
Abstract
Chronic constipation (CC) is an extremely common condition with an estimated prevalence of up to 24%. Most patients with CC should be treated in primary care. Changes in lifestyle, including increased intake of dietary fibre, fluid, and exercise, should be attempted in most patients. Osmotic or stimulant laxatives are indicated if there are insufficient effects of lifestyle changes. Prokinetics and secretagogues should be restricted to those not responding to basic treatment. Anorectal physiology tests and assessment of colorectal transit time are indicated if medical treatment fails or if symptoms indicate severely obstructed defecation. If symptoms indicate an underlying structural disorder, barium or magnetic resonance evacuation proctography is indicated. Biofeedback therapy is effective in patients with dyssynergic defecation. In patients with other evacuation disorders, rectally administered laxatives or transanal irrigation should be attempted. Surgery is restricted to the minority of CC patients with very severe symptoms not responding to conservative treatment.
Introduction
Chronic constipation (CC) is an extremely common disorder with an estimated prevalence ranging between 2% and 24%.1,2 The prevalence of CC increases with age and may reach 80% in nursing home residents. 2 Constipation has severe consequences for the quality of life of those affected and costs to individual patients and to society in general are significant.
Definition of chronic constipation according to the ROME III criteria
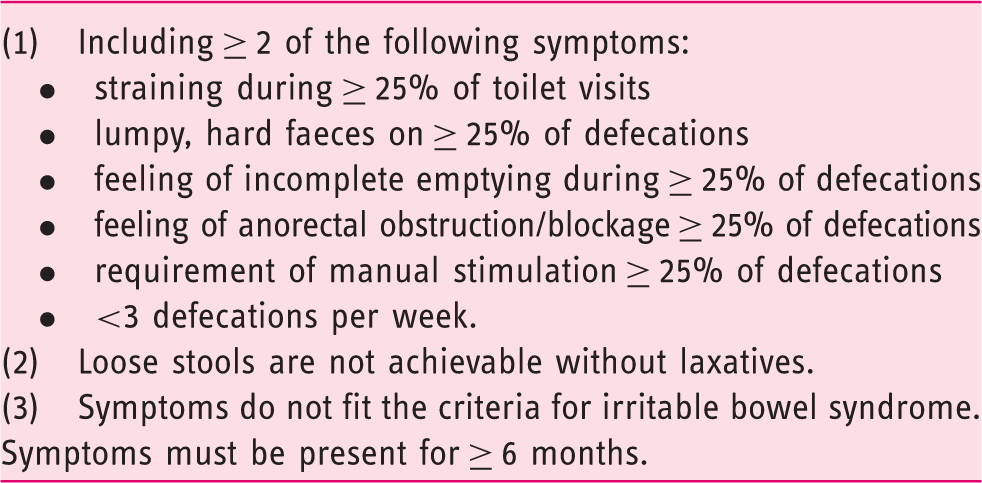
Within the last decade our understanding of the pathophysiology behind CC has improved and several new drugs or treatment principles have been introduced. The following is a clinically orientated review of modern management of CC.
Pathophysiology of constipation
CC is often classified from the objective test used.
From transit studies, CC is commonly classified as slow transit constipation with abnormally slow transit throughout the whole colorectum, outlet disorder where transit is mainly delayed in the distal colorectum, or normal transit constipation where the subject has symptoms of constipation but colorectal transit time is normal. 4
From anorectal physiology tests a subgroup of patients can be identified as having dyssynergic contraction of the pelvic floor during defecation. Others have rectal hyposensation determined by rectal balloon distension, 5 while some have structural disorders found on evacuation proctography or magnetic resonance imaging. Very often more than one abnormality can be found in the same patient and abnormal tests are common among healthy subjects without symptoms of CC. Thus, no test can stand alone in the evaluation of individual patients.
Colorectal contractions are generated by the interstitial cells of Cajal. The most important contraction patterns are (a) segmental contractions located to short segments of the colon with the main function of mixing colonic contents and (b) high amplitude colonic contractions that move colonic contents through large distances and often precede defecation.
The number of interstitial cells of Cajal is reduced in some patients with CC. Recent studies with fibre optic high resolution manometry have provided detailed information about motility in patients with slow transit constipation. Thus, patients with CC appear to have (a) significantly reduced amplitude of colonic contractions, including fewer high amplitude colonic contractions, (b) reduced gastrocolonic response after meals, and (c) significantly more retrograde contractions. 6
Outlet dysfunction is a common form of constipation often non-responsive to conservative treatment. The main symptoms are straining, difficult rectal evacuation or a sense of incomplete evacuation. It may affect up to 50% CC patients referred to tertiary care. 7 Patients with outlet dysfunction can be divided into those with structural causes (i.e. large rectocele, rectal prolapse or perineal descensus) and patients with a functional defecation disorder, mostly dyssynergic defecation. 8 Dyssynergic defecation is characterized by inability to coordinate abdominal muscle pushing effort and pelvic floor muscle relaxation on straining. Severe outlet disorder can also be seen with damage to the reflex arch between the colorectum and the spinal cord. 9
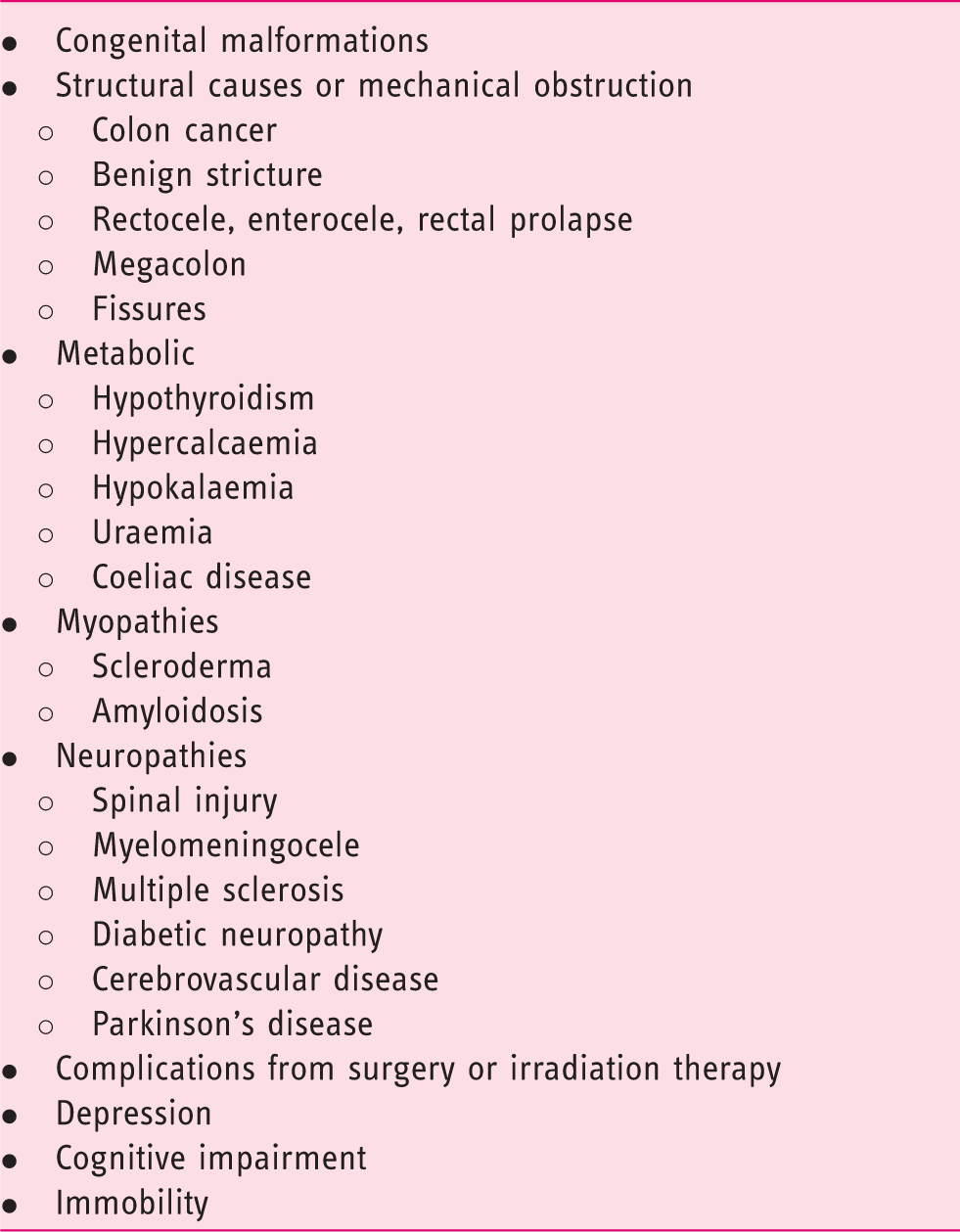
Examples of conditions causing secondary constipation
Basic clinical evaluation of patients with CC
Most patients with CC should be treated in primary care. If alarm symptoms indicating colorectal cancer or other organic disease are present, endoscopy should be performed according to local guidelines.
The anamnesis should include: duration of symptoms, comorbidity, previous gastrointestinal or anorectal surgery, stool frequency, stool consistency, difficult rectal evacuation, sense of incomplete evacuation, straining, sense of obstruction during defecation, digital evacuation of the rectum, vaginal digitation to empty the rectum, digital support of the perineum, abdominal massage, unsuccessful attempts at defecation, abdominal pain, bloating, pain during evacuation, signs of rectal prolapse, enterocele or cystocele, previous treatment, concomitant medication, and impact on social activities and quality of life. A brief assessment of diet, fluid intake and physical activity should be included. Furthermore, symptoms of bladder or gynaecological disorders should be noted. A history of physical abuse or psychiatric disorder may cause special considerations about therapy.
Abdominal palpation should be performed to exclude abdominal mass. Digital anorectal examination should be performed at rest to exclude tumours in the ampulla or anal canal. Digital anorectal examination is performed during attempted defecation to identify pelvic floor contraction. If difficult evacuation is a main complaint, bimanual vaginal and rectal examination can be performed to identify rectocele. Patient reporting symptoms of rectal prolapse should sit on a commode and be asked to bear down for two minutes to identify a rectal prolapse.
In most patients treatment can be initiated after the simple evaluation described above.
Advanced evaluation of patients with CC
Patients not responding to basic treatment with lifestyle modifications, laxatives or other medical treatment as described below should be considered for more advanced evaluation. The same is true for patients with symptoms of severely obstructed defecation or underlying structural disorders. Advanced evaluation of patients with CC usually includes: assessment of colorectal transit time, anorectal physiology tests, and imaging of the rectum and the pelvic floor.
The most commonly used method for estimating colorectal transit time is radio opaque markers. Several protocols exist but basically three variants are used: (A) single intake of radiopaque markers followed by a single abdominal X-ray (usually after four days), (B) intake of radiopaque markers on successive days (usually three or six days) followed by a single abdominal X-ray on day four or seven, or (C) single intake of radiopaque markers followed by successive abdominal X-rays. Method A is simple and easy to both patients and staff, but it only provides semi-quantitative estimates of colorectal transit time.
10
Method B provides quantitative information on total and segmental colorectal transit times (in hours or days), but requires that the patient remembers to take the markers at the correct time.
11
Method C is usually not used because it requires more than one X-ray and exposes the subjects to more irradiation than the other methods. Examples of normal and prolonged colorectal transit times are shown in Figure 1.
Examples of normal (a) and prolonged colorectal transit time in a patient with slow transit constipation (b).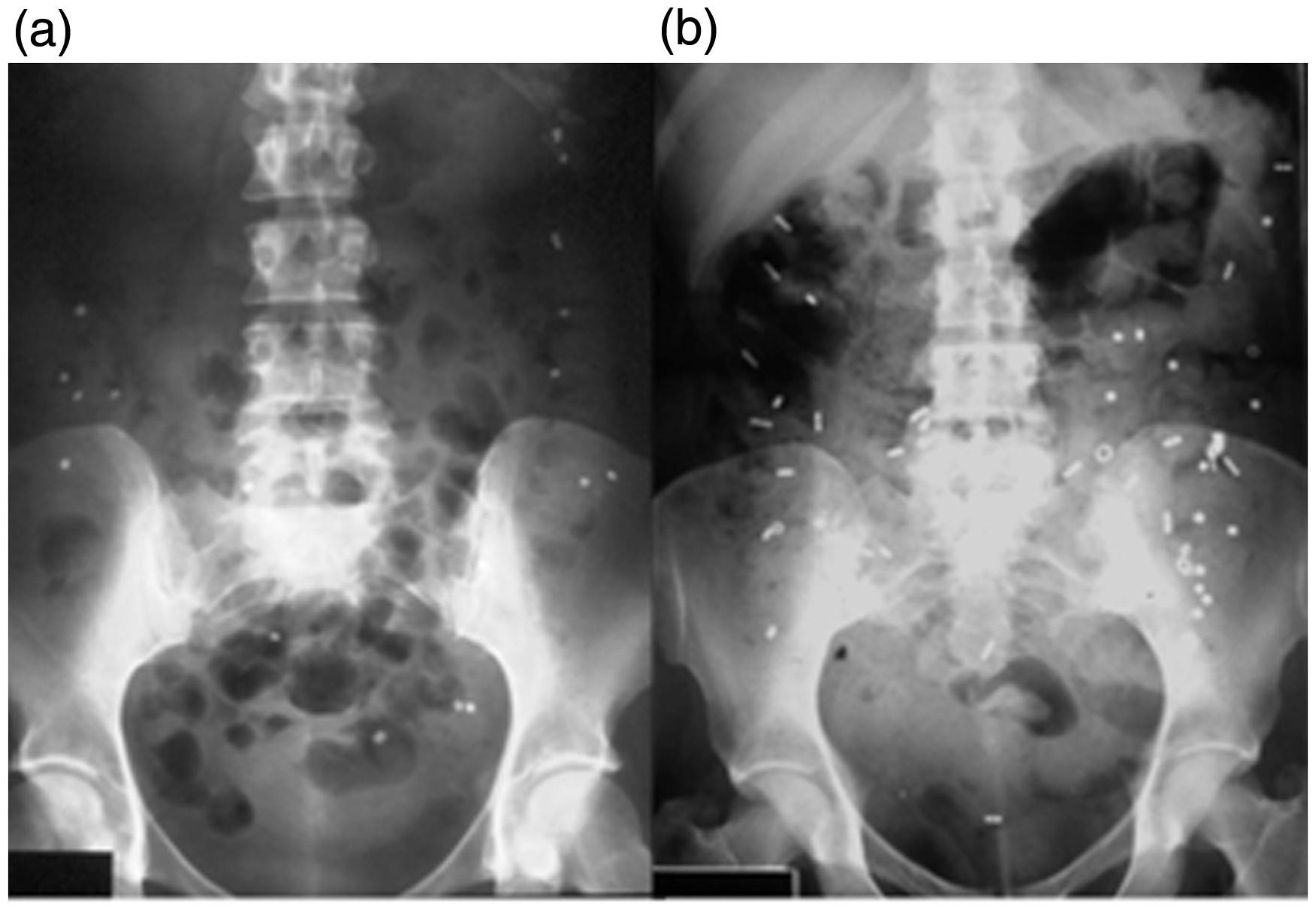
The wireless motility capsule and the novel Motilis 3D-Transit system hold promise for future evaluation of regional and whole-gut motility and transit times in CC.12,13
Anorectal physiology tests in patients with CC are different from those used in patients with faecal incontinence. In CC the following tests are commonly used: assessment of rectal sensation, rectal capacity and compliance during balloon distension, anal manometry during rectal balloon distension and anal sphincter electromyography during rectal balloon evacuation. 14
Rectal sensitivity and capacity are usually tested by rectal distension by a balloon or a bag. 14 The aim is to identify subjects with a hyposensate rectum. Usually, volumes are registered at ‘first sensation’, ‘urge to defecate’ and ‘maximum tolerable volume’. From volume–pressure relations, rectal compliance can be computed. Even though commonly used, rectal distension with a balloon is hampered by inherent sources of error. 14 Investigation with a barostat is more accurate but also very time consuming. A new ‘fast barostat’ has recently been introduced. 15
Anal manometry during rectal balloon distension is mainly performed to identify patients with Hirschsprung’s disease. Absence of the rectoanal inhibitory reflex, mediating internal anal sphincter relaxation during rectal distension, indicates Hirschsprung’s disease but deep biopsies are necessary to confirm the diagnosis.
Electromyography of the external anal sphincter during attempted evacuation of a rectal balloon is performed to identify paradox contraction of the pelvic floor during defecation. 8 The inability to expel the balloon supports the diagnosis. 16 Unfortunately, there is considerable disagreement between various tests of evacuatory function. 17
The anatomy of the rectum and surrounding pelvic organs during defecation are usually evaluated with evacuation or magnetic resonance proctography.18,19 Either modality is indicated if structural disorders, e.g. rectocele or rectal intussusception, are suspected as a cause of difficult evacuation. Regardless of methods, structural disorders are extremely common in asymptomatic subjects and their presence does not necessarily explain the symptoms or indicate surgical treatment.
The main limitations with all anorectal physiology tests are the extreme variability between subjects and substantial overlap between asymptomatic healthy subjects and patients. However, the identification of patients with Hirschsprung’s disease and the much more common patients with pelvic floor dyssynergia is important because the conditions should be treated with surgery and biofeedback, respectively.
Lifestyle modifications for CC
CC is associated with low intake of fibre and fluid. 20 Dietary fibres are resistant to hydrolysis by enzymes in the small intestine and pass unabsorbed to the colon, where they retain water and add bulk to the stools. Increased intake of fibre can reduce colonic transit time and alleviate symptoms.21,22 Side effects mainly include the production of gas causing abdominal discomfort and flatulence.21,22 This is mainly observed with short water-soluble fibres. Unless the subject is dehydrated, moderate increase of water intake does not affect colorectal function or reduce symptoms of constipation. An intake of two litres of water daily will, however, enhance the positive effects of dietary fibre. 23
Constipation is strongly associated with immobility. In healthy subjects physical activity stimulates colorectal motility thereby reducing colonic transit time. 24 In patients with chronic idiopathic constipation, moderate physical activity 30–60 min per day improves stool consistency. 25 In patients with drug-induced constipation, it should be considered if the drug can be substituted with another less likely to cause constipation.
Basic treatment with laxatives
Basic and advanced treatment of chronic constipation
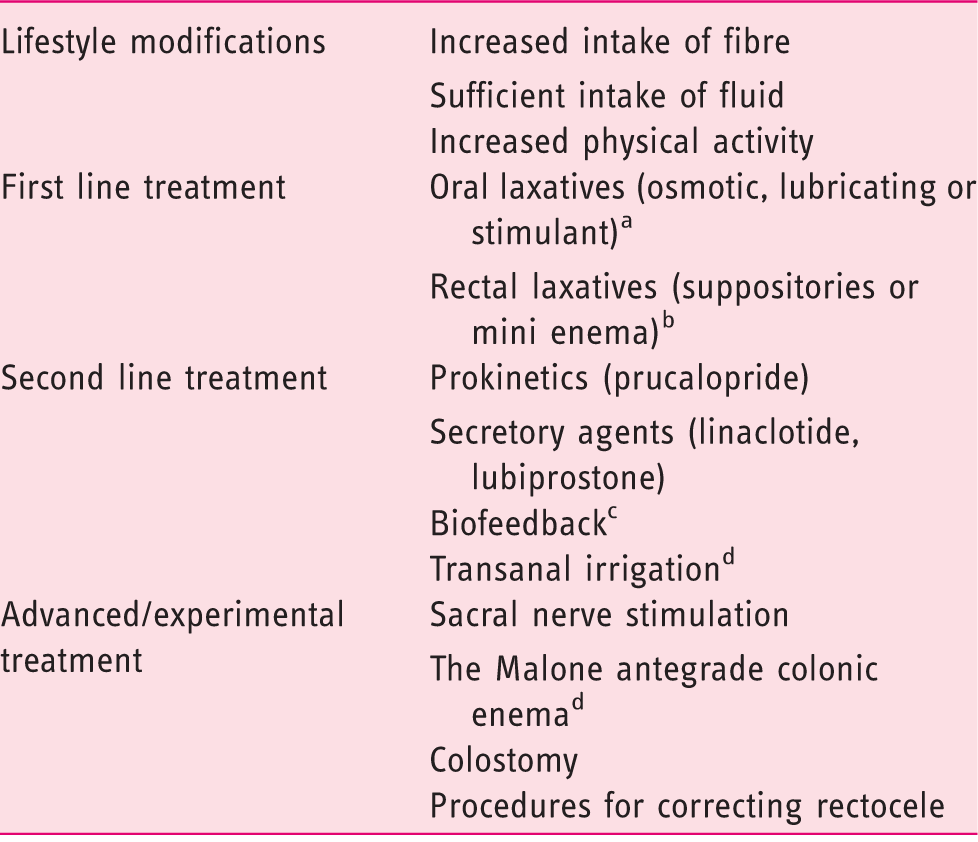
No data exist to recommend one oral laxative against others.
For patients with symptoms of evacuatory dysfunction.
For patients with dyssynergic defecation.
Mainly for patients with constipation secondary to neurological disorders.
Most commonly used laxatives have been used for several decades and only few publications have documented their effect. Thus, no placebo controlled study exists on the efficacy of magnesium. Randomised trials have shown that lactulose in superior to placebo. 26 Also, placebo controlled trials have found that PEG reduces symptoms of CC.27,28 Unfortunately, no study has been performed to compare the most commonly used laxatives to each other or to investigate whether there is an additional effect from combining laxatives. Therefore, choice of laxative will be determined by local preferences and cost.
In patients with difficult rectal evacuation and in patients with the combination of constipation and faecal incontinence, suppositories or mini enema should be attempted.
Prokinetics and secretagogues
Prucalopride is a 5HT-4 agonist with enterokinetic properties. In randomized placebo-controlled, clinical trials, prucalopride reduced colorectal transit times and alleviated symptoms in patients with idiopathic CC. 29
Linaclotide and lubiprostone enhance secretion from the gut wall and thereby reduce colorectal transit time and symptoms. Both linaclotide and lubiprostone have proven superior to placebo in double-blind placebo-controlled trials among patients with CC.30–32 Even though the effects of prucalopride, linaclotide and lubiprostone against CC are well-documented, the number needed to treat in order to reach a meaningful clinical response is approximately 3–5. In Europe, linaclotide has so far only been approved for IBS-C, but in several other countries including the US it has been approved on wider indication also including CC.
Biofeedback
Biofeedback (BFB) therapy is an instrument-based conditioning treatment which aims to restore a normal pattern of defecation by training the patient on adequate use and coordination of abdominal and pelvic floor muscles. In addition, some centres focus on enhancing rectal sensory perception, but this is without clear evidence of incremental benefit.
It has been debated whether BFB has a positive effect on constipation in general or only in those with functional defecation disorder. 8 However, recent data show that BFB has long-term effect against constipation due to functional defecation disorder only. 33 Recently, randomized controlled clinical trials have provided unequivocal evidence that biofeedback therapy is effective both short and long-term for severe constipation due to dyssynergic defecation.34–36 Thus, instrument-based biofeedback is more effective than pelvic floor exercises (Kegel’s training), sham biofeedback, conservative treatment and laxatives (Macrogol). Potential limitations are the access to high level of therapist expertise and patient motivation.
Transanal irrigation
Transanal irrigation (TAI) with a water enema installed through the rectum was introduced against severe constipation and faecal incontinence in children with spina bifida or anorectal malformations. 37 In adult patients the primary indication is neurogenic bowel dysfunction. When performed correctly, TAI will empty the colorectum distal to the splenic flexure. 38 In a randomized trial among patients with severe constipation and faecal incontinence after spinal cord injury, TAI was superior to ‘best standard care’. 39 The procedure is, however, time consuming as most patients need to perform it every second day and the time spent at each procedure is 30–45 min. Thus, the proportion of patients continuing treatment after three years is approximately 50%. 40 Furthermore, TAI may be useful in patients with evacuation disorders after anorectal surgery or congenital malformations. 41
Surgical treatment of CC
Sacral nerve stimulation (SNS) is a minimally invasive procedure whereby an electrode is placed in a posterior foramen of the sacral bone. SNS may alleviate CC in approximately 50% of highly selected patients. 42 The mechanism of action for SNS in CC remains obscure and further studies are need to confirm the clinical effects.
By the Malone operation, also termed the antegrade colonic enema (ACE), a small stoma is constructed from the appendix. 43 Through the appendicostomy a catheter can be inserted to administer the enema in the caecum. Usually 1.000 ml are given every second day to empty the whole colorectum. 44 If the patient no longer has the appendix, a ‘neoappendix’ can be created from ileum or part of the caecum. The ACE is mainly used in patients with severe constipation or faecal incontinence secondary to neurological disorders. The procedure is safe but minor complications are extremely common, i.e. experienced by up to 80%, especially because of stenosis of the appendicostomy. The ACE is only used at few institutions and high reversal rates have been reported. However, with thorough selection and instructions of patients long-term results may be good. 45
Colectomy with ileorectal anastomosis is reserved for a very small group of patients with severe symptoms not responding to other kinds of treatment. In most cases, colectomy will increase the frequency of defecation and reduce the use of laxatives. 46 However, the quality of studies on the subject is very variable and guidelines for selection of patients with CC for colectomy do not exist. 46 The pathophysiology of CC is complex, including some with pan-enteric dysfunction, and often colectomy does not solve the clinical problem. Furthermore, the rate of perioperative complications has been reported as high as 43% with a readmission rate after 30 days of 29%. 47
Special considerations in patients with secondary constipation
Constipation is very common in patients with neurological disorders. Thus, up to 95% of patients with spinal cord injury suffer from constipation,48,49 including 65% who have to perform digital stimulation or evacuation of the anorectum. 49 Constipation is also reported by approximately 40% of patients with multiple sclerosis, 50 and by 79% of patients with spina bifida. 51 The patients very often suffer from a combination of faecal incontinence and constipation.48–51 Therefore, treatment will aim at emptying the rectosigmoid either through digital anorectal stimulation or with mini enema (Clysma). If this fails TAI is an option. 39 A pilot trial has indicated that prucalopride has an effect against constipation secondary to spinal cord injury. 52 Patients not responding to conservative treatment or patients with very poor mobility and hand function can be offered ACE, 45 or a colostomy/ileostomy.
Patients with Parkinson’s disease have constipation partly because of reduced number dopaminergic neurons in the colon and autonomic neuropathy and partly because of dystonia of the striated external anal sphincter muscle.53,54 The main symptom is difficult evacuation. 55 The severity of constipation is associated with the severity of Parkinson’s disease. 55 Treatment will usually include dietary fibre in combination with laxatives or prokinetics. 56
Some patients with myopathy of the gut, especially patients with systemic scleroderma, may have constipation while others have diarrhoea or faecal incontinence. 57 Diabetic autonomic neuropathy may affect transit through all regions of the gastrointestinal tract. Some patients have severe constipation while others have intractable diarrhoea. 58 As with patients with myopathy, objective information about regional transit times is important in order to target treatment which usually includes laxatives or prokinetics.
Treatment with opioids will usually cause constipation. Standard treatment with laxatives should be attempted. If this fails, prucalopride or the mu opioid receptor antagonist naloxegol should be attempted.59,60
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.