
Abstract
Background and aim
The optimal timing of oral refeeding in acute pancreatitis is unclear. This study aimed to perform a systematic review with meta-analysis of randomized controlled trials (RCTs) that compared early oral refeeding with standard oral refeeding in acute pancreatitis.
Methods
PubMed, the Cochrane library, and the Igaku-Chuo-Zasshi database were searched in order to identify RCTs eligible for inclusion in the systematic review. The weighted mean differences (WMDs) or odds ratios (ORs) with 95% confidence intervals (CIs) were calculated.
Results
Five eligible RCTs were included. Compared with standard oral refeeding, early oral refeeding significantly decreased the length of hospital stay (WMD: −2.22, 95%CI: −3.37 to −1.08, p = 0.0001). Although there was heterogeneity (I2 = 56%, p = 0.06), subgroup analysis of the refeeding criteria (immediate group and hungry group) eliminated the heterogeneity. There was no significant difference between the early refeeding group and standard refeeding groups with respect abdominal pain and distension (OR 1.14; 95%CI 0.65–1.99 and OR 1.53; 95%CI 0.81–2.90).
Conclusions
Compared with standard oral refeeding, early oral refeeding safely reduced the length of hospital stay in patients with acute pancreatitis.
Keywords
Introduction
Acute pancreatitis is a common disease that involves hospitalization. Estimated incidences range from 5.4/100,000 population per year in England to 79.8/100,000 in the United States, where more than 220,000 patients with acute pancreatitis are hospitalized each year.1,2 With regards to nutrition, fasting is performed in order to avoid pancreatic stimulation and facilitate pancreatic rest. The European Society of Parenteral and Enteral Nutrition guidelines suggest that, in mild acute pancreatitis, enteral nutrition (EN) is unnecessary, if the patients can consume normal food after 5–7 days. 3 In addition, EN is indicated, if possible, in severe necrotizing pancreatitis. 3 A meta-analysis demonstrated that significantly better mortality outcomes were observed when EN was started within 24 hours of admission compared with when it was administered between 24 and 72 hours. 4 However, the optimal timing of oral refeeding was unclear. Recently small randomized control trials (RCTs) were performed to investigate the timing of oral refeeding. Although some RCTs demonstrated a shorter length of hospital stay (LOHS) without differences in adverse events, this was not observed in another RCT.5–9 Our objective was to perform a systematic review and meta-analysis of RCTs comparing the benefits and risks of early and late oral refeeding, in order to achieve a better understanding of the optimal timing of oral refeeding.
Methods
Before performing the meta-analysis, we developed a protocol in order to define the search strategies and determine the study selection criteria, as well as identify the methods for relevant data extraction, quality assessment, and statistical analysis. 10
This meta-analysis was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). 11
Search strategy
PubMed, the Cochrane library, and the Japanese Igaku-Chuo-Zasshi database were used by two of the co-authors of this report (MH and TN) in order to perform a systematic literature search (from 1950 to 10 August 2015). A combination of the key words, ‘pancreatitis’, ‘oral’, ‘randomized’, and ‘nutrition’ was used for the search. Trials published in any language were included.
Inclusion and exclusion criteria
This study included all RCTs that compared the LOHS and rates of adverse events between early and standard oral refeeding in cases of acute pancreatitis. Duplicate publications and reviews were excluded.
Outcome measures
The LOHS and adverse events were the primary and secondary outcomes in this study, respectively.
Data extraction and interpretation
Two of the authors (MH and TN) independently examined all trials for eligibility. Disagreements were resolved by consulting a third author (HS). Particular attention was given to the started timing of the oral refeeding. Standardized data abstraction sheets were prepared. Extracted data included interventions, outcomes, and study quality.
Assessment of methodological quality
The methodological quality of each study was assessed using the risk-of-bias tool outlined in the Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0). 12 Two authors (MH and TN) evaluated all studies and assessed five key RCT quality influencers including the sequence generation, allocation concealment, blinding of participants and outcome assessors, management of incomplete outcome data, completeness of outcome reporting, and other potential threats to validity. Any discrepancy was resolved by consulting a third author (HS).
Statistical analysis
Data were entered into the Review Manager (RevMan; The Cochrane Collaboration, 2008; The Nordic Cochrane Centre, Copenhagen, Denmark). Separate analyses were performed for each outcome using a weighted mean difference (WMD) or an odds ratio (OR) with 95% confidence interval (CI). Heterogeneity was calculated by the I2 test, that showed that the rate of variation across studies was due to heterogeneity rather than chance (ranging from 0 [no heterogeneity] to 100 [maximum heterogeneity]). 13 An I2 score of ≥50% indicates more than moderate heterogeneity. All results were reported with a 95% CI. 14 A p-value of <0.05 indicated statistical significance. The random-effect model was used for all assessments, regardless of the significance of the heterogeneity.15,16 Some trials reported the median as the measure of treatment effect, with an accompanying interquartile range. For the purpose of our analysis, the medians were assumed as equal to the means, and the standard deviation (SD) was estimated from the interquartile range (SD = interquartile range × 0.74).17,18 In some trials, the patients in the early refeeding group were immediately allowed to eat as tolerated. In other trials, the decision to refeed was determined according to the patients’ verbalization of feelings of hunger or upon the return of bowel sounds. Therefore, we divided all eligible trials into the immediate and hungry groups, respectively, and performed subgroup analysis. Finally, we used funnel plot asymmetry to detect any publication bias in the meta-analysis and Egger’s regression test to measure funnel plot asymmetry.19,20
Results
Search results
We found 53 citations during our database search (Figure 1). Among these, 39 trials were rejected based on the exclusion criteria. Twenty trials were duplicate citations, 10 were unrelated to our topic and nine were reviews. The full texts of the remaining 14 eligible studies were examined. Another nine studies were excluded due to comparisons between the nasoenteric tube with ‘nil-by mouth’ (n = 4),21–24 total parental nutrition (n = 2),25,26 and oral diet (n = 1),
27
respectively, as well as between liquid diet and solid diets (n = 2)28,29 (Figure1). Finally, five studies were included in the systematic review and meta-analysis.5–9
Study flow of RCTs included in the systematic review.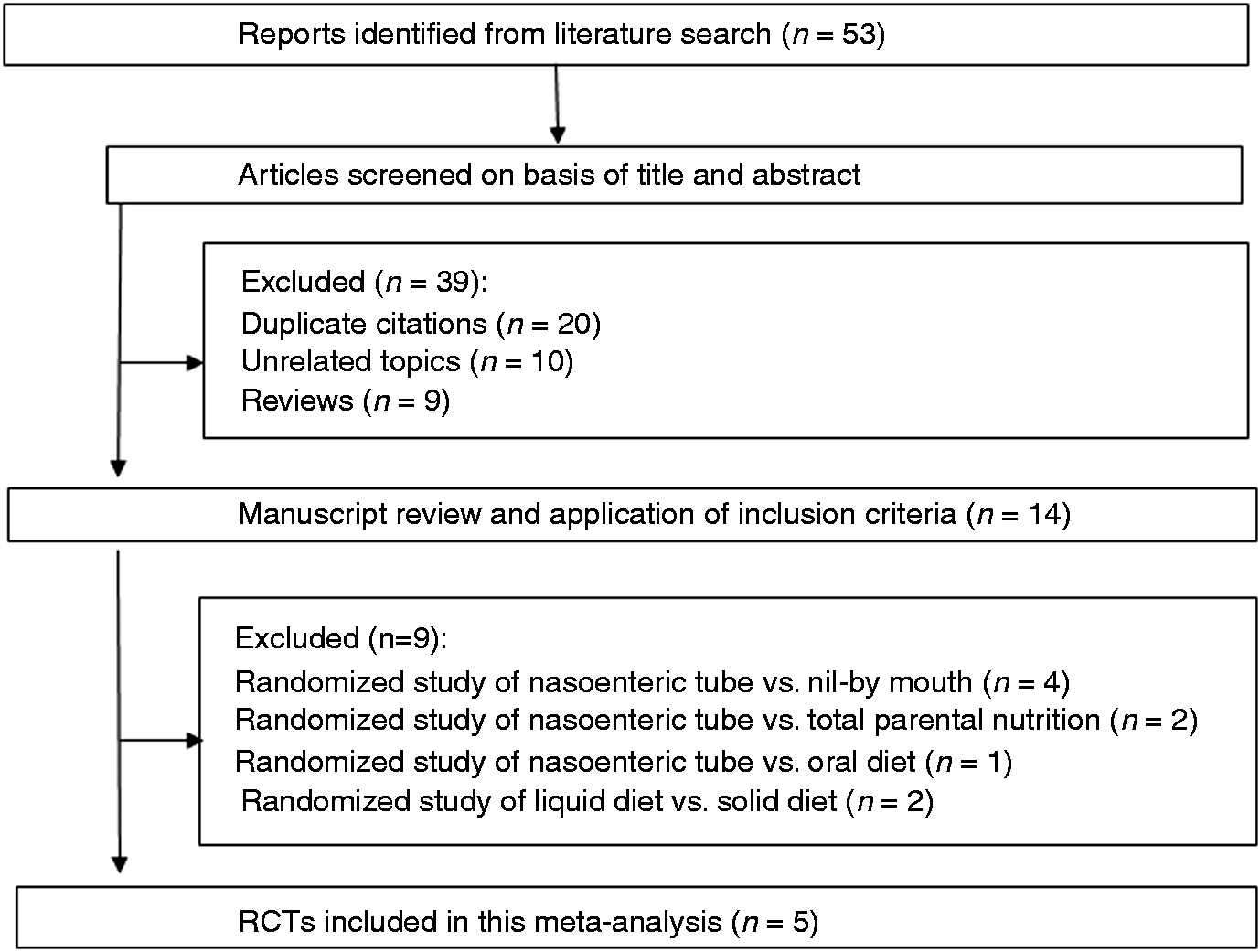
Quality assessment
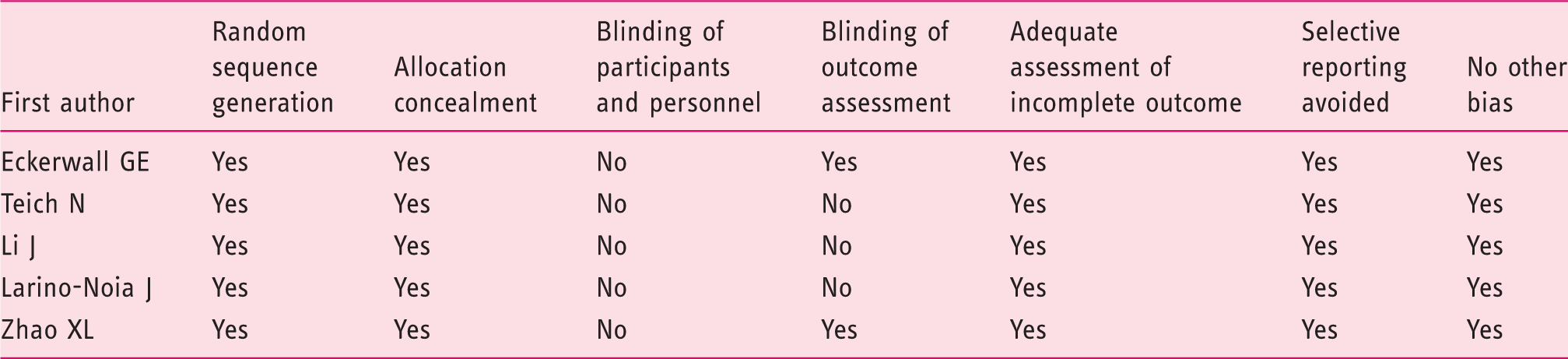
Evaluation of bias of RCTs included in the systematic review
Meta-analysis results
Characteristics of studies included in the systematic review
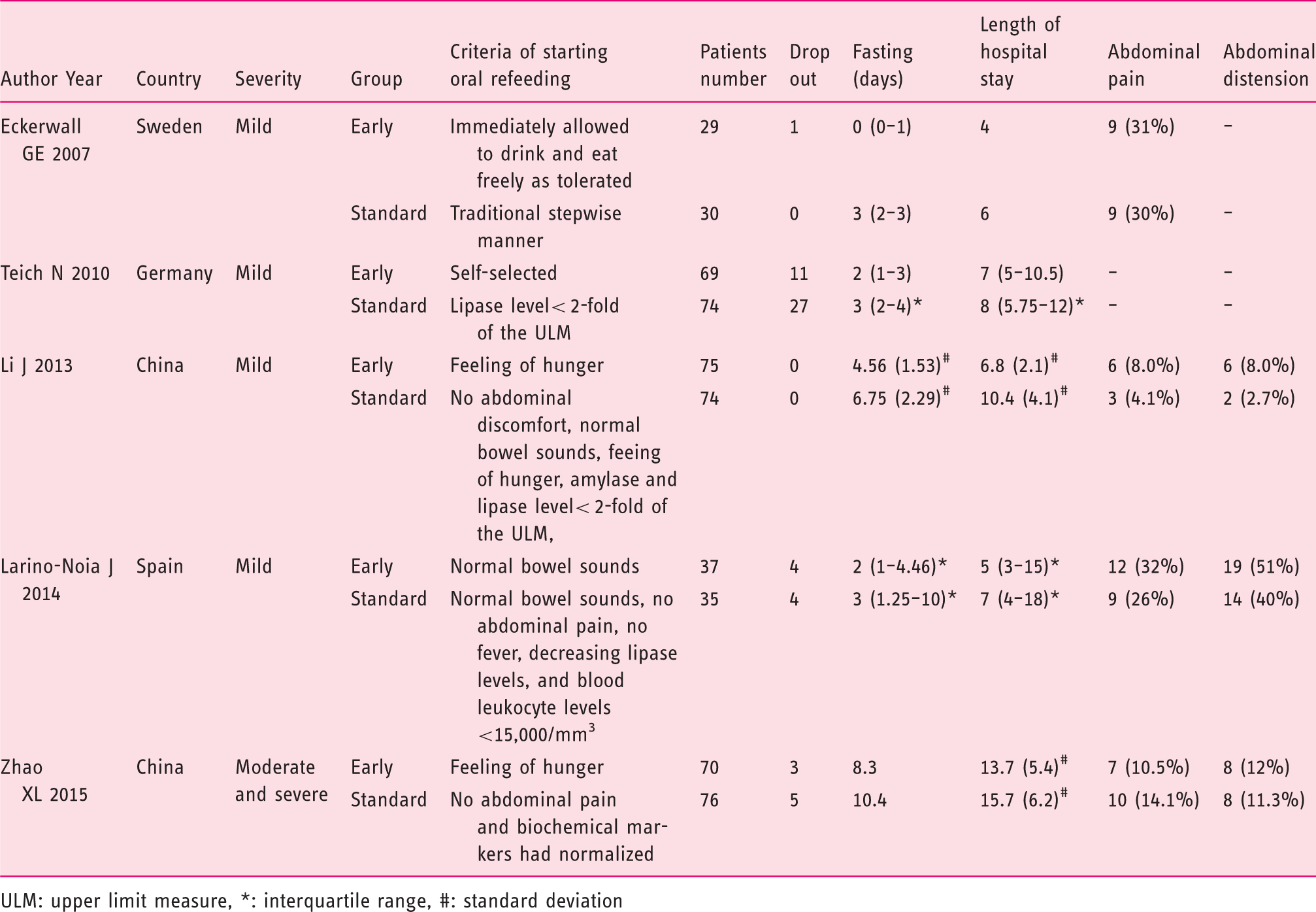
ULM: upper limit measure, *: interquartile range, #: standard deviation
Length of hospital stay
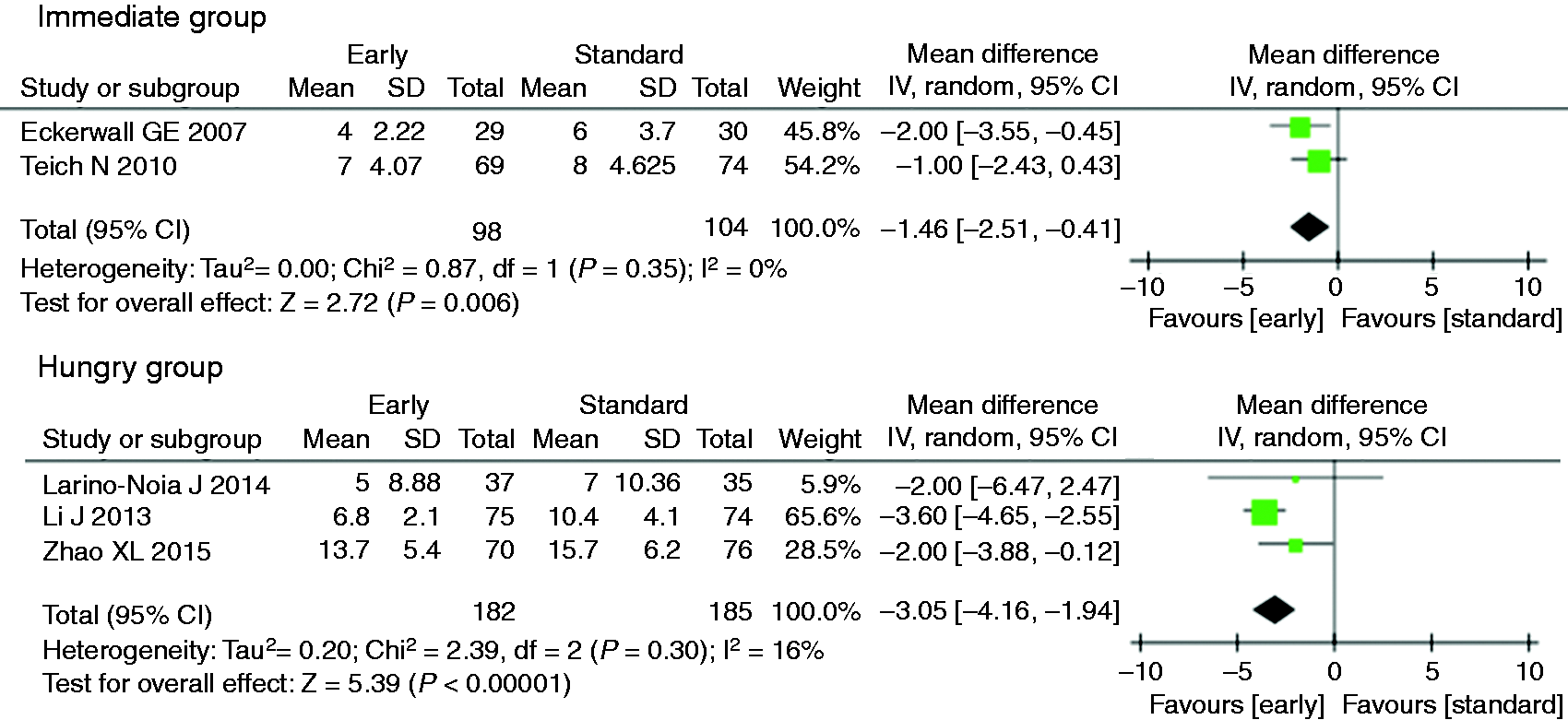
The LOHS was recorded in all five studies. Compared with standard refeeding, early refeeding significantly decreased the LOHS (WMD: −2.22, 95%CI: −3.37 to −1.08, p = 0.0001, Figure 2). However, there was heterogeneity among the trial results (I2 = 56%, p = 0.06). In two studies5,6 the patients in the early refeeding group were immediately allowed to eat as tolerated. In the remaining three studies7-9 the decision to refeed was determined by patients’ verbalization of feelings of hunger or upon the return of bowel sounds. Subgroup analysis indicated a significantly lower LOHS with early compared with standard refeeding for both the immediate and hungry groups (WMD: −1.46, 95%CI: −2.51 to −0.41, p = 0.006 and WMD: −3.05, 95%CI: −4.16 to −1.94, p = 0.0001, Figure 3), and the absence of heterogeneity (I2 = 0%, p = 0.35 and I2 = 16%, p = 0.30).
Forest plot displaying the weighted mean difference (WMD) and 95% confidence interval (95% CI) of each study for length of hospital stay (LOHS). Forest plot displaying the weighted mean difference (WMD) and 95% confidence interval (95% CI) of each study for length of hospital stay (LOHS) in subgroup analysis of refeeding criteria (immediate group and hungry group).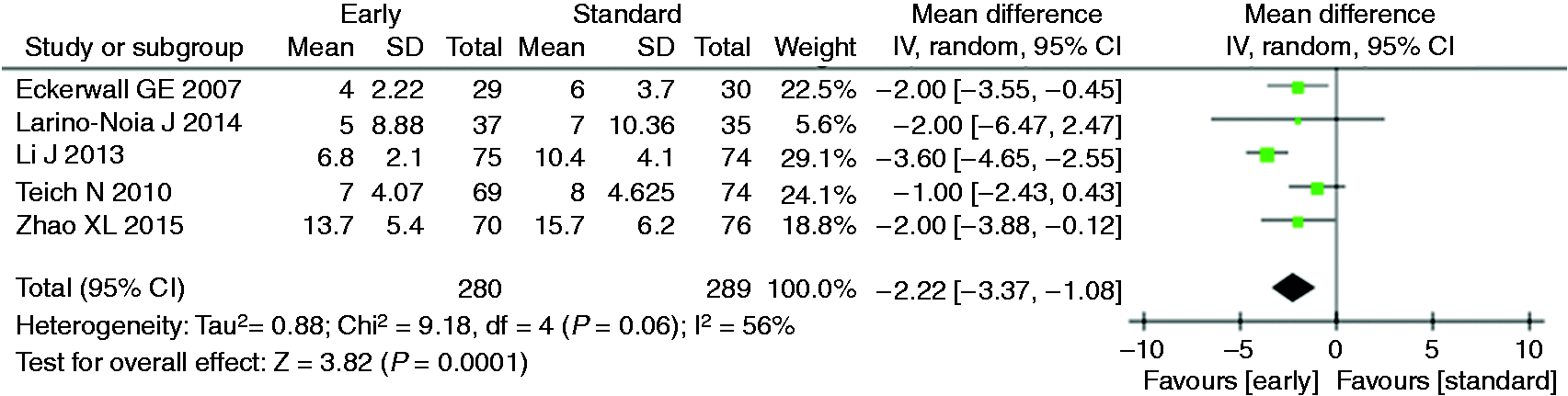
There was no evidence of publication bias because the Egger test suggested no significant asymmetry of the funnel plot (p = 0.453), (Figure 4).
Funnel plot of the included studies for length of hospital stay (LOHS) in acute pancreatitis.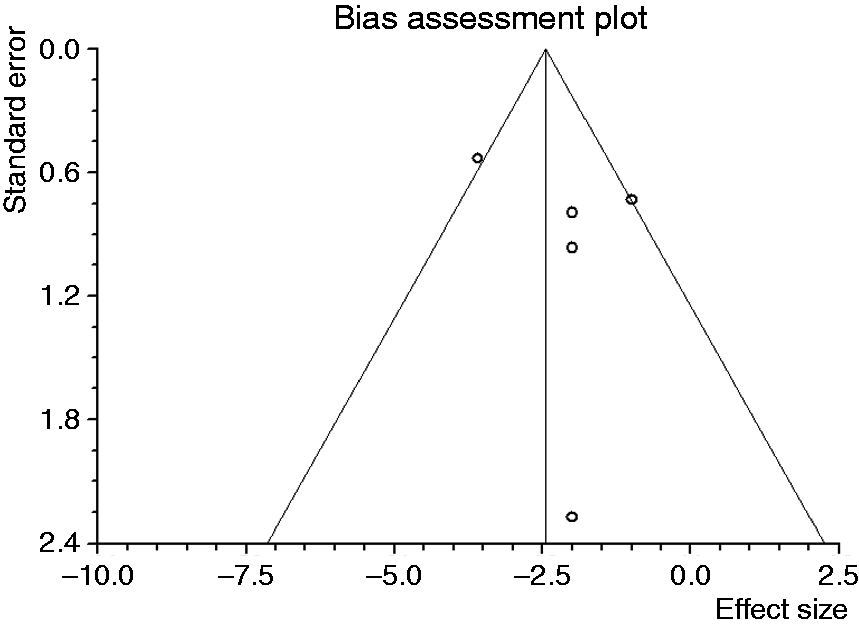
Adverse events
Abdominal pain relapse
Abdominal pain was recorded in all five studies. In four studies, the abdominal pain was described as present or absent, while a visual analog scale was used to describe the abdominal pain in one study. Thus, we included the four studies with abdominal pain description as present or absent in the meta-analysis. There was no significant difference between the early and standard refeeding groups according to abdominal pain (OR 1.14; 95%CI 0.65–1.99) (Figure 5) and no significant heterogeneity among the four studies (I2 = 0%, p = 0.67).
Forest plot displaying the odds ratio (OR) and 95% confidence interval (95% CI) of each study for abdominal pain and abdominal distention.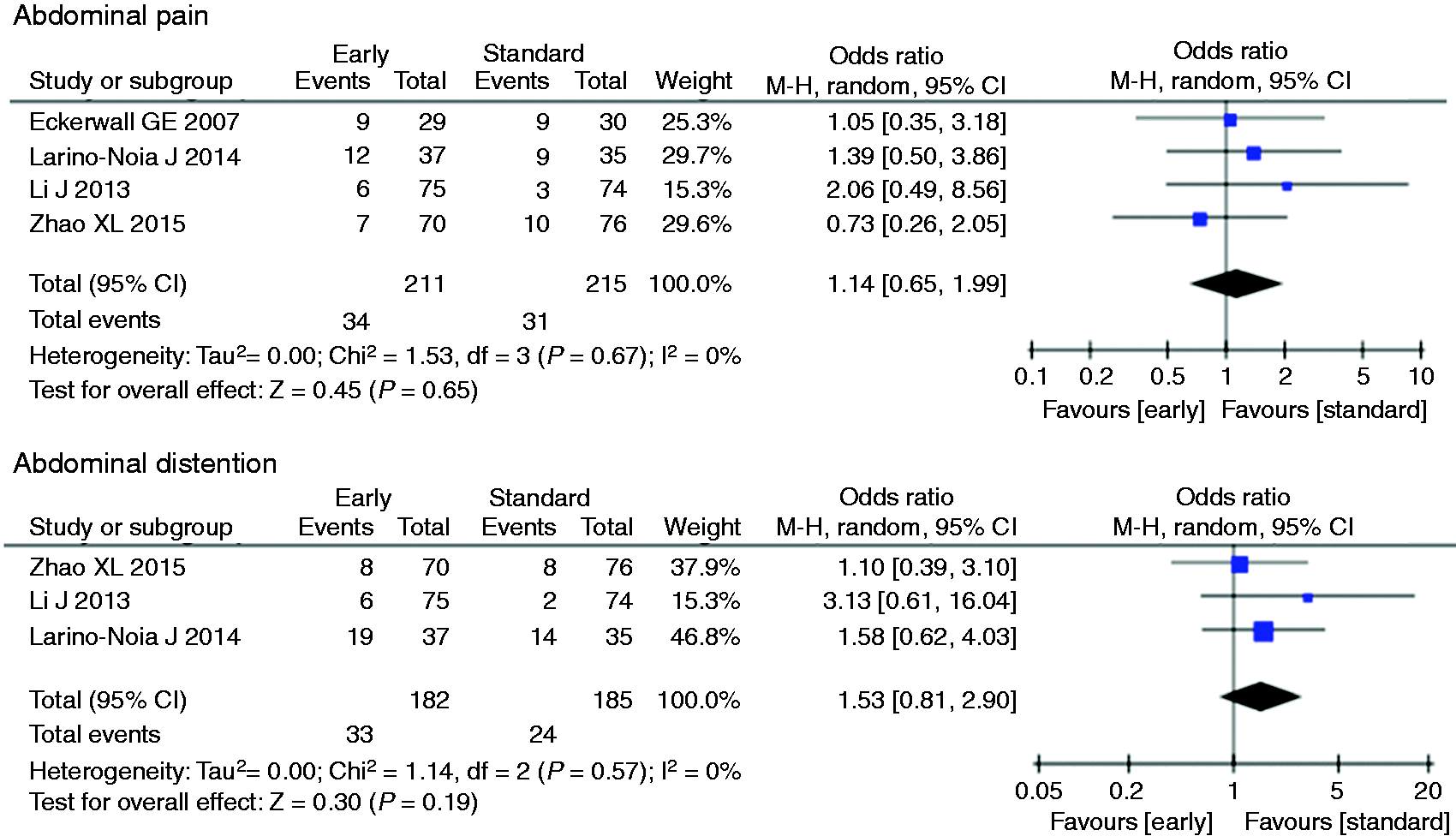
Abdominal distension
The abdominal distension was recorded in three studies. There was no significant difference between the early and standard refeeding groups. (OR 1.53; 95%CI 0.81–2.90) (Figure 5), and no significant heterogeneity among the three studies (I2 = 0%, p = 0.57).
Nausea
Nausea was recorded in two studies by Eckerwall et al. 5 and Larino-Noia et al. 8 There were 66 patients in the early oral refeeding group and the 65 patients in standard oral refeeding group. There was no significant difference between the early and standard refeeding groups (OR 0.62; 95%CI 0.20–1.90), and no significant heterogeneity in the two studies (I2 = 34%, p = 0.22).
Vomiting
Vomiting was recorded in two studies by Eckerwall et al. 5 and Larino-Noia et al. 8 There were 66 patients in the early oral refeeding group and the 65 patients in standard oral refeeding group. There was no significant difference between the early and standard refeeding groups (OR 1.00; 95%CI 0.29–3.44). There was also no significant heterogeneity between the two studies (I2 = 34%, p = 0.22).
Other adverse events
Other adverse events, including diarrhea, pleural effusion, atelectasis, fluid collection, postprandial fullness and readmission within 3 months, were recorded in one study. Diarrhea, pleural effusion, atelectasis, fluid collection and readmission within 3 months, were reported by Eckerwall et al. 5 The total number of patients was 59. Postprandial fullness was reported by Larino-Noia et al. 8 and the total number of patients was 72. There was no significant difference between the early and standard refeeding groups in each study.
Discussion
This systematic review and meta-analysis revealed that early oral refeeding in acute pancreatitis reduces LOHS with no significant differences in the adverse events. This is the first systematic review of the optimal timing of oral refeeding in acute pancreatitis. It is worth noting that this meta-analysis also demonstrated heterogeneity in the LOHS. Factors contributing to this variability may include the selection criteria of the participants, severity of pancreatitis, refeeding schedule, and criteria for refeeding. Subgroup analysis of the refeeding criteria (immediate and hungry groups, respectively) eliminated the heterogeneity.
The results of this study might affect treatment strategy and potentially reduce the cost of hospitalization in acute pancreatitis. The reasons for the shorter LOHS in early oral refeeding include shorter fasting time and accelerated recovery. If the shorter fasting time caused abdominal pain relapses or some adverse events, shorter LOHS would not be observed. However, our systematic review demonstrated that there was no significant difference between the early and standard refeeding groups, according to adverse event. In a study involving rats, although the orally fed rats had adverse blood levels of pancreatic enzymes, more severe inflammatory changes were observed in the pancreas of the rats that were fed parenterally. This study suggests that certain hormones released from the duodenum upon stimulation by oral nutrient intake lessen the severity of pancreatitis. 30 Thus, early oral refeeding might accelerate recovery.
There are several published meta-analyses of nutrition in acute pancreatitis. The meta-analysis by Li et al. showed that significantly better mortality outcomes were observed when EN was started within 24 hours of admission compared with when it was administered between 24 and 72 hours. 4 The meta-analysis conducted by Chang et al. demonstrated that nasogastric feeding was safe and well tolerated compared with nasojejunal feeding. 31 The meta-analysis conducted by Meng et al. showed that in comparison with the clear liquid diet, neither the non-liquid soft nor solid diet increased pain recurrence after refeeding. 32 The non-liquid diet reduced hospitalization. 32 In addition, another RCT revealed no significant difference between the jejunal tube and oral refeeding methods. 27 These results indicate that early oral refeeding with a solid diet might provide better outcomes and is safe for acute pancreatitis patients. The results of our meta-analysis were also supported by these studies.
This systematic review has several limitations. First, the choice of the LOHS as a primary outcome may entail bias because a physician or medical team determined the discharge decision; the patient’s information may have been concealed from the physician or medical team; the decision may have been affected by the patient or their family’s desire; the timing of discharge (i.e. weekend); and other factors. Ideally, the primary outcome is the length of days until the pancreatitis has resolved. Second, most of the study participants had mild pancreatitis. Therefore, it may be necessary to carry out EN in patients with severe pancreatitis. Third, each study was very small. Thus, the adverse effect might not be revealed by the small sample size of patients. There is still no consensus about the definition of ‘early’ refeeding. Further studies with larger numbers of patients are warranted, in order to clarify the safety and efficacy of early refeeding for acute pancreatitis.
In conclusion, early oral refeeding is safe and reduces the LOHS compared with standard oral refeeding in acute pancreatitis.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of Interest
During the last 2 years, Author HS received scholarship funds for the research from Astellas Pharm Inc., Astra-Zeneca K.K., Otsuka Pharmaceutical Co., Ltd., Takeda Pharmaceutical Co., Ltd., and Zeria Pharmaceutical Co., Ltd. and received service honoraria from Astellas Pharm Inc., Astra-Zeneca K.K., Eisai Co., Otsuka Pharmaceutical Co., Ltd., Takeda Pharmaceutical Co., Ltd., and Zeria Pharmaceutical Co., Ltd. Author TK received scholarship funds for the research from Astellas Pharm Inc., Astra-Zeneca K.K., Otsuka Pharmaceutical Co., Ltd., Takeda Pharmaceutical Co., Ltd., Eisai Pharmaceutical Co., Ltd., Zeria Pharmaceutical Co., Ltd., Tanabe Mitsubishi Pharmaceutical Co., Ltd. JIMRO Co., Ltd., Kyorin Pharmaceutical Co. Ltd., and received service honoraria from Astellas Pharm Inc., Eisai Pharmaceutical Co., Ltd., JIMRO Co., Ltd., Tanabe Mitsubidhi Pharmaceutical Co.Ltd., Otsuka Pharmaceutical Co., Ltd., Takeda Pharmaceutical Co., Ltd., Miyarisan Pharmaceutical Co. Ltd., and Zeria Pharmaceutical Co., Ltd. Author NY received scholarship funds for the research from Astra-Zeneca K.K., Takeda Pharmaceutical Co., Ltd., Eisai Co., Top Corporation, Kaigen Pharm Co., Ltd., ASKA Pharmaceutical Co., Ltd., FUJIFILM Corporation, Boston Scientific Japan K.K., Century Medical Inc., and Covidien Japan Inc. The funding source had no role in the design, practice or analysis of this study. There are no other conflicts of interests for this trial.