
Abstract
Background
Chronic anal fissure is a frequent and disabling disease, often affecting young adults. Botulinum toxin and lateral internal sphincterotomy are the main therapeutic options for refractory cases. Botulinum toxin is minimally invasive and safer compared with surgery, which carries a difficult post-operative recovery and fecal incontinence risk. The long-term efficacy of Botulinum toxin is not well known.
Objective
The aim of this study was to evaluate the long-term efficacy and safety of Botulinum toxin in the treatment of chronic anal fissure.
Methods
This was a retrospective study at a single center, including patients treated with Botulinum toxin from 2005 to 2010, followed over at least a period of 5 years. All patients were treated with injection of 25U of Botulinum toxin in the intersphincteric groove. The response was registered as complete, partial, refractory and relapse.
Results
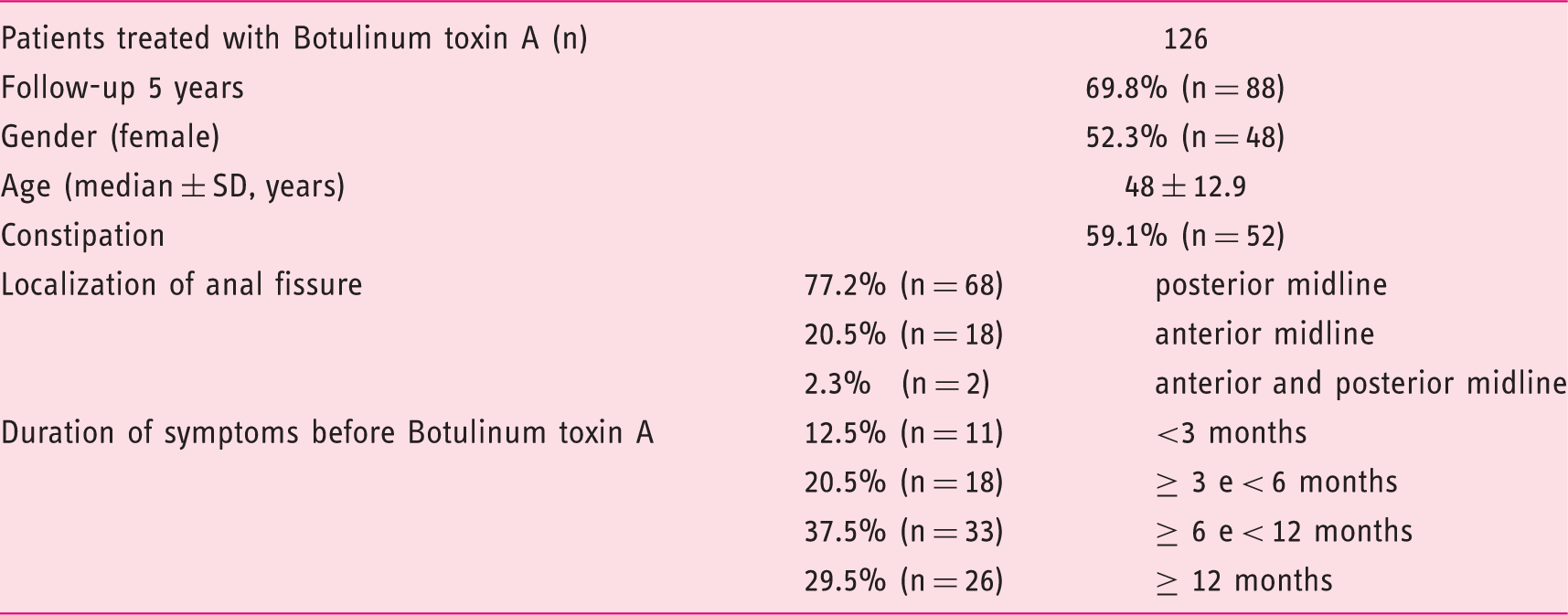
Botulinum toxin was administered to 126 patients, 69.8% (n = 88) were followed over a period of 5 years. After 3 months, 46.6% (n = 41) had complete response, 23.9% (n = 21) had partial response and 29.5% (n = 26) were refractory. Relapse was observed in 1.2% (n = 1) at 6 months, 11.4% (n = 10) at 1 year, 2.3% (n = 2) at 3 years; no relapse at 5 years. The overall success rate was 64.8% at 5 years of follow-up. Botulinum toxin was well tolerated by all patients and there were no complications.
Conclusion
The use of Botulinum toxin to treat patients with chronic anal fissure was safe and effective in long-term follow-up.
Introduction
Anal fissure is a linear ulcer in the anal canal, distal to the dentate line.1–3 Chronic anal fissure is a frequent and disabling disease, affecting both genders and especially young adults. 4 The clinical hallmarks are post-defecatory pain and/or bleeding. A chronic fissure is defined as a fissure that has not healed after more than 4–12 weeks of treatment.1–3,5
The pathogenesis of chronic anal fissure remains poorly understood. The sphincter spasm seems to cause relative local ischemia that precludes the healing of the fissure.1,6
Most cases of idiopathic fissure are located in the posterior midline (where the blood supply is relatively low), but other locations are also found. 3 Fissures in lateral positions should raise suspicion for an underlying disease such as Crohn’s disease, venereal infection, trauma, tuberculosis, human immunodeficiency virus, dermatologic conditions, chemotherapy and local or systemic malignancy.2,3
Current therapies for chronic anal fissure aim at the reduction of the tonus of the internal anal sphincter and relief of symptoms. First-line treatment includes conservative measures (fiber supplement, increase water intake, proper anal hygiene, laxatives, anti-inflammatory/analgesics/anesthetics and healing ointments) and topical treatment (nitrates and calcium channel blockers ointments). 7 A systematic review demonstrated that both diltiazem and glyceryl trinitrate are equally effective in the management of chronic anal fissure (48–88% and 33–68%, respectively). 3 However, diltiazem is associated with a lower incidence of headache and recurrent fissure and thus should be the preferred option. 3
Botulinum toxin (BT) and lateral internal sphincterotomy (LIS) are the main therapeutic options for refractory fissures. BT causes a temporary sphincter paresis for approximately 3 months, allowing fissure healing: the release of acetylcholine at the presynaptic nerve endings with neuromuscular transmission blockade causes a chemical denervation of the sphincter muscles. 6 Although BT has been in use since the 1990s, 8 currently there is no consensus on dosage, precise site of administration or number of injections to perform.6,7 BT is a safe and effective treatment, well tolerated, minimally invasive and administered on an outpatient basis. It causes a temporary lesion of the anal sphincter, and subsequently some patients may develop transient flatus (up to 18%) or fecal (5%) incontinence, that resolves quickly.3,9
Surgery is reserved for medically refractory cases. LIS is considered as the first-line surgical option for the patients who have failed to respond to conservative management.1,5,10
Three meta-analyses showed that LIS was superior to BT in terms of healing rate and lower recurrence rate. On the other hand, BT is safer and associated with a significant lower rate of incontinence.10–12 The lack of studies with a long-term follow-up seems to be a limitation. 10 The main purpose of this study was to evaluate the long-term efficacy and safety of BT in the treatment of anal fissure.
Materials and methods
This was a retrospective observational study at a single center that included 126 patients with chronic anal fissure treated with BT between 2005 and 2010. Chronic anal fissure was defined as an ulceration in the posterior or anterior anoderm for at least 8 weeks. All patients had failed previous conservative and topical therapies. Patients with other conditions (perianal fistulas or abscesses) or with previous surgery on the anal canal were excluded.
Botulinum toxin type A (Botox®) was injected into the intersphincteric groove or in the internal anal sphincter while the patient was lying in knee-to-chest position. A total dose of 25U was diluted in 0.5 ml isotonic saline and was injected with an insulin syringe (26G needle). Half of the total dose was injected on both sides of the fissure (at 3 and 9 o’clock positions). No sedation or local anesthesia was used. The patient was discharged immediately after the procedure. Follow-up data were obtained for a period of at least 5 years. Patients were re-examined at 3 and 6 months, and 1, 3 and 5 years later. During follow-up, perianal examination was performed and patients’ records were reviewed for symptoms or side effects.
The response to treatment was registered as complete (symptomatic remission and complete fissure cicatrization), partial (symptomatic improvement but persistence of the fissure), refractory (without symptomatic improvement or fissure cicatrization) and relapse (recurrence of symptoms and appearance of fissure after complete response).
The primary endpoint of the study was complete healing and symptomatic improvement after BT treatment. All patients without a complete response at 6 months were offered a second injection of BT or surgery.
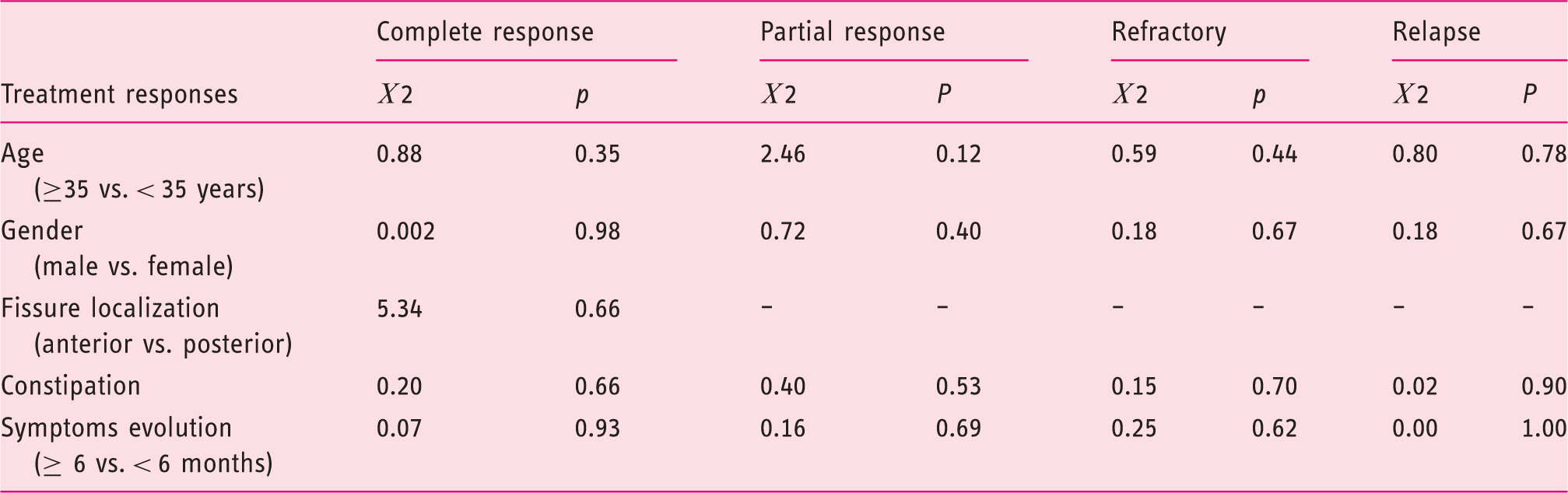
Statistical analysis was performed using SPSS® (version 21.0 for Windows®, SPSS inc®, Chicago, IL, USA). The results are expressed as absolute frequency (n), percentages (%) and means ± standard deviation. The relationship between clinicodemographic characteristics and response to treatment with first BT treatment were analyzed with use of Chi-Square Test (χ2). P-values of less than 0.05 were considered to indicate statistical significance.
Results
Demographic and clinical characteristics (%, percentage; n, absolute frequency); SD, standard deviation)
At 3 months of follow-up, 76.1% (n = 67) patients had satisfactory response, complete response was obtained in 46.6% (n = 41) and partial improvement in 23.9% (n = 21). No response was verified in 29.5% (n = 26). Relapse was observed in 1.2% (n = 1) at 6 months, 11.4% (n = 10) at 1 year, 2.3% (n = 2) at 3 years; no relapse at 5 years. Treatment and responses are shown in Figure 1 and Table 2. There was no difference between the groups with complete response and refractory for gender, age, duration of symptoms, fissure localization and constipation (see Table 3).
Flow chart showing the clinical course and the treatment options during 5 years-follow-up (n; absolute frequency). Clinical responses to first injection of Botulinum, to second injection of Botulinum toxin and to lateral internal sphincterotomy at 5-year follow-up (%, percentage; n, absolute frequency) Relationship between demographic and clinical characteristics and response to treatment with first BT treatment (Chi-Square Test (χ2), confidence interval 95%, (-) invalid data)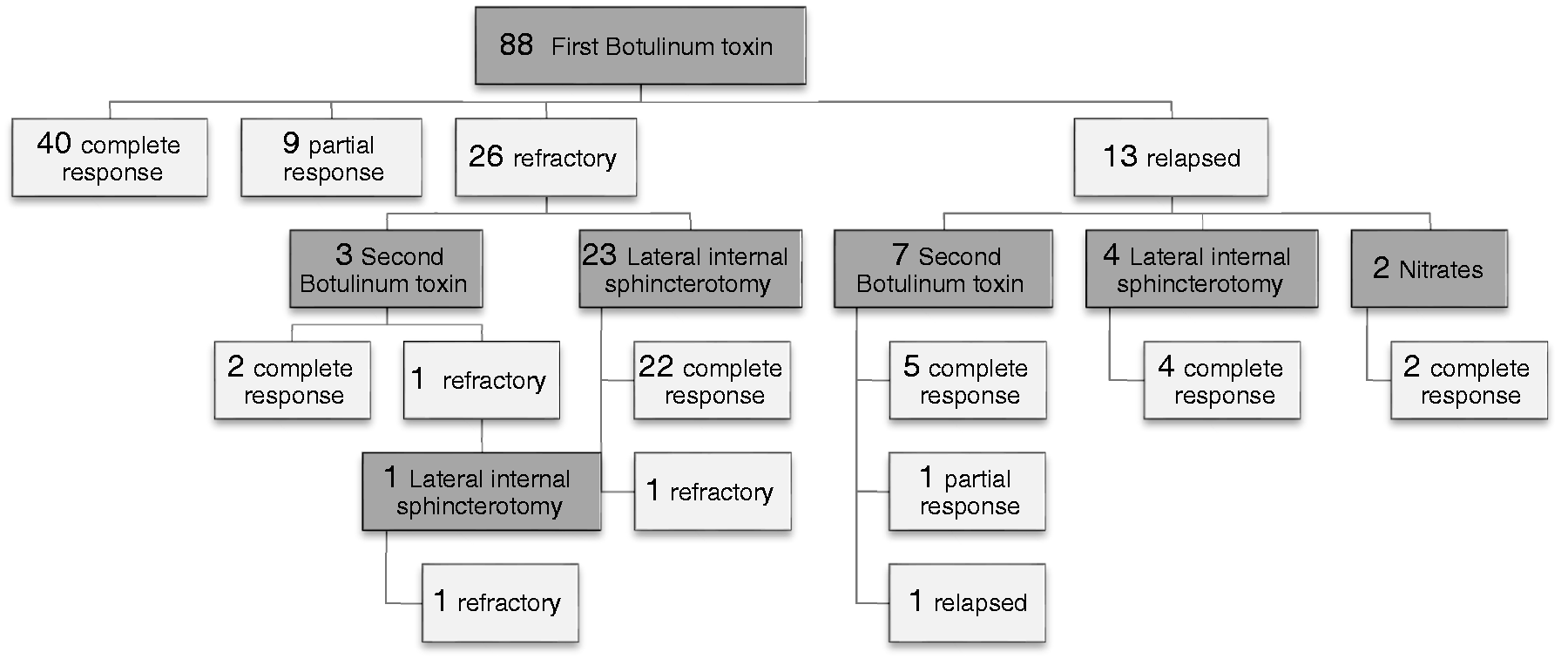
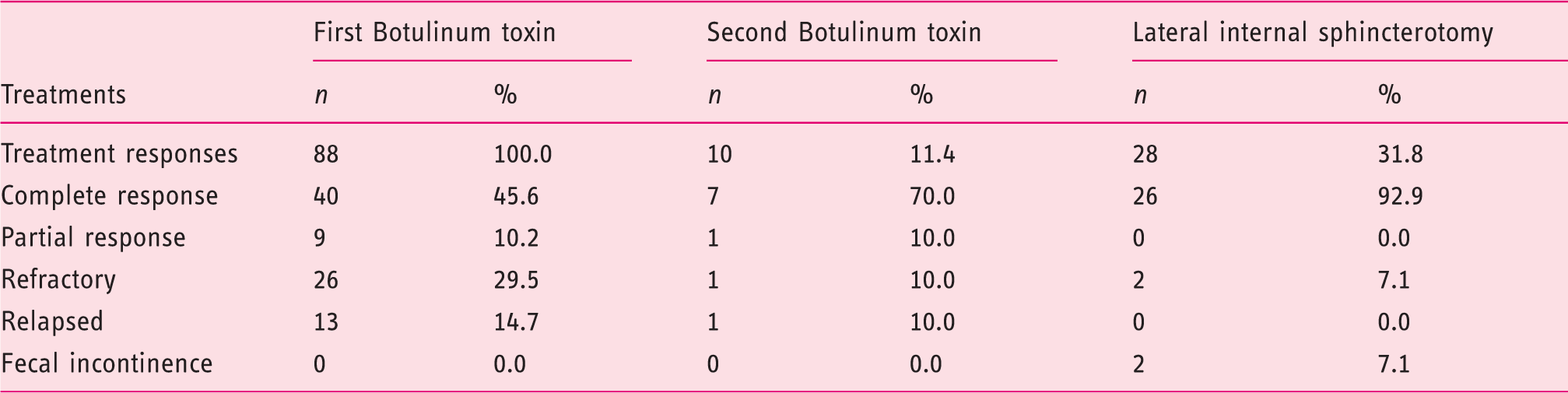
Non-satisfactory response to first BT treatment, either no response or relapsed, was observed in 44.3 % (n = 39). All these patients were referred to general surgery consultation. Twenty-eight patients were submitted to LIS and 26 patients improved after surgery (the surgery success rate was 92.9%). Ten patients with non-satisfactory response refused surgery and were assigned to second injection with BT with 80% (n = 8) efficacy (see Figure 1 and Table 2).
At 5 years’ follow-up, the treatment with BT was considered long-term efficacious in 64.8%, including those with complete response or adequate symptoms and the patients submitted to a second BT injection. This symptom relief was accomplished avoiding surgery.
The BT injections were well tolerated and there were no complications or side effects. The surgical approach was associated with a difficult post-operative recovery with significant anal pain in all the patients, and there were two (7.1%) patients with fecal incontinence, one of them with permanent incontinence.
Discussion
Anal fissures are painful and can cause significant discomfort and stress for a patient. BT emerged as a valuable minimally invasive treatment to chronic anal fissure refractory to conservative management with dietary modifications, anal hygiene, diltiazem and nitrates. The dosage of BT reported ranged from 20 to 100U, with several methods of injection application (directly under the fissure or in both sides of the fissure or circumferential injections). There is no dosage or procedure with evidence of superiority.2,3,7,11 Our procedure included two injections of 12.5U of BT injected on both sides of the fissure, with a 5-year follow-up efficacy of 64.8% and with no related complications. This supports the hypothesis that BT injection is an effective and safe therapy for chronic anal fissures after patients fail conservative management, and these results are similar to the literature. A systematic review showed a BT overall healing rate of 67.5%. 2 Nevertheless, the previous results in healing rate diverge between 41–90.7% at 3 months, with recurrence rates of 20.6–54% at 6 months in different studies.3,7,9,11,13–16
Our series also proved that BT efficacy was maintained during long-term follow-up (5 years). In fact, we verified that the recurrence was 11.4% at 1 year, with no significant recurrence at 3 and 5 years of follow-up. Our data showed a lower recurrence rate compared with a systematic review that revealed a recurrence of healed fissure exceeding 40–50% after 1 year. 2
A second injection of BT could be an important therapeutic solution for patients with non-satisfactory response to a first injection, because it was effective (80%), well tolerated and with no complications. However, in our series, it was only performed in those patients who had non-satisfactory response and refused surgical intervention. This result was also similar to the literature, where healing rates are around 60–95% after the second session of injections, with recurrence rates of 12.5% at 6 months and with no reports of anaphylaxis.2,3,7 The value of a second injection of BT was also reflected by patients’ opinions, with almost one-third (30.8% n = 12/39) of patients with non-satisfactory response after first BT injection refusing surgery after acknowledging the possible complications.
Currently, LIS is the treatment of choice for chronic fissures that fail conservative management, achieving higher healing rates (68–100%) and lower recurrence rate than BT.5,10,11,15 LIS, which permanently weakens the sphincter, carries a more difficult post-operative state and may be associated with anal deformity. 1 Despite this high efficacy, LIS is associated with higher rates of incontinence than BT; up to 47.6% of patients after LIS found some level of post-operative disturbance of continence.5,10–12 A recent meta-analysis showed that long-term risk of continence disturbance after LIS is significant (approximately 15%), with frank fecal loss in about 1%. 5 Our data showed 7.1% of patients with fecal incontinence after surgery. Rare complications of LIS include infection, fistula formation and local hematoma; 1 none of these were reported in our results. Other innovative sphincter-saving surgical techniques, such as fissurectomy alone or combined with BT injection/anoplasty and flap procedures with BT injection, revealed a high healing rate without surgical sequelae or anal incontinence.5,6,17–19
Due to the rate of incontinence and the invasiveness of surgery, BT has gained recognition. Compared with surgery, the BT procedure is simpler, cheaper, minimally invasive and well tolerated, does not need anesthesia, is performed in an outpatient setting, and patients are discharged immediately, with a resting period after the procedure not necessary. Long-term efficacy is almost 65% for 5 years, with minimal risk of incontinence, and treatment is easy to re-administer if failed initially, with high efficacy (80% healing rate).
The absence of a control group, lack of anorectal manometry examinations, possibility of observer bias (clinical follow-up data of patients were recorded by different doctors) and the study design (retrospective analysis) are the key limitations of this study.
In conclusion, our results support that BT is safe, effective and durable option for the management of chronic anal fissure, and offers the possibility of avoiding a sometimes inevitable, but more expensive and complex, surgical option, with the risk of incontinence associated with LIS.13,15
This study supports the hypothesis already described, 13 that BT may be the first-line therapy for chronic and medical refractory anal fissure and a surgical approach should only be recommended for patients in whom repeated BT injections fail or for patient preference, demanding a more aggressive treatment. Further randomized control trials including more patients with long-term follow-up are needed to confirm our results.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.