
Abstract
Background
Treatment options for achalasia include endoscopic and surgical techniques that carry the risk of esophageal bleeding and perforation. The rare coexistence of esophageal varices has only been anecdotally described and treatment is presumed to carry additional risk.
Methods
Experience from physicians/surgeons treating this rare combination of disorders was sought through the International Manometry Working Group.
Results
Fourteen patients with achalasia and varices from seven international centers were collected (mean age 61 ± 9 years). Five patients were treated with botulinum toxin injections (BTI), four had dilation, three received peroral endoscopic myotomy (POEM), one had POEM then dilation, and one patient underwent BTI followed by Heller's myotomy. Variceal eradication preceded achalasia treatment in three patients. All patients experienced a significant symptomatic improvement (median Eckardt score 7 vs 1; p < 0.0001) at 6 months follow-up, with treatment outcomes resembling those of 20 non-cirrhotic achalasia patients who underwent similar therapy. No patients had recorded complications of bleeding or perforation.
Conclusion
This study shows an excellent short-term symptomatic response in patients with esophageal achalasia and varices and demonstrates that the therapeutic outcomes and complications, other than transient encephalopathy in both patients who had a portosystemic shunt, did not differ to disease-matched patients without varices.
Keywords
Introduction
Achalasia is a very uncommon primary motor disorder of the esophagus characterized by incomplete relaxation of the lower esophageal sphincter (LES) and impaired esophageal motility.1,2 This clinically presents with symptoms of dysphagia, regurgitation, chest pain, and/or weight loss. All current treatments aim at reducing LES resting pressure with botulinum toxin injection (BTI), pneumatic dilatation, peroral endoscopic myotomy (POEM), or Heller's myotomy commonly with a partial anti-reflux procedure. 2
The presence of portal hypertension with varices is infinitely rarely reported to occur in conjunction with achalasia and the choice of treatment in this context represents a challenging therapeutic dilemma, even in specialized centers. To the best of our knowledge, 12 cases reports have been described in the literature with only eight patients having received treatment.3–13 The limitation of oral food intake and subsequent weight loss observed in achalasia will inevitably have detrimental consequences in cirrhotic patients; significant weight loss and malnutrition could aggravate pre-existing hypoalbuminemia, precipitating cirrhosis complications (i.e. ascites and spontaneous bacterial peritonitis) and expose patients to cachexia and/or vitamin deficiency and its sequelae. 14 Furthermore, persistent food stasis and progressive esophageal dilatation can increase the risk of esophagitis which could conceivably increase the risk of inflammation, erosion and ulcer formation and subsequent variceal bleeding. On the other hand, all achalasia treatments themselves carry the burden of complications, including bleeding and full thickness esophageal perforation, the consequences of which could be compounded, even life-threatening, in patients with cirrhosis. 15 Therefore, the risks of the interventions must be carefully weighed against the intended benefits. Yet, due to the paucity of published data and the rarity of this combination of disorders, the therapeutic management and the outcomes of different treatment modalities have only been anecdotally described. To this aim, we describe the trends in therapeutic interventions undertaken in the largest cohort of achalasia patients with varices treated at tertiary care institutions around the world.
Methods
Study design
This is a retrospective, multicenter case-series of patients with achalasia and concomitant esophageal varices who received treatment at seven international tertiary referral centers: University College Hospital (UCH, London, United Kingdom), Royal Adelaide Hospital (Australia), Washington University (St Louis, USA), Edouard Herriot Hospital (Lyon, France), University of Padova (Italy), University “Federico II” (Naples, Italy), and Amsterdam Medical Centre (Netherlands). Experience from physicians/surgeons treating this rare combination of disorders was sought through the International Manometry Working Group. As this was a retrospective assessment from multiple international centers, acquiring consent was not possible; however, all patient data were rigorously anonymized during the data collection and analysis process.
Study patients
Achalasia patients with concomitant varices presenting between 2008 and 2016 were retrospectively reviewed. The pre-treatment evaluation of patients included Eckardt score symptom assessment, endoscopic evaluation, esophageal varices grading, barium swallow and high-resolution esophageal manometry (HRM). 16 Most cases were reviewed in multidisciplinary settings and the decision of the type of treatment was endorsed by weighing the individual risk-to-benefit ratio on a case-by-case basis. In all patients, a careful retrospective chart review was performed, recording variables including age, gender, type of treatment, need for re-intervention, treatment of esophageal varices and timing of variceal eradication (i.e. pre- or post-achalasia treatment), etiology, and severity of concomitant liver disease as assessed by the Child–Pugh score. 17 The occurrence and type of any endoscopic and/or post-endoscopic complications were also sought.
Prior to treatment, achalasia severity was assessed by using the Eckardt score, according to previously standardized methods. 18 Patients were followed up at one and approximately 6 months after the initial treatment and the symptomatic response was reassessed. In agreement to that reported from previous studies, treatment success was defined as a decrease in the Eckardt scores to less than 3. 19 Twenty age-matched achalasia patients without varices who were treated at UCH served as disease-matched controls.
Statistical analysis
The data were entered into an anonymized database and analysis was performed using SPSS (Statistical Package of the Social Sciences) 10.0.1 for Windows. The Eckardt score values are presented as median/interquartile range (IQR) and the change in total Eckardt score before and after treatment was compared using paired Student's t-test for parametric variables. An α-error ≤ 0.05 was considered as statistically significant.
Results
Patient demographics
Characteristics, treatment and outcomes of all 14 patients with achalasia and esophageal varices.
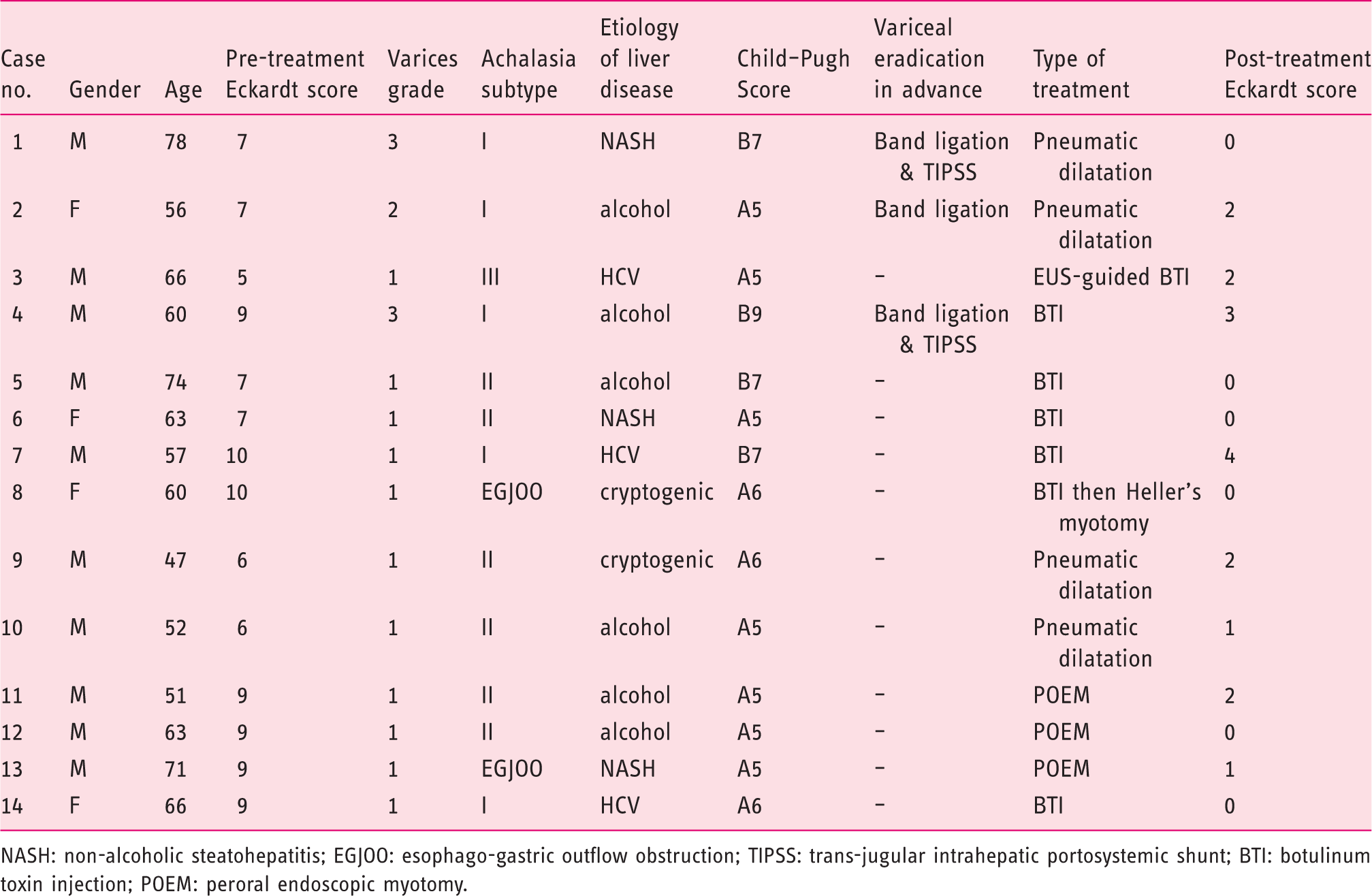
NASH: non-alcoholic steatohepatitis; EGJOO: esophago-gastric outflow obstruction; TIPSS: trans-jugular intrahepatic portosystemic shunt; BTI: botulinum toxin injection; POEM: peroral endoscopic myotomy.
As part of their diagnostic work-up, 10/14 (69%) patients had a barium swallow and all but one had an HRM study performed. Based on the HRM results, patients were subcategorized as having type I (4 patients), type II (6 patients), type III achalasia (2 patients), and/or esophago-gastric junction outflow obstruction (EGJOO) (2 patients), in accordance with the Chicago classification. 21 One of the patients did not tolerate pre-treatment manometry but the diagnosis of advanced Type I achalasia was based on clinical, endoscopic, endoscopic ultrasound (EUS), and radiological findings. The median pre-therapy Eckardt score was 7.8 (IQR 6–9). Table 1 summarizes the baseline characteristics of the studied population.
Interventions
The decision of the type of treatment was often endorsed by a multidisciplinary team, taking into account the individual risk-to-benefit ratio on a case-by-case basis. Variables that impacted the decision-making process for treatments included age, severity of esophageal varices, pre-treatment symptom scores (i.e. absence of significant weight loss), baseline liver function tests (i.e. coagulation abnormalities and/or thrombocytopenia), one-year mortality risk of patients based on the overall comorbidities and associated cirrhosis, as well as achalasia subtype and mucosal disease. Three out of 14 patients (2 patients with F3 and 1 with F2 varices, respectively) underwent variceal eradication prior to achalasia therapy with endoscopic band ligation. In two patients with F3 varices, ligation was followed by a trans-jugular intrahepatic portosystemic shunt (TIPSS). None of the other 11 cases had variceal eradication in advance. Patients had a diverse selection of achalasia treatments. Six patients (mean age 63 ± 6 years) were treated with BTI, one of which under EUS guidance in attempt to avoid submucosal and peri-esophageal collaterals. One patient in the BTI group subsequently underwent Heller's myotomy as symptoms persisted at one-month follow-up. Five patients (mean age 58 ± 13 years) had pneumatic dilation to at least 30 mm. Finally, three patients (mean age 61 ± 10 years) received POEM, one of whom required subsequent pneumatic dilatation as symptoms persisted at 1-month follow-up (see Figure 1).
Selection of treatments used in the whole cohort of patients with achalasia and varices. At 1-month follow-up, three patients had persistent symptoms, two of whom were in the botulinum toxin group and one in the POEM group. One patient (Eckardt score 10) underwent Heller's myotomy and one patient (Eckardt score 7) had a subsequent pneumatic dilatation. The remaining patient had a partial symptomatic relief (Eckardt score 4) not limiting oral food intake.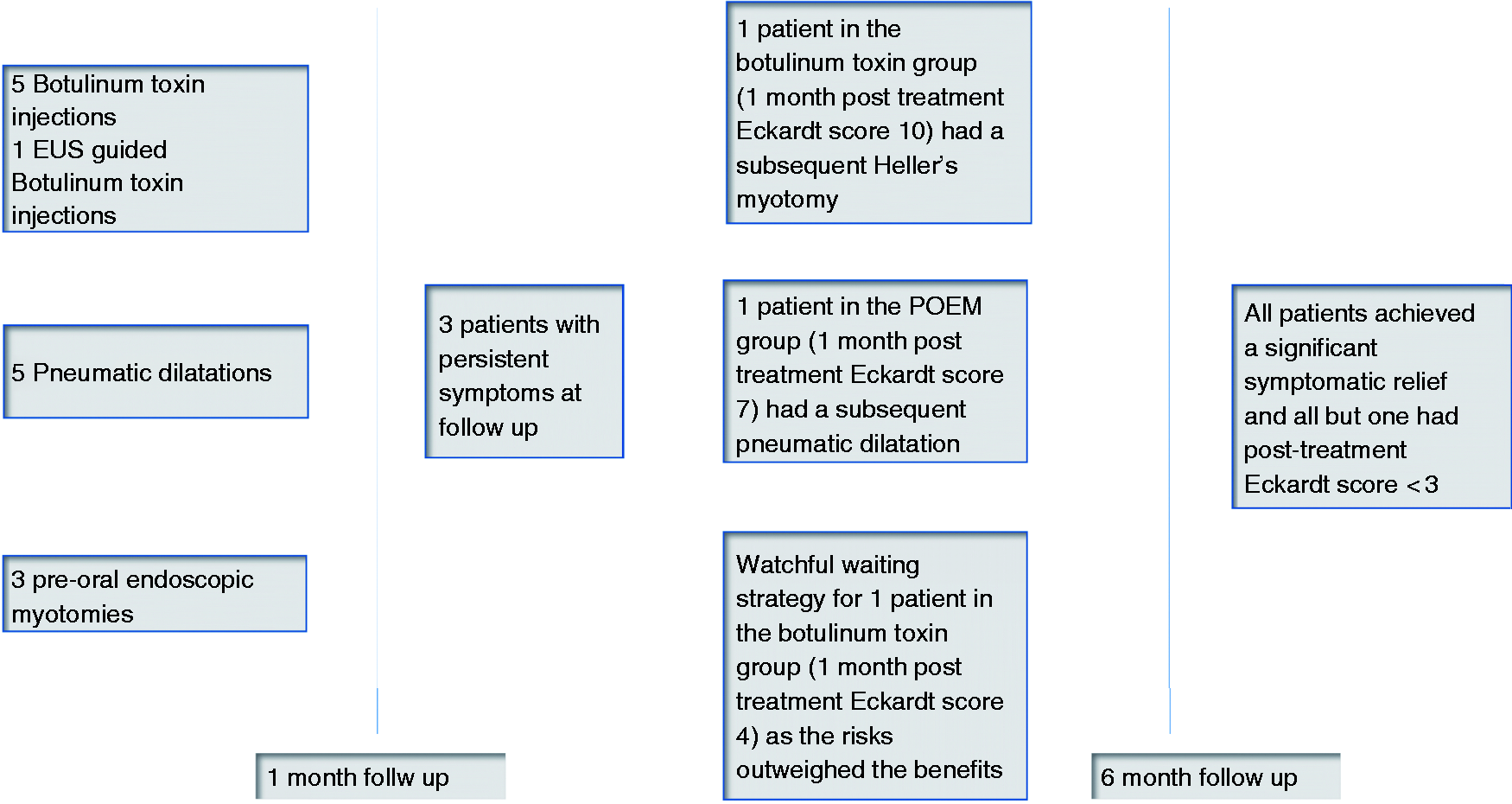
Treatments outcomes
All patients exhibited a significant symptomatic improvement at 6 months follow-up of their final procedure. The median post-intervention Eckardt score was 1.3 (IQR 0–2; p < 0.0001), with an average Eckardt score drop of 6.5 ± 2.0 compared to baseline. When considering the different treatment modalities, the changes in Eckardt scores were 5.8 ± 1.6 in the BTI group, 5.3 ± 1 in the pneumatic dilatation group, and 8.0 ± 1 in the POEM group, respectively. The only patient treated with Heller's myotomy scored zero 6 months after surgery, with a change in Eckardt score value of 10. All but one patient (in the BTI group; Eckardt score 4) had a final Eckardt score of ≤3 and were therefore considered as successfully treated. There were no complications related to bleeding or perforation post-operatively. However, both patients who underwent TIPSS developed a transient episode of acute encephalopathy, which delayed the pneumatic dilatation.
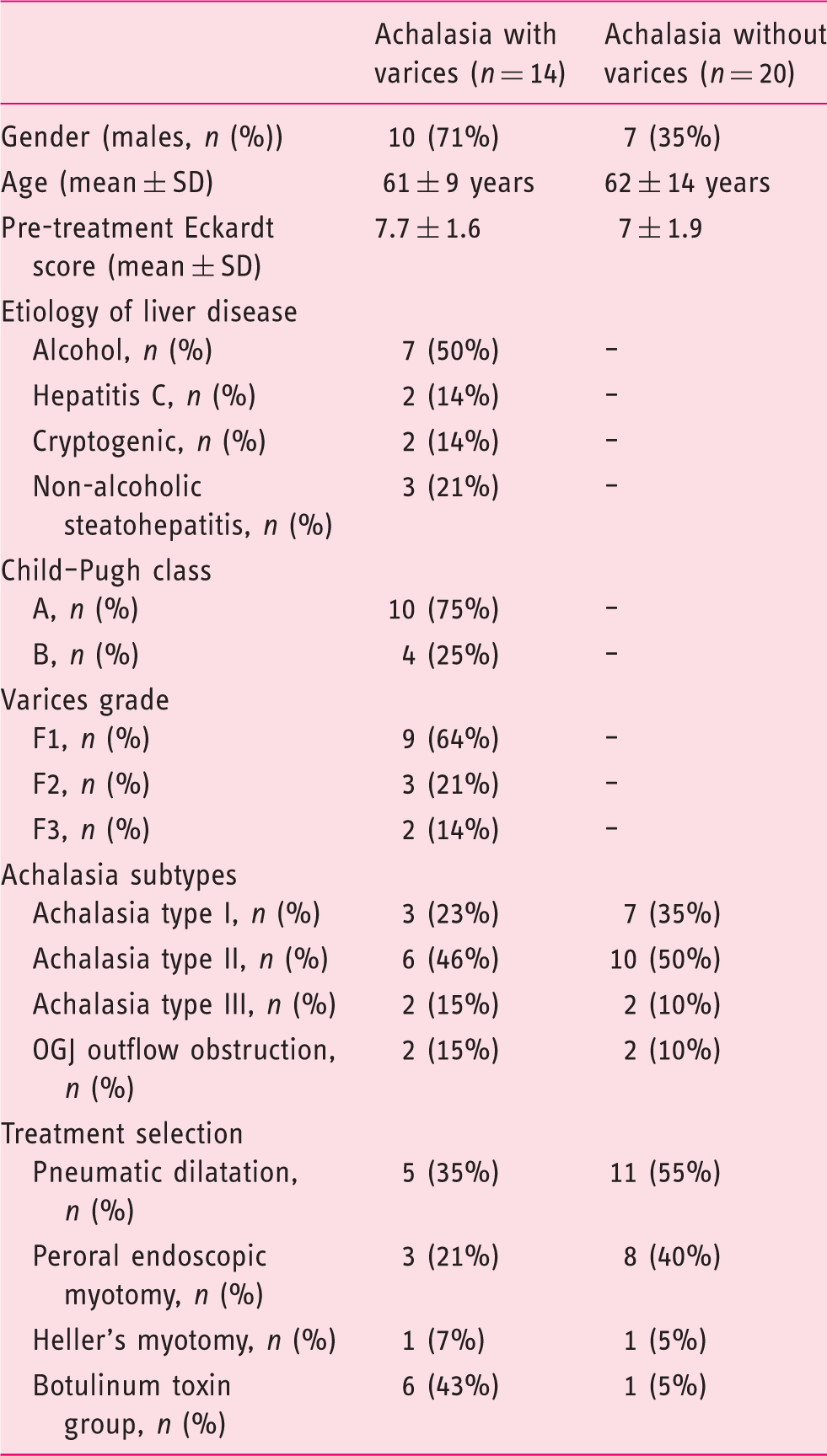
Twenty consecutive achalasia patients without varices (7 males, mean age 62.9 ± 14.8) served as disease- and age-matched controls. Table 2 summarizes the baseline characteristics of the controls. There were no significant differences in the average change of Eckardt score values (6.5 ± 2.0 vs 6 ± 1.1) or median post-operative Eckardt scores at 6-month follow-up (1.3 vs 1.0 ± 2.1) compared to baseline in patients with and without varices, respectively. The choice of treatment in disease-matched control patients without varices is depicted in Table 2. Only a single patient in the control group had undergone BTI as first line therapy. In the control group, one patient required pneumatic dilatation following the POEM procedure, whilst another had a subsequent Heller's myotomy following incomplete relief after dilatation. Also, in the control group, all but one patient had a significant improvement achieving a final Eckardt score of less than three and no differences were observed compared to the population of achalasia patients with varices (see Figure 2).
Mean pre- and 6 months post-treatment Eckardt score in the population of achalasia patients with varices (n = 14) compared to age and disease matched controls (n = 20). All patients displayed a significant reduction in Eckardt scores following treatment (at least a 2-point decrease compared to baseline). All but one patient in both populations had a 6-month Eckardt score ≤ 3. Baseline characteristics of achalasia patients with esophageal varices (n = 14) and controls without varices (n = 20). In the control group, one patient treated with POEM subsequently had to undergo a pneumatic dilatation in order to achieve a good symptomatic relief, whilst a patient who had pneumatic dilatation subsequently preceded to having a Heller's myotomy.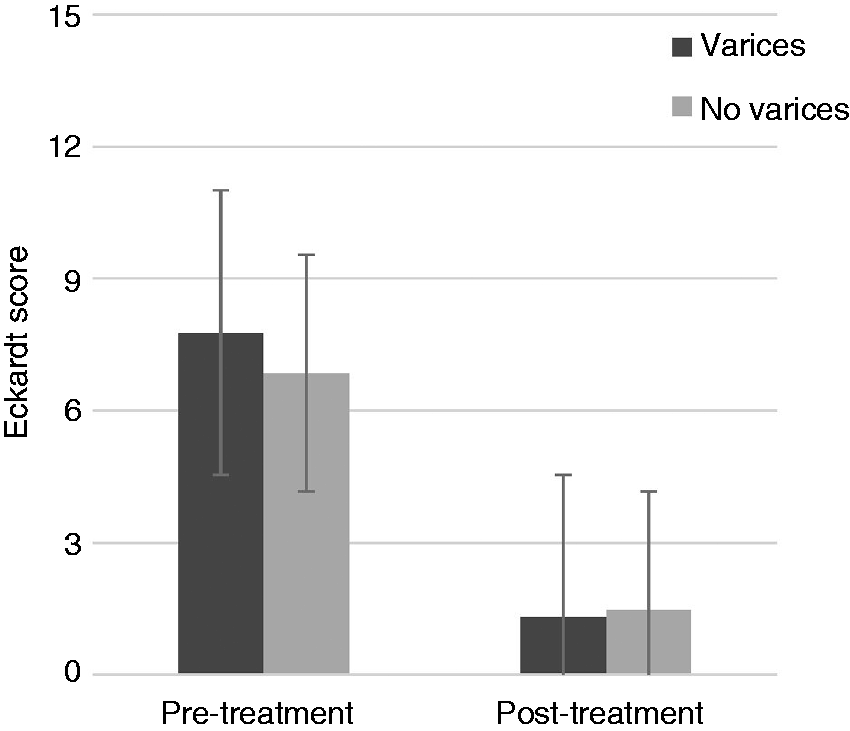
Discussion
The case series presented describes the experience of centers from around the world in investigating and treating patients with the rare combination of achalasia and esophageal varices. This study demonstrates excellent outcomes in terms of complications and symptomatic response, which did not differ to those of a disease-matched population of achalasia patients without varices. However, it must be noted that the presence of varices and the presumed increased risk of hemorrhage due to the underlying liver disease have strongly influenced the therapeutic decision-making. As compared to controls, in nearly 45% of the overall population of achalasia patients with varices, BTI (with or without EUS guidance) was the treatment of choice, whilst only a single patient in the control group had undergone BTI as first line therapeutic intervention.
Although recognized as one of the most common major esophageal motor disorders, achalasia represents a rare condition with an estimated prevalence of 10 in 10,000 and an incidence rate ranging from 1.07 to up to 2.8 new cases per year per 100,000 population.22,23 The coexistence of esophageal varices with achalasia is therefore infinitely rare, and to the best of our knowledge, is described in literature in only a small number of isolated case reports.3–13 A common presenting symptom of achalasia is restricted caloric intake and subsequent weight loss. Malnutrition in patients with cirrhosis is of concern, ranging from 50% up to 90%, rising alongside Child–Pugh score.24–26 In a large, nationwide analysis of cirrhotic patients, malnutrition has been associated with an increased incidence of complications including ascites, reduced survival, worsening hepatic function as well as risk of variceal bleeding and surgical morbidity and mortality.26,27 This suggests that the consequence of further reduction in oral intake related to esophageal achalasia will compound the risk further, potentially impacting on the long-term survival of patients. On the other hand, therapeutic interventions for achalasia carry a risk of esophageal bleeding and perforation, the consequences of which can be compounded by the coexistence of cirrhosis, especially considering the increased risk of hemorrhage, thrombocytopenia and coagulopathy. 28
All achalasia interventions have risks and benefits and the choice of therapy normally depends on the availability of local expertise as well as patient choice; 29 however; with the additional complexity of having portal hypertensive disease and varices, this decision needs to be carefully measured. Treatment options presented in this case series of 14 patients with achalasia and varices include BTI, pneumatic dilatation, surgical or endoscopic myotomy. Older patients, with their increased burden of comorbidities, pre-existing coagulopathy and/or thrombocytopenia have been successfully treated with BTI. The benefit of using EUS to guide therapy is not clear and previous case reports have suggested that EUS guidance could conceptually prevent the risk of inadvertent injection of toxin into the varices and can help avoid submucosal and peri-esophageal collaterals.5,6 Yet, in this cohort, only one patient had EUS-guided BTI with no difference in terms of outcome or complications observed compared to the others in the BTI group. The literature confirms that although BTI can exhibit a good symptomatic response in the short-term, it does not halt progression of achalasia, with less than 50% of treated patients maintaining a good response at one year. 30 In our series, one of BTI-treated patients subsequently required a Heller's myotomy; however overall, at short term follow-up of 6 months, only one patient had a suboptimal symptomatic response with an Eckardt score that remained above 3.
In younger patients, with lower grade varices and well-compensated liver cirrhosis, other therapeutic modalities can be undertaken safely. In this series, five of the 14 patients underwent pneumatic dilation to at least 30mm diameter, while four had surgical or endoscopic myotomy with no bleeding or perforation complications described.
It is not clear if variceal eradication should be undertaken in advance, and if so, if this should be with superficial eradication with band ligation and/or with diversion of portal flow with TIPSS. On one hand, variceal eradication might conceptually reduce the risk of bleeding, while on the other hand, it has been advocated that band ligation prior to achalasia treatment might induce esophageal scarring and, in turn, worsen the dysphagia; 4 however, in this series, there did not appear to be any difference in treatment outcomes in the patients who had band ligation prior to achalasia treatment (2 F2 and 1 F3 varices patients) compared to those who did not. In both patients who had TIPSS, there was a transient period of encephalopathy.
Although POEM is increasingly being advocated as first line therapy in many institutions, even in the elderly, 31 the additional consequence of varices, portal hypertension and comorbidities associated with cirrhosis is likely to influence therapeutic decision-making. This is indeed reflected in our cohort as only 21% of patients in the varices group underwent POEM compared to 40% in the controls.
Recent studies have shown that the 2- and 5-year outcomes following sequential pneumatic dilatation and laparoscopic Heller's myotomy are comparable, with a random-effects model risk ratio of 1.05 and 1.17 (p = 0.49 and 0.34 at 2 and 5 years follow-up, respectively).
32
However, as shown by a recent meta-analysis, esophageal perforation rates after laparoscopic Heller's myotomy were lower than balloon dilation (0.8% vs 4.9%), and during long-term follow-up (>6 years), nearly 25% of patients required repeated dilatations.30,33,34 This might compound the likelihood of potential complications with repeated invasive therapies in the context of concomitant varices and suggests that in patients with a favorable long-term survival based on the underlying liver disease with a low general anesthesia risk, it might be reasonable to consider single therapy, with surgical or endoscopic myotomy.
34
Based on this presumption, a suggested modified therapeutic algorithm for patients with achalasia and concomitant varices is presented in Figure 3. However, it is important to underline that these recommendations are based on experts' opinion, and caution should always be exercised when managing these patients, taking into consideration the theoretical risks of complications, preferably with the therapeutic decision-making being undertaken within a multidisciplinary setting with all relevant professionals.
Proposed therapeutic algorithm in patients with esophageal achalasia and varices. All treatment modalities offer benefits and can involve risk. The therapeutic choice should be endorsed by a careful multidisciplinary evaluation of the individual risk-to-benefit ratio based on the center's expertise.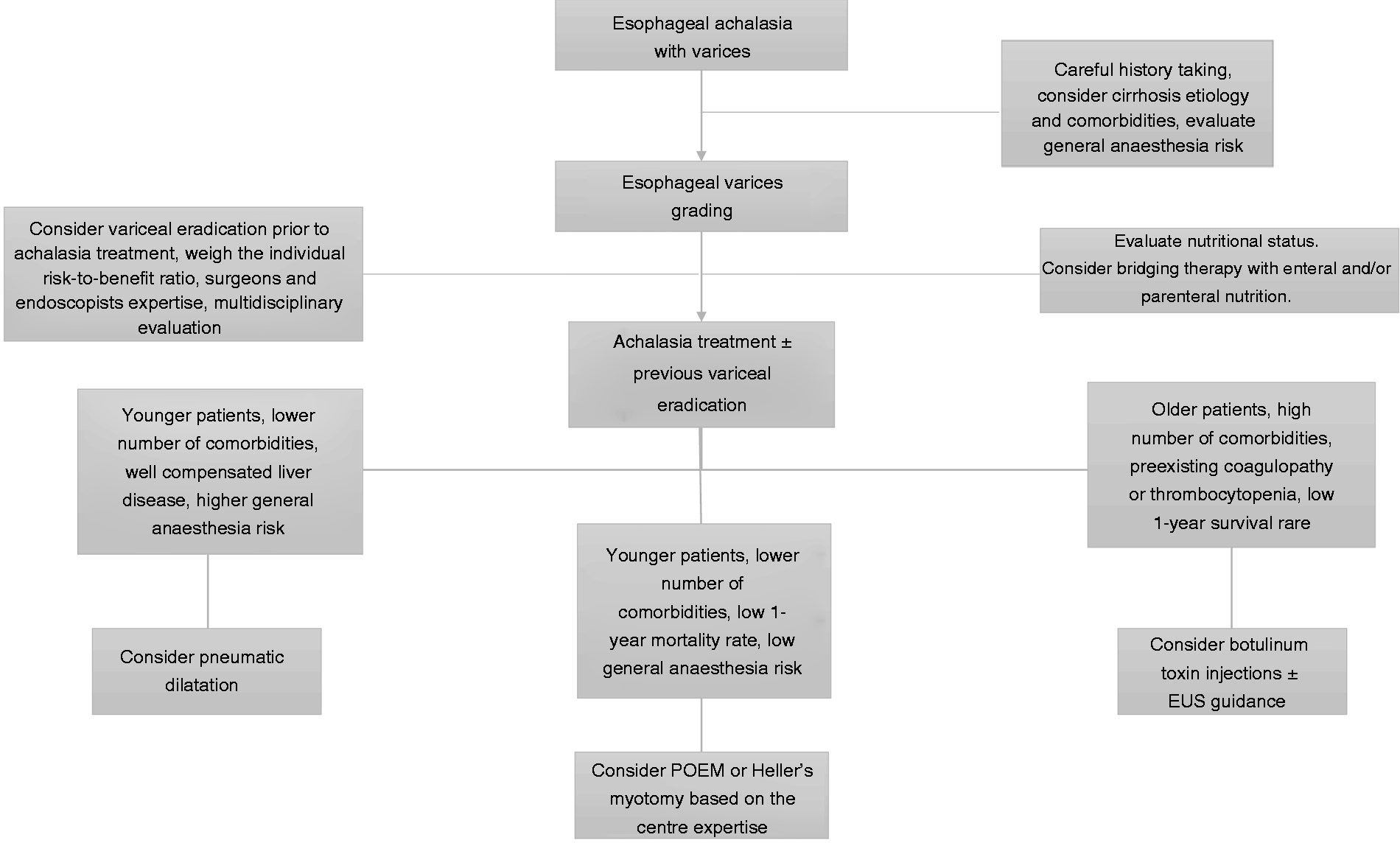
This study has several limitations that merit discussion. First, this is a retrospective case-series conducted over several years in tertiary referral centers. It therefore reflects the local expertise and experience in treating achalasia. Secondly, nearly 65% of subjects had low grade varices (F1) which might at least partially explain the absence of serious adverse events and/or major bleeding episodes. It is also possible that there was underlying reporting bias and that patients with favorable outcomes were preferentially volunteered for inclusion into this series. Furthermore, the decision for therapy was not standardized and not every treatment was based upon multidisciplinary discussion. Finally, the follow-up period is short (6 months), so no definite conclusions about the long-term therapeutic outcome can be drawn. Longer follow-up information was not possible as acquisition of patient information was based on a retrospective search from various international institutions, and beyond 6 months many patients were lost to contact, discharged, or deteriorated due to the underlying liver disease which either precluded further therapy or led to patient demise. Nonetheless, to the best of our knowledge, we herein report for the first time the outcomes of the largest population of patients with achalasia and varices. Our results suggest that, at least in the short-term, all treatment modalities can be safely considered with symptomatic outcomes mirroring those of standard achalasia without varices. It appears therefore that despite the presence of varices, all conventional achalasia treatments are safe and effective, provided that the interventions are performed in the specialized settings.
Footnotes
Declaration of conflicting interests
None.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
Informed consent was not required as this was a retrospective document based on historical data.
Ethics approval
Ethics approval was not required.