
Abstract
Background
Gastric subepithelial tumors represent a diagnostic and therapeutic challenge, given their histologic heterogeneity and potential malignant behavior.
Objective
The objective of this article is to evaluate the interest, efficiency and safety of endoscopic resection for subepithelial gastric lesions of size <20 mm.
Methods
We conducted a single-center retrospective study in a tertiary care center.
Results
A total of 33 lesions (10 malignant/23 benign lesions) were studied. Mean histological size was 14.5 mm. Nine EMR, 18 ESD and six hybrid resections were performed. A total of 93.9% lesions were resected in one piece. At six months’ follow-up, complete and definitive resection was obtained in 96.7% of cases. A vertical resection was insufficient in four cases. One GIST needed a complementary surgical resection, one neuroendocrine tumor was successfully treated by a new ESD session and two pancreatic rests were not additionally treated given the benign character and the absence of residual tissue in endoscopic control after six months. There was only one severe adverse event (2.9%); one pneumoperitoneum with ESD, three bleeding with one ESD and two EMR, always treated conservatively or endoscopically.
Conclusion
Endoscopic resection is safe and should be the procedure of choice for both diagnosis and definitive resection of subepithelial gastric lesions of size under 20 mm.
Keywords
Introduction
Subepithelial tumors (SETs) of the stomach are a diverse set of lesions from different submucosal tissue layers with cell-type-dependent specific evolution. The management of SETs is currently mainly based on endoscopic ultrasound (EUS) evaluation.1,2 The standard strategy for the management of gastric SETs advises that EUS allows confirming the intramural position, narrowing the differential diagnosis and determining the need for resection. 3 For lesions of a size <20 mm, regular monitoring by EUS is recommended. Endoscopic resection is indicated specifically when lesions grow in size or if they measure more than 20 mm, according to the EUS presentation and to the supposed histological subtypes. 4 However, SET characteristics as determined by EUS may not allow concluding on their malignant behavior.5,6 Furthermore, conventional biopsy, EUS-guided fine needle aspiration (EUS FNA) and EUS-guided Tru-Cut biopsy (EUS FNB) all have a low diagnostic accuracy rate for SETs, inferior to 65%.7,8 Therefore, the current standard strategy of surveillance until malignant evolution vs practicing a definitive resection is debatable.
Given uncertain diagnosis with EUS ± FNA or FNB, the burden of years of EUS follow-up and the risk of malignancy even for lesion of size <20 mm,9,10 endoscopic resection (ER) such as endoscopic submucosal dissection (ESD) is a good alternative to obtain an optimal tissue sampling and a curative treatment in selected SETs.11,12 In this context, the place of ER for gastric SETs of size <20 mm should be evaluated.
Methods
We performed a single-center, retrospective study of data collected in a prospective manner from patients with submucosal lesions of the stomach (SLS) that were endoscopically resected between September 2007 and December 2013. The study was conducted and monitored under institutional review board committee approval. The endoscopic center is highly specialized in therapeutic endoscopy, and especially in EUS with a rate of approximately 1000 EUS performed per year by four specialized hospital endoscopy practitioners. Eligible patients were of all ages, of all American Society of Anesthesiologists (ASA) score, who underwent an ER of all kinds of SLS. Previous attempt of ER or surgical resection was allowed and all SLS were previously evaluated by EUS ± FNA. There were no exclusion criteria. Data collection was conducted in a completely anonymous way by two physicians affiliated with the unit, external to the four endoscopists who performed the exams. To establish our list of patients we used a computer-generated database (4D program®) of all patients who underwent an ER by gastroscopy. Of these 505 patients, we manually collected all patients who underwent an ER of SLS (N = 33) and their individual characteristics. The different characteristics were established in an Excel® table of clinical criteria, technical resection used, both endoscopic and histological results, and potential adverse events.
All participants had a previous EUS ± FNA that confirmed the subepithelial position, the characteristics of the lesions and the predictive diagnosis. The method of resection was not fit in a protocol and was dependent on the practitioner’s choice, according to the characteristic, position or history of resection of the SLS. The three ER methods used for our patients were endoscopic mucosal resection (EMR), ESD or hybrid resection (HR) combining ESD at the edges of the lesion following by EMR for the final central resection. The quality of lateral and depth margins and the size of lesions were taken into account both for macroscopic resection and for histological examination. We also determined if the ER was complete, in one piece and whether a new treatment had been performed in case of an incomplete resection. Adverse events were also noted and separated according to their timing: early in the first 24 to 48 hours postoperatively or late after 48 hours postoperatively. Finally, results of a six-month follow-up comprising at least a new gastroscopy were collected. All these different data were collected manually through a computer program (Hospital Manager®) that allows managing medical records in our hospital. If any data were lacking, they were recovered from the family doctor or directly from the patients by phone.
The aim of this study was to determine the interest, the efficiency and the safety of ER for SLS of size <20 mm. The secondary end points were to determine the histological subtype and the characteristics of SLS, and to analyze the concordance rate between initial EUS ± FNA examination and final histological diagnosis.
Results
Clinical characteristics of patients
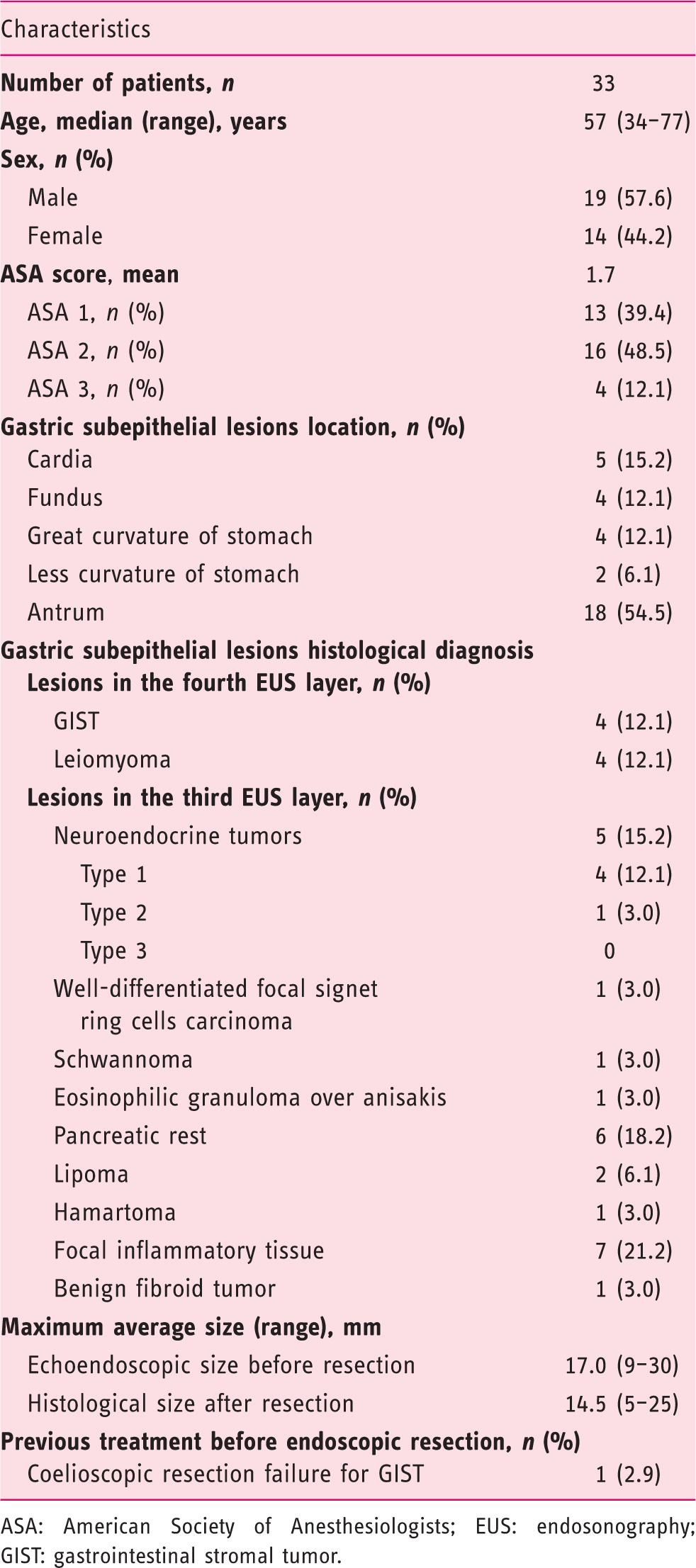
ASA: American Society of Anesthesiologists; EUS: endosonography; GIST: gastrointestinal stromal tumor.
Resection results

EUS: endoscopic ultrasound; EMR: endoscopic mucosal resection; ESD: endoscopic submucosal resection; HR: hybrid resection; SET: gastric subepithelial lesion; GIST: gastrointestinal stromal tumor.
A total of five adverse events were noted (15.1%), with four intraoperative adverse events and one late adverse event. There was only one severe adverse event (3.0%) corresponding to an intraoperative pneumoperitoneum after ESD for leiomyoma, managed conservatively. Three adverse events were bleeding after one ESD and two EMR always treated conservatively or endoscopically. One intraoperative anaphylactic shock over curare happened during an ESD, independent of the endoscopic procedure.
EUS and EUS FNA evaluation before resection
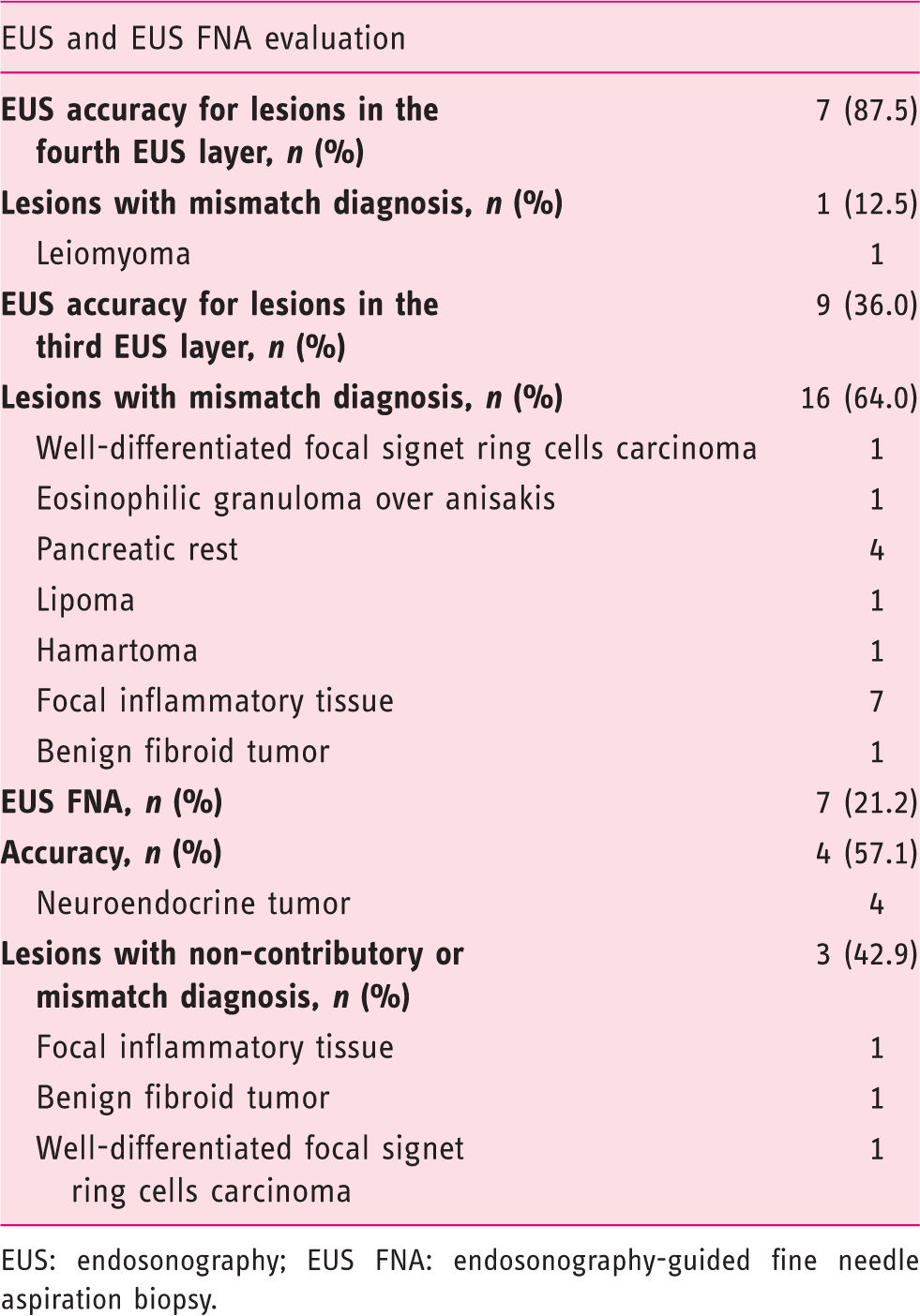
EUS: endosonography; EUS FNA: endosonography-guided fine needle aspiration biopsy.
Discussion
Endoscopic removal by ESD of early gastric cancer or relapse after EMR are currently recognized techniques with a success rate between 81% to 93% and show an acceptable safety profile.14,15 The most important issues for ER in case of early gastric tumors is to determine the limits of resection with the minimum of adverse events in order to achieve a complete and sustainable resection without local or distant recurrence. The management of SLS presents an additional difficulty given the submucosal location of the lesions.
This study shows the experience of a single Western European center in the endoscopic management of SLS based on clinical retrospective data. The majority of lesions that we encountered were benign, with a predominance of leiomyoma, pancreatic rest and focal inflammatory tissue. Approximately one-third of lesions had a potential or malignant behavior like GIST or NETs, corresponding to the data reported in the literature.16,17
Our results show an excellent success rate for endoscopic management of SLS with a complete and definitive resection for 96.7% of cases at six months. Only one case of NETs needed two ER sessions, with one HR followed by ESD. These results are comparable to previous data in the literature with an efficiency of ESD for gastric SETs described between 90% to 96.8%.18,19 The criterion of size with a mean size <20 mm, the location of SLS mainly in the antrum and the quality of practitioners can be taken into account to explain this successful rate.14,20 It should be noted that only one GIST located in the antrum, of a size of 15 mm, with malignant behavior (ki67 > 5%, mitotic rate > 5/50 high-power field (hpf)) and positive vertical margin after ESD, needed a complementary surgical treatment. We cannot conclude anything with our results about the impact of previous treatment on the quality of ER. The only patient with a previous failed attempt at surgical resection was a patient with a low-grade GIST of the fundus, finally completely and definitely resected by ESD.
Regarding the technical aspects and quality of resection, ESD seems to be superior to EMR and HR. We observed one case of incomplete macroscopic resection with EMR, two cases of piecemeal resection with HR, and none for ESD. Besides being able to complete resection in one piece, ESD provides a better evaluation of margins and especially for vertical limits of resection. 21 The overall safety profile is acceptable (88.0%) with only one significant intraoperative pneumoperitoneum. 22
A previous EUS is mandatory to confirm the subepithelial position of lesions, and the possibility of ER. 23 EUS alone, even with a diagnostic algorithm based on EUS findings, 24 cannot substitute for the histological diagnosis to determine the exact histological subtypes and potential malignant behavior of gastric SLS. 1 EUS concordance is particularly poor for lesions inside the third EUS layer and the interest of FNA or FNB for SLS is also limited with an accuracy ranging from 52% to 89% for EUS FNA6,25 and from 55% to 71% for EUS FNB6,26 in the literature. Even if results of FNA or FNB suggest a benign nature of SLS (in 28.6% in our study), it is difficult to establish a definitive diagnosis given a potential false-negative result (a well-differentiated focal signet ring cells carcinoma in our case, for example). De facto a reliable decision for the management of SLS should not be based only according to these explorations. Moreover, substantial adverse events related to biopsies are also described, with bleeding in up to 22% with EUS FNA 27 and septic adverse events in up to 4% with EUS FNB. 28 EUS FNB presents also more technical failure given the location of lesions and the use of the Tru-Cut needle. 6 A strip biopsy or EMR/ESD with partial resection is also described to obtain enough tissue for diagnosis. However, these techniques are not completely accurate (approximately 90%), 29 show almost the same inconvenience and potential complications as a complete ER, and can lead to difficulties in case of future need for ER. These methods may perhaps show a potential for management of larger gastric SETs to reduce the need for surgical operation, and have less potential for lesions of size <20 mm, in our opinion. Concerning our policy to practice EUS FNA or FNB for SLS, we stopped performing routine systematic biopsies after the development of ER given all the reasons previously described. This explains the small number of EUS biopsies realized in our study and the lack of biopsies performed for SLS in the fourth EUS layer, which could correspond to a GIST with potential malignant behavior.
Our study shows that the global management of SLS has been modified by ER in 29/33 cases (87.9%), which allowed stopping a costly follow-up for benign lesions in 23/33 (69.7%), permitted a definitive oncological treatment in 10/33 (30.3%), and discovered and treated a misdiagnosed malignant cancer (well-differentiated focal signet ring cells carcinoma) in one of 33 (3.0%). Patients with gastric SLS show poor compliance with surveillance recommendations, around 45%, 30 which highlights the importance of our results. Moreover, EUS practitioners present a significant ambiguity regarding criteria for malignancy and management of such tumors,31,32 and EUS biopsies are not totally accurate for SLS. The psychological comfort of patients has not been quantified in our study. But we can suppose that the need of a regular follow-up for an uncertain histological SLS can be stressful for some patients.
ER is more difficult to perform for SLS in the fourth EUS layer, with additional potential complications such as perforation and peritoneal seeding of tumor cells in case of malignant lesions like GIST. 33 The management of such lesions must be discussed in a multidisciplinary way, in order to decide the best resection pathway and oncological support. A SLS located deep in the fourth EUS layer with protrusion to the peritoneal side should be surgically resected or removed by endoscopic full-thickness resection for selected cases. 34 Our study is not designed to evaluate the management of such tumors and does not provide an answer to this problem. In contrast our results show an acceptable efficiency and safety profile for ER of SLS and GIST located superficially in the fourth EUS layer with protrusion to the lumen side of the stomach. Seven of eight lesions (88%) were fully and definitively resected, with only one GIST requiring additional surgical resection.
In conclusion, our data indicate that ER is efficient and safe for both diagnosis and definitive resection for SLS of size <20 mm. Given the risks of malignant behavior and the low accuracy of EUS ± FNA for gastric SETs, it can be recommended that ER should be the practice of choice after having confirmed the subepithelial position of SLS by EUS. Concerning the management of SLS larger than 20 mm or in a deep position in the fourth EUS layer, additional studies are needed to define the place of ER compared to the surgical pathway.32,35
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.