidities has been poorly evaluated in patients with chronic liver disease, such as liver cirrhosis (LC). Some studies have focused on IPMNs in liver transplant patients, and reported that in this particular subset of immunosuppressed patients IPMNs do not have a more aggressive behaviour.10,11
However, as cirrhotic patients may be evaluated for many treatments depending on their prognosis and comorbidities, the presence of CPNs, and the related increased risk of developing pancreatic cancer over the entire gland, 12 might have an impact on their management. Moreover, there is some evidence that aetiological factors for LC, such as hepatitis B and C viruses (HBV, HCV), alcohol abuse and metabolic syndrome, might be associated with an increased risk of pancreatic cancer.13–15
However, whether patients with LC have an increased risk of harbouring preneoplastic pancreatic lesions is unknown. We therefore aimed to evaluate the prevalence and the nature of PCLs in patients affected by LC, and possible features associated with their occurrence.
Materials and methods
Study design and population
This was a retrospective case–control study. Cases of LC were selected among those prospectively enrolled in a dedicated database. The inclusion criteria for the case group were a diagnosis of LC and having undergone at least one of the following abdominal imaging procedures: contrast-enhanced computed tomography (CT), contrast-enhanced magnetic resonance imaging (MRI) and magnetic resonance cholangiopancreatography (MRCP) at our Radiology Department, between 2006 and 2015, for any indication.
LC was diagnosed either by histology or by biochemical and radiological findings. 16
A previous diagnosis of pancreatic disorders leading to the radiological investigation was an exclusion criterion for the case group.
The control group consisted of sex- and age (±5 years)-matched inpatients admitted to the hospital for different acute conditions, who underwent one of the abovementioned radiological procedures for liver- and pancreas-unrelated indications. Exclusion criteria for the control group were a previous diagnosis of liver or pancreatic disorders or of gastrointestinal neoplasms. While data on the aetiology of LC were available for all patients, data on alcohol and tobacco use were not available for controls, who were not matched for such variables.
All patients gave written informed consent. The study received approval from the local Hospital Review Board.
Radiological procedures
Computed tomography (CT)
CT scans were performed with a multidetector CT (MDCT) machine (16 slices) (General Electrics (GE) LightSpeed). The following technical parameters were used: 120 kV, mAs 120–180, slice thickness 3 mm and pitch 1. Examinations were performed before and after intravenous administration (through the placement of needle 16-18 G into a vein of the right arm) of 120–150 ml (2 ml/kg) of non-iodinated contrast medium at a speed of 3–3.5 ml/s. Dynamic study after contrast medium consisted of an arterial (30 s later) and a portal phase (70 s later). Once the images were obtained, multi-planar reconstructions (MPR) and 3D volume rendering (VR) were performed when necessary.
Nuclear magnetic resonance (MR)
MR examination was carried out with 1.5 Tesla equipment with a four-single phased array coil positioned on the patient’s upper abdomen. The MR protocol involved the use of T1-weighted gradient echo (GRE) sequences with in-phase and out-of-phase echotime, T1-weighted fat-suppressed GRE sequences, and T2- weighted half-Fourier single-shot turbo spin-echo (HASTETSE). The dynamic study was performed during administration of 0.1 mmol/kg body weight of gadolinium chelates with a four-phase technique: precontrast, pancreatic phase (30–40 s), portal venous phase (80 s) and delayed phase (180 s). The dynamic study used a T1-weighted 3D GRE volumetric interpolated breath-hold examination (VIBE) sequence with chemically selective fat saturation in the axial plane.
Magnetic resonance cholangiopancreatography (MRCP)
MRCP was performed using a 2D single-slab rapid acquisition in coronal planes and a 3D HASTE sequence with respiratory triggering in a coronal oblique plane depending on the course of the main pancreatic duct as visualized on a 2D sequence acquired in the axial plane. The 3D HASTE source images were analysed and subsequently processed with thin Maximum-intensity projection (MIP) algorithm and MPR.
The CT or MRI images were reviewed independently by two radiologists (M.D.P. and F.C.) on a picture archiving and communication system workstation. The radiologists were blinded to the clinical features (either LC or controls) and to the results of other possible examinations, such as ultrasonography or endoscopic ultrasound, if performed. A template was designed to record the cyst morphology details according to standard radiological criteria. 17 Each reader recorded the number, size and location of each cyst, ‘worrisome features’ (such as cyst of 3 cm, thickened enhanced cyst walls, non-enhanced mural nodules, main pancreatic duct size of 5–9 mm, abrupt change in the main pancreatic duct with distal pancreatic atrophy and lymphadenopathy) and ‘high risk stigmata’ (such as enhanced solid component and MPD size of 10 mm),7,18 if present. In patients with multiple cysts, data were recorded separately for each cyst. For every diagnosed PCL, the more likely diagnosis was attributed according to the radiological characteristics. In case of disagreement, the radiological features were discussed with a third senior radiologist (E.I.), and a final diagnosis was made for each case.
Clinical features of patients with liver cirrhosis
All demographic and clinical characteristics of LC patients were recorded in a database, including the aetiology, the severity of liver dysfunction expressed through Child–Pugh score, 19 the possible diagnosis of hepatocarcinoma (HCC), the age at LC diagnosis, the age at time of radiological imaging, and the time interval between the diagnosis of LC and the radiological imaging.
Statistics
Differences between LC and controls in terms of prevalence of PCLs, and between LC patients with and without PCLs, were analysed. The Fisher test was used for comparison of proportions for categorical variables and Student’s t-test for continuous variables. Multiple logistic regression analysis was employed to investigate factors associated with the diagnosis of PCLs. Tests of statistical significance and confidence intervals were two-sided; a p value <.05 was considered to be statistically significant. Dedicated software (MedCalc, Mariakerke, Belgium) was used throughout the study.
Results
General features of liver cirrhosis patients and controls
Demographic and clinical characteristics of liver cirrhosis patients and controls.
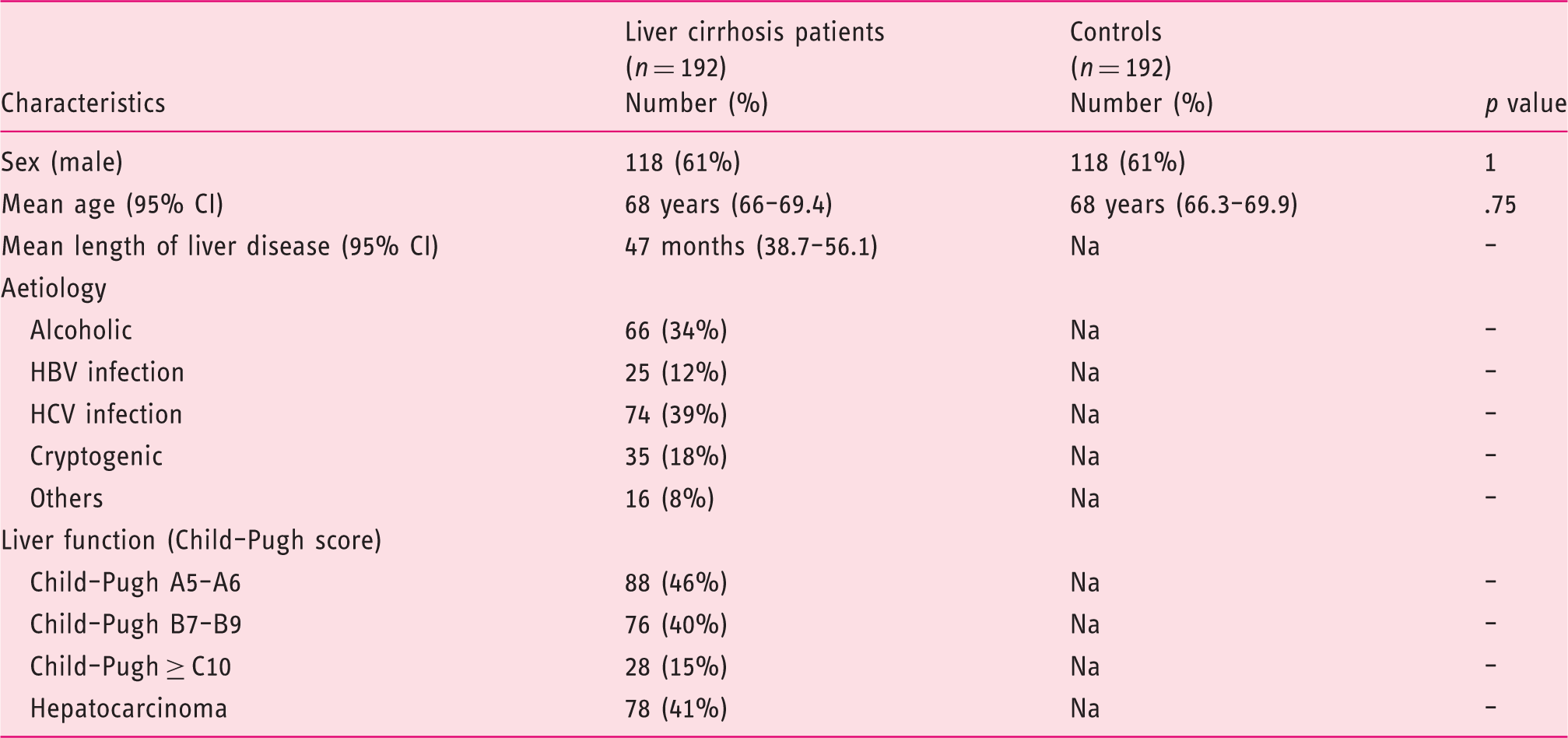
HBV: hepatitis B virus; HCV: hepatitis C virus; Na: not applicable.
Prevalence of PCL in LC patients and controls
Prevalence and type of pancreatic cystic lesions in liver cirrhosis patients (cases) and controls.
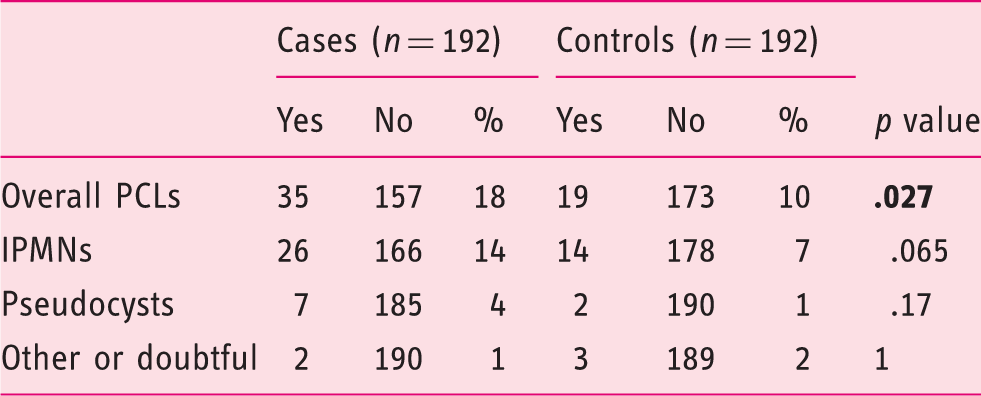
IPMNs: intraductal papillary mucinous neoplasms; PCLs: pancreatic cystic lesions. Bold indicates statistical significance
As a significant portion (78/192, 41%) of the LC patients also had a diagnosis of HCC, and as it has been reported that IPMNs are often associated with other tumours, we compared the rate of diagnosed IPMNs in LC patients with or without HCC with that of controls. A diagnosis of presumptive IPMN was made in 11/78 (14%) HCC patients, 15/114 (13%) LC patients without HCC and 14/192 (7%) of controls. Thus, the diagnosis of HCC did not seem to be associated with a higher risk of IPMN.
Many of these PCLs were not reported in the original radiological report and were described after re-evaluation for this study. The finding was described in the initial report for only 21 of the 35 (60%) LC patients and 9 of the 19 (47%) controls with a final diagnosis of PCLs.
PCLs were diagnosed by CT scan in 11% of cases and 7% of controls, respectively, by MR in 10% of cases and 3% of controls, and by MRCP in 36% of cases and 23% of controls. There was no significant difference in the percentage of patients receiving MRCP in the two groups (12% in LC cases vs. 18% in controls; p = .08).
All the 40 patients (26 LC and 14 controls) with presumptive IPMN were diagnosed incidentally, without any specific symptoms, and all the lesions were of the branch-duct type (BD-IPMN), without high risk stigmata or worrisome features.7,18 The main diameter of BD-IPMNs was 10 mm in LC patients and 8.2 mm in controls. However, 38% of the LC patients and 7% of controls had BD-IPMN with cystic diameter between 10 and 20 mm (p = .06). The only two lesions with a diameter >20 mm were diagnosed in the control group. There were also no differences among IPMNs diagnosed in both groups in terms of focality (rate of multifocality 46% vs. 57%; p = .74), main duct diameter and localization (data not shown).
All LC patients with pancreatic lesions suspected of being PP (7 of 192 patients, 4%) were asymptomatic and without a history of acute pancreatitis. Interestingly, the diagnosis of PP was not associated with alcoholic cirrhosis (only two of seven LC patients with PP had an alcohol-related liver disease). Similarly, the two patients in the control group with radiological finding of PP did not have a history of previous acute pancreatitis or known pancreatic disorders.
Factors associated with the diagnosis of CPLs in cases and controls
Factors associated with the diagnosis of pancreatic cystic lesions at the logistic regression analysis.

MRCP: magnetic resonance cholangiopancreatography. Bold indicates statistical significance.
Factors associated with the diagnosis of intraductal papillary mucinous neoplasms in the logistic regression analysis.

MRCP = magnetic resonance cholangiopancreatography. Bold indicates statistical significance.
Differences between patients with LC with and without associated PCLs
Comparison of demographic and clinical characteristics between liver cirrhosis patients with and without pancreatic cystic lesions.
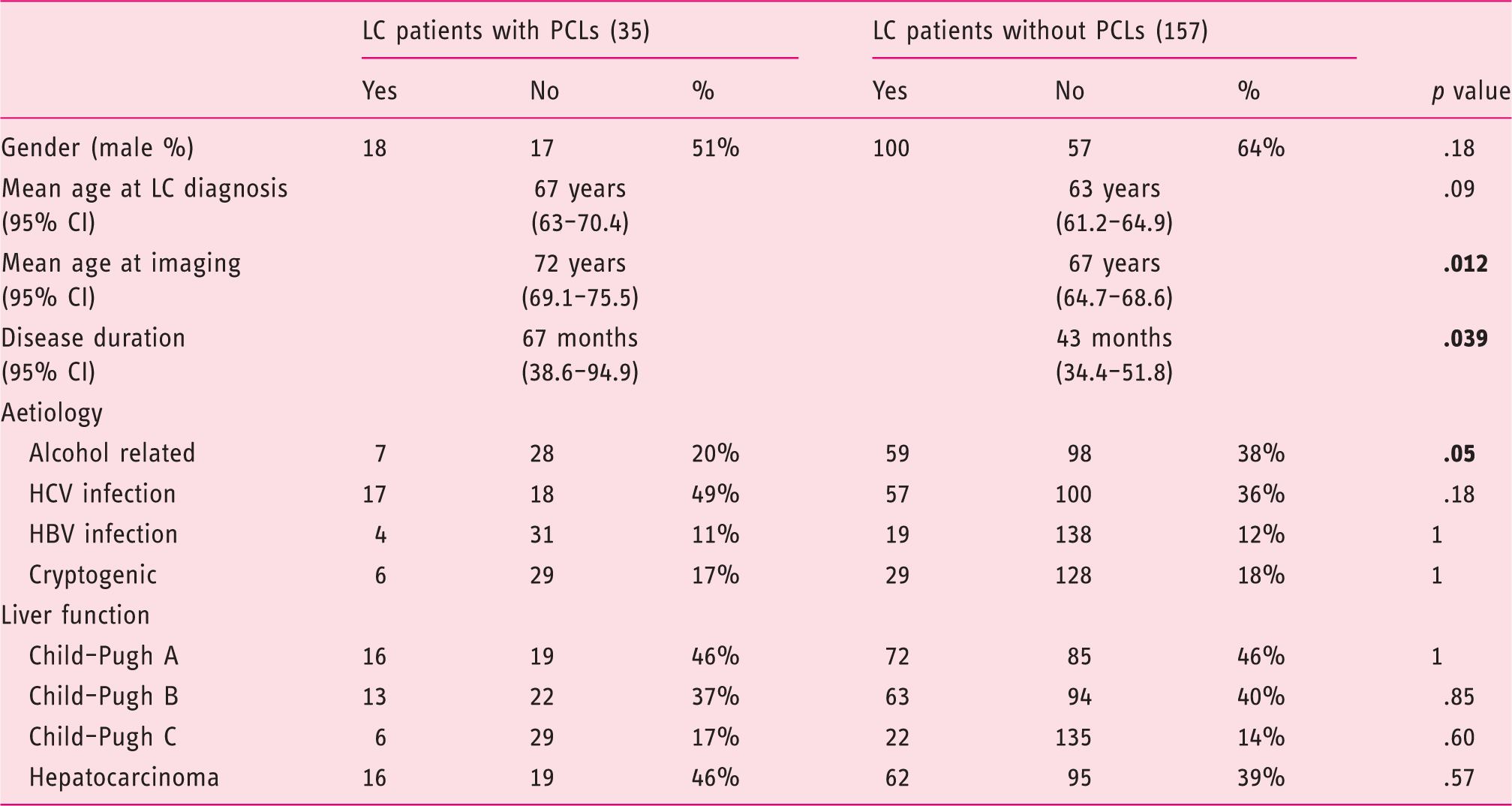
HBV: hepatitis B virus; HCV: hepatitis C virus; LC: liver cirrhosis; PCLs: pancreatic cystic lesions. Bold indicates statistical significance.
No characteristics of LC patients were associated with the diagnosis of IPMN.
Discussion
Patients with LC have a relatively long disease history, and during this course of time they might undergo multiple treatments, such as those for viral hepatitis and HCC, and eventually liver transplantation. The diagnosis of a preneoplastic pancreatic lesion might thus modify their treatment plan. Furthermore, some risk factors for LC, such as HBV and HCV infection and alcohol abuse, might also be associated with the occurrence of pancreatic cancer and of IPMNs.13,14,20 However, there have been no previous studies investigating the prevalence and characteristics of PCLs in LC patients.
In the present study, 18% of patients with LC had PCLs, and in 74.3% of these cases the lesions were categorized as presumptive IPMN, a lesion that has a potential malignant behaviour and requires treatment or follow-up.7,8,9,18 This rate was higher than that observed in a matched control group (p = .027), which instead showed a prevalence in keeping with those recently reported in the general population. 21
A number of population studies have investigated the rate of PCLs both in asymptomatic subjects and in liver transplanted patients. The former3,4,22,23 are generally represented by retrospective database studies, showing a high heterogeneity in the prevalence of PCLs due to different radiological examinations and study design. In those studies, the prevalence of PCLs ranged from 4.2% to 44.7%. An interesting study analysed the entire population of a small geographical area (San Marino) and detected the true prevalence of PCLs in the general population, which was 5.4% and increased to 13% in individuals older than 80 years. 23 However, that study employed only CT scan, which is known to be less sensitive than MRI in diagnosing PCL. 24 A few studies investigated the prevalence of PCLs in transplanted patients10,11,25,26 with a rate ranging from 6.7% to 60%.
In the present study, the prevalence of IPMNs was higher in LC patients compared with controls (14% vs. 7%, respectively), although this difference was only close to statistical significance (p = .065), probably due to the relatively low absolute number of subjects with IPMN in the two groups. Only 20% of the PCLs were instead shown to be PP according to their radiological characteristics.
Additionally, the multivariate analysis showed that LC was an independent factor associated with the diagnosis of presumptive IPMN (OR 2.4, 95% CI 1.01–5.24, p = .028). These findings suggest for the first time that LC patients might be at increased risk of developing PCLs and thus, potentially, pancreatic cancer.
Notably, while the ages of the LC and the control group did not differ significantly, in the present study, older age was associated with an increased prevalence of PCLs. In the comparative analysis between LC patients with and without PCLs, those with PCL were significantly older at the time of the imaging procedure, but not at the time of LC diagnosis, and had a longer history of cirrhosis.
Although the present results should be considered with caution, as they were obtained in a retrospective setting and are possibly prone to bias, they might suggest that a long-standing liver disease, characterized by a state of chronic systemic inflammation, is related to an increased proliferation of the pancreatic ductal epithelium, leading to the development of IPMNs. Indeed there is evidence that in LC a high concentration of pro-inflammatory cytokines occurs, including interleukin (IL)1α, IL6 and hepatocyte growth factor (HGF), tumour necrosis factor (TNF)α and transforming growth factor (TGF)β.27–29 Notably, in a study investigating the expression of inflammatory proteins in pancreatic cystic fluid during Endoscopic Ultrasonography (EUS), an increased concentration of HGF in PCLs was shown. 30
Furthermore, having undergone an MRCP was associated with a higher risk of being diagnosed with a PCL. This latter finding was expected, as MRCP has a high sensitivity to investigate the pancreatic ductal system and to diagnose PCLs, but as the rate of LC patients and controls undergoing MRCP was not different, this does not cause any bias.
In order to investigate the association between LC and both PCLs and IPMNs, we compared the features of LC patients with and without a diagnosis of PCLs or IPMNs. The aetiology of cirrhosis and its severity, or the presence of HCC, were not related to the diagnosis of PCLs or IPMNs. In particular, the rate of HCC in our LC population was relatively high despite a relatively low Child–Pugh score. This could be due to the selection of a population of LC patients for whom a second-level radiological examination (CT scan and/or MRI) was deemed necessary, or possibly to an underestimation of disease duration. However, the rate of IPMN was not higher in patients with LC and HCC.
Our results are in accordance with a previous study conducted on a selected group of LC patients undergoing liver transplantation, 10 in which the presence of PCLs and IPMN was retrospectively investigated. Both clinical characteristics (such as diabetes and insulin use, body mass index (BMI) and smoking) and cirrhosis-related characteristics (aetiology and HCC) were analysed, without finding any significant correlation with the occurrence of PCLs.
Nevertheless, our study population is possibly more representative of LC, as it is not limited to a selected group of subjects screened for liver transplantation.
Whether the presence of PCLs in LC patients could alter their clinical course, especially in those who are candidates for liver transplantation and immunosuppressive therapy, is uncertain. Two recent studies compared the results of follow-up of patients with IPMN who were and who were not treated with immunosuppressive drugs,11,26 without reporting a worse outcome in patients on immunosuppression.
In the present study, all the presumptive IPMNs detected were small BD lesions, either unifocal or multifocal, equally distributed in the pancreatic gland, and none of them showed signs suggestive of potential malignant evolution. Therefore, there is no evidence suggesting a more aggressive behaviour of IPMNs in LC patients, and the clinical significance of these lesions seems rather small, although our data are limited to the time of diagnosis and a long-term follow-up study could be of interest.
A surprising finding of the study is the lack of association between the diagnosis of probable pseudocysts and any history of pancreatitis or alcohol abuse. Indeed, only seven of nine patients with LC and pseudocysts had an alcoholic aetiology. This might possibly be due to the classification as viral of some LC patients with a previous exposure to alcohol abuse.
It is interesting to note that PCLs were not described in a significant number of the original radiological reports, and these lesions were often identified only after the review of the images. It is well known that a non-negligible proportion of PCLs, especially those with small diameters, are not described in imaging reports in patients without a past history of pancreatic disease. In a previous study, 69% of cystic lesions with a mean diameter of 6 mm were not reported in the original report. 4 In our experience, PCLs with a diameter <10 mm were not described in 40% of LC patients and in 53% of controls in the first radiological report.
The strengths of this study include its original hypothesis, the analysis of a well-characterized LC cohort and the inclusion of a control group without pancreatic or liver disorders, both of which underwent at least one radiological examination at the same radiological unit, with review of the findings by two dedicated radiologists.
The main limitation concerns the retrospective design and lack of information about factors, such as smoking, BMI, diabetes and family history of pancreatic cancer, that might also influence the occurrence of PCLs. Furthermore, as the diagnosis of PCL type (i.e. IPMN or other) was only obtained radiologically, a misdiagnosis cannot be excluded, and the diagnoses should be considered presumptive. However, this is the case for the vast majority of PCLs in clinical practice; thus, the present information can be considered useful in the real-life setting.
In conclusion, the present study suggests that PCLs are more common in LC patients than in matched controls, and that most of these lesions are presumptive IPMNs. The occurrence of PCLs in LC patients seems to be related to age and disease duration. The mechanisms for the observed findings are unclear and deserve further study, although a role for a pro-inflammatory milieu or the direct influence of aetiological factors for LC might be hypothesized. Given the higher accuracy of MRCP in diagnosing PCLs, future prospective studies should employ this method in all patients and controls.
Footnotes
Acknowledgements
None.